
Abstract
A survey using a community-based sample (N = 650) was conducted to identify motivational and cognitive predictors of individuals’ propensity to intervene against intimate partner violence (IPV). A hierarchical regression analysis showed that motivational factors accounted for the greatest proportion of the variance in self-reported propensity. Specifically, personal norm (i.e., an individual’s felt obligation to intervene) was the strongest individual predictor, followed by affective response (i.e., the extent to which an individual responds to IPV with negative emotions). Although cognitive factors explained only a small portion of the variance, the propensity to intervene was significantly higher for respondents who perceived IPV as a prevalent issue and who did not view the perpetrator as responsible for the solution of IPV. The findings suggest that attempts to facilitate public intervention should target specific, rather than general, aspects of public norms and beliefs about IPV.
Intimate partner violence (IPV) is a widespread global problem (Coker, Smith, Bethea, King, & McKeown, 2000; Kramer, Lorenzon, & Mueller, 2004). IPV refers to any behavior between intimate partners that causes physical, sexual, or psychological harm or distress, and includes aggressiveness, coercion, abuse, and controlling behavior (World Health Organization, 2010). Although there is strong public consensus regarding the undesirability of IPV, some people are reluctant to personally intervene when suspecting cases of IPV (Gracia & Herrero, 2006; West & Wandrei, 2002). Very little previous research has addressed factors that predict individuals’ propensity to intervene (for exceptions, see Beeble, Post, Bybee, & Sullivan, 2008; West & Wandrei, 2002). Knowledge about such predictors is crucial for the design of information campaigns aimed at increasing public intervention, because specific information appeals—targeting particular factors that inhibit and facilitate desirable behavior—tend to be more effective than general appeals (Lewandowsky, Ecker, Seifert, Schwarz, & Cook, 2012; Noar, Benac, & Harris, 2007).
In this article, we present a public survey exploring individual predictors of the propensity to intervene against IPV. While we acknowledge that prosocial behavior is determined by a wide range of individual and situational variables, we focus here on two classes of predictors—motivational and cognitive—that we consider to be particularly relevant in the current context.
Motivational Predictors
For people to engage in behavior that transcends immediate self-interest, there need to be sufficient motivational underpinnings. Common for all motivational predictors of behavior is that they produce a felt need to engage in a behavior, either because the behavior entails desirable consequences or because the failure to enact the behavior may bring about negative consequences (Molden, Lee, & Higgins, 2008). Here, we focus on two factors that we expect to be particularly relevant in the context of IPV: personal norms and affective response.
Personal Norms
Norms are explicit or implicit rules stipulating what behaviors are expected or appropriate in particular circumstances (Schwartz, 1977). While social norms are standard or ideal behavior to which individuals in a social group try to conform (Schwartz, 1977; Schwartz & Howard, 1984), personal norms embody the individual nature of norms and vary across individuals (Schwartz, 1977). In previous research, personal norms have been found to predict moral and altruistic behavior, such as blood donation (Armitage & Conner, 2001), reduced car use (Nordlund & Garvill, 2003), and recycling (Andersson & von Borgstede, 2010). Personal norms have not been investigated specifically in relation to intervening against IPV. In accordance with previous findings in other domains, however, we expect that the strength of a personal norm to take action against IPV will be predictive of individuals’ propensity to intervene.
Affective Response
IPV, because of its moral relevance and abusive nature, is likely to trigger affective reactions such as anger, contempt, and sadness. Two strands of research suggest that the extent to which people experience such negative affect in response to IPV may predict how likely they are to take intervening action. First, according to the negative-state relief model (Cialdini et al., 1987), people may act prosocially to enhance their own affective state and to eliminate the negative feelings elicited by observing others’ suffering (Maner & Gailliot, 2007; Manucia, Baumann, & Cialdini, 1984; but see C. Miller, 2010, for exceptions). Second, affective response is an indicator of perceived personal relevance (Zuwerink & Devine, 1996). Hence, people who react with intense emotions when hearing or thinking about IPV are also likely to consider the issue personally relevant. Personal relevance, in turn, strongly predicts whether people are willing to take action in line with their attitudes (Krosnick, 1988). In sum, we expected self-reported negative affect in response to IPV to be a positive predictor of the propensity to intervene.
