
Abstract
Violence against women has been recognized as both a major public health problem and a human rights violation worldwide. Research has documented the association between physical/sexual intimate partner violence (IPV) and mental health, measured by the 12-item General Health Questionnaire (GHQ-12) among women in reproductive age. This study underlines that different types of IPV is independently associated with mental health status. Results also show effects of IPV on mental health may not only be immediate but also be long term. These findings suggest that efforts to identify women with mental health problems should include screening for the types and history of IPV victimization.
Background
Although much less attention has been paid to mental health globally, increasing attention has been focused on the women’s mental health problems in the past decade. Mental health problems are contributing factors to the global burden of disease and disability (Prince et al., 2007). As reproductive capacity forms a central part of women’s identity in most societies, higher risks for mental health problems among women have been attributed to their reproductive roles and gender disadvantages (WHO & UNFPA, 2009). The mental health status of a mother has been closely linked with healthiness and wellness of her children. Recent available data indicated that malnutrition, low birth weight, and other developmental problems are associated with an increased risk of children’s health whose mothers suffer from mental disorders (Harpham, Huttly, De Silva, & Abramsky, 2005; Patel & Prince, 2006; Walker et al., 2007).
Intimate partner violence (IPV) is another important issue associated with gender-based violence. Although gender-based violence has long been seen as a private family matter in many countries (Andersson et al., 2010; Gracia & Herrero, 2007), in the past few years it has been recognized as both a public health problem and a human rights violation (Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008; Jewkes, Levin, & Penn-Kekana, 2002; Kishor & Johnson, 2006; Koenig, Stephenson, Ahmed, Jejeebhoy, & Campbell, 2006). However, the global health burden from violence against women in reproductive age group is about 9.5 million disability-adjusted life years (DALYs; The World Bank, 1993). It has been increasing in most countries in the world (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006; Tokuç, Ekuklu, & Avcioglu, 2010; United Nations, 1996).
Not only is IPV a substantial health problem by virtue of its direct effects, such as physical and sexual, but it also might contribute to the overall burden of disease as a risk factor for women’s mental health problems. Recent studies have consistently shown a significant association between IPV and mental health outcomes in women, including various physical and chronic conditions and poor self-rated health (Ellsberg et al., 2008; Howard, Trevillion, & Davies, 2010; Ishida, Stupp, Melian, Serbanescu, & Goodwin, 2010; Patel et al., 2006; Pillai, Andrews, & Patel, 2008).
Research on the mental health effects of IPV has been constrained by several factors. Most studies have been undertaken on clinical rather than population-based samples, mainly in Western and developed countries. Furthermore, many studies have had small sample sizes, and consequences of IPV on the mental health of women have not been measured consistently in those studies (Ellsberg, Heise, Peña, Agurto, & Winkvist, 2001; United Nations, 2006).
The purpose of this population-based study is to describe the prevalence and impact of separate effects of physical and sexual IPV on women’s mental health in a representative sample of reproductive age (15-49 years) in a developing-country setting.
Method
Data
This cross-sectional survey was conducted in Sivas city center, Turkey, between September 2009 and April 2010. Sivas is a semirural province situated in the Middle Anatolia, with a population of about 700,000. The socioeconomical level of the city is average compared with other cities of the country. There are significant disparities in the socioeconomic characteristics between the quarters of the city. The population aged 15 to 49 years in the city center was 86,419 (TUIK, Turkish Statistical Institute, 2007).
Study Design and Setting
The sample size was determined as 2,246 individuals. This is large enough to estimate an expected prevalence of IPV of 40% (see, for example, Tokuç et al., 2010) from a large population with a margin of error for a 95% confidence interval of ±2%. Target population of the study comprises about 38,000 households in the 63 quarters. A multistage cluster sampling scheme was used for the selection of the survey sample. A sampling frame was prepared by making a list of quarters by number of households. (The households in each quarter were determined by using the records of the electricity company.) The number of households drawn from each quarter was determined in proportion to the population size of quarters from the list. A total of 11 quarters (as cluster) were selected randomly. The starting point for each quarter was randomly selected street and dwelling number. Nonresidential (e.g., commercial) and/or temporary residential properties (e.g., hotels) were excluded. In visited dwellings with more than one eligible respondent, one woman was randomly selected for the interview. If the woman selected was available, consent was sought and an interview arranged. A minimum of three return visits were made to each household at different times on different days to maximize the chance of obtaining an interview. It was explained to women that their participation in the study would be completely voluntary and that all information obtained would be kept confidential. After written and verbal consent to participate were obtained, the interview was conducted in a quiet room in each house. Face-to-face interviews were performed by eight trained final-year medical students. The study was approved by the Human Research Ethics Committee of Cumhuriyet University.
