
Abstract
Many children with invisible chronic illnesses (ICIs) are living to adulthood, necessitating that they prepare for their future. Health care and education systems have different meanings and processes for transition, although both systems are designed to help young adults prepare for independence. As health care and educational services support and educate each child and the adult he or she will become, it makes sense for these systems to coordinate their services to improve student postschool outcomes. This article addresses the importance of coordination and collaboration between health care transition and education transition for youth with ICI. The authors present a model that may be used to guide the efforts to coordinate these two forms of transition along with recommending preliminary steps that can be taken to facilitate this merger.
Many children with chronic illnesses are now living into adulthood, necessitating that they and their families prepare for adulthood. Approximately 15% to 18% of all children have a chronic illness defined as a medical condition that lasts more than 3 months and impacts normal activities (University of Michigan Health System, 2011). Many students who appear healthy may have an invisible chronic illness (ICI) such as asthma, diabetes, cystic fibrosis, cancer, AIDS, and congenital heart problems (Grady, 2009). These students have a better chance of living into adulthood than in 1999. A comparison of census data (U.S. Census Bureau, 2011) for 1999 and 2007 shows death rates indicated the following decreases by disease—diabetes mellitus: 10%, chronic lower respiratory disease: 10%, cerebrovascular disease: 32%) cancer: 11%, and diseases of the heart: 28%. Students with ICI may be eligible for services under the Individuals With Disabilities Education Act of 2004 (IDEA, 2004) under “other health impaired” if (a) they have limited strength, vitality, or alertness and (b) their educational performance is negatively impacted (National Dissemination Center for Children With Disabilities, 2009). Students eligible for services under IDEA are required to have a transition Individualized Education Program (IEP) beginning when they turn 16 (IDEA). Alternately, some students with ICI may be eligible for services under Section 504 of the Rehabilitation Act of 1973 (Office of Civil Rights, 2002). Although students under a Section 504 Plan are not required to receive transition planning, accommodations and needed support services are covered. As the Section 504 Plan stays in effect in postsecondary settings, it can be used to assist students to identify and plan for their postschool outcomes (Office of Civil Rights, 2002; Repetto et al., 2006).
Historically, educators have worked toward education transition (ET), and health care providers have worked toward health care transition (HCT) but the word transition has very different meanings in the two fields (Blum, 1995; Will, 1984). Families have been left to straddle these two worlds that traditionally have not interacted to support students with ICI. Logically, this separation does not make sense: Health care and educational interests are integral parts of each child and the adult he or she will become. Yet, transition processes for teens with chronic illness have not evolved into an integrated system (Repetto, Gibson, Lubbers, Gritz, & Reiss, 2008b). It is important to bring ET and HCT together to help children with ICI grow up and develop the full range of life skills.
Beyond addressing the educational and medical needs of these students, a coordinated effort is important to the overall well-being of the adolescents and young adults who deal with their illness on a daily basis and at the same time have concerns about their future. In addition, as youth with chronic illness often do not “look” sick or disabled, they are often confronted by misunderstanding and judgment from others. The following quote from a young adult with ICI illustrates this issue.
The hardest part to deal with, for me, is not being sick; it is the suspicion and lack of understanding about disability from people in my community that is the most disturbing. For example, if I am feeling up to getting out of the house for a little while with one of my family members, I am chastised for being seen out, how I look, and what I’m doing. Many people are of the opinion that if I am well enough to be out, then I should go to school and function normally. People’s ignorance has been, and continues to be, the largest obstacle that I have to face. (Grady, 2009, p. 2)
This article addresses the importance of coordination and collaboration between HCT and ET for youth with ICI. The authors present a model that may be used to guide the efforts to coordinate these two forms of transition along with recommending preliminary steps that can be taken to facilitate this merger.
ET
Models of ET have been in existence since 1984 when the concept of transition was introduced as a federal initiative for students with disabilities (Will, 1984). The initial concept of transition was defined by the level of supports needed for students to successfully move from high school to employment. Subsequent models extended this concept to include preparation throughout elementary and secondary school for postsecondary life in the community, employment, and education (Brolin & Loyd, 2004; Halpern, 1985; Sitlington, Neubert, & Clark, 2010). In 1994, the Division of Career Development and Transition supported a broad view of transition by publishing this definition in its position paper on transition.
