
Abstract
This article illuminates the unique experiences of older LGBTQ + adults in cities based on intersectionality theory. The main themes that emerged from the review of the literature were fear and isolation, service access, housing, and economic instability. The scholarship shows that many forms of marginalization influence this group's access to housing as well as health and care services for older LGBTQ + adults. I argue that planners must advocate for policies, trainings, and data collection to increase the social inclusion, economic security, health, housing and safety of older LGBTQ + adults.
Keywords
Why Plan for LGBTQ + Older Adults
Older LGBTQ + adults represent a large constituency today, currently estimated at three million U.S. adults over the age of 50 (Fredriksen-Goldsen and Kim 2017) and growing to an estimated 20 million by 2060 (Fredriksen Goldsen et al. 2019). By 2050, 40% of LGBTQ + older adults will be people of color, which is double the current population (Adelman 2016). Although there has been a recent increase in attention to planning for aging populations (Choi and Warner 2015; Kan, Forsyth and Molinsky 2020; Warner and Rukus 2013; Warner, Homsy and Morken 2017), older LGBTQ + adults remain largely invisible in aging services, policies, and research (Fredriksen-Goldsen 2016). The American Planning Association's Aging in Community Policy Guide only mentions older LGBTQ + adults once (APA 2014). Planning practitioners remain slow to respond to the unique needs of a diverse aging population.
Older LGBTQ + adults face heightened risks of social isolation, including housing, economic, and health disparities. This group requires different, targeted social and environmental support from their cities and neighborhoods. A gender life course framework of cumulative (dis)advantage (Carpenter 2010) contextualizes the decades of legalized and interpersonal discrimination and criminalization that older LGBTQ+ adults have faced, resulting in resilience for some and vulnerability for others. These life course changes have also resulted in spatial shifts, especially a dispersal from historically gay neighborhoods, which may have added effects on their physical and mental wellbeing (Doan 2018; Ghaziani 2014; Gieseking 2013; Podmore 2006; Tongson 2011). Compared to non-LGBTQ + older adults, LGBTQ + older adults experience higher risks of disability, homelessness, social isolation, depression, poverty, alcohol dependence, housing deficiencies and premature institutionalization (De Vries 2014; Espinoza 2011; Fredriksen-Goldsen et al. 2011; Witten 2014; Zelle and Arms 2015). LGBTQ + older adults are also twice as likely to live alone, twice as likely to be single, and 3 to 4 times less likely to have children, with many estranged from their biological families (MAP and SAGE 2010; SAGE 2020b). These factors make LGBTQ + older adults particularly vulnerable to social isolation and its related problems given gerontology's core principle of substitution (Cantor and Mayer 1978) whereby older adults first seek care from a spouse, then adult children, and then other family.
Planning scholars (Forsyth 2011; Wesley 2015) have identified the need for planners to study the unique needs of older LGBTQ + adults, particularly with respect to housing (Hillier and Bunten 2021) and community-level LGBTQ + aging solutions in different geographies, as well as social and physical environments (Ranahan 2017). The lack of longitudinal data on older LGBTQ + adults illuminates a gap in the research. In order to understand how planners could improve the lives of older LGBTQ + adults in the U.S., I will review scholarship on older LGBTQ + adults’ experiences with social isolation, service access, economic instability, and housing. The minimum age for LGBTQ + adults studied in the literature is 45 years old. While some studies have a defined maximum age for their sample, others study the experiences of the “oldest old” adults, which the World Health Organization (2001) defines as 80 years and older. The final part of the paper will review recommendations for planners to better meet the needs of older LGBTQ + adults.
On Terminology
I use the term “older adult” or “older person” interchangeably throughout this paper because the United Nations Committee on Economic Social and Cultural Rights of Older Persons declared a preference for the term “older persons” instead of “elderly,” which was seen as ageist (1995). 1 The Journal of Geriatric Physical Therapy supported this language as “precise, accurate, and value-free” (Avers et al. 2011). The national organization, Old Lesbians Organizing for Change (OLOC), however, uses “old” to reclaim the term for consciousness-raising with a feminist mission (Raphael 2006). Older lesbians in advocacy groups such as OLOC and ZamiNobla, the National Organization of Black Lesbians on Aging, are transforming their communities and society by discussing aging in a positive way. Without taking traditional, heteronormative paths, older lesbians in OLOC find resistance in lesbian-feminist critiques of capitalism, difference, and healing that show promise for a radical approach to planning by bringing disadvantaged gender and sexual minorities “from margin to center” (hooks 1984).
The literature reviewed in this paper samples older adults who are part of the Silent Generation (born from 1925 to 1942) and Baby Boomers (born 1943–1960) (see Strauss and Howe 1991 for expanded analysis of generational cohorts and Myers 1983 for a cohort analysis on planning for housing mobility). Because few LGBTQ + people among these generations have reclaimed queer in the same way that younger generations have, I do not use queer and instead use LGBTQ + as an umbrella term to describe anyone who does not fall inside of traditional heterosexual, cisgender, and/or endosexed identities. This may include but is not limited to those who identify as gay, lesbian, bisexual, transgender, two-spirit, pansexual, genderqueer, agender, and/or intersex. In a few instances, I use LGB, instead of LGBTQ + , if the study did not sample transgender older adults. In doing so, I seek to avoid homogenizing language that conflates gender identity and sexual orientation, which might lead to inaccurate data reports (Westwood, 2020).
This project contributes to queer scholarship as it questions assumptions about gender, sex, and sexuality to the development of material and social change (Browne and Nash 2010; Cohen 1997; Ghaziani and Brim 2019). A central goal of this paper is to demonstrate the need for “distinctively queer methods” in studying planning for aging in order to integrate historically complex, changing subjects with multi-issue identity politics (Ghaziani and Brim 2019, 10). This fluidity is especially important in planning for aging because “older adults” is not a stable category so the “best practices” for today must allow for new possibilities to reflect the shifting needs of LGBTQ + people to emerge as they age in the future.