Cognitive Predictors
In addition to motivation, prosocial behavior is contingent on the extent to which an individual holds cognitive structures (e.g., beliefs, thoughts) that promote such behavior (see, for example, Worden & Carlson, 2005). We consider as cognitive those factors that concern individuals’ beliefs about the causes, nature, and stability of a phenomenon. In the present research, we focused on three factors related to individuals’ beliefs about IPV: causal attribution, solution responsibility, and perceived prevalence.
Causal Attribution
Attribution research concerns how people assign causes to other’s behavior (Fiske & Taylor, 1991; Weiner, 2008). Attribution theory has given central importance to the distinction between internal (or dispositional) and external (or situational) attributions of behavior (e.g., Jones & Davis, 1965; Kelley, 1973; Weiner, 1985); that is, whether a behavior is perceived to be caused by internal characteristics of the actor (e.g., personality, ability) or by something external to the actor (e.g., other people, situational constraints). The internal–external dimension of causal attribution has been applied in research on people’s perceptions of a range of social problems (Carroll, Perkowitz, Lurigio, & Weaver, 1987; Palazzolo & Roberto, 2011; Zucker & Weiner, 1993), and individuals are generally more prone to help others when the problem is attributed to external as opposed to internal factors (Rudolph, Roesch, Greitemeyer, & Weiner, 2004). Translated to the current context, people who perceive IPV as caused by factors within the offender and/or victim (e.g., substance abuse, personality characteristics; Yick & Agbayani-Siewert, 1997) may expect interventions from the outside to be of little use, whereas people who attribute IPV to external causes (e.g., socialization of male aggression; Worden & Carlson, 2005) should be more likely to view the problem as susceptible to external influence. Hence, we expected individualistic attributions to be negatively related, and external attributions to be positively related, to the propensity to intervene against IPV.
Solution Responsibility
Although IPV is generally considered to be unacceptable, there is little consensus within authorities and the public as to who should take action against it (Simon et al., 2001). An individual’s beliefs about who should contribute to the solution of IPV may predict his or her own propensity to intervene against it. Arguably, people who construe IPV as a societal, as opposed to a private, problem would be more prone to identifying themselves as partly responsible for its solution. A large amount of research has shown that the tendency to ascribe responsibility to one’s self is indeed a powerful predictor of prosocial intentions and behavior in various contexts (De Groot & Steg, 2009; Kaiser & Shimoda, 1999; Schwartz, 1977). Hence, we expected that individuals who ascribe responsibility for the solution of IPV to external, societal agents, as opposed to the offender and/or victim, would be more prone to intervening.
Perceived Prevalence
Studies on the prevalence of IPV have typically been attempts to assess or estimate the incidence of IPV in different populations (see, for example, Kramer et al., 2004; Tjaden & Thoennes, 2000). In contrast, only a few studies have investigated the perceived prevalence of IPV in the general public (Beeble et al., 2008; Neighbors et al., 2010; Witte & Mulla, 2012). Research has shown that perceiving IPV as a prevalent issue predicts the willingness to help victims (Beeble et al., 2008) and the perceived need for community interventions (Jakobsson, von Borgstede, Krantz, Spak, & Hensing, 2012). In accordance with these findings, we hypothesized that perceptions of IPV prevalence would positively predict individuals’ propensity to intervene against IPV.
The Present Study
To investigate individual predictors of the propensity to intervene against IPV, we conducted a survey using a large community-based sample. The survey contained measures of each of the predictors treated above, and respondents’ self-reported propensity to intervene served as criterion variable. Based on the relevant research literature, we hypothesized that the propensity to intervene against IPV would be positively related to (a) the strength of personal norms advocating intervening action, (b) negative affective response to IPV, (c) causal attributions to external/societal as opposed to individualistic factors, (d) ascription of solution responsibility to external agents rather than the offender/victim, and (e) perceived prevalence of IPV in the society.