Survey Instrument
The proposed content of the questionnaire was reviewed by three research experts for face validity, and it was piloted with 10 women to judge the time needed for administration and to test for clarity and logical flow. There were two sections in the questionnaire. The first section requested details of the participant’s demographic information, such as age, education level, number of persons living in household, current marital status, employment status, smoking, alcohol consumption, the place where they had spent the majority of their life, and if they had any type of health insurance, a brief medical history (types of illnesses), perceived health status, and income level. The annual income level was self-reported as 1 (<US$10,000), 2 (US$10,000-US$20,000) and 3 (>US$20,000). Health-related problems were also coded as 1 = presence or 0 = absence.
In the second section, the questionnaire included the IPV questions adapted from scales used in other studies, such as the World Health Organization (WHO) Multi-Country Study on Women’s Health and Life Events (WHO, 2003).
Measures of IPV
In this survey, detailed information about the different types of violence (physical, sexual, and emotional) was obtained. The violence items were adapted from the Conflict Tactic Scales-2, which have been widely used in demographic and reproductive health surveys across cultures (Straus, Hamby, Boney-McCoy, & Sugarman, 1996). Each type of violence consisted of the acts was described below.
For physical violence, women were asked whether a current or former partner had ever slapped her or thrown something at her that could hurt her; pushed or shoved her; hit her with a fist or something else that could hurt; kicked, dragged, or beaten her up; choked or burnt her on purpose; threatened her with, or actually used, a gun, knife, or other weapon against her.
Sexual violence was defined by the following three behaviors: being physically forced to have sexual intercourse against her will; having sexual intercourse because she was afraid of what her partner might do; being forced to do something sexual she found degrading or humiliating.
Emotional violence included verbal attacks (insults, humiliations), control and power (isolation from family and friends, impeding decision making, economic abandonment), pursuit, harassment, and verbal threats.
Thus, the questions in the current study covered emotional, physical, and sexual violence. These questions had three possible responses: “many times,” “sometimes,” and “never.” A woman was considered to have ever experienced lifetime physical IPV if she answered “many times” or “sometimes” to any of the questions about physical IPV, and the same applied to emotional and sexual abuse. To examine whether the mental health consequences of IPV are immediate, long lasting, or both, two mutually exclusive time frames were used: within the previous 12 months (current) and more than 12 months ago (past).
Measures of Mental Health
The study included two mental health indicators: emotional disorder and self-perceived health status. Emotional health status was assessed with the 12-item General Health Questionnaire (GHQ-12; Goldberg, 1972). This short-form screening instrument has been validated in different countries and contexts (Goldberg et al., 1997; Piccinelli & Simon, 1997), including Turkey (Kılıç, 1996), and it has also been used in studies on the impact of IPV on women’s health (Romito, Molzan, & De Marchi, 2005). It covers anxiety, depression, and self-esteem, as experienced in the past month. This instrument is widely used to screen for mental health problems in nonpsychiatric services, and its application in research settings as a screening tool is well documented. The answers of participants were scored according to Goldberg’s original scoring method. In this method, response categories scores were 0, 0, 1, and 1, respectively. This gives scores ranging from 0 to 12. The total score was determined by adding the score obtained for each answer in the questionnaire. Scores of 4 and above based on the GHQ-12 guidelines were considered as positive for emotional disorders.
The survey included two widely used self-report health questions to asses self-perceived health status (Bowling, 2005). The presence of a limiting long-term illness was assessed by the following question: “Do you have any long-term illness, health problem or disability which limits your daily activities or the work you can do?” Finally, self-perceived health was also assessed with the following question: “How would you say your current health status is, compared with your health status last year?” The response options were “better,” “the same,” and “worse.” This measure that reflects both physical and mental health has widely accepted validity and a demonstrated association with morbidity and mortality (Kyffin, Goldacre, & Gill, 2004).