Transition refers to a change in status from behaving primarily as a student to assuming emergent adult roles in the community. These roles include employment, participating in post-secondary education, maintaining a home, becoming appropriately involved in the community, and experiencing satisfactory personal and social relationships. The process of enhancing transition involves the participation and coordination of school programs, adult agency services, and natural supports within the community. (Halpern, 1994, p. 117)
The IDEA of 1990, the IDEA Amendments of 1997, and the IDEA Improvement Act of 2004 mirror this broad definition of transition. Through this legislation transition, services are mandated to be offered to students with disabilities by age 16 addressing the areas of (a) instruction, (b) community experiences, (c) employment, (d) postsecondary living skills, (e) functional vocational evaluation, and (f) related services. Appropriate measurable postsecondary goals related to training, education, employment, and independent living along with needed transition services are required through the IEP.
As transition models, definitions, and legislations have evolved, researchers have studied research-based transition practices (Brolin, 1997; Halpern, 1993; Kohler, 1996; Patton, 1999; Test et al., 2009; Wehman, 1996). Many of these research-based practices could provide a formal structure for including HCT in ET. For example, Test et al. (2009) identified 16 evidence-based transition practices that were linked to improved student outcomes. Six of the identified effective practices (interagency collaboration, parental involvement, self-advocacy/self-determination, self-care/independent living, social skills, and student support) could be used to incorporate HCT into ET. In another study, Kohler (1996) developed the Taxonomy for Transition Programming covering five areas of (a) family involvement, (b) program structure, (c) interagency collaboration, (d) student development, and (e) student-focused planning all of which can include HCT components. A recent study by Landmark, Ju, and Zhang (2010) identified eight substantiated best practices in transition, all could be part of HCT, including (a) paid or unpaid work experience, (b) employment preparation, (c) family involvement, (d) general education inclusion, (e) social skills training, (f) daily living skills training, (g) self-determination training, and (h) community or agency collaboration.
Although HCT could theoretically be planned for within current educational transition models and programs, there is little if any evidence that this is occurring. A study of related services conducted as part of the National Longitudinal Transition Study indicated that although youth receive services for mental health and other health concerns, a majority of these services are offered outside of the school system. Only 53% of youth report having a school-based case manager to coordinate their services (Levine, Marder, & Wagner, 2004). A survey conducted by Repetto et al. (2008b) asked members of interagency transition teams questions related to their knowledge of HCT, and whether they felt it was an important topic to include in transition planning. A total of 44% of survey respondents were school personnel (e.g., teachers, administrators, school-based therapists, school-based health personnel), 39% were agency representatives (e.g., Vocational Rehabilitation, Centers for Independent Living, Division of Blind Services), with the remaining 17% of respondents comprised of family members, student representatives, and others. The majority of the respondents reported having never heard of or knowing a little about HCT. Even though most participants indicated little knowledge of HCT, 95% agreed that it was important to include health-related goals, issues, tasks, and concerns in transition IEPs. Survey participants were also asked to rate how often 16 HCT-related IEP goals were included in transition planning. Their ratings indicate that participants were able to link HCT to more generic transition IEP goals that are not HCT specific, while noting little inclusion HCT-specific transition IEP goals. Goals rated as most often included in transition planning that could be HCT related included (a) identifying and accessing agencies, (b) learning self-determination skills, (c) becoming independent in self-care, (d) improving interpersonal communication skills, (e) using transportation, and (f) completing job applications. Conversely, the HCT-related IEP goals rated as never or rarely being part of transition planning included (a) completing health forms and communicating with health care professions, (b) understanding health insurance, (c) maintaining personal health records, (d) knowing how to maintain overall good health, and (e) knowing when and how to access urgent medical care. The results of these studies indicate that HCT is not currently infused into school-based transition practices, although the need for the inclusion of HCT in transition planning is supported. The increased number of students with ICI in our school systems makes this need even more compelling. If students with ICI are not able to manage their health needs, they will not be successful in postsecondary education or employment making HCT planning a crucial component of their education.
HCT
HCT is the process through which young adults are taught to move from child-centered (pediatric) to adult-oriented health care. Most HCT activities focus on ensuring that the teen with chronic illness is able and ready to take on tasks related to caring for his or her condition (e.g., taking medications, ordering refills, telling someone about the condition, making medical appointments). The field of HCT for chronically ill teens is relatively new. In 1993, Rosen noted a lack of official transition policies, citing the American Academy of Pediatrics statement that care by pediatricians might extend beyond the age of 21, based on patient needs. By 2002, Reiss and Gibson identified policy recommendations for both families and health care professionals. These included having a future orientation, flexibility of timing in moving to adult health care, gradually increasing responsibility in self-management of health care needs, development of a transition plan, and celebration of transition. The “Consensus Statement on Health Care Transitions for Young Adults With Special Health Care Needs,” jointly developed by the American Academy of Physicians and the American Association of Pediatrics (2002), established a foundation for HCT. Guidelines included in the report recommend that (a) all children have continuity of care between pediatric and adult health care, with a physician explicitly responsible for facilitating the HCT process, (b) medical students and physicians be trained in the knowledge and skills necessary to develop an individualized HCT plan, (c) a medical summary be prepared, and (d) continuous health insurance be available.