Intersectional Framework
Identifying the unique needs of people who are LGBTQ + and older through a framework of intersectionality offers a radical potential for serving those with multiple identities on the margins; those who are neither fully served nor recognized within single-identity-based politics and movements. With an extensive intellectual and political genealogy, intersectionality comes out of Critical Race Theory (Delgado and Stefancic 2017), Black feminism (Lorde 1984; Smith 1983), and women of color theorizing and praxis (Anzaldúa 1987; Combahee 1983; Lugones 1994, 2007; Moraga and Anzaldúa 1981) to describe the unique experiences of people with multiple marginalized identities (Cohen 1997, 1999; Collins 1998, 2004; hooks 1989; Johnson 2001, 2018). Legal scholar, Kimberlé Crenshaw (1991), coined the term to describe and recognize Black women as situated within overlapping, simultaneous, and mutually constituting systems of oppression (i.e. gender and racial). In other words, Black women's experiences are not the combination of Black men's experiences with racism and white women's experience with sexism, but, rather, an experience unique from both demographics. Crenshaw (1991) also uses intersectionality to highlight that Black women's experiences with overlapping systems of oppression also manifests in their marginality within social movements that resist the very subordination they experience (i.e. feminism and anti-racism). Scholars emphasize that intersectionality¬–and being intersectional¬–is rooted in and oriented toward social transformation that challenges systems of oppression (Collins and Bilge 2016; Hancock 2007; May 2014, 2015).
This paper is not meant to essentialize the experiences of all older LGBTQ + adults in the United States considering this heterogeneous group has conflicting identities, such as race, class, and gender. I explore the lived experiences of older LGBTQ + adults through a lens of intersectionality to understand the ways that planners, policymakers, and service providers might acknowledge older people's differences based on their LGBTQ + identity and consider how those differences may influence their access to places, resources, and services. Intersectionality attends to both lived experiences and sites of structural power (Cho, Crenshaw, and McCall 2013).
Dominant planning frameworks tend to promote a limited and universalizing approach for people who are aging, rather than an intersectional, holistic view of identity that centers structural power and agency limited by poverty (Hillier and Bunten 2021). Neglecting the heterogeneity of experience within a single category as extensive as age is inadequate, even misleading. Scholarship on planning for aging populations highlights the importance of public engagement and collaboration with older people for better community health (Zhang, Warner, and Wethington 2020) and service delivery (Warner, Homsy, and Morken 2017), but largely neglect the effects of sexual orientation and gender identity (SOGI) on their access to health, care services, and housing.
Planning scholars are beginning to write about the LGBTQ + community with an intersectional lens by making visible the diversity within the LGBTQ + population, centering the multiple identities that people in the LGBTQ + community hold (Catungal 2015; Doan 2011, 2015; Frisch 2015; Irazábal and Huerta 2016; Wesley 2015; Whittemore 2015). Queer planning brings planning scholarship into conversation with feminist and queer studies around the fundamental notion that gender and sex are a fluid performance based on place, time, politics, and discourse (Butler 1990; Doan 2011; Foucault 1978). Bringing traditionally separated disciplines together in queer planning shows the multiple axes of disenfranchisement that limit the recognition, representation, and citizenship of the LGBTQ + population. As the literature on queer planning grows, scholars and practitioners must pay additional attention to aging and the unique needs and desires of older LGBTQ + adults.
Sources of Fear & Social Isolation
Queer theorists have long demonstrated the importance LGBTQ + people's access to social interaction as a way of constituting and developing one's LGBTQ + identity. Queer theorist, Lisa Duggan (1993), defines identity construction as “a process in which contrasting ‘stories’ of the self and others¬–stories of difference¬–are told, appropriated, and retold as stories of location in the social world of structured inequalities” (793). In short, LGBTQ + identity is inherently relational, as postcolonial queer feminist scholar, Sarah Ahmed (2006), puts it. Given the importance of social relations for some LGBTQ + people's identity, older LGBTQ + adults’ heightened risks of social isolation can be especially detrimental to their sense of self, compared to older heterosexual adults.
Stigma based on LGBTQ + identity has had disproportionate impacts on older LGBTQ + adults as they lose support systems and risk greater social isolation. As such, being a part of a larger, united community can be especially important for this group. Fredriksen Goldsen et al. (2019) suggest that social isolation is the strongest predictor of low quality of life and depression for older LGBTQ + adults. Given this heightened importance of social inclusion, older LGBTQ + adults’ most important services are social events and support groups with 89% of older LGBTQ + adults reporting their pride in participating in LGBTQ + community (Fredriksen-Goldsen et al. 2011). According to data from CenterLink and the Movement Advancement Project (MAP) (CenterLink & MAP 2016), 61% of the 105 LGBTQ + community centers reported providing services to fit the unique needs of older adults, as well as programs focused on older LGBTQ + adult outreach or physical and mental health programs.
Although the wider LGBTQ + community seems to show support for older LGBTQ + adults vis-à-vis services, a report on improving the lives of older LGBTQ + adults conducted by MAP and Services & Advocacy for LGBT Elders (SAGE) (MAP & SAGE 2010) found that older LGBTQ + adults often feel unwelcome in the larger LGBTQ + community and at LGBTQ + community centers, specifically (Boggs et al. 2017). This finding contributes to the rich scholarship that demonstrates queer spaces have been and continue to exclude marginalized members of the LGBTQ + community based on race, class, and gender; and, I would also add age (Bell and Valentine 1995; Browne, Lim and Brown 2007; Malanson 2005; Nast 2002; Oswin 2008; Walcott 2007). Considering many social spaces, LGBTQ + or not, have a youth-oriented culture that can feel alienating to older adults, it is no wonder that this report also found 42% of older gay men tend to feel the LGBTQ + movement does not engage older LGBTQ + adults in activities enough.