Statistical Analysis
Data were analyzed using Statistical Package of Social Science (SPSS Inc., Chicago, IL) for Windows version 16.0. Quantitative data were presented as mean ± standard deviation (SD). Categorical data were expressed as percentages. Prevalence for the different lifetime IPV categories and for current and past IPV in our sample was first calculated. Differences between IPV and mental health indicators were assessed using chi-square test. The association between each type of current and lifetime IPV (physical, sexual) and potentially overlapping risk factors for mental health problems: Women’s socioeconomic status, marital status, level of education, annual household income, employment, number of person living in household, having health-related problems, and whether they are victims of IPV were investigated using logistic regression analysis. Mental health indicators by types of IPV experienced in the past 12 months and more than 12 months ago were also assessed. The model fit used in the study was evaluated by R2 values. A p value of <.05 was considered statistically significant.
Results
Demographic Characteristics
Among the initial sample of 2,246, 17 did not fit the inclusion criteria. A further 326 declined to participate (mainly arguing that they did not have time to complete the interview), whereas 59 could not be contacted at their home and 1,844 agreed to be interviewed and gave informed consent. The mean age of the sample was 31.3 (SD = 9.8) years. The 1,844 (85.0% response rate) women completed the questionnaire.
About one third (32.9%) of the participants were in 15 to 24 age group, and 13.0% of them were above 44 years old. Table 1 presents the demographic characteristics of the sample. Most of the women did not have a university degree (71.6%), and more than half of them (54.0%) lived with 1 to 4 persons. Most respondents had health insurance (85.4%, including those with the Greencard which is given to poor persons by the Health Ministry of Turkey for health insurance). In the year prior to the survey, 62.5% of women were married, and 66.2% of women had a household annual income equal or more than US$10,000. More than one fourth of them were employed (26.1%). The rates of current smoking and regular alcohol consumption were 6.3% and 1.8%, respectively.
Baseline Characteristics of the Participants as They Exposed to Intimate Partner Violence or Not, and Total Sample
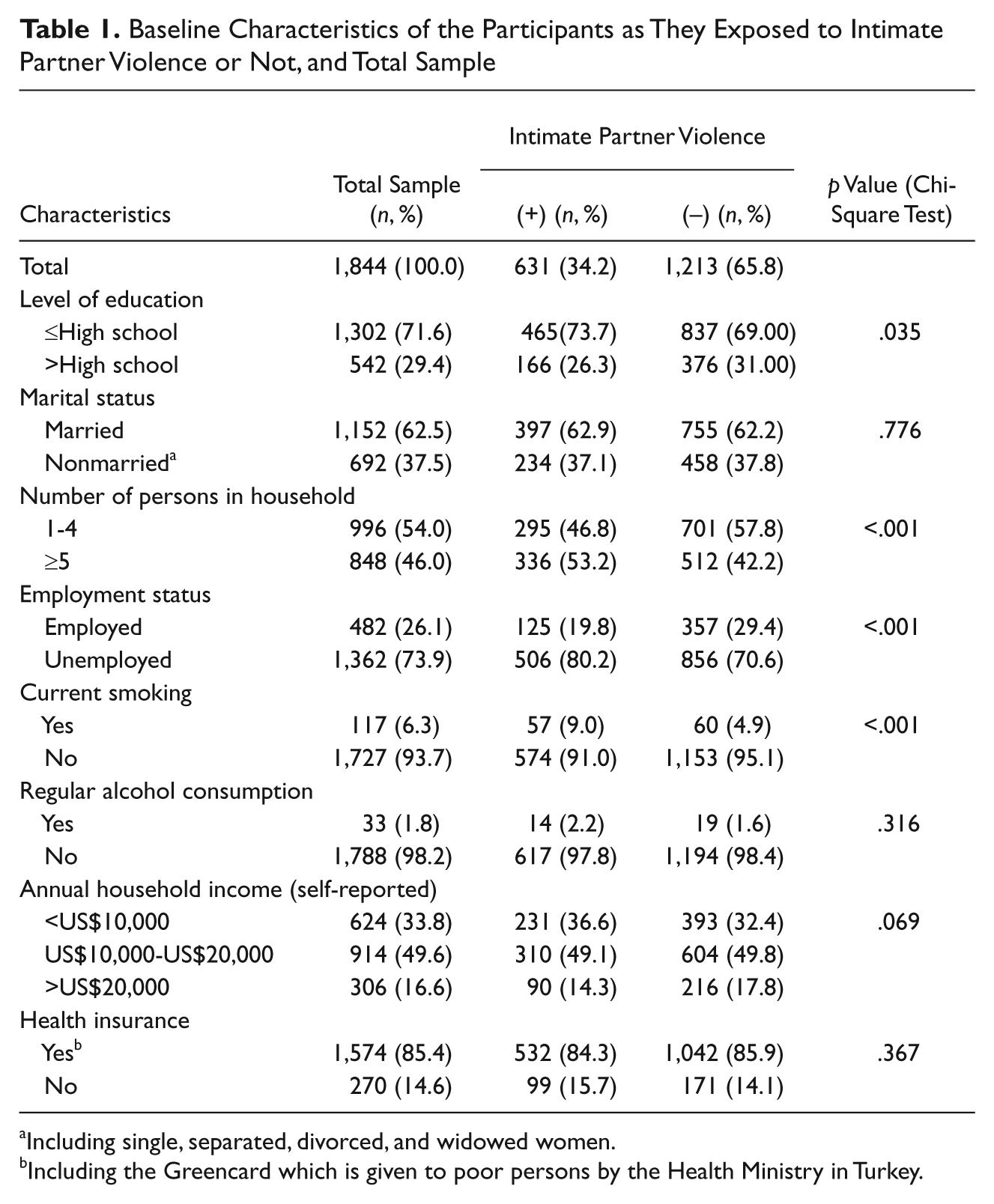
Including single, separated, divorced, and widowed women.