Clinicians, researchers, and policy writers have continued to assess HCT needs and to propose specific approaches to providing services (Callahan, Winizer, & Keenan, 2001; Felden et al., 2006; Flume, Taylor, Anderson, Gray, & Turner, 2004; Freed & Hudson, 2006; Scal & Ireland, 2005). However, few universally applicable models for implementation of HCT have been proposed. This is in large part because each pediatric and adult setting, and each health condition, present unique challenges. The absence of a legal mandate for HCT also contributes to the lack of standardization in HCT. Although there is no legal mandate for transition, there is promise in the movement toward enhancing transition systems of care with the addition of a transition outcome measure to the Healthy People 2020 public health campaign (Healthy People 2020: Topics and Objectives; Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services, 2010). Previously under the Healthy People 2010 initiative, HCT was mentioned in passing as part of outcome measure 16-23, which addressed increasing the proportion of states that had services systems for children with special health care needs. Now under Healthy People 2020, HCT planning is included as an individual outcome measure—DH-5: Increase the proportion of youth with special health care needs whose health care provider has discussed transition planning from pediatric to adult health care.
In the struggle to meet the health care needs of young adults with chronic illness, clinicians and policy experts have remained focused almost exclusively on the health-related skills that teens should acquire prior to transitioning to adulthood. Although employment or continued education are considered important aspects of adulthood (Ferguson, 2010; Freyer, 2010; Lotstein, Inkelas, Hays, Halfon, & Brook, 2008; Treadwell, Telfair, Gibson, Johnson, & Osunkwo, 2010; Wong et al., 2010), health care is considered the priority, and the focus of most HCT programs are the illness-specific self-care skills needed to be learned by the teen. The implication, rarely stated, is that it is only if young adults take care of their health needs that they will be able to function in other adult roles. The life skills necessary to achieve these secondary goals, or the resources that would help with ET goals, however, are rarely included in HCT efforts. A few authors (Bowes, Sinnema, Suris, & Buhlmann, 1995; Jackson, 2003; Landau, 1995), notably all from countries other than the United States, acknowledge the theoretic importance of vocation, sexuality, and family life in adulthood, but only Landau (1995) mentioned the importance of involving school personnel in preparation for adulthood. This recommendation is limited to the school nurse, continuing the exclusive focus on health, without involving other educational personnel. The majority of health care professionals assume that the word transition applies solely to HCT and are unaware that a similar process occurs in education. The HCT literature does not address the possibility that health care professionals and education professionals might work together to prepare a teenager with chronic illness for adulthood.
The Education–HCT (E-HCT) Model
Development of E-HCT
We advocate the merger of ET and HCT to (a) decrease duplication of effort and cost, (b) increase empowerment of teens and families as they experience the process of becoming an adult in a unified process, (c) increase support for students through the collaboration of health and education professionals, and (d) increase creativity in problem-solving through the synergy of education and health professionals working together. We expect such a merger will, in turn, lead to improved outcomes for youth and young adults with chronic illness. The issue is how best to develop an effective system to integrate these processes.
ET already has identified research-based practices (Kohler, 1996; Test et al., 2009) offering a base for including HCT in the ET process. Therefore, it seems logical to begin building this merger in ET by expanding current research-based practices to include HCT. Expanding educational transition to incorporate HCT will encourage collaboration between the two fields eventually expanding the focus of HCT to address the impact of illness on educational, vocational, recreational, and social adult roles. In this article, we introduce the E-HCT Model, a conceptual model for incorporating HCT into ET. It is important to note that the E-HCT Model does not yet have empirical support and thereby represents an initial base for continued and expanded study.
