
Abstract
Betrayal trauma theory postulates that traumas perpetrated by a caregiver or close other are more detrimental to mental health functioning than are traumatic experiences in which the victim is not affiliated closely with the perpetrator. This study is the first to examine the concept of betrayal among a sample of individuals with a history of homelessness. A total of 95 homeless or formerly homeless adults completed the Brief Betrayal Trauma Survey, the Posttraumatic Stress Disorder Checklist–Civilian Version, the Center for Epidemiologic Studies Depression Scale the Perceived Stress Scale, and a demographics questionnaire assessing participants’ histories of homelessness, health, and relationships with their families. Regression analyses were conducted to explore the associations between high betrayal (HB) and low betrayal (LB) trauma exposure, relationship with family, and physical and mental health symptoms. Exposure to HB traumas in childhood and poor family relationships predicted earlier age at first episode of homelessness, and participants who had been exposed to a greater number of traumas during childhood were more likely to be revictimized during adulthood. Trauma exposure as an adult and earlier age of first homeless episode predicted symptoms of posttraumatic stress disorder, while trauma exposure alone predicted symptoms of depression and perceived stress. Number of medical diagnoses was associated with trauma exposure and becoming homeless at an older age. These findings emphasize that even among the most marginalized and multiply victimized individuals in our society, traumas that are characterized by a higher degree of betrayal are associated with more adverse outcomes.
Homelessness is a serious public health problem that occurs at the intersection of personal, situational, demographic, economic, and familial factors (Koegel, Melamid, & Burnam, 1995). A recent point-in-time estimate reported that 636,017 homeless persons were identified in communities across the United States (National Alliance to End Homelessness, 2012), and as many as 3.5 million Americans are believed to experience homelessness in any given year (National Alliance to End Homelessness, 2009).
The lives of homeless individuals are laden with adversity, and the chaotic and often traumatic circumstances that accompany homelessness may precipitate or exacerbate mental health and physical problems. Research documents high rates of childhood and adulthood trauma among the homeless (e.g., Ryan, Kilmer, Cauce, Watanabe, & Hoyt, 2000; Stein, Leslie, & Nyamathi, 2002; Tyler, Melander, & Noel, 2009). In a sample of 372 homeless adolescents, Tyler and Cauce (2002) found that 29% and 47% of participants reported being sexually and physically abused, respectively. Childhood abuse among homeless young people has been associated with subsequent intimate partner violence (Slesnick, Erdem, Collins, Patton, & Buettner, 2010; Tyler et al., 2009); a greater likelihood of trading sex for food, shelter, money, or drugs (Tyler, Hoyt, & Whitbeck, 2000); and elevated risk of self-directed violence (Torchalla, Strehlau, Li, Schuetz, & Krausz, 2012). North, Smith, and Spitznagel (1994) discovered that more than 40% of homeless men and women confirmed at least one violent trauma in their adult lives, most commonly assault for men and rape for women. Conservative estimates report that 20% of homeless men and more than 30% of homeless women meet lifetime criteria for posttraumatic stress disorder (PTSD; North & Smith, 1992), compared with a rate of 6.8% in the general population (Kessler et al., 2005). A recent Australian study found that lifetime PTSD diagnosis among homeless adults may even exceed 50% (Taylor & Sharpe, 2008).
Lack of insurance limits access to health care, and immediate survival demands (e.g., obtaining food and shelter) compete with seeking preventive health care (Barrett, Fogel, Garrett, & Young, 2011). A large survey of patients at federally qualified health centers confirmed disparities among homeless and housed patients in the prevalence of chronic illnesses, mental health conditions, and substance use disorders (Lebrun-Harris et al., 2012). A growing body of literature also links trauma exposure to adverse health outcomes through behavioral, social, cognitive, and emotional pathways (Kendall-Tackett, 2002), all of which may be especially influential in the lives of individuals who are homeless.
Homeless individuals often describe histories of chaotic early family lives marked by a dearth of social support and abuse (Lalonde & Nadeau, 2012). Social support has been shown to exert a buffering effect against the development of PTSD (Hyman, Gold, & Cott, 2003) and may also be protective against revictimization. People who suffer abuse or neglect may have difficulties trusting other people or institutions (e.g., law enforcement), even those that may have benevolent intentions (Gobin & Freyd, 2009). This may preclude abuse survivors from cultivating healthy social support networks later in life, which may make them more vulnerable to adverse outcomes, including homelessness and revictimization. Indeed, homeless individuals who perceive themselves as having good social support are less likely to be revictimized (Hwang et al., 2009).