Including the Greencard which is given to poor persons by the Health Ministry in Turkey.
General Health Status of the Sample
In this study, we found that health-related problems such as hypertension, diabetes mellitus, or coronary disease were more common among abused women. Fewer abused women than nonabused perceived their health status to be “very good” or “good” (86.4% vs. 95.4%), whereas more abused women reported their health to be “poor” or “very poor” (13.6% vs. 4.6%).
Almost 29% of the women presented emotional distress. More than three fourth of the sample (79.8%) considered their current health status as good (or as bad) as it was the previous year, whereas 12.5% reported it was better and 7.7% worse.
Intimate Partner Violence
Prevalence of IPV was found as 34.2% in this study. Ratio of women reported having experienced physical violence at some time in their life was 10.3%, and 5.7% reported IPV in the past 12 months. Rate of women reported having experienced sexual violence at some time in their life was 6.8%, and 3.7% reported sexual violence in the past 12 months.
Women experienced violence were differed by means of education, employment status, number of living person in household, and smoking history of women whose had not exposed to violence. There were no differences in the health insurance status, marital status, regular alcohol consumption, and annual household income between women exposed to violence and women not exposed to violence (Table 1).
Women exposed to violence were mainly had lower level of education (73.7% vs. 69.0%, p = .035) than women not exposed to violence. More women exposed to violence were living in households with more than 4 persons (53.2% vs. 42.2%, p <.001) and unemployed (80.2% vs. 70.6%) compared with women not exposed to violence. The rate of current smoking was higher in women exposed to violence compared with women not exposed to violence (9.0% vs. 4.9%, p <.001).
Table 2 presents the adjusted odds ratios and 95% confidence intervals for the independent variables that emerged as significant predictors of IPV victimization experienced in the past 12 months and more than 12 months ago based on multivariate logistic regression analysis. Logistic regression analysis showed that women only living in households with more than 4 persons is significantly associated with risk of physical type of violence regardless of timing of the abusive episodes (OR = 1.65, r = .064, p = .018 for current physical abuse, and OR = 2.07, r = .071, p = .003 for past). Being educated less than a high school (OR = 8.96, r = .067, p = .030) and having less-than-US$$10,000 annual household income (OR = 2.64, r = .003, p = .009) were significantly associated with risk for physical violence in current abuse. Having at least one type of chronic illnesses, such as, hypertension, diabetes, or coronary disease, is significantly associated with risk for physical type of violence in current abuse (OR = 2.07, r = .083, p <.001) and with risk for sexual abuse regardless of timing of the abusive episodes (OR = 4.80, r = .037, p <.001 for current sexual abuse, and OR = 7.02, r = .144, p <.001 for past). Interestingly, being unemployment was significantly associated with lower risk for physical violence in the past period (OR = 0.58, r = –.051, p = .035). In addition, being married was also significantly associated with lower risk for sexual type of violence both in current period and in the past period (OR = 0.20, r = –.110, p <.001; and OR = 0.18, r = –.143, p <.001, respectively; Table 2).
Relationship Between Sociodemographic Variables and Types of IPV Experienced in the Past 12 Months and More Than 12 Months Ago in Logistic Regression Analysis, With Odds Ratios and 95% Confidence Intervals (n = 1,844)

Statistically significant p values.