The E-HCT Model was developed by the Interdisciplinary Collaborative on Healthcare and Education Transition (ICHET), which has been focusing on this issue for the past 4 years through biweekly meetings, teaching an online E-HCT graduate course, publishing related journal articles, impacting policy development, writing grant proposals, and giving national presentations. The members of ICHET are interdisciplinary, including a physician, parent, medical social worker, child health policy expert, and a college of education professor. The mission of ICHET is as follows:
To enhance service, provide training and conduct research to support the successful, comprehensive transition of youth and young adults with special health care needs from pediatric to adult-oriented health care; from school to higher education and employment; and from adolescence to adulthood and the ongoing pursuit of dreams and ambitions.
The E-HCT Model is similar to other conceptual models of transition. The difference lies in “maintenance of health for positive outcomes in adulthood” as the central focus of the model (see Figure 1). This focus is intended to support the outcome foci of postsecondary education, community, family, leisure, and employment found in other transition models by ensuring adults remain healthy to be successful in all areas. It is for this reason that E-HCT is viewed as an overlay model to established transition models extending rather than supplanting current effective practices. The following discussion of the E-HCT Model components includes needed extensions (see Table 1).

Education–Health Care Transition Model
The E-HCT Model Components
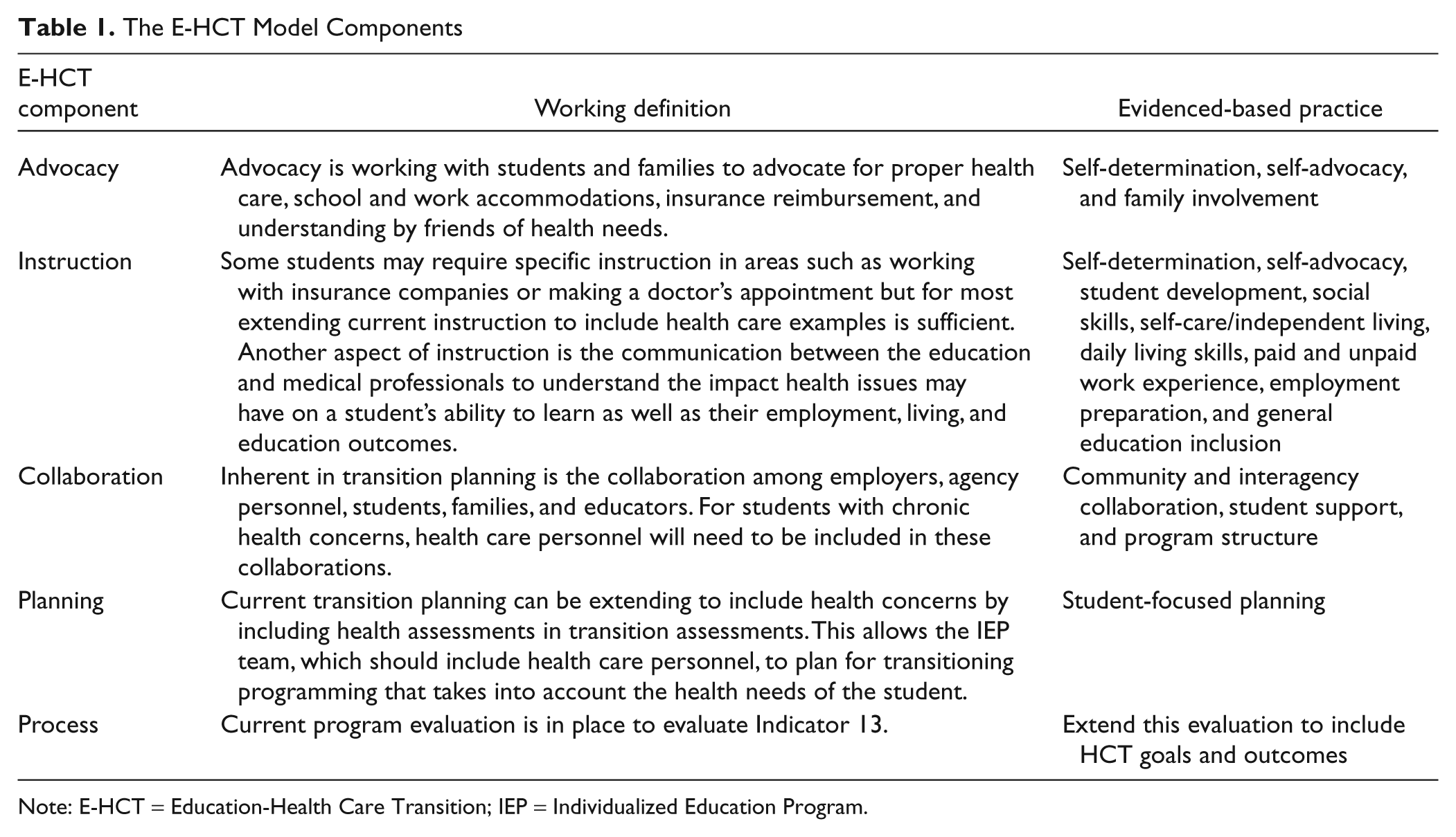
Note: E-HCT = Education-Health Care Transition; IEP = Individualized Education Program.