Method
Sample
Data were gathered in January of 2011 through an internet-based questionnaire distributed to 1,070 Swedish community members above 18 years of age. The sample was recruited via an independent online survey company (CINT), hosting respondent panels with more than 425,000 members in Sweden (a country of 9.5 million inhabitants). A reminder was sent after 2 weeks by e-mail to non-responding panelists. Data collection was terminated after 34 days, with a final response rate of 60.7% (N = 650). Overall, the sample adequately reflected the demographic character of the Swedish adult population: About one half of the respondents were female (52.2%), ages ranged from 18 to 80 years (M = 48.3, SD = 18.3), one half of the respondents (50.3%) had a college/university degree as their highest achieved or attempted education, and a majority of the respondents (70.5%) had at least one child. The survey took approximately 10 min for respondents to complete, and they received about 3 EUR for their participation.
Measures
The survey included close-ended items about respondents’ (a) propensity to intervene against IPV, (b) personal norm about intervening, (c) affective response, (d) cause attribution, (e) attribution of solution responsibility, and (f) perceived prevalence of IPV. Unless otherwise stated, items were presented as statements to be rated on 5-point Likert scales (1 = strongly disagree, 5 = strongly agree). Index variables were created by averaging responses to items pertaining to the same predictor or outcome variable (see below). All items were created specifically for the current study. The internet-based questionnaire required respondents to answer all questions and, thus, there were no missing data.
Propensity to intervene
Three items addressed respondents’ propensity to intervene against IPV (“I am prepared to take action against IPV even if it entails personal sacrifice”; “Whenever I hear about IPV, I feel a strong desire to do something about it”; “I am ready to do something actively to eliminate IPV”; Cronbach’s α = .90). The index variable created from these items was used as the criterion variable in the subsequent regression analyses. The distribution of the variable did not deviate considerably from normality (skewness = −.19, SEskewness = .10; kurtosis = −.09, SEkurtosis = .19), and the variable was deemed appropriate as outcome variable in a linear regression analysis.
Personal norm
Respondents’ felt obligation to intervene when discovering or suspecting IPV was assessed through four items (“If I suspect a case of IPV I ought to follow up my suspicion”; “It is my personal obligation to intervene whenever I suspect IPV”; “If I suspected IPV in my social environment, I would feel bad if I didn’t do anything about it”; “I ought to contribute to an openness about talking about IPV”; α = .83).
Affective response
To measure respondents’ affective response, we asked them to rate the extent to which hearing about IPV makes them feel angry, sad, disgusted, and scared, respectively, on four separate scales (“Please indicate the extent to which you experience each of the following feelings when hearing about IPV”; 1 = not at all, 5 = extremely; α = .63).
Causal attribution
Respondents answered four items about their tendency to attribute IPV to external or societal causes (“IPV is caused by the partners’ external life circumstances,” “IPV is caused by structures in society,” “IPV is caused by cultural factors,” “IPV is caused by the offender’s previous exposure to IPV”). These items, however, showed poor internal consistency (α = .55). Moreover, pairwise correlations among the items were not sufficiently high (rs < .40) to allow the creation of a reliable index variable. Therefore, these items were excluded from subsequent analyses.
Two items addressed internal attributions (“IPV is caused by characteristics of the victim,” “IPV is caused by characteristics of the offender”). However, because these two items were weakly and negatively correlated (r = −.11), victim attribution and offender attribution were treated as separate predictors in subsequent analyses.
Solution responsibility
Respondents rated the extent to which the offender and the victim, respectively, are responsible for preventing IPV (1 = not at all responsible, 5 = very responsible). Offender responsibility and victim responsibility did not correlate with each other (r = −.01) and were treated as separate predictors in subsequent analyses. Respondents made similar responsibility ratings for five groups of actors outside of the relationship (family and close friends, acquaintances, school/workplace, community members, and formal authorities); these items were averaged to form an index variable labeled external responsibility (α = .89).
Perceived prevalence
To measure the perceived magnitude of IPV as a societal problem, we created three items addressing the prevalence of IPV (“The media exaggerate the prevalence of IPV,” “Most people know a victim of IPV,” “IPV occurs more often than most people think”). The first of the three items was reverse scored before the index variable was created (α = .62).
Results
Intercorrelations, means, standard deviations, and range for the main variables are presented in Table 1. Although most of the hypothesized predictors were significantly intercorrelated, the average strength of the correlations was modest, indicating a low risk of multicollinearity when considered simultaneously as predictors of the propensity to intervene.
Intercorrelations and Descriptive Statistics for Propensity to Intervene and Hypothesized Predictors.
