
Abstract
The aim of this study was to illuminate experiences of the process of recovering from pathological dissociation. The study used data from interviews with six female participants diagnosed with pathological dissociative disturbances. All the women had a history of having been sexually abused. Data were analyzed using Interpretative Phenomenological Analysis (IPA). Two main themes emerged in the analysis: social and relational change and self in movement. The themes mirror the interplay in the recovery process that took place both intrapsychically and with regard to the relational interplay between self and other significant people. The recovery process was dependent on an incipient sense of security in relational interaction, and this process was hindered by insecurity and ambivalence in relationships. Each patient’s relationship with her therapist also played a crucial role for the participants.
Keywords
Introduction
Dissociation is a complex phenomenon, and a plethora of theories surround the term. The different ways of viewing dissociation converge around the idea that dissociation represents a failure or an inability to integrate ideas, information, affects, and experiences (Howell, 2005). This perspective is also formulated in Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994, 2000) and International Classification of Diseases, 10th Revision (ICD-10; World Health Organization, 2007). Pierre Janet was the first person to use and develop the term dissociation, in the late 1800s. He was also the first to describe the association between psychological trauma and dissociation. Howell (2005) and van der Hart and Dorahy (2009) argue that Janet’s use of the term hysteria includes, for instance, post traumatic stress disorder (PTSD), somatoform dissociation, and dissociative dysfunctions. Howell (2005) also mentions the psychoanalyst Ferenczi, who argued that psychological shock could emerge in a relational context. He describes connections between child abuse and trauma and writes about the traumatizing effects of sexual abuse during childhood, as well as the dissociation that can arise from it (Howell, 2005).
During the last 30 years, the term dissociation has been brought to the fore again. Several papers and books presenting theories and research about dissociation and its linkage to trauma, attachment, and neurobiology have been published (Liotti, 2006, 2009; Lyons-Ruth, 2008; Schore, 2009; van der Hart, Nijenhuis, & Steele, 2006). Lyons-Ruth (2008) argues that current research highlights disorganized attachment in a child and lack of emotional presence in the caretaking person as important factors in the development of dissociative disturbances.
In van der Hart et al.’s (2006) model of structural dissociation, the phenomenon is trauma induced and linked to a posttraumatic part of the personality. Structural dissociation involves dissociated parts as trauma avoidant or trauma fixated. van der Hart and Dorahy (2009) describe a broader view of dissociation, understood as a continuum that may comprise the whole personality, ranging from adaptive and normal dissociation (used, to different degrees, by everybody) to extreme pathological dissociation.
Bromberg (1998, 2006, 2009) argues that psychoanalytic theory has moved away from the classical psychoanalytical perspective of the conscious as a separate domain toward an idea of a nonlinear, dialectical process of meaning construction. In this view, the mind is made up of shifting parts that have varying degrees of access to perception and cognition. Using this perspective, the dissociative nonconscious is not viewed as necessarily linked to forgetting over time; different self-states can be considered as subjective realities that alternate, moving between foreground and background.
Pathological dissociation is a serious disorder that may paralyze a person’s ability to function socially and emotionally. Only a few studies of treatment of dissociative disorders are extant in the research literature, and even fewer use qualitative analysis methods in which patients describe their experiences of treatment and recovery (Brand, Classen, McNary, & Zaveri, 2009; Hirakata, 2009; Phanichrat & Townshend, 2010). But such studies may be important for understanding how dissociation can be treated (Brand, 2012).
The purpose of this study was to examine and interpret the ways people diagnosed with dissociation ascribe meaning to their personal experiences of the recovery process, using Interpretative Phenomenological Analysis (IPA) for the analysis (Smith, 2004). The concept of recovery was regarded as an ongoing process rather than a final result (Pitt, Kilbride, Nothard, Welford, & Morrison, 2007).