Betrayal Trauma Theory
Betrayal trauma theory posits that traumatic experiences vary in degree of interpersonal violation based on the relationship between the victim and the perpetrator, and that a victim will suffer greater consequences when the perpetrator is a close other (Freyd, 2012; Freyd, DePrince, & Gleaves, 2007). Traumas higher in betrayal occur “when the people or institutions on which a person depends for survival significantly violate that person’s trust or well-being” (Freyd, 2008, p. 76). For instance, sexual or physical abuse by a caretaker or intimate partner would be considered a high betrayal (HB) trauma, while traumas that are not interpersonal in nature (e.g., natural disasters) or are perpetrated by aggressors with whom there is little or no relationship (e.g., a stranger) are regarded as low betrayal (LB) traumas.
According to betrayal trauma theory, when trauma is perpetrated by a close other, especially a caretaker, a child is placed in an unsolvable bind. To deem a caretaker culpable yields great risk, as the child is dependent on the adult perpetrator to have his or her basic survival needs met (Goldsmith, Barlow, & Freyd, 2004). Moreover, leaving the abusive situation may result in loss of access to life-sustaining resources, ultimately resulting in homelessness. To avoid these situations, a child may experience a form of unknowing (e.g., dissociation), an adaptive blindness to the betrayal, which enables him or her to continue to trust and to rely on the caretaker for survival needs (Freyd, 1997). While this lack of awareness offers a short-term solution, it carries with it psychological risks. Children abused by an immediate or an extended family member tend to suffer greater internalizing problems than children who were victimized by a distant other (Tremblay, Hébert, & Piché, 1999). Likewise, HB traumas are associated with greater symptoms of PTSD, depression, and anxiety than are LB traumas (Goldsmith, Freyd, & DePrince, 2012; Tang & Freyd, 2012). As trauma survivors grow older and become increasingly self-reliant, they “may become conscious of strong feelings of betrayal” (DePrince & Freyd, 2002, p. 75), leading to a distrust of other people, and even institutions, on which they rely (Gobin & Freyd, 2009). Indeed, institutional betrayal adds yet another layer of victimization. For example, college-aged women who reported coercive or unwanted sexual experiences that were followed by failure of an institution, such as a university, to take action to respond to the event, suffered increased posttraumatic symptoms (Smith & Freyd, 2013). Disabling psychological symptoms, coupled with lack of trust, may be another path to homelessness.
Current Study
Although betrayal and its relationship with trauma sequelae have been researched in a variety of populations, including undergraduates and community samples, this concept has not been investigated in homeless populations. Moreover, scant research has explored the relationship of homeless individuals to perpetrators who victimized them, and the emotional and physical health ramifications of the proximity of those relationships have not been elucidated. Tyler and Cauce (2002) found that among homeless adolescents with a history of physical abuse, the majority had been harmed for the first time by a family member, most commonly a biological parent. Of those who had been sexually abused during childhood, 35% were victimized first by either a relative, an older sibling, or a biological parent (Tyler & Cauce, 2002). To date, a limited number of studies have reported that traumas with a higher degree of betrayal are more strongly associated with mental and physical health difficulties (Edwards, Freyd, Dube, Anda, & Felitti, 2012; Freyd, Klest, & Allard, 2005; Goldsmith et al., 2012), but this has not been examined among homeless individuals. The present study sought to investigate the association between self-reported trauma exposure and various aspects of physical and mental health in a sample of homeless adults. Three hypotheses based on betrayal trauma theory were proposed:
Method
Participants
Participants were recruited between April 2009 and February 2011 using fliers posted at an outpatient clinic that provides services to homeless and impoverished persons in Miami, Florida, and through word-of-mouth in the homeless community. Participants were English-speaking adults (N = 94) ages 18 to 65 years who were homeless or who reported a history of homelessness (see Table 1 for demographic information). The measures were part of a larger neuropsychological test battery. Prospective participants were excluded if they reported using drugs or alcohol in the 8 hours prior to participation or if they were suspected to be under the influence. Four participants who initiated the consent process withdrew participation midway through the study, citing conflicting obligations (e.g., need to retrieve personal belongings from a day program before it closed for the day). No participants who began the consent process were excluded on the basis of substance use concerns.