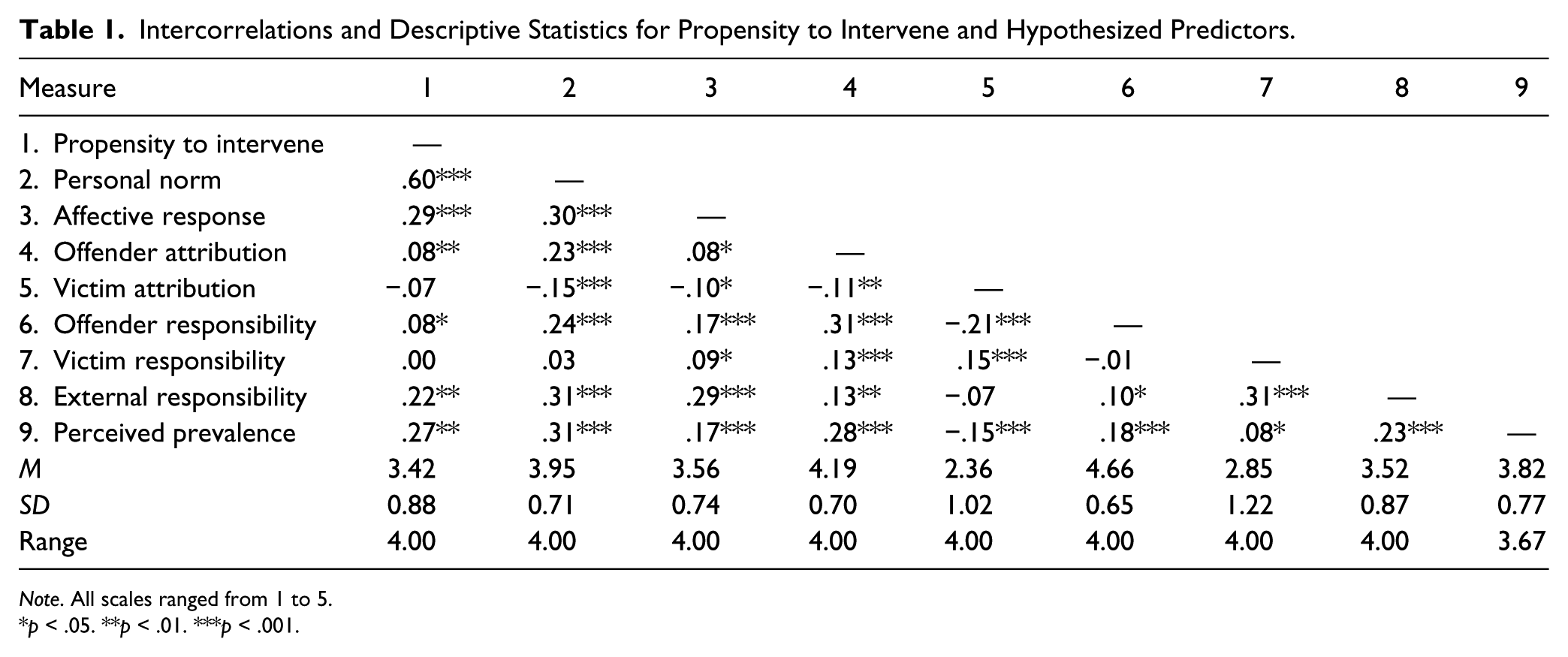
Note. All scales ranged from 1 to 5.
p < .05. **p < .01. ***p < .001.