Method
Participants
The participants were six women who had been diagnosed with a dissociative disturbance according to ICD-10 criteria. The diagnoses included F447, mixed dissociative disorders, and F448, other dissociative disorders. We gained access to the women by contacting colleagues who worked in open psychiatric units with clients who had undergone various types of trauma. The criteria for inclusion in the study were that the women had been diagnosed with a dissociative disorder and that they were in the late stages of their psychotherapeutic treatment or had finished it. Dissociation is a nomothetic term. The study uses the term for identifying a group of persons with severely problematic experiences. Only rarely do the subjects themselves use this concept about themselves.
One participant was between 20 and 30 years of age, four were between 30 and 40, and one was between 40 and 50. Four participants were single, one was married, and one lived with a man without being married. All women had passed high school and several of them had university education.
The women were assigned pseudonyms to ensure confidentiality. An informational letter was sent to potential participants explaining the aim of the study and how the interviews would be conducted. Additional psychotherapeutic support was offered, if needed, after the interviews, and participants were informed that they could stop the interview whenever they wished without offering an explanation. The study followed the ethical code of Uppsala University.
Procedure
The participant interviews were semistructured. The purpose was to allow participants to describe their experiences, thoughts, and feelings in a detailed and thorough way. We followed an interview guide consisting of seven questions and follow-up questions. A vignette was used as a starting point to ensure that the phenomenon we wanted to examine was clear to the participants and that they were amenable to discussing it. The vignette is shown in Table 1.
Vignette for the Semi-Structured Interview.
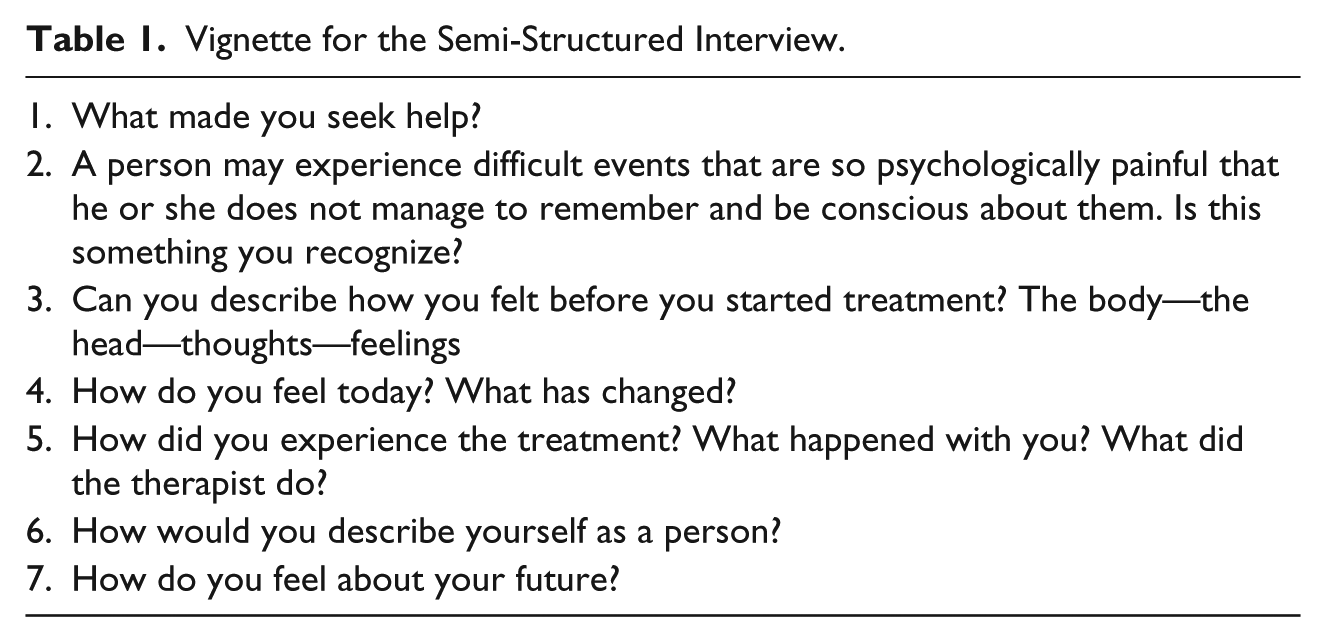
The interviews lasted between 1 and 2 hr each. They were tape recorded and transcribed verbatim, providing about 100 pages of text as a basis for analysis.