By 1977, Douglas Kimmel and Chris Almvig had heard many stories from older LGBTQ + adults’ regarding their experiences with isolation from the broader LGBTQ + movement, catalyzing them to found SAGE, Services & Advocacy for GLBT Elders. SAGE is the first organization dedicated to ensuring that LGBTQ + older adults age with respect and dignity (Gutterman 2021; SAGE 2020a). Since its establishment, SAGE has become the most influential social service and advocacy organization to serve LGBTQ + older adults in the United States. The national network provides supports, resources, and spaces for LGBTQ + older adults to build relationships and find care (SAGE 2020a). 2
Many older LGBTQ + adults fear harassment and discrimination, which can often manifest in social isolation that leads to a disconnection from necessary and supportive services (Butler 2004; Cahill, South and Spade 2000). Though LGBTQ + people can experience ageism, discrimination, and social isolation at any age, from people both in LGBTQ + spaces (Han 2007; Malanson 2005; Robinson 2015) and outside of them (Dwyer 2015; Gray 2009), the effects of cumulative, lifelong disadvantage among older LGBTQ + adults can lead to different disparities than those of LGBTQ + younger adults and LGBTQ + youth (Carpenter 2010). These support networks are so important for aging adults because they can lead to greater access to aging and health services as well as improved health outcomes (SAGE and AARP 2021). More specifically, support is often necessary for older LGBTQ + adults to both complete daily tasks as well as cope with larger challenges and transitions later in life (e.g. financial, emotional, physical). As the LGBTQ + community continues to disperse outside of traditional gayborhoods (Anacker 2011; Bain and Podmore 2021; Forsyth 1997; Ghaziani 2019; Gieseking 2013; Podmore 2006), older LGBTQ + adults could be facing added challenges in finding social networks that foster a sense of belonging.
Due to homophobia from aging and health care service employees, as well as other residents if one is living in a retirement community, several studies have shown that older LGBTQ + adults 50 years and older fear disclosing their LGBTQ + identity (Gardner, de Vries, and Mockus 2014; Stein, Beckerman, and Sherman 2010; Löf and Olaison 2020; Espinoza 2014; Adelman, 1986; Kum 2017). Older LGBTQ + adults’ fear of discrimination might be reflective of the cumulative discrimination they have experienced over their lifetime. One respondent in Hash; (2006) qualitative study of older adult caregivers for their same-gender partners described the anticipation of fear, “Even though I was not treated badly, I always had that fear that I could be treated badly . . . there is always a threat that you carry around in your heart that they can be bad to you” (133). Queer theorists have long cited disclosure, or “coming out,” as an integral part of gender performance that resists heterosexism, provides liberation from restrictive norms, and promises progress toward LGBTQ + equity and broader social transformation (Butler 1993; Sedgwick 1990).
Based on a national survey of 200 LGBTQ + adults 80 years and older, Fredriksen-Goldsen et al. (2019) found that 80% of respondents experience ongoing discrimination (e.g. media stereotypes, insults, and invalidation), which predicted a lower quality of life as well as physical and mental health problems. In the Caring and Aging with Pride study of 2,560 LGBTQ + adults aged 50 to 95, Fredriksen-Goldsen et al. (2011) found that respondents have experienced police violence (27%), had an object thrown at them (23%), and had their property damaged or destroyed (20%). Transgender older adults reported higher levels of violence and discrimination in all categories. Policymakers can adopt an LGBTQ + long-term care residents’ bill of rights to begin protecting the livelihoods of older LGBTQ + adults as they seek health and care services (SAGE and AARP 2021).
Fearing ignorance, discrimination, and abuse by service providers, police, and healthcare workers (Boggs et al. 2017), older LGBTQ + adults would benefit from a mandate of a minimum level of staff trainings on LGBTQ + cultural competency and nondiscrimination policies for state-funded providers (SAGE 2020b). In a 2010 national study of aging providers, only one-third of responding agencies offered staff training on LGBTQ + issues (Knochel et al. 2011). This is even more important for older LGBTQ + adults who experience the additional fears and discrimination based on race, ethnicity, class, origin, citizenship status, marital status, language, and English proficiency/accent (Auldridge and Espinoza 2013; Barnes 2005; Kum 2017; MAP and SAGE 2017; Martinez 2015; Woody 2014, 2015).
Discrimination is also a factor in older LGBTQ + adults’ work environments. Based on a 2014 cross-section of a longitudinal study of 2,450 LGBTQ + adults age 50 and older, most older LGBTQ + adults in the U.S. report workplace disadvantages, which can result in long-term economic disparities or an added need for full-time employment among the oldest of LGBTQ + adults (Fredriksen-Goldsen et al. 2017). Other older LGBTQ + adults may also choose to stay working in order to mitigate loneliness and remain engaged in their communities. More research is needed to better understand the motivations for employment among the oldest LGBTQ + adults in order to work through both the social and economic support that can help them stay healthier longer. Planners and others interested in social inclusion, health, and community quality have very little information to go on, particularly about everyday lived experiences, for how to build bridges for older LGBTQ + adults. Ranahan (2017) suggests that community-based organizations, such as religious institutions, might be the most effective agents in connecting with underserved and socially isolated members of the LGBTQ + community.
Objectification, invisibility, and isolation are key issues raised by older lesbians (Raphael and Cruikshank 2015). In Woody's (2014) qualitative study of ageism and heterosexism among 15 older African American lesbians and gay men, one lesbian age 67 explained: What I find is like being placated because you are older. I have to say things two and three times, not because they don’t hear me, but because they don’t see me. It's like I’ve become invisible or something. And now I have to raise myself and my voice to be heard [she sits straight in her chair to demonstrate]. …Because they see my gray hair or see me walking slowly…it's like I don’t know anything (156).
Healing from internalized ageism through consciousness-raising work is a central focus for OLOC's organizing model. More research needs to be done to understand the extent to which OLOC's reclamation of “old” is a useful tactic for liberation from internalized ageism. With lower likelihoods of social support and higher likelihoods of living alone than heterosexual older adults, self-deprecation suggests one of many root causes for older LGBTQ + adults’ higher rates of depression and isolation compared to non- LGBTQ + older adults (Fredriksen-Goldsen 2016).