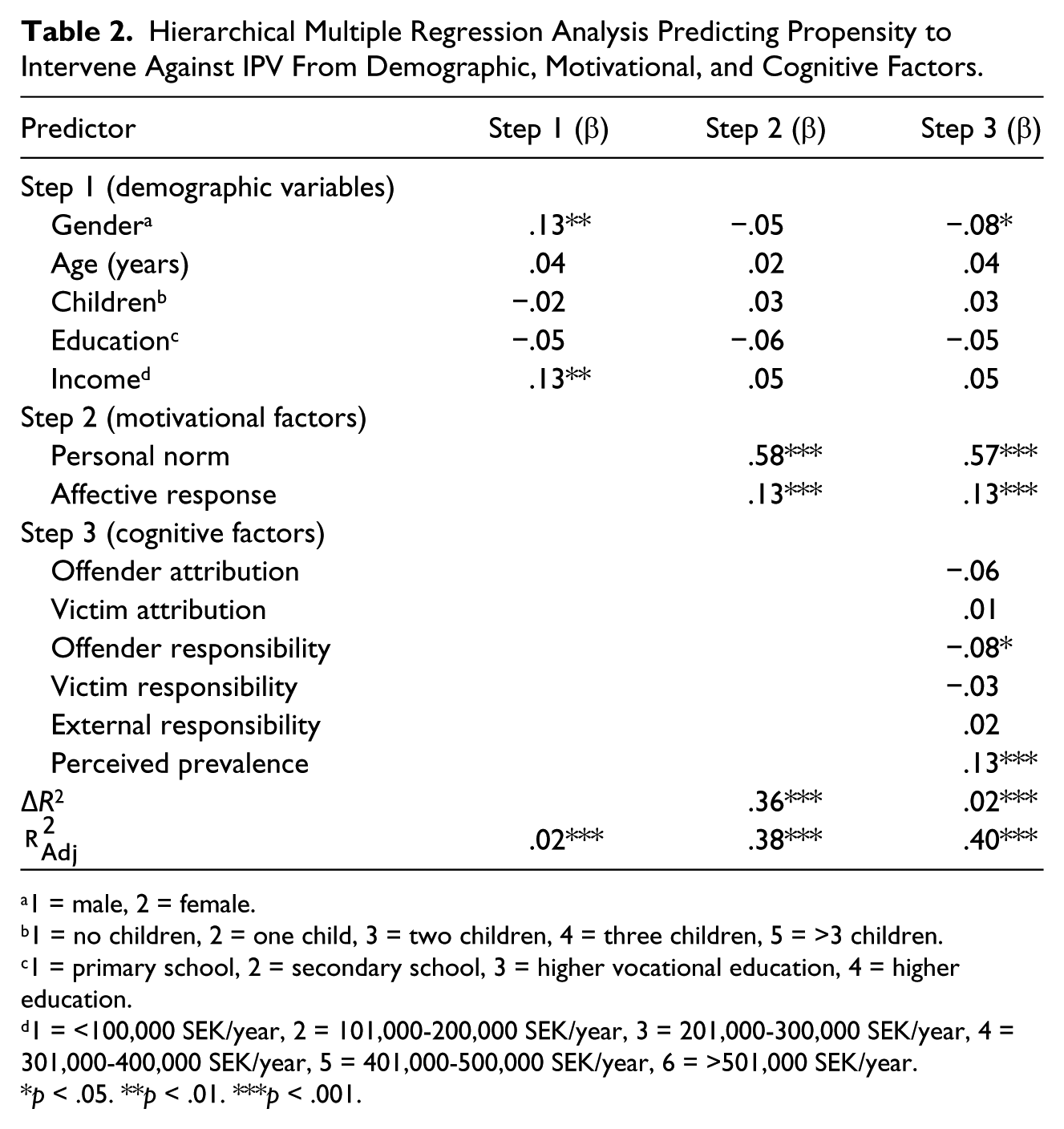
A hierarchical regression analysis was conducted on respondents’ reported propensity to intervene against IPV, with demographic variables entered as predictors in Step 1, motivational factors in Step 2, and cognitive factors in Step 3. The results of the analysis are presented in Table 2.
Hierarchical Multiple Regression Analysis Predicting Propensity to Intervene Against IPV From Demographic, Motivational, and Cognitive Factors.
1 = male, 2 = female.
1 = no children, 2 = one child, 3 = two children, 4 = three children, 5 = >3 children.
1 = primary school, 2 = secondary school, 3 = higher vocational education, 4 = higher education.
1 = <100,000 SEK/year, 2 = 101,000-200,000 SEK/year, 3 = 201,000-300,000 SEK/year, 4 = 301,000-400,000 SEK/year, 5 = 401,000-500,000 SEK/year, 6 = >501,000 SEK/year.
p < .05. **p < .01. ***p < .001.
The demographic variables (Step 1) were entered for control purposes and accounted for only 2 % of the variance in the propensity to intervene,
The addition of motivational predictors (Step 2) led to a large and significant increase in explained variance, ΔR2 = .36, F(2, 643) = 190.38, p < .001. Both respondents’ personal norm and affective response came out as significant unique predictors. The stronger the perceived personal obligation to intervene, and the stronger the negative affect felt in response to IPV, the more respondents were inclined to intervene against IPV.