Intimate Partner Violence and Mental Health
As shown in Table 3, women exposed to IPV was more likely to have mental distress and a bad self-perceived health status. Mental distress and worsened self-perceived health status were significantly associated with physical type of violence, regardless of timing of the IPV episodes. Mental distress and worsened self-perceived health status were significantly associated with sexual violence in the current episode.
Mental Health Indicators by Types of IPV Experienced in the Past 12 Months and More Than 12 Months Ago (n = 1,844)
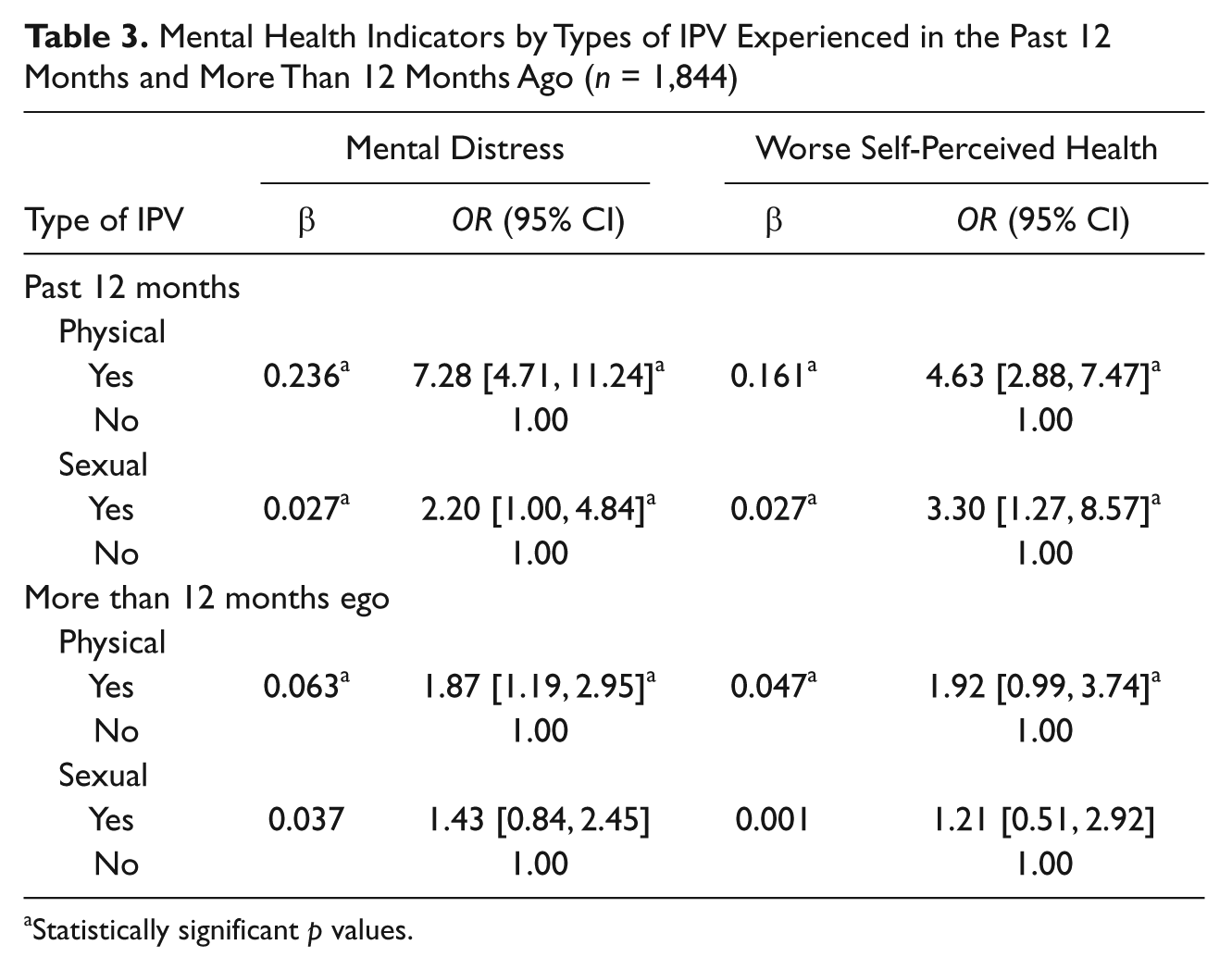
Statistically significant p values.