Data Analysis
We applied IPA to analyze the interviews. IPA describes each person’s unique experiences, as well as their common experiences; the aim is to examine experiences in a specific group. IPA rests on phenomenological and hermeneutical ideas (Ashworth, 2008; Finlay, 2008; Larkin, Watts, & Clifton, 2006; Smith, Flowers, & Larkin, 2009). The researcher’s active role in the research process as interpreter of the participants’ lived experiences and worldviews is emphasized in IPA. According to Smith et al. (2009) and Reid, Flowers, and Larkin (2005), IPA is linked to interpretative theory in a so-called double hermeneutics in which the researcher tries to understand the participant as he or she tries to assign meaning to the world. The method is idiographic in that it carefully examines every individual on a case-by-case basis before providing statements of a more general nature. IPA is useful when the topic being researched is subjective, relatively new, and process oriented and when questions about identity, the self, and meaning are important (Osborn & Smith, 2008; Shinebourne & Smith, 2009; Smith & Osborn, 2008).
The analysis of the interview statements followed the rules and steps outlined by Smith et al. (2009). As a first step, we read and reread the text to gain an initial understanding of the participants’ experiences and worldviews and to identify structures and connections. Thoughts, concepts, questions, and linguistic observations that came up during the course of the reading were written down. In the next step, we identified important themes of conceptual nature. Interconnected themes were collected into clusters, which were assigned their own headlines. This procedure was repeated for all the interview texts. Next, we searched for patterns and themes in the texts and consequently reevaluated certain themes, moved them around, assigned them different names, and changed their levels. This procedure resulted in a list comprising overarching themes and subthemes that reflected the participants’ experiences. The analysis was presented in a running text supported by carefully selected excerpts from each participant’s statement. The analysis took place first and foremost on a descriptive level and then on a second, more openly interpretative level. Some interpretations were made on a micro level, examining only a few words. Existing theory about dissociation was used in the interpretation of the answers, in accordance with the guidelines that Smith et al. recommend.
Results
Two main themes emerged that reflected the meaning participants assigned to their recovery processes and to their experiences of recovering from dissociation. The main themes were social and relational change and self in movement—themes that capture the women’s experiences of the recovery process. Each theme comprises several subthemes, such as changing environmental and interpersonal relations, the relationship with the therapist, the interplay between peace and chaos in the body and mind, and the shift from splitting to becoming an integrated human being.
This recovery process was described as a time-consuming, ambivalent movement. The level of security perceived in social circumstances was a crucial starting point for building inner security and for beginning to work with previously dissociated experiences.
Social and Relational Change
The results show that the recovery process can be seen as ambivalent and subject to the influence of both external and internal factors, such as relief at reaching a safe environment, the significance of children, and the degree of safety in relationships. The patient’s relationship with the therapist was crucial to recovery from dissociative disorders.
Changing environmental and interpersonal relations
All the women in this study had been physically and psychologically abused and assaulted; all but one had been sexually abused during childhood. They all shared the experiences of having left dysfunctional environments and of having ended relationships in which abuse had taken place. To actually leave the places was described as an important step toward starting the recovery process. The physical safety that leaving generated was a prerequisite for beginning psychological treatment and a process of change. All the women maintained this outer safety while the recovery process was under way, though they did so in different ways.
For some of the women, the physical separation from the abusive relationship was regarded as a step from death to life. For some it became clear that an alternation took place between external safety and inner development. Other people’s actions and capacity to offer support were described by all the women and contributed to their development.
Madeleine stated that the continuous physical abuse she experienced in her relationship led to a physical and psychological impoverishment that culminated during her pregnancy. At that time, the seriousness of her situation became obvious to her. She related an extremely dramatic event characterized by strong affects, mainly sheer fear.