Descriptive Statistics for Study Participants (N = 94).

Note: GED = General Equivalency Diploma
Measures
Assessments were administered by the principal investigator (first author) and a team of research assistants, all of whom were doctoral-level graduate students in a clinical psychology program who had received prior training administering the assessment battery.
Brief Betrayal Trauma Survey (BBTS)
The BBTS (Goldberg & Freyd, 2006) inquires about 12 traumatic events an individual may have endured, each rated on a 3-point scale (i.e., never, 1 or 2 times, more than that). Two time intervals are queried—before and after age 18. Good psychometric properties have been reported (Goldberg & Freyd, 2006). Responses were recoded into dichotomous categories of “never” and “1 or more times” and summed (Freyd et al., 2005). Items describing traumas not perpetrated by another person or involving a perpetrator with whom the victim was not close are considered LB, whereas interpersonal traumas perpetrated by a close other are considered HB. Total scores were derived for traumas experienced during both time intervals, as well as for subscale scores for HB and LB traumas in each age range.
PTSD Checklist–Civilian Version (PCL-C)
The PCL-C (Weathers, Litz, Herman, Huska, & Keane, 1993) is a 17-item inventory that assesses for PTSD symptoms (Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.]; DSM-IV-TR; American Psychiatric Association, 2000, criteria) and quantifies the severity of symptoms during the preceding month. Symptoms are rated on a 5-point Likert-type scale (i.e., not at all, a little bit, moderately, quite a bit, extremely), with total scores ranging from 17 to 85. The PCL-C is used as a screening measure but has demonstrated 90% diagnostic efficiency when compared with the Clinician Administered PTSD Scale (Blanchard, Jones-Alexander, Buckley, & Forneris, 1996). It has good test–retest reliability and internal consistency (Ruggiero, Del Ben, Scotti, & Rabalais, 2003; Weathers et al., 1993).
Center for Epidemiologic Studies Depression Scale (CES-D)
The CES-D (Radloff, 1977) is a 20-item measure designed to assess depressive symptomatology in the prior week. Items are rated on a 4-point Likert-type scale (i.e., rarely or none of the time, a little or some of the time, occasionally or a moderate amount of the time, most or all of the time). Scores range from 0 to 60, with higher scores indicating more severe symptoms. The CES-D has demonstrated good psychometric properties in community and psychiatric settings (Radloff, 1977), as well as in homeless samples (LaGory, Ritchey, & Mullis, 1990; Wong, 2000).
Perceived Stress Scale (PSS)
The PSS (Cohen, Kamarck, & Mermelstein, 1983; Cohen & Williamson, 1988) is a 10-item measure designed to gauge the degree to which a person has experienced life as uncontrollable and/or unpredictable in the last month. Items are rated on a 5-point Likert-type scale (i.e., never, almost never, sometimes, fairly often, very often). Scores range from 0 to 40. Higher scores indicate a greater degree of stress. Among a nationally representative sample of 2000 participants, the average score was 15.52 (SD = 7.44; Cohen & Janicki-Deverts, 2012). Good psychometric properties have been reported (Roberti, Harrington, & Storch, 2006).
Demographic and personal information
A questionnaire was utilized to gather demographic and background information and participants’ histories of homelessness. Items used in the current analyses included age at first homeless, quality of relationship with family (i.e., great, okay, poor, I do not have a relationship), and medical conditions. Chronic conditions included arthritis, diabetes, hypertension, high cholesterol, HIV/AIDS, physical disability, sexually transmitted disease (not including HIV), seizures/epilepsy, tuberculosis, and “other.” A variable was created by summing the number of number of reported medical diagnoses.
Research Ethics
Research ethics of relevance to this population were considered (Runnels, Hay, Sevigny, & O’Hara, 2009). Materials were written at no higher than a sixth-grade reading level. A synopsis of key points in the informed consent form was provided verbally to each participant, and the complete form was read aloud, unless a participant indicated a preference for reading it independently. To thank them for contributing to the study, participants were provided a gift card to a nearby sandwich shop and an up-to-date list of nearby shelters, mental health resources, and services. The Institutional Review Board at Nova Southeastern University approved this study.