Service Inaccessibility
Older LGBTQ + adults’ social isolation can manifest when service providers erase LGBTQ + adults’ differences and lived experiences, believing all older adults have the same issues and should be treated the same (Choi and Meyer 2016). Considering many older LGBTQ + adults have experienced violence over their life courses because of their LGBTQ + identity, their increased fear of discrimination needs to be incorporated into the services provided to them (Fredriksen-Goldsen 2016). Health and aging care service access are particularly important considering older LGBTQ + adults face higher rates of chronic conditions compared to the non-LGBTQ + older adult population. Based on Wallace et al. (2011) study of data from the California Health Interview surveys, including 1,052 older LGB 3 adults aged 50–70, lesbian and gay women are 1.35 times more likely to experience psychological distress and 1.32 times more likely to be living with a physical disability compared to similarly aged heterosexual women. Though the study does not control for HIV infection, older gay and bisexual men report fair or poor self-assessed health status 1.5 times more often than straight men with similar demographics. Compared to cisgendered and endosexed older LGBTQ + adults, older transgender and intersex adults have added challenges with medical and service access (Nowakowski, Sumerau and Lampe 2020; Witten and Eyler 2012). In a nationally representative survey of 2,376 people ages 45–75, Espinoza (2014) found that 20% of LGB older adults and almost half (44%) of transgender older adults fear that disclosing their sexual orientation/gender identity would damage their relationships with healthcare providers.
Fredriksen-Goldsen et al. (2013) found that discrimination and stigma can deter some older LGBTQ + adults from accessing public services and programs, such as those for substance abuse, housing, or veterans. Generating more visibility and awareness for pre-existing services that center older LGBTQ + adults is something that planners could do. Spatial service inventory profiles, for example, can be helpful for understanding where services are, how accessible they are, and where service gaps exist. Just as older adults generally participate in the community planning process (Micklow, Warner and Kinsella 2015), older LGBTQ + adults can benefit from and enjoy participating in LGBTQ + community and organizations (MAP and SAGE 2010). These findings raise questions for how planners might reflect older LGBTQ + adults’ community participation in the more mainstream planning process.
Informal care is an important service for older LGBTQ + adults, but it is also more difficult for them to access, compared to heterosexual cisgender adults (Choi and Meyer 2016). LGBTQ + older adults are actually more likely to be providing informal care than receiving it, according to Croghan, Moone and Olson (2014) data on 495 LGBTQ + older adults in the Twin Cities area of Minnesota. Given the disproportionate lack of access to care services, older LGBTQ + adults might feel more comfortable seeking non-LGBTQ + specific services should care service workers for older adults have culturally sensitive trainings, which advocacy organizations like SAGE provide to agencies across the country (SAGE 2020a). Porter and Krinsky (2014) studied the efficacy of LGBTQ + aging trainings for elder service providers at four training events in Massachusetts. Service-providers’ pre- and posttest surveys indicated a positive change with statistically significant improvement in providers’ attitudes, knowledge, and behavioral intention to challenge homophobic remarks. More curriculum, however is needed on transgender older adults. These findings show promise for institutional culture change.
A national needs assessment conducted by SAGE in 2004 revealed that older LGBTQ + adults are twice as likely to be single, twice as likely to be living alone, and less likely to have children to care for them (90%), compared to their non-LGBTQ + counterparts (20%) (Cook-Daniels 2004; MAP and SAGE 2010). Instead, older LGBTQ + adults tend to have “chosen family” (i.e. non-biological close friends), LGBTQ + community organizations, and religious groups to care for them. Studies on older lesbians, specifically, debunk myths of the “old lonely lesbian” by highlighting the strong networks of informal care that older lesbians have developed (Adelman 1986). More qualitative research is needed to understand how older people live and thrive outside of heteronormative networks, particularly lesbians and transgender people. Such knowledge and networks can have great potential for improving care services, social inclusion policies, and community plans.
It is not enough for planners to acknowledge how and when older LGBTQ + adults experience services differently. Planners need to consider how to redistribute power and neighborhood resources to develop and strengthen communities of care for older LGBTQ + people. Ranahan (2017) suggests more collaboration across healthcare, human service agencies, public leadership, and advocacy coalitions in order to develop more intersectional policies that respond to the complex needs of older adults who are also LGBTQ + . Intersectional policies might mean that we need to overlay “fair aging laws” on to existing “fair housing laws” to ensure that LGBTQ + older adults are equally protected. Integrating a feminist planning ethic (Hendler 2005) into planners’ practice could also strengthen caring relationships. Regional planners could follow the leads of regional equity activists by decentering single-issue, emergency responses and, instead, prioritize long-term mutual learning to improve social services for a heterogeneous public (Lawson 2007).
Housing & Economic Instability
Inclusive and affordable housing pose a major concern for people in the wider LGBTQ + community (Ahmed 2019; Baker et al. 2018; Barnes 2005; Forsyth 2011; Gieseking, 2020; Herek 2009; Hillier and Bunten 2021; Irazábal and Huerta 2015; Micklow and Warner 2014; Robinson 2020), but particularly for older LGBTQ + adults. In 2013, the Equal Rights Center conducted a nationwide “matched pair” telephone test to determine the extent of stigma that older LGBTQ + adults faced when searching for senior housing. When self-identified older LGB and heterosexual adults with similar personal and financial profiles reached out to the same senior housing communities, almost half (48%) of older LGB adults experienced adverse treatment in terms of availability of housing, pricing, financial incentives, amenities, or application requirements (Equal Rights Center 2014).
LGBTQ + -specific senior homes are opening across the country (e.g. Openhouse in San Francisco and the Triangle Square in West Hollywood), but many are not affordable for the disproportionately low incomes of older LGBTQ + adults (e.g. Choi and Meyer 2016; Forsyth 2011). Based on a collaborative report from the MAP and SAGE (2017), more LGBTQ + adults aged 50 and older live at or below 200% of the federal poverty level (33%) compared to their non-LGBTQ + counterparts (26%). While this demonstrates economic disadvantages among the general LGBTQ + community, subgroup differences illuminate even greater economic disparities among older LGBTQ + adults living at or below the 200% of the federal poverty level: 40% of African American LGBTQ + older adults, 40% of Hispanic LGBTQ + older adults, 47% of bisexual older men, 48% of bisexual older women, and 48% of transgender older adults (Emlet 2016; Fredriksen-Goldsen 2016; Kim et al. 2016). Still, the long wait lists for every development demonstrate a need for more subsidized housing specifically for this historically underserved age group.
Considering older women of all sexual orientations are twice as likely to live alone than men, single women with a median age of 78 account for 58% of households spending more than half of their income on rent (Curran 2017). The disproportionate poverty of older women, in general, worsens for lesbians. Goldberg (2009) studied the effects of discrimination for same-gender partners in employer-sponsored retirement plans and found that women in same-gender partnerships were disadvantaged. Female same-gender couples over 65 had, on average, $12,000 (20%) less than their heterosexual counterparts (Goldberg 2009).