Advocacy
Advocacy not only involves working with students and families to advocate for proper school and work accommodations and social supports but also includes such advocacy activities as locating adequate insurance coverage, assistance navigating the health care system asking the doctor questions during medical visits, and the ability to call one’s physician when having increased symptoms. This requires the extension of the evidence-based practices such as self-determination and self-advocacy (Landmark et al., 2010; Test et al., 2009) to include health-related concerns.
Instruction
The goal for all youth with ICI should be that they have adequate health literacy, and this can be accomplished within our E-HCT framework. Health literacy is defined as, “The degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (Office of Disease Prevention and Health Promotion, 2010, p. 20). Students may require specific instruction in areas such as working with insurance companies or making doctor appointments, but for the most part, extending current instruction to include health-related needs is sufficient. For example, mathematics skills of probability can be used to help a teen learn to weigh the risks and benefits of a recommended treatment or medication. English skills can focus on reading handouts related to instructions for cleaning medical equipment or completing forms to obtain insurance. Students can use anatomy and physiology classes to better understand their illnesses. As indicated in Table 2, the instruction component includes many evidence-based transition practice such as learning social skills, daily living skills, and ways to adapt learning and work to ensure successful postschool outcomes.
Extending the Taxonomy of Transition Planning to Include Health Care
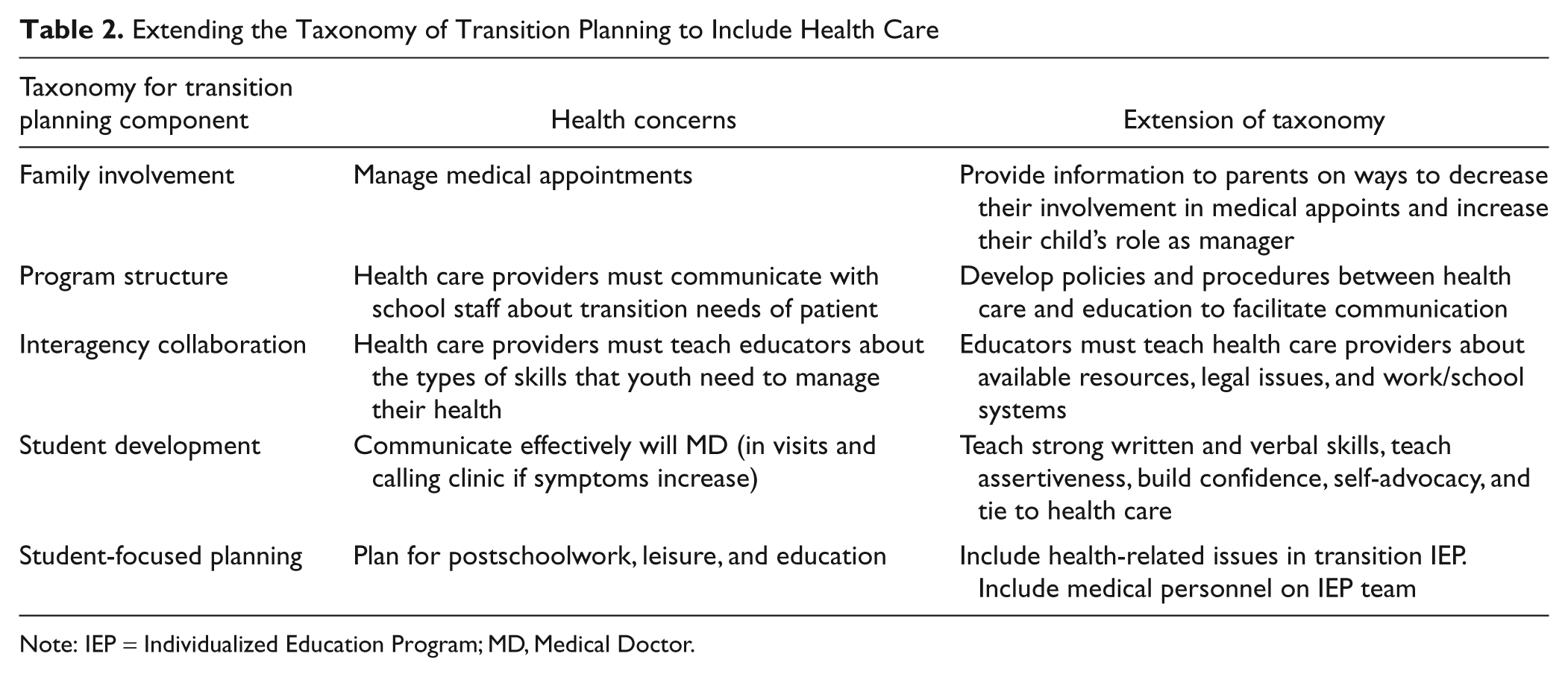
Note: IEP = Individualized Education Program; MD, Medical Doctor.