Data Analysis
Fewer than 1% of data points were missing, and missing data were handled differently for each measure. Missing data on the BBTS were coded as 0 (no exposure; see Goldsmith et al., 2012). One participant’s age at first homeless episode was missing, and that participant was excluded from analyses where that variable was considered. On the PCL-C and the CES-D, missing values were replaced using two-way imputation, in which a participant’s other scores on the same measure, as well as other participants’ scores on the missing item, are used to estimate scores for missing items (Sijtsma & van der Ark, 2003; van Ginkel & van der Ark, 2005). For regression analyses, all variables were entered into the models simultaneously as no particular variable or set of variables was considered to be more or less relevant in testing our hypotheses. Indices of collinearity were well within acceptable limits, except as noted.
Results
Participants’ mean age at the time of their first homeless episode was 35.9 years (SD = 12.4; range = 14-63 years). Twenty percent of participants became homeless for the first time during adolescence or young adulthood (i.e., by the age of 25 years). Participants had been homeless for a total of 6.1 years (SD = 6.8), and most (64.9%) had experienced multiple episodes of homelessness. All but two participants (97.9%) reported at least one of the traumatic events queried by the BBTS. Because events were assessed for two age categories (before and after age 18), scores ranged from 0 to 24. The mean number of traumas reported was 8.7 (SD = 5.7). Most participants reported one or more LB traumas during childhood (68.1%) and adulthood (85.1%), with 90.4% reporting at least one lifetime LB trauma (see Table 2). Similarly, at least one lifetime HB trauma was reported by 87.9% of the sample, with 70.2% reporting one or more childhood HB traumas and 72.3% reporting at least one adulthood HB trauma. Participants were multiply exposed, with 47.9% and 66.0% reporting exposure to four or more types of traumas during childhood and adulthood, respectively.
Exposure to LB and HB Traumas During Childhood and Adulthood.

Note. LB = low betrayal; HB = high betrayal; BBTS = Brief Betrayal Trauma Survey.
Mean scores on symptom measures were high and fell in the clinically significant range (see Table 3). A majority of participants (77%) had scores greater than 16 on the CES-D, and 40% scored above 50 on the PCL-C. Scores on the PSS indicated high levels of perceived stress (M = 21.0, SD = 7.5), with 79.8% of the sample scoring higher than average (Cohen & Janicki-Deverts, 2012). Most participants (75.5%) indicated they had been diagnosed with one or more of the major medical conditions surveyed, and more than half (55.3%) endorsed at least two diagnoses.
Descriptive Statistics (N = 94).

Note. LB = low betrayal; HB = high betrayal; PCL-C = PTSD Checklist–Civilian Version; CES-D = Center for Epidemiologic Studies Depression Scale; PSS = Perceived Stress Scale; PTSD = posttraumatic stress disorder.
Hypothesis 1
Childhood exposure to HB trauma and poorer relationship with family were hypothesized to be associated with younger age at first homeless episode. As hypothesized, exposure to more childhood HB trauma (β = −.33, t = −2.53, p < .05) and poorer self-reported relationship with family (β = .32, t = 3.03, p < .01) each predicted younger age of first homeless episode. Exposure to childhood LB trauma was not a significant predictor (β = .07, t = .52, p > .10).
Hypothesis 2
It was hypothesized that exposure to childhood trauma and age of first homeless episode would predict exposure to trauma in adulthood. Exposure to a greater number of childhood HB (β = .31, t = 2.89, p < .01) and LB traumas (β = .37, t = 3.43, p < .01) and younger age of first homeless episode (β = −.19, t = −2.22, p < .05) each predicted more exposure to LB trauma as an adult. In partial support of this hypothesis, exposure to more childhood HB trauma (β = .61, t = 6.23, p < .01), but not LB trauma (β = .14, t = 1.45, p > .10) or age at first homelessness (β = −.01, t = −.18, p > .10), predicted more exposure to HB trauma during adulthood.
Hypothesis 3
Becoming homeless at a younger age and being exposed to more traumas during adulthood were hypothesized to predict worse mental health symptoms and greater numbers of medical diagnoses. First, attempts were made to explore the independent effects of HB trauma and LB trauma experienced during adulthood on current symptoms by entering BBTS subscales as separate variables in regression models predicting current symptoms. By entering those subscales of the BBTS as separate variables in regression models predicting current symptoms. Although the overall models were significant, individual betas were not, a situation that may occur when multicollinearity exists (Friedman & Wall, 2005). Although collinearity diagnostic tests were well within acceptable limits (variance inflation factor = 2.03-2.04), a correlation matrix revealed that adult HB trauma and adult LB trauma had very similar correlations with symptom measures (see Table 4). Thus, there was concern that measuring those subscales separately was redundant in this sample. To remedy this problem, a total score was calculated by summing the number of traumas during adulthood, and this variable was used in place of subscale scores in regression models predicting current symptoms.