Economic disparities are likely due to the gender wage gap, which is then severely compounded for same-gender female couples and worsens for women of color (American Association of University Women 2018). Goldberg (2009) also used data from the Survey of Consumer Finance and the American Community Survey (2005–06) to find that female same-gender couples tend to rely most on social security and other public benefit programs but receive less income from these benefits, compared to heterosexual and male same-gender couples. This finding suggests another rationale for older LGBTQ + adults working later in their lives, compared to their heterosexual counterparts.
Economic disparities affect savings and access to social programs that typically support older adults (Martinez 2015). LGBTQ + older adults who are not married, or whose partner died or retired prior to the legalization of same-gender marriage, may face additional economic challenges in accessing necessary programs (e.g. pensions, inheritance, veterans’ benefits, immigration benefits, spousal survivor and retirement benefits, social security benefits) (MAP and SAGE 2017). Espinoza (2014) also found that half (50%) of all single LGBTQ + older adults felt they will need to work well beyond retirement age, compared to only 36% of partnered LGBTQ + older adults and 27% of single non- LGBTQ + older people. In other words, older LGBTQ + adults’ cumulative disadvantage puts them at greater financial risk as they age, making inclusive housing more difficult to attain since it tends to come with such a high price tag (Cahill and South 2002; Forsyth 2011).
Planning for affordable and inclusive housing means dismantling discriminatory zoning policies and removing barriers to development proposals for LGBTQ + -specific housing. Based on two Supreme Court cases, Village of Belle Terre v. Boraas (1974) and Moore v. City of East Cleveland (1977), municipalities can broadly restrict the types of household arrangements such that “queering” the definition of “family” in the zoning code would advance protections and awareness of older LGBTQ + adults’ lived experiences. Shifting the limited definition of family (i.e. related by blood, marriage, or adoption) toward establishing a right of co-residence would be more compatible with contemporary rights to privacy in intimate associations, as argued by the Supreme Court (Oliveri 2016). Planners should create a taskforce to review how family is defined (SAGE and AARP 2021). Given older LGBTQ + adults’ high rates of familial rejection (40%) based on their LGBTQ + identity (Pew Research Center 2013) and low likelihood of children (90% for LGBTQ adults and 20% of non-LGBTQ adults) (Cook-Daniels 2004), a right of co-residence may disproportionately help older LGBTQ + adults and households because of the community's historic and contemporary focus on “chosen family,” complex kinship networks, and communal living.
In order to respond to the needs of a diversifying suburban population, planners must vary housing options by challenging exclusionary zoning ordinances for single-family houses (Micklow and Warner 2014; Warner, Homsy, and Morken 2017). Feminist planning scholars have long repudiated the American planner's preference for single-family detached houses as a production of patriarchal, capitalist dominance (Markusen 1980). Zones for single-family houses have regulated and continue to police communities of color and the kinship structure of residents (Frisch 2002). Scholars have argued that there is a “missing middle” housing structure whereby medium-density sparsely exists, compared to the detached single-family house and large apartment complexes, constituting not only a social harm but an environmental harm, as well (Wegmann 2020). In addition to developing more “middle” housing structures, scholars of social isolation (Barry et al. 2002) advocate for mixed-use zoning and decreased minimum lot sizes because affordable housing is a material condition necessary for social participation. Micklow and Warner (2014) suggest planners and local policymakers also permit more options to retrofit single-family houses.
Planning Policy Context
Planners are supposed to improve spaces and places that people inhabit, and understanding patterns of everyday life, including those of older LGBTQ + adults, is a critical part of the planning analysis (Frisch 2015). Federal and state legislation can structure urban environments and neighborhoods through funding guidelines (e.g. Community Development Block Grants), policies (e.g. Fair Housing Act), partnerships, and training procedures. As a parting blow from the Trump Administration in January, 2021, the Department of Health and Human Services (DHHS) passed legislation permitting social-service providers that receive government funds to discriminate based on SOGI. Five months later, the DHHS reversed the law, though the fragility of SOGI rights became clear (Lambda Legal 2021a). Over half the states in the U.S. still lack explicit protections in education, housing (See Figure 1), credit, and public accommodations, such as grocery stores or gas stations, based on SOGI (Movement Advancement Project 2020). The 2020 Supreme Court case Bostock v. Clayton County, Georgia granted the first federal protections based on SOGI, which is limited to workplace discrimination in businesses with 15 or more employees (Human Rights Campaign 2019; U.S. EEOC 2020). This ruling could have profound implications for the economic justice of the queer community, as well as relieving shame and stigma that discriminatory policies might cause.