Instruction can also relate to the training of education professionals to better understand the impact health issues may have on a student’s ability to learn. For example, a student with cystic fibrosis will have periodic pulmonary exacerbations and will be absent from school. Students with diabetes may need to miss class due to high or low blood sugars, and teens with kidney disease may become fatigued and need to rest during class. Understanding the cause of the absences and working out ways to accommodate them prior to a symptom exacerbation will facilitate continued student learning. Conversely, education professionals can instruct health care professionals on the education and vocational resources available to help teens prepare for their futures. Health care professionals can, in turn, incorporate these resources, and the skills necessary to use them, into HCT efforts.
Collaboration
Inherent in ET planning is the collaboration among employers, agency personnel, students, families, and educators. For students with chronic health concerns, health care personnel will need to be included in these collaborations. Communication concerning health-related needs is critical to planning a student’s educational and transition program. Extending current partners to include health care personnel requires an understanding of the confidentiality mandates each discipline operates within. Essential for collaboration is the development of guidelines on how to monitor and address confidentiality mandates (Repetto, Gibson, Lubbers, Gritz, & Reiss, 2008a) and recommendations on how to manage the different modes of communication (terminology, acronyms, paradigms) of the two professions.
Each profession will need to educate the other on the roles and availability of various health care and education personnel along with the best methods of communicating. We believe that identifying one member of the health care team (e.g., nurse or social worker) and one individual from the school (e.g., teacher, school nurse, transition coordinator, or guidance counselor) for each transitioning student is most likely to succeed. The health care representative can attend the school transition IEP meeting (by phone or Skype, if necessary). The school representative can be invited to attend a clinic visit, to understand the full ramifications of the student’s illness and the treatment implication. If this is not possible, a phone conversation with the health care representative may suffice. At a minimum, school and health care personnel should share their written plans and goals, through mutually developed planning forms.
Planning
Current transition planning can be extended to include health concerns by including identification of health needs as part of the ET assessments. This allows the IEP team, which should include health care personnel, to plan for transitioning programming that takes into account the health needs of the student. Health care professionals can assist not only with the future health care needs of the student but also with information on how these needs may impact the students work/education and the accommodations that will be required. For this component of the E-HCT Model to be successful, all members on the IEP team need to have working knowledge of the terms used by the various disciplines. First and foremost is the understanding that “transition” has very different meanings to health care and education professionals. For example, a HCT goal might be to educate students about skills needed to maintain health. In ET, this goal might be to learn skills for optimal educational and vocational success. A merged E-HCT goal might be to learn the skills needed to maintain health for optimal educational and vocational success. Specific steps toward this goal would then be elucidated (e.g., learn underlying physiology of illness, identify how medications help, initiate call to pharmacy for refills). School and health care personnel would each work on these activities from their own perspective, or tasks could be divided between school and health care personnel.
Process
The E-HCT Model provides for ongoing process evaluation, including ongoing professional development and implementation oversight. Each district will need to establish their own process for the inclusion of E-HCT in current district transition practices and assessments.
Application of E-HCT
One way educators can view the application of the E-HCT Model is as an extension of the transition programming components that have been established as key to positive postschool outcomes (Kohler, 1996; Test et al., 2009). Building on the work of Kohler (1996) and Test et al. (2009) ensures that the E-HCT is an extension of evidence-based practices contributing to positive student outcomes. The additional health-related components have been identified through literature reviews, data from a HCT survey (Repetto et al., 2008b), and expert opinion, as provided by ICHET members. Table 2 illustrates the extension of transition programming to facilitate E-HCT. The additional health-related components are incorporated into transition programming along with the current components of the Taxonomy for Transition Programming (Kohler, 1996). For example, listed under Student-Focused Planning are several competencies identifying areas of IEP goal setting, including postsecondary education or training, vocational, community-related and residential, recreation and leisure, and educational programs. In the E-HCT Model, an added component to IEP goal setting is medically related IEP goals. Another example is extending the current planning team to include medical personnel on the IEP team. In this manner, HCT needs are infused into the established school-based transition programming.