Pearson r Correlations Among Trauma Measures and Current Symptoms (N = 94).

Note. LB = low betrayal; HB = high betrayal; PCL-C = PTSD Checklist–Civilian Version; CES-D = Center for Epidemiologic Studies Depression Scale; PSS = Perceived Stress Scale; PTSD = posttraumatic stress disorder.
p < .05. **p < .01.
Separate regression analyses were conducted with the PCL-C, CES-D, PSS, and number of medical diagnoses (see Table 5). For PTSD symptoms, the hypothesis was supported. Exposure to more trauma as an adult and younger age of first homeless episode each predicted more severe PTSD symptoms. Trauma exposure, but not age of first homeless episode, predicted worse symptoms of depression and stress. Exposure to a greater number of traumas was associated with endorsing more medical diagnoses, but, contrary to our hypothesis, so was older age of first homeless episode.
Associations Among Trauma Exposure, Age of First Homeless Episode, and Current Symptoms (N = 94, df = 2, 92).
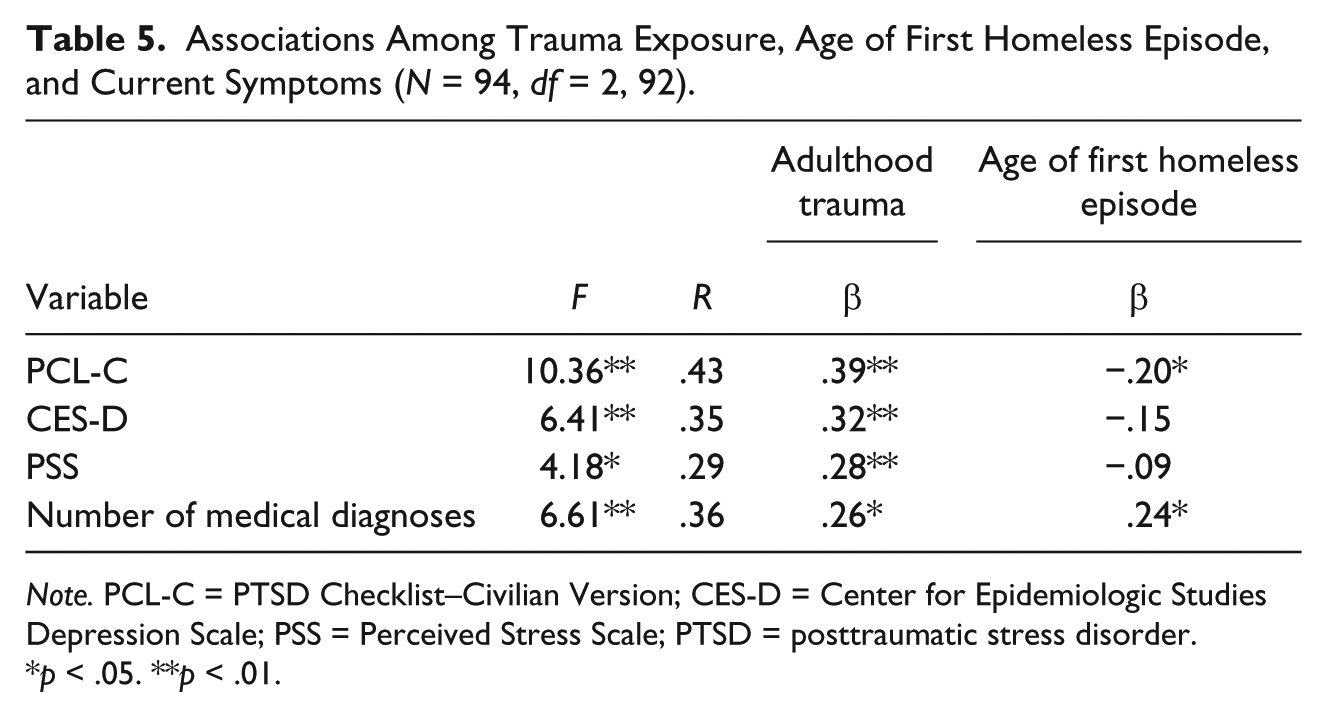
Note. PCL-C = PTSD Checklist–Civilian Version; CES-D = Center for Epidemiologic Studies Depression Scale; PSS = Perceived Stress Scale; PTSD = posttraumatic stress disorder.
p < .05. **p < .01.