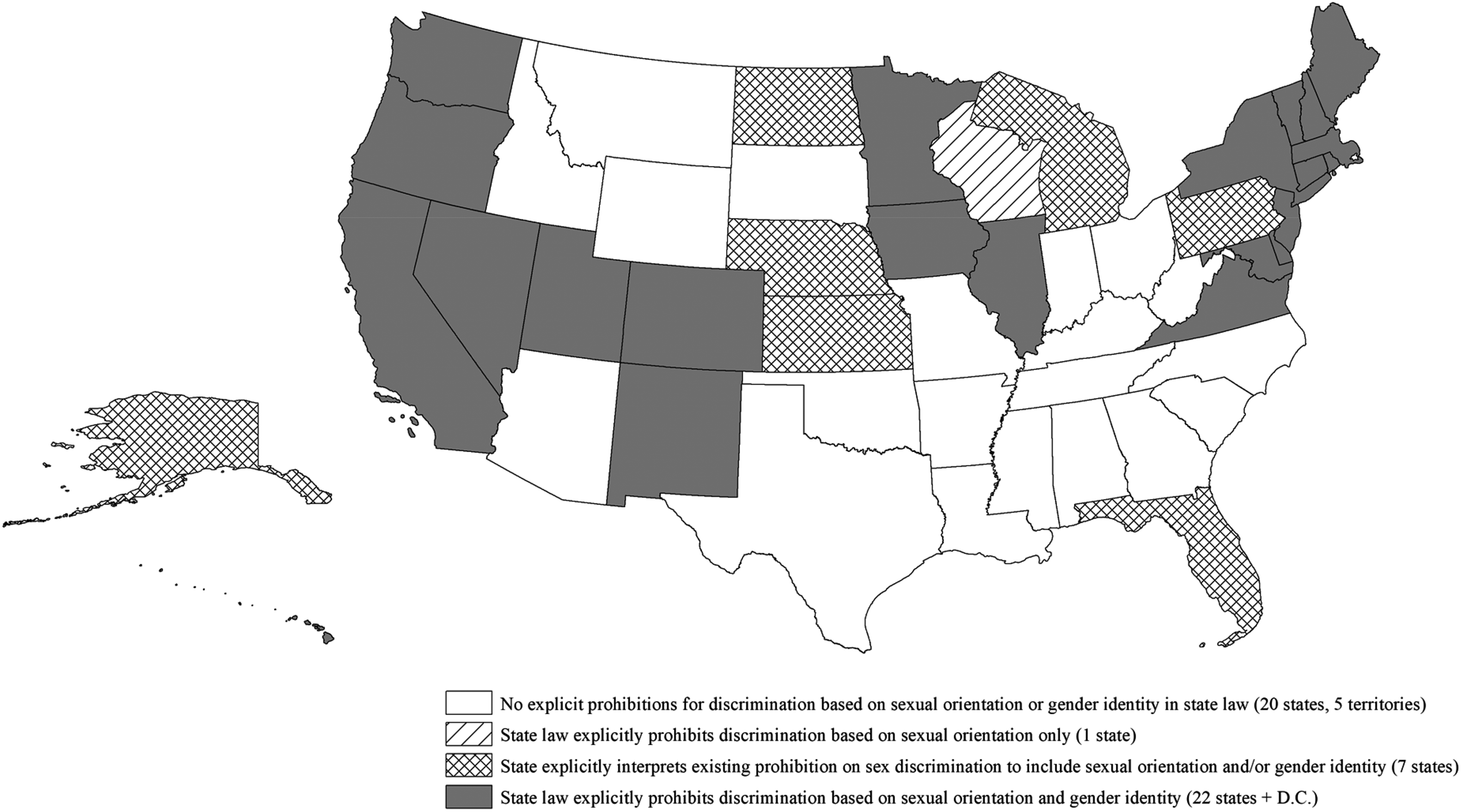
Map of housing nondiscrimination laws by states based on sexual orientation or gender identity (data source: Movement Advancement Project 2020).
President Biden issued an executive order that interprets the Bostock decision to mean that LGBTQ + people are also protected wherever federal law prohibits sex discrimination (i.e. health care, housing, and education) (Lambda Legal 2021b). Though the executive order might bring temporary relief, it is important to note that executive orders can change with a new administration and, as such, LGBTQ + advocates are still seeking a more permanent solution. The Biden-Harris administration has already rescinded the Trump administration's anti-diversity Executive Order (EO 13985), begun data collection of LGBTQ + people to improve care and treatment, and ended the Trump administration ban on transgender people serving openly in the military (EO 14004) (Medina and Santos 2021).
Though the Biden administration, as well as federal agencies, have issued orders toward greater equity for LGBTQ + people, state legislatures are granting the right to discriminate against LGBTQ + people in hospitals, homeless shelters, and nursing homes (Lambda Legal 2021a). Barely halfway through 2021, state legislatures across the country are enacting more anti-LGBTQ + bills into law this year than in the last three years combined (Ronan 2021). The National Organization of Black Lesbians on Aging has issued “an urgent call for local, state and federal governments to strengthen and reinforce policies and practices that work toward filling the gaps in the public's knowledge about lesbian aging and health and helps make visible the lived experiences of Black lesbians” (Woody 2015, 56). Planners’ advocacy for legal protection could increase the economic security, health, housing and safety of all LGBTQ + people, especially older LGBTQ + adults.
Legal protection, with accountability and enforcement measures, is essential for older LGBTQ + adults (Equal Rights Center 2014). The U.S. Department of Housing and Development (HUD) developed an “Equal Access Rule” to ensure that no owner, administrator, or lender of HUD housing could discriminate against people based on their actual or perceived sexual orientation, gender identity, or marital status (US HUD 2015). On February 11, 2021, HUD even issued a memorandum stating their interpretation of the Fair Housing Act (FHA) as prohibitive of discrimination on the basis of SOGI, directing both HUD offices and recipients of HUD funding to enforce the FHA as such. This important advancement moves toward protecting older LGBTQ + adults who seek government-subsidized housing, but implementation has been difficult. Emergency shelters and other group housing, for instance, have rarely implemented this rule for their own everyday practices (Hillier and Bunten 2021). Even with federal policies from Biden's executive order, we are now seeing how states’ legalization of discrimination dictates how, or whether, a state will protect their residents from discrimination on the basis of SOGI. Considering older adults are at higher risk of contracting COVID-19, explicit non-discrimination protections also need to apply to COVID-19 relief and aid (MAP, SAGE and the Center for American Progress 2020).
Planners should advocate to include “individuals isolated due to sexual orientation or gender identity” as a “greatest social need” group in the Older Americans Act (OAA) (LGBT Aging Center 2012; SAGE and AARP 2021). Although this designation does not require any network or service to consider older LGBTQ + adults as a group of greatest need, the policy builds awareness of older LGBTQ + adults’ unique challenges and can lead to greater financial support for older LGBTQ + adults, thereby mitigating housing and health issues (LGBT Aging Center 2012). Considering most states experience disparities in funding for both aging and LGBTQ + issues, the money to research individuals at the intersection of the two communities is particularly scarce, demonstrating the need for intersectional policies (Choi and Meyer 2016). Because funding is so sparse for the unique needs of older LGBTQ + adults, planners should apply for grants to develop more inclusion in services and the built environment, such as universal design (Warner, Homsy and Morken 2017), through the Administration for Community Living in the U.S. Department of Health and Human Services. Planners could also affect the housing stock available to older LGBTQ + adults by seeking grants from the US Department of Housing and Urban Development.