The last time I was beaten up I was pregnant . . . and I managed to get out of it with the help of my daughter. She helped me because I was lying in my own pool of blood that day . . . and I told her that if she could just fetch my bag—she was four years old when it happened—she picked up my handbag; then we managed to hide in a room and lock [the door] so I could call the police.
Madeleine’s pregnancy became an extra motivating force here, as she already knew whom to turn to for help. But when she grasped the feeling of the life growing inside her, the possibility of being exposed to death motivated her to make the choice to request help, albeit by leaning on the four-year-old daughter’s capability to assist. This can be seen as a metaphor for the alternation between internal and external factors that further the change process. The experience that the change and recovery come about alternately was shared by all the participants.
For the majority of the women, the move to safer environments facilitated the process of inner change.
For Mona, moving to a foster home brought her enormous safety. The mother in this family helped Mona to value continuous inner and outer safety: “Safety must be the most important thing in life; safety is when I have a mother, somewhere to live, and friends.”
Living in a secure environment and building a relationship with the mother there allowed Mona to experience safety and confidence in a close relationship. She had amnesia of her former traumatic experience for several years while she lived in that family’s home. Mona felt seen and could trust the mother, who noticed when Mona did not feel well. It seems that the mother became a link between the outer and the inner world. When Mona moved away from that home to go to school, she found she could no longer manage: the memories began to return. And it was the family mother who helped Mona relate her experiences to hospital personnel: “I felt horrible . . . but I had my mother with me.”
Significant others
Significant others seem to have served as a supportive force for the women in seeking and maintaining safety, and relationships with significant others (e.g., children, friends, and new partners) influenced change and inner development.
Half the study participants had children, and all spoke of their love for them. Every woman in the study described her child or children’s importance in her life and mentioned the children’s influence on her decision to end an abusive relationship and leave the destructive milieu. The children became a part of putting words to what had occurred. Maria explained,
It became clear that we needed to go away, me and the children, and the children had said before that they were used to me going around like a zombie—they felt like I just went around doing what I should do.
This quotation makes obvious that the children’s view of a past situation comes first, along with the speaker’s experience of strong feelings of responsibility toward her children and a fear for their safety.
Maria’s, Madeleine’s, and Marit’s children constituted a deeply felt meaning in life for these women, as well as a strong incentive for ending dysfunctional relationships. There was reciprocity in these relationships in that the women gained energy from the children that enabled them to struggle to keep themselves alive and the children safe.
The women shared that others had influenced their development either positively or negatively. These statements underscore the importance of external safety and of disentanglement from destructive patterns in relation to the environment.
Margot, who had no children, described the importance of a safe relationship with her boyfriend when other people, including relatives, made life difficult for her. She said that her boyfriend affirmed her and often understood her needs: “I felt awful, but at least I had my boyfriend around, who made it possible for me to tell my mother things I have wanted to say for years.” There was a difference between Margot’s relationships with members of her birth family and the one she experienced with her boyfriend, a relationship she felt was secure and supportive. She mentioned that her boyfriend had encouraged her by commenting on a change in her voice; she now had more strength when speaking, he said. Margot asserted that this gave her more confidence and more self-respect, characteristics that in turn command more respect from others. It became apparent that several women experienced a need to feel (external) safety with significant others, and a long process seems to be needed before they regain trust in others and in themselves or can look for trust that they have never known. Whether others in their surroundings were supportive influenced the women’s recovery processes.
The relationship with the therapist
Each woman described both treatment and her relationship with her therapist as central to the recovery process. Treatment was described as a time-consuming, nonlinear process marked by ambivalence. Margot called it “absolutely the most difficult thing I have done in my life. At the same time, [it was] the very best thing I’ve ever done.”
Maria emphasized the value of the other, the importance of being able to share with another human being after years of silence and isolation: “It took me time to start talking about it, to get somebody who listened, another human being—only that.” The only here seems to refer to a fundamental need Maria felt to meet and mirror herself in another human being, something that had not been available to her before.