A set of post hoc regression analyses were conducted to determine whether duration of homelessness rather than age at first episode of homelessness predicted symptoms in the hypothesized direction. Trauma exposure but not duration of homelessness significantly predicted worse symptoms of PTSD, depression, and stress, and more medical diagnoses (see Table 6).
Associations Among Trauma Exposure, Duration of Homelessness, and Current Symptoms (N = 94, df = 2, 92).

Note. PCL-C = PTSD Checklist–Civilian Version; CES-D = Center for Epidemiologic Studies Depression Scale; PSS = Perceived Stress Scale; PTSD = posttraumatic stress disorder.
p < .05. **p < .01.
Discussion
The purpose of this study was to examine the relationship among traumas with varying degrees of betrayal and psychological symptoms and medical diagnoses in a sample of adults who were at the time of the study or had been homeless. As expected, participants endorsed very high rates of trauma exposure during childhood and adulthood. Being exposed to multiple types of traumas was the rule rather than the exception in this sample, and participants endorsed high scores on the PCL-C and the CES-D. Likewise, scores on the PSS were substantially higher than those found in the general population, which aligns with prior research that demonstrated a relationship between lower socioeconomic status and elevated levels of stress (Cohen & Janicki-Deverts, 2012).
Exposure to a greater number of HB traumas during childhood and a poorer relationship with family predicted younger age at first episode of homelessness. Given that HB traumas are perpetrated by someone close to the victim, it is likely that family members were responsible for at least a portion of the violence to which participants were exposed early in their lives. As predicted, LB traumas were not associated with earlier onset of homelessness. LB traumas may or may not be interpersonal in nature and can occur in chaotic families, as well as in families where a greater degree of stability exists.
Exposure to a greater number of LB traumas during adulthood was predicted by HB and LB traumas during childhood, a finding that is consistent with research on revictimization (McIntyre & Widom, 2011; Widom, Czaja, & Dutton, 2008). Younger age at first homeless episode also predicted LB traumas in adulthood and was associated with a greater total number of years being homeless (r = −.30, p = .003). It is not surprising that participants who were homeless longer were exposed to more LB traumas, given that homeless individuals are typically in closer physical proximity to potential offenders, and the likelihood of repeat victimization increases with duration of homelessness (Tyler, Gervais, & Davidson, 2012). Consistent with the work of Gobin and Freyd (2009), experiencing HB but not LB traumas during childhood predicted exposure to HB traumas during adulthood, indicating, tragically, that circumstances on the streets yield further betrayal, victimization, and violence rather than a reprieve from the abusive familial relationships that were endured at home (Whitbeck, Hoyt, & Ackley, 1997). Zurbriggen and Freyd (2004) asserted that exposure to traumas high in betrayal may be detrimental to cognitive mechanisms that enable an individual to make self-protective decisions later in life. For example, a survivor of HB traumas may be less astute at recognizing an unhealthy relationship and, consequently, less likely to make the choice to remove himself or herself from a situation that may risk further victimization. This mechanism may help to explain the high rates of recurrent HB trauma in this sample. The sequelae of betrayal trauma may also make it more difficult for those who have been victimized to establish a healthy social network, which would help to insulate an individual against adverse outcomes such as homelessness. These findings corroborate those of prior studies, lending further support to the tenets of betrayal trauma theory.
The hypothesis that trauma exposure and earlier onset of homelessness would predict more severe PTSD symptoms was supported. This is consistent with recent research that indicates greater exposure to trauma and poorer socioeconomic situations are related to PTSD (Klest, Freyd, & Foynes, 2012). Perceived stress and depression were predicted by trauma exposure only and were not significantly associated with age of first homeless episode. On examining these findings, we hypothesized that duration of time homeless may be a more influential factor than age of first homeless episode, as the effects of homelessness (e.g., victimization, social and economic deprivation) are likely cumulative over time. However, this alternative hypothesis was also not supported. These results were not consistent with predictions, and several explanations are offered. Earlier onset of homelessness may be associated with symptoms of stress and depression, but the effect size may be too small to be detected in this sample. Alternatively, and perhaps more likely, homelessness itself may be a risk factor for stress and depression, regardless of when in life it occurs or for how long it lasts. Variation in symptom severity may be better explained by the additive impact of stressors and traumas above and beyond the shared stressor of homelessness.