Next Steps
Education Policy Implications
Policy experts, educators, health professionals, researchers, and funding agencies must begin to recognize the importance of integrating ET and HCT, thus taking steps toward merging these two processes. Many of the potential barriers to this merger (Reiss & Gibson, 2002; Repetto et al., 2008a; Repetto et al., 2008b; Rosen, 1995) can be addressed through the clarification and expansion of current transition practices (see Table 3). The following are examples of how these barriers might be addressed under current systems and mandates.
Barriers to HCT Along With Solutions
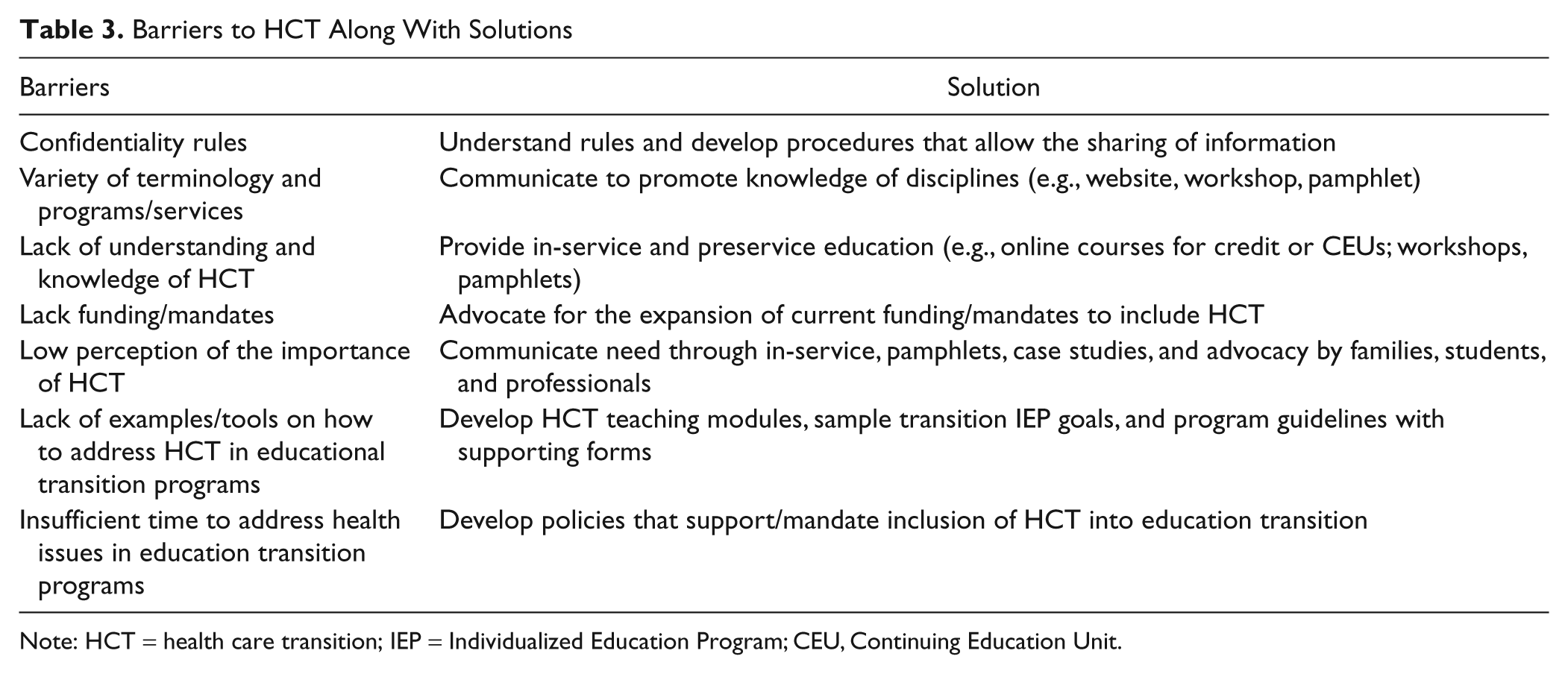
Note: HCT = health care transition; IEP = Individualized Education Program; CEU, Continuing Education Unit.