Half the participants gave direct accounts of an increasing ability to reflect that had emerged from the women’s relationships with their therapists. This relationship carried a deeply felt psychological dimension for all the women that had to do with the experience of building and maintaining a safe, close relationship with another human being in which difficult memories could be shared.
Moa had never had a safe relationship before she met her therapist, and for her (as for the other women), a relationship with a therapist built on trust and mutuality made it possible to approach and address dissociated material and to proceed through the recovery process.
Moa described this metaphorically: [The therapist] gave me something like a scene where I could exist, and that was security I needed to let these demons out; it was like that. It seems that the “scene,” located in the imagination—normally where fiction is experienced—became a safe place in which Moa dared to approach her painful memories, which were no longer “real” or tangible. She stated that it took one and a half years before she noticed or truly saw the therapist, as she had perceptions only of the therapy room. She talked about her own inability to experience mutuality and said that this capacity had evolved slowly:
I’ve regarded myself as a person who can’t mirror myself in others, or who doesn’t have the ability to reach out—what I call a silver lining, which is transferred. And she [the therapist]—she is capable of reaching out. So I’ve considered it. But suddenly I’m in touch with another human being, and I think I’ve never been like that before.
The “silver lining” symbolizes an ability to meet and share something with another human being. This thread made of silver became a metaphor for how precious this new experience was to Moa.
All the women in this study discussed the importance of being able to put words to what had happened to them and of exploring it with their therapists.
Self in Movement
The women’s way of looking at the self had changed, and they described a development toward regaining their value as human beings and as subjects. All the women expressed a strong ambivalence regarding the process of remembering that which had been dissociated that had to do with what they might come to know and a fear of what they might remember or discover about what had happened.
The interplay of peace and chaos in body and mind
All the women mentioned pathological dissociation as an elusive state, difficult to understand; they shared the experiences of an absence or lack of something and of having removed the self from contact with the world.
Every participant exhibited a personal understanding of this absence. Moa described it as “a break out of memory, falling apart, and not being aware of it.” While Moa’s experience had a physical aspect, Maria’s metaphors deal with more intangible figures, mist and clouds: “The cloud is like memory; it’s nothing I will sort of think about.”
Margot gave voice to the fact that she had a hint about something she did not yet know to the extent that she was able to formulate it—as if she had been in a state of being her own detective, reluctantly uncovering painful memories:
Yes, I am an expert on or have been an expert on suppressing things—yes, to a degree that I have actually not known, so to speak. Or at heart I have known what happened and who it was that hurt me. I have had glimpses, flashes of memories—very rapid—and a feeling about what happened, but I’ve had no memory, real memory, of the episode.
The majority of the women described the dissociative state as an experience of not being able to hold together body and mind, an experience of not remaining in the body. Both Marit and Moa described memories of watching themselves from a distance, as having visual control of something uncontrollable. Marit said, “Some memories are sort of as if I flew up under the ceiling—being above everything and seeing what’s happening. There was no feeling inside myself in the body. Moa said this: I remember the abuse visually from above, near the ceiling, as if I sat in a small corner watching myself down there.” Both Marit and Moa described contemplative a part of themselves, while other women expressed more directly that they had left their bodies. Like Marit, they mentioned that they had no bodily sensation, or that the body did not exist for them.
Most women describing the pathological dissociated state indicated that the longing for it could be as strong as the longing to escape from it. They spoke of a feeling of peace and calm and of being disconnected, separated from physical and psychological pain. Moa said,
I think I’d rather remember myself up by the ceiling than in that body lying there, and I’d rather remember that peace . . . Yes, I unfortunately and unwillingly also remember the other perspective.
This ambivalence apparently serves as protection from distressful feelings; Margot also described it when she spoke of scent memories from the abuse starting to come back:
“What’s happening? Am I going wild?”—and thoughts like that. And also one part of me tried constantly to persuade myself that this never happened—this other part, the scared part that doesn’t want this to be true.