Discussion
This survey highlights the association between IPV victimization and mental health problems in a large sample of women in reproductive age in a middle Anatolian city. The prevalence of mental health problems in women who had ever experienced physical, emotional, or/and sexual violence is consistent with those previously reported studies (Bradley, Smith, Long, & O’Dowd, 2002; Richardson et al., 2002; Ruiz-Pérez et al., 2006). Results of this study regarding IPV prevalence by type also agree with previous studies, wherein the most frequently reported IPV category was emotional violence (Hegarty & Bush, 2002; Ishida et al., 2010; Ruiz-Pérez et al., 2006). This finding highlights the importance of studying the different kinds of violence effect on mental health.
The prevalence of physical violence found in this study is comparable with data from other population-based studies performed in developed countries that they have been reported 10% to 14% of estimated physical violence rates over a 1-year period in women living with an intimate person in their home (Rollins & Oheneba-Sakyi, 1990; Smith, 1987; Straus & Gelles, 1986). A study from United States, as carried out in the medical setting, reported a higher rate (23%) of physical violence among adult women lived with intimate partners (Hamberger, Saunders, & Hovey, 1992). Since physical violence is frequently associated with injury, women sampled in medical environments would be expected to have a higher prevalence than women sampled in population settings.
Previous population-based studies reported that the prevalence of sexual violence ranges from 8% to 9% (Dalal & Lindquist, 2010; Ruiz-Pérez et al., 2006; Schroll, Tabor, & Kjaergaard, 2011). The percentage of sexual violence reported in this study was lower than in those previously reported large sampled studies. Women who participated in this study may tend to “underreport” their experiences of sexual violence because they may be less likely to view the incident as abusive.
The risk for experiencing IPV has been universal (Jewkes, 2002) because of IPV frequently evolves from patriarchal and traditional social structures (e.g., women’s lack of financial autonomy and low socioeconomic status) that imply women’s subordinate status in the society (Heise, Ellsberg, & Gottemoeller, 1999). This study shows how sociodemographic characteristics could be associated with IPV. The present data demonstrated that women who are less educated and living in households more than 4 people were exposed to IPV more than other women. This observation consistent with the results of other studies from Turkey (Tokuç et al., 2010) and reports from other countries (Kishor & Johnson, 2006; Parish, Wang, Laumann, Pan, & Luo, 2004).
Number of studies have found that certain sociodemographic conditions are associated with physical violence (Bonomi et al., 2006; Ishida et al., 2010). This study shows that, women who living in households with more than four people are at the risk of physical violence. Risks for physical violence were also more frequent in women who are less educated, having health-related problems and with low family income. Women with better socioeconomic condition may not be dependent on their partners as do women with lower socioeconomic conditions. In other words, women with well socioeconomic conditions are more autonomous and possess the resources and skills necessary for better recognition and termination of a potentially abusive relationship.
The findings of this study demonstrated a strong association between IPV and mental health problems. Violence experiences, in addition, associated with increased levels of mental distress and worsened self-perceived health status. The self-assessment of worsened mental health among women exposed to IPV in the current study is consistent with findings from other studies concerned with mentally and physically assaulted women (Holden, 2003; Walling et al., 1994). Findings of the present research strongly suggested that the different types of IPV might have different effects on women’s mental health status.
Women experiencing either physical (regardless of timing) or sexual violence (within the past 12-month period) were more likely to have mental distress and more likely to report a poor self-perceived health status than never-assaulted women. Self-perceived health status has been demonstrated to be a very good predictor of morbidity and mortality (Fanslow & Robinson, 2004; Kyffin et al., 2004), and it reflects both mental and physical health; one would expect a high positive correlation between mental distress and self-perceived health status in all women exposed to IPV.
Despite all the usual biases of self-reporting, this population-based study highlighted the differential associations between IPV and poor mental health by the type and timing of IPV and several important policy recommendations should be suggested from this study. This study show that violence in the previous year were strongly associated with worsened mental health and that women who experienced IPV in the past were also more likely to have mental distress than never-assaulted women. This finding suggests that the effects of IPV on mental health may not only be immediate and acute but could also be long term or even become chronic (Romito, Molzan, & De Marchi, 2005).
In conclusion, there are clear differences in the experience of IPV and associated mental health outcomes. Strategies to reduce the burden of women’s mental health problems should include efforts for early determination and prevention of IPV against women in reproductive age.
Footnotes
Acknowledgements
The author wish to thank all the participants who gave up their time to participate in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.