The OAA policy shift could also lead to more data collection, which state agency providers recommended for improving services (Choi and Meyer 2016). In 2017, the US Department of Health and Human Services eliminated questions about older LGBTQ + adults from two critical surveys, one of which measures services funded by the OAA (Singh, Durso, and Tax 2017). The Trump Administration continued to roll back data collection on LGBTQ + people who benefit from federal programs. Aging network representatives at a 2015 convening reported effective strategies for developing LGBTQ + -inclusive senior care (Choi and Meyer 2016). The Director of Georgia's Department of Human Services’ Division on Aging reported that the State “worked with service providers to establish a database of LGBT friendly providers, and updated intake materials [i.e. assessment forms] to include LGBT elements” (Choi and Meyer 2016). Integrating these questions into national surveys can make queer and trans communities visible (De Vries 2014; Hillier and Bunten 2021).
People disclosing their LGBTQ + identity, even for data collection, have and continue to pose serious risks such that people often choose to stay strategically silent to protect oneself (Foucault 1978; Halperin 1995). Frisch (2021), however, advocates for a queer reading of the U.S. Census in order to increase recognition, rights, and acceptance of LGBTQ + neighborhoods, communities, and status (Anacker and Morrow-Jones 2005; Brown and Knopp 2006; Doan 2019). Because the Census develops preliminary local data to inform planning analyses, asking SOGI questions on the U.S. Census can lead to more diverse services as well as more services specific and appropriate to the needs of older LGBTQ + adults (Redcay et al. 2019). Planning scholars must also ask SOGI questions to respondents in order to understand how planning can learn and respond to the needs of the LGBTQ + community. In addition to improved data collection, state agencies should train providers on LGBTQ + issues and encourage more sharing practices across municipalities and states (Choi and Meyer 2016).
Planners can be transformational leaders by collecting data, understanding and articulating the ways in which laws at every level positively or negatively affect older LGBTQ+ adults, and hearing stories in order to systemically implement plans and policies that integrate diverse voices (Turesky and Warner 2020). As Barbara Love notes in her theory for “Developing a Liberatory Consciousness” (2000), systems do not perpetuate themselves, people's actions do.
Queering A Plan for Aging
Scholarship in queer planning has pushed planners to move beyond mere acknowledgment and tolerance of the LGBTQ + population, demonstrating how the field can shape the lives and possibilities of a heterogeneous LGBTQ + community (Doan, 2010, 2015; Doan and Higgins 2011; Frisch 2002; Goh 2018). I have applied a theory of intersectionality to understand the unique needs and experiences of older LGBTQ + adults, which may vary based on the effects of other identities, such as race, gender, and class. My goal is to begin to highlight the heterogeneity of experiences among older LGBTQ + adults while also illuminating shared experiences upon which to build meaningfully inclusive coalitions. Sameness is not necessary to form group interests and, as Audre Lorde (1984) reminds us, celebrating the “creative function of difference” can create powerful connections and courage across communities. Older LGBTQ + adults have experiences and histories unique from older heterosexual adults, thus requiring planning policies that address their specific needs for places in which they live, work, and recreate (Doan 2015). The current literature demonstrates the need for planners to develop intersectional aging policies and plans that address social isolation and fear, economic and housing disparities, and service inaccessibility for LGBTQ + people as they age.
To plan for the diverse and shifting needs of older LGBTQ + adults, planners must integrate a framework of cumulative (dis)advantage (Carpenter 2010) into existing planning for aging analyses, which advocate for improvements to service delivery and the built environment (Warner, Homsy and Morken 2017). Developing inclusive improvements to the built environment and services can be costly, but planners can find the money and remedy the harms from cumulative disadvantage by advocating for redistribution through changes to local budgets. For example, police have long been a source of fear and violence for the LGBTQ + community (Boggs et al. 2017; Chauncey 1994; Cohen 1997; Delany 1999; Faderman 1991; Faderman and Timmons 2006; Fredriksen-Goldsen et al. 2011; Hanhardt 2013; Martinez 2015; Quinn 2019; Warner 2002; Winkle 2015). As many planning scholars have advocated (Dorries and Harjo 2020; Simpson, Steil, and Mehta 2020; Stein 2019), planners can promote sharp reductions to police and military budgets in order to increase budgets for inclusive services and the built environment, which would also reduce the exposure between law enforcement and potentially vulnerable people, both domestically and abroad.
Creating a more inclusive built environment for all physical abilities reflects older LGBTQ + adults’ higher risks of disability and mobility issues than heterosexual older adults (Fredriksen-Goldsen et al. 2011). Changing the built environment is critical to planning for aging populations through age-friendly building codes, inclusionary zoning, density bonuses, universal design, and land use policies that generate affordability and density, which can mitigate social isolation (Barry et al. 2002; Plouffe and Kalache 2010; Ramsey-Musolf 2017; Warner, Homsy and Morken 2017). In the short term, planners can facilitate community services and housing access to support older LGBTQ + adults through trauma-informed, LGBTQ + culturally sensitive provisions (MAP & SAGE, 2017; Agyeman and Erickson 2012; SAGE 2020b), and redirect funds specifically for LGBTQ + older adults’ livelihoods.
Older LGBTQ + adults are remarkably strong and resilient, having developed creative coping mechanisms for surviving and thriving amid hyper-surveillance and policing throughout much of their life course (Kia 2016). Aging and social services’ historic (and present) lack of support for the unique needs of LGBTQ + people indicate why older LGBTQ + adults do not look to public services, and people working for these institutions, for healing and support. In order to regain this community's trust, public service employees and planners should develop relationships with the local LGBTQ + grassroots activists, community centers, and social services to advance equity (Dubrow, Knopp and Brown 2015).
Beebeejaun (2017) suggests that inclusive possibilities outside of formal state spaces can reduce disparities in representation in leadership and political roles. Given the strength of the U.S. LGBTQ + community's history with collective action (Alexander 2005; Bell and Valentine 1995; Chauncey 1994; Cohen 1997; Cvetkovich 2003; D'Emilio 1992, 2002, 2012; D'Emilio & Freedman 1997; Enke 2007; Faderman 1991; Faderman and Timmons 2006; Hanhardt 2013; Katz 1992; Kenney 2001; Kennedy and Davis 1993; McKinney 2020; Meyerowitz 2002; Muñoz 2009; Quinn 2019; Spruce 2021; Stryker 2017; Snorton 2017; Warner 2002) and service provision (Knopp and Brown 2021; Schulman 2012), service development for the unique needs of older LGBTQ + adults in the U.S. could build on the strengths already in this community. Outside of the U.S., communities have been developing their own LGBTQ + politic to fit their cultural grammar in places such as China (Rofel 2007), Lebanon (Moussawi 2015) and South Africa (Tucker, 2009). Their collective organizing might also prove beneficial for developing and implementing LGBTQ + -inclusive aging services, internationally.