With the addition of cognitive factors (Step 3), there was a small but significant increase in explained variance, ΔR2 = .02, F(6, 637) = 3.97, p < .001. Of the variables entered at this stage, offender responsibility, B = −.10, SE = .05, p = .023, and perceived prevalence, B = .15, SE = .04, p < .001, served as significant unique predictors. Hence, a weaker tendency to perceive the offender as responsible for solving the problem and a stronger tendency to view IPV as a major problem were associated with a higher propensity to intervene. The coefficients for personal norm, B = .70, SE = .04, p < .001, and affective response, B = .16, SE = .04, p < .001, remained highly significant.
Moreover, gender emerged as a significant predictor, B = −.14, SE = .06, p = .027; controlling for all other predictors, being a woman as opposed to a man was associated with a lower propensity to intervene. The final model explained about 40% of the respondents’ variation in the propensity to intervene against IPV,
Discussion
The results of the current study showed that both motivational and cognitive factors were significantly related to respondents’ self-reported readiness to take intervening action against IPV. The full predictor model explained 40% of the variance in reported propensity, illustrating the high relevance of the selected predictor variables. Motivational factors accounted for most of the explained variance, indicating that these may be especially important to consider in future attempts to increase public IPV intervention. We now turn to a discussion of the individual factors identified as significant predictors.
The strength of respondents’ personal norm endorsing intervention was the single strongest predictor of the propensity to intervene. This result mirrors findings from research on prosocial behavior, showing that people generally act in the interest of others when such behavior is prescribed by internalized values (Schwartz & Howard, 1984). In the current study, personal norm was operationalized as an individual’s perceived obligation to intervene and the anticipated bad conscience that would result from a failure to intervene. It thus appears that moral considerations are a key to understanding individual differences in intervention propensity. Strategies targeting precursors of personal norms may prove effective to increase public intervention. For instance, because personal norms often develop through the internalization of social norms (Fiske, 2004; D. T. Miller & Prentice, 1996), increased interpersonal communication about IPV intervention may influence individuals’ personal norms and, in turn, their propensity to intervene.
The extent to which respondents experienced negative emotions when confronted with IPV came out as the second strongest predictor of intervention propensity. This result resonates well with previous findings that negative affective responses can promote helping behavior (Cialdini et al., 1987; Manucia et al., 1984; but see C. Miller, 2010, for exceptions). Possibly, our respondents saw intervention as a means of reducing the emotional discomfort produced by IPV, as would be predicted by the negative state-relief model (Cialdini et al., 1987). It is also possible that our measure of negative affect is served as a proxy for perceived personal relevance of IPV; the issue may be more emotionally charged for individuals who feel more personally affected. High personal relevance, in turn, is reliably associated with an increased tendency to act in accordance with one’s beliefs and attitudes (Zuwerink & Devine, 1996). Regardless of the underlying mechanism, our findings suggest that public intervention against IPV may be facilitated by affectively rich information appeals, such as vivid illustrations of IPV cases or information about the emotional impact of IPV on victims.
Two cognitive variables came out as significant predictors in our analysis. It should be noted, however, that these variables explained a substantially smaller portion of the variance than did motivational factors and should be interpreted with greater caution. Respondents who perceived IPV as a prevalent problem reported, as expected, a higher propensity to intervene than did respondents who made low prevalence estimates. Thus, the importance of prevalence beliefs is supported both by prospective reports of behavioral intentions (i.e., the current study) and by retrospective reports of actual behavior (Beeble et al., 2008). Given the tendency of media portrayals to focus primarily on extremely violent cases of partner abuse (Manganello, Webster, & Campbell, 2006), it is possible that many people underestimate the prevalence of less extreme and more common forms of IPV. Hence, information campaigns providing concrete statistical details on the frequency of IPV in an accessible fashion (e.g., “X out of 100 persons have been verbally, sexually or physically abused by their partners”) may be effective to increase the likelihood of public intervention.