Clarify mandates
Under current law, students served by IEPs, many having ICI, are mandated to receive transition planning and services from age 16. Administrators need to clarify that transition planning can and should include planning for transition outcomes related to the health needs of these students.
Develop confidentiality guidelines
One crucial initial issue that needs to be addressed is confidentiality (Repetto et al., 2008a). The ability of health care workers to communicate with educators is governed by The Health Insurance Portability and Accountability Act of 1996 (HIPPA, 2001), while educators operate under The Family Education Rights and Privacy Act of 1974 (FERPA) and IDEA (2004). Each of these mandates has different applications and consequences that both disciplines need to understand to communicate freely about student needs. Guidelines have been developed by the U.S. Department of Health and Human Services and U.S. Department of Education (2008) to assist local school systems and health care professions to develop a set of procedures unique to their programs.
Provide staff development
One identified barrier is the lack of understanding, information, and general knowledge on HCT. Administrators could provide this information through a series of in-services, a website, newsletters, or fact sheets. Topics needing to be addressed include the following:
Privacy concerns: Outline ways health care workers and educators work together under current confidentiality mandates (e.g., obtain permission to share information protected by privacy laws with health care providers).
Define ICI: Describe what ICI is and how it impacts students. Discuss the needs of these students and strategies to meet them.
Define HCT: Define HCT and how it impacts the lives and instruction of students with ICI.
Collaboration: Provide guidelines for working with families, educators, and health care workers to meet the HCT needs of students. Teachers should be able to identify specific HCT activities for each learner. Activities may include, but are not limited to, identifying appropriate contact person on health care team, including health care providers in IEP meetings, and scheduling periodic update meetings or phone calls.
Curriculum development: Develop educational strategies for incorporating HCT into current curriculum in a manner that retains student confidentiality.
Extension of IEP planning: Provide examples of IEP goals that expand transition IEP planning to address the health needs of students who have ICI.
In addition to these changes, administrative support for the expansion of transition to include HCT needs to be evident in schools. This can be shown by providing time for educators and health care workers to collaborate, offering staff development on the topic and addressing concerns that may arise. Perhaps most important is fostering a school culture that accepts and values HCT, and understands the need to assist youth with ICI in planning for positive postschool outcomes.
Ongoing Model Development
The proposed E-HCT Model constitutes preliminary work that has not yet been verified by research. The model reflects concepts that will need to be further studied. In an ongoing effort to improve E-HCT, the ICHET members plan to develop and pilot individual components of the E-HCT model, as described below. In addition, efforts will continue to be taken through presentations, articles, and course works to increase awareness nationally of the benefits of an integrated education and HCT process.
In a first step in assessing, implementing, and evaluating the E-HCT Model, we plan to conduct focus groups of health care professionals, education professionals, and families to identify all barriers within the four elements (advocacy, instruction, collaboration, and planning), of the model. Second, we will outline proposed solutions, based on focus group suggestions, ICHET members’ ideas, and the opinions of additional national experts. These solutions will be organized according to the four elements of the model. Third, we will develop and field test instructional modules for health care and school professionals to implement the E-HCT Model components in a concrete and practical manner. It is anticipated that these materials will include clear descriptions of the confidentiality laws for each professions and how to work within these mandates (e.g., releases of information); information sheets with a summary of the knowledge sets, perspectives, and conceptualization of transition held by each profession; descriptions of curriculum activities that could enhance skills necessary to navigate the health care system; and collaborative checklists for professionals working in both ET and HCT.
Additional research is needed to address the following questions: “How does having an ICI impact postsecondary outcomes, including employment, education, health care, and social life?” “What types of accommodations need to be available in postsecondary setting to support individuals with ICI?” “How can we best train medical and education personnel in E-HCT?” “How does having an ICI impact future planning?” and “What are the stories of individuals with ICI transitions into adulthood?”
Summary
At present, ET and HCT operate in separate spheres. This is a false dichotomy, and to best prepare youth with ICI for gratifying and productive lives, it is important to integrate these two processes. This is a crucial area impacting the lives of future adults with chronic illness. ICHET is moving forward to validate and field test the E-HCT Model. In the meantime, even small steps (e.g., encouraging communication, providing in-service) can advance this cause immensely. In many ways, the framework for the E-HCT Model is already in place with current evidence-based secondary transition programming, and simply expanding these services to include planning for the health needs of youth with ICI will improve the postschool outcomes of these students.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.