Fainstein (2013) warns that representation without political power, even from independent planners, requires political backing from social movements or progressive politicians. Collective action is necessary in the absence of representation (Meyer and Fine 2017) and older LGBTQ + adults are already mobilized. Older lesbians in OLOC and ZamiNobla, the National Organization of Black Lesbians on Aging, are creating their own spaces of care to meet their needs, not waiting for public institutions to make them visible (Raphael 2006). This activism within the LGBTQ + community may offer a care model that reduces isolation, stigma, loneliness, and stress (Lyons 2015), benefitting people of all ages and SOGI (Fredriksen-Goldsen 2016). Planners can build relationships with LGBTQ + movements by bringing together advocacy groups like SAGE with Area Agencies on Aging to address key service needs across their regions. Planners can also connect with SAGE to support a taskforce that would create an inclusive definition of family, which can have enormous implications for expanding access to affordable and inclusive housing, paid family leave, and family caregiving laws (SAGE and AARP 2021).
Planners might consider following the leads of, and collaborating with, older LGBTQ + leaders by asking them to serve on committees to create more culturally sensitive responses to aging and health (MAP and SAGE 2017). Beginning a dialogue (Forsyth 2011) and encouraging storytelling (Choi and Meyer 2016) can alleviate social isolation and regain the trust of this group. These participatory planning suggestions come with the caveat that planners may face challenges in gaining participation because many older LGBTQ + adults experience discomfort, fear, and even harm with disclosing their LGBTQ + identity in either formal state spaces or even at LGBTQ + centers with younger LGBTQ + people present (Boggs et al. 2017; Kia 2016). Representation can require a lot of work from a group that might have little capacity, so planners must also do their own work to enhance the capacity of older LGBTQ + adults to navigate aging, social, and health services.
Understanding this age cohort's struggle for recognition in the past, and the spaces that allowed for their thriving, can inform their current experiences and values. Planning's historic role in regulating and enforcing heterosexist (Frisch 2002) and ageist norms has been largely ignored in mainstream planning history, and so, too, have the histories of LGBTQ + people, particularly LGBTQ + people of color. Although the norms that planning generated have evolved over time, telling the same stories through everyday repetition can give a mask of permanence to them, thereby detrimentally affecting those who are not recognized, erased (Ahmed 2006; Foucault, 1971; Taylor 1992). Planners seeking justice for older LGBTQ + adults must also excavate “a local genealogy of QPoC [queer people of color] activism that continues to be excluded from the archives” (Bacchetta, El-Tayeb and Haritaworn 2015, 773). Dubrow (2012) considers the importance of preserving LGBTQ + history in the built environment through recognition of places of homophobia (e.g. mental institutions) and places of LGBTQ + liberation (e.g. The Compton's Cafeteria in San Francisco).
Planners can look to the U.S. National Park Service's LGBTQ Heritage Initiative (Springate 2016) as an example for future historic preservation initiatives centering LGBTQ + people, particularly those underrepresented within the LGBTQ + community. The NPS LGBTQ Heritage Initiative recognizes that preservation is a public act, with public funds, and thus must attend to “everyone's past” (Springate 2016, 02–12). They do so by (1) increasing the number of LGBTQ+ affiliated properties in the National Register of Historic Places; (2) identifying, documenting, and nominating LGBTQ + affiliated places as National Historic Landmarks; (3) engaging scholars and community members to identify, research and tell the stories of LGBTQ + places to preserve and nominate for recognition; and (4) encouraging NPS affiliates to interpret place-based LGBTQ + stories that preserve and celebrate LGBTQ + legacies for future generations. Historic preservation planning, in this way, can begin to remedy harms, preventing misrepresentation and erasure, as an act of archival justice (Rawson 2015) and restorative planning (Schweitzer 2016).
Studying the everyday lives of older LGBTQ + adults through a feminist lens of the right to the city (Lefebvre 1991) can show planners and policymakers how to advocate for and recognize everyday actions as a way to foster just cities (Fainstein 2013), democratic societies (Purcell 2014), spaces of hope (Harvey and Harvey 2000), or “redemptive possibilities,” (Beebeejaun 2017, 331). This proposition echoes queer theorists’ rejection of overarching, grand narratives and, instead, focuses on partial, locally-situated knowledges of everyday life to highlight the details of life-in-place that might be momentarily part of a collective reality (Bailey 1999; Browne & Nash, 2010; Haraway 1991).
In addition to practitioners, planning scholars play a central role for older LGBTQ + adults’ liberation. Parker (2016) suggests planning scholars look inward by shifting the dominant scholarship, which is steeped in racism and “cultural misrecognition” such that injustices manifest in representation, interpretation, and communication (Fraser 2013). Planning educators must diversify the professional field in terms of race (Thomas 2008) and other identities of difference (Agyeman and Erickson 2012). Educators also have the capacity to help students realize their heteronormative and ageist biases, values, and goals which may ultimately shape their capabilities for listening and understanding in community planning practice.
Defining and understanding differences within LGBTQ + communities can not only be a source of social justice in planning, but also a matter of survival for a significant part of planners’ communities. José Esteban Muñoz (2009), situated in queer feminist and queer of color critiques, envisions a queer utopian futurity, not with a focus on the present and a pragmatic gay agenda or identity, but with dreams of collectivity and difference. We must begin to conceptualize how to “queer” a plan for aging, while also being mindful that this is not a static group and that younger LGBTQ + people might have different needs and desires as they age. Planners have the capacity to provide opportunities for older LGBTQ + adults to thrive today and in the future, so it is critical for planners to understand how their policies, processes, and spaces may influence this group's well-being and healing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.