In line with expectations, the tendency to view the offender as responsible for resolving IPV was negatively related to respondents’ propensity to intervene. Unexpectedly, however, no significant relationship with propensity to intervene was found for ascriptions of responsibility to the victim or to external agents. It may seem that, by isolating responsibility to the offender, respondents were able to reduce the responsibility ascribed to themselves and to other external agents. This explanation, however, is at odds with the fact that offender responsibility was weakly positively (rather than negatively) related to the measure of external responsibility. Instead, it may be that offender responsibility is particularly salient when people form IPV intervention intentions, and that the perceived responsibility of the victim and external actors is seen as relatively less relevant. Further research is necessary to understand the complex role of perceived solution responsibility in public responses to IPV.
The current study contributes with knowledge about what facilitates or inhibits individuals’ propensity to intervene against IPV. Such knowledge may be useful when designing information campaigns to increase public awareness and victim-supportive responses. Previous research indicates that customized persuasive attempts, attuned to the values and goals held by the target audience, are more successful than attempts to persuade a general audience (Lewandowsky et al., 2012; Noar et al., 2007). Hence, depending on what constitutes the main psychological barrier to intervening against IPV, different individuals may be receptive to different types of information. For instance, individuals who are kept from intervening because they underestimate the frequency of IPV cases in their social environment may benefit from information about the actual prevalence of IPV in society. In contrast, individuals who fail to intervene because they see the offender as the primal problem solver may be more responsive to information about authentic IPV cases that have been successfully prevented by external and public interventions. Future research should develop instruments that can reliably classify individuals according to their major psychological barriers and, subsequently, elaborate information strategies addressing specific barriers.
The identified predictors in the present study may have implications not only for intervention but also for the prevention of IPV. If public intervention can be increased by addressing behavioral predictors, the intervention is likely to translate into a collective standpoint that condemns IPV. This paves the way for the formation of social norms proclaiming intolerance to violence. Such social norms may have preventative benefits, because they signal to victims and perpetrators that violence is unacceptable and entails social retribution.
A few limitations of the current study should be noted. First, propensity to intervene was assessed by asking respondents to estimate their future responses to IPV. Such self-reports are associated with a number of potential error sources, such as social desirability and memory unreliability (Krosnick, 1999). Thus, it is unclear to what extent respondents’ reported intentions would correspond with their actual behavior in response to authentic IPV incidents. Intention–behavior consistency has, however, been thoroughly examined in other behavioral domains (e.g., consumer decisions, health-related behaviors, academic achievements) and the bulk of evidence indicates that intentions are generally quite predictive of subsequent behavior (Sheeran, 2002). Hence, self-reports were deemed adequate as a measure of propensity in the current study. In addition, direct measures of intervention behavior (e.g., observation) raise a number of ethical issues and are impractical for studying large, community-based samples. The survey methodology is a common strategy to avoid these issues. A second limitation relates to the fact that all predictor variables were considered in direct relation to the propensity to intervene. We may, therefore, have overlooked more complex patterns and indirect paths. One possibility is that some predictors precede others in a causal chain. For instance, a personal norm endorsing intervention may develop as a result of various cognitive considerations (e.g., causal attribution, responsibility judgments). Another possibility is that some factors serve as moderators of other predictor variables. For instance, it may be that personal norms are more likely to translate into intervention behavior when accompanied by high (versus low) prevalence estimates. The internal dynamics of predictor variables may be fruitfully explored using advanced statistical procedures (e.g., structural equation modeling) or experimental methods. Finally, the variables in our analyses were measured exclusively with items that were designed specifically for the current study. While this was necessary given the lack of appropriate measures in the literature, our use of unstandardized measures may raise concern regarding the reliability of our findings. This concern can be addressed by future replication attempts.
Conclusions
In this study, we have identified motivational and cognitive factors that may act as determinants of individuals’ propensity to intervene against IPV. These findings contribute to the scientific understanding of the psychological processes involved when people form intervention intentions. Moreover, our findings provide an empirical basis for the development of information strategies aimed at increasing public IPV intervention. Specifically, we have isolated a few predictors of intervention propensity that may be especially relevant to target in future information campaigns. Because such campaigns tend to be more effective if tailored according to the needs of the target audience, fruitful next steps for research would be to develop reliable ways of identifying groups of individuals with different psychological barriers and, in turn, to elaborate focused information strategies addressing those barriers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Swedish Crime Victim Compensation and Support Authority given to the third author.