It was predicted that a greater number of traumas would be associated with poorer health, which was, indeed, the case. A growing literature links mood disorders with hyperarousal of the sympathetic nervous system. Psychosocial stressors, including trauma, may have an impact on the development of mood disorders but may also be pathways to inflammatory health conditions (e.g., cardiovascular disease and diabetes; Currier & Nemeroff, 2010; Miller, Maletic, & Raison, 2009). It was also expected that individuals who became homeless younger would report a greater number of medical conditions, because the harsh conditions on the street may have a deleterious effect on health status; however, this was not the case. Older age at the time of first homeless episode was associated with more medical diagnoses. Of course, older adults are more likely to suffer certain health conditions; thus, more health problems might be expected among an older cohort. The supposition is supported by Schanzer, Dominguez, Shrout, and Caton (2007) who found that many newly homeless adults had medical and psychiatric conditions prior to becoming homeless. It is possible that for at least some individuals in our sample, poor health was more a contributor to, rather than an effect of, homelessness. Individuals who become homeless later in life may have been burdened and/or made destitute by poor health through interactive effects of comorbid mental health conditions, limited financial resources, and poor social support. Moreover, it is possible that individuals who become homeless later have remained for longer periods of time with his or her abuser(s). This supposition is consistent with the tenets of betrayal trauma theory, which suggest that cognitive coping mechanisms, such as dissociation, may serve a survival function for the victim by allowing him or her to remain attached to an individual on whom he or she is dependent (Zurbriggen & Freyd, 2004).
This study has a number of limitations that warrant discussion. Participants were a convenience sample and were recruited at a primary care clinic, which may have led to a biased recruiting of individuals who had greater health needs or who presumably had better access to medical and behavioral health services. Likewise, excluding individuals who had used alcohol or drugs in the 8 hours prior to study participation may have led some prospective participants to choose not to participate. Thus, this sample may not be representative of the larger homeless population, and findings may not generalize to other, more socially isolated individuals or to those who have more severe substance use difficulties. Because it was cross-sectional in design and retrospective in nature, this study may have involved over- or under-reporting of traumas and family difficulties, particularly given that participants were asked to recall events from their childhoods. In addition, although participants were reassured that their responses were confidential, some participants may have been reluctant to disclose fully the extent of their past victimization, given the sensitive and potentially stigmatizing nature of the topic. Our sample size was also small, which precluded more complex analyses and limited its power to examine differences between subgroups (e.g., males vs. females). Despite these limitations, this is the first study of which we are aware to explore betrayal in relation to psychological and physical health functioning in a homeless population.
Conclusion
These results support betrayal trauma theory and substantiate findings of recent research that notes the relationship between HB trauma exposure and adverse long-term physical and mental health outcomes (Edwards et al., 2012; Gobin & Freyd, 2009). This study adds uniquely to this burgeoning area of research by introducing betrayal as a potentially important factor in understanding symptoms among homeless adults and by demonstrating that among individuals who are homeless—the most marginalized and vulnerable individuals in society—those persons whose lives were marred by victimization perpetrated at the hands of caregivers tend to fare worse psychologically and to suffer more victimization later in their lives. These findings underscore the importance of early intervention after trauma to prevent long-term adverse outcomes, including homelessness. In effect, what would be considered a tertiary intervention for trauma exposure becomes a primary or even secondary prevention for homelessness. In addition, these findings add to the body of literature on trauma among individuals who are homeless and have implications for frontline service providers. Physicians, mental health providers, social workers, and other service providers (e.g., shelter staff) may benefit from education regarding the emerging findings about betrayal trauma and its relationship with mental and physical health.
Footnotes
Acknowledgements
First and foremost, we wish to thank the individuals who kindly offered their time to participate in this study. We also thank Jessica Karle, Robyn Hardie, Cynthia King, Tracy Chisholm, Patrick Aragon, Rachel Orleck, and Alexandra Bodden for their assistance with data collection, as well as Dr. Frederick P. Rivara for his editorial commentary on an earlier draft of this manuscript.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Mackelprang received fellowship support from the National Institute of Child Health and Human Development (T32HD057822) during the preparation of this article.