The ambivalence can be understood as an inner insecurity about whether one wants or has the ability to examine what had happened. Margot’s statement shows the way she experienced different parts of her that could not cooperate. Her use of the words going wild indicates a fear of losing control, going mad, an experience that was shared by half the participants, who explicitly expressed a state of chaos when the memories surged. Marit gave voice to this as follows:
There was no controlling how the memories came back. Then I was not in the here and now; I was transferred to a time when I was a child. So I lost, in a way, both time and space . . . You lose the concept of time and of everything—suddenly you are just thrown back to something you don’t want to remember . . . which was also upsetting.
This statement indicates that linear time breaks up and the division between now and then disappears.
From split to unity: Becoming human
The women’s views of themselves contained descriptions of “not being,” of not experiencing the self as a subject, as a human being. The recovery process involved ambivalence and insecurity regarding identity and human dignity, and fear was a prominent affect. Madeleine said,
I felt totally worthless as a person. I felt—I felt that I was worthless. I didn’t fully know who I was. I felt mixed up. I felt like I was down in a huge deep hole, and I tried to escape, but I never came up. I felt I was thousands of meters below ground and I couldn’t see the light of life. I had no hope at all; everything was black for me.
But this feeling that she had been buried alive or was not truly alive changed, and Madeleine also related that her self-confidence had slowly started to return, though she remained ambivalent: “I don’t think I will ever be whole as a person again.” Her thoughts mirrored a deeply felt human despair and helplessness; as she spoke, she held on to the word I almost as a means of not losing herself.
Regaining human dignity seems to involve eradicating an experience of objectification and of existing only for the fulfillment of others’ needs, mostly as a sexual object. Marit described her experience of this development:
Then if I felt bad or not, it was like the same shit—it was only me. It didn’t matter. Yes, I was only a product in a way. I was only to be consumed, and that was what I was meant for—being used and abused.
Some women used metaphors to put words to their experiences. Maria said, “I was like a zombie, you could say I felt like a mitten.” Moa remarked, “It has made me a survivor instead of being stone dead.” Descriptions of oneself as a “zombie” or “stone dead” can be seen as metaphorical references to another possible death in connection with abuse. Talking about being dead in connection to the abuse allows an interpretation of a different kind of death—a death of the soul that is the price of physical survival.
All the women except one indicated that the affect fear had influenced them most in life and had contributed to their pathological dissociation. For the majority of the participants, fear imbued life. But they also related that increasing insight and awareness during their treatment had reduced the fear. As Margot said, “It’s very important, I have found out, to understand. Because when I understand my own reactions I am less afraid; I become more aware, and that helps a lot.” Margot’s fear was also reduced when she was able to identify the perpetrator; she said, “The demon has now got a face.”
Marit talked about affects as different parts of her inner self and discussed the ways anger, sorrow, and fear related to one another. She described this as follows:
The sorrow about what had happened—at that moment it was just sadness—was naturally very afraid of meeting anger about what had happened, because the sad part was also afraid that if she met anger, anger would blame her for what had happened.
It seems that Marit needed to separate the affect fear—otherwise, she would have felt more guilt. Marit later related that with increased understanding she could feel that her own guilt decreased.
Half the women discussed guilt. Marit also explained the ways that her feelings of guilt changed as the recovery process proceeded; she indicated that the contact between and awareness about different affective states increased: “They know each other . . . I have more understanding about why I did as I did . . . All the parts realize that they have had one part each, so I should survive.”
During the interviews both Margot and Moa were reminded of their former split, dissociated state, although they both had proceeded well in the process toward greater unity of the self: Margot noted, “Now I get a black out . . . When we talk about it I feel that I become as I was then.” And Moa said, “I am stressed and have stomach pain, or stress . . . When I sit here I go back; I’m squeezing my throat closed.” They were both aware of what was happening to them and were able to put it into words and relate to the experiences during the remainder of the interview.
Discussion
The aim of this study was to investigate the recovery processes of women who had dissociative symptoms. The women reported that both the origin of dissociation and the recovery from it took place in relationships. All six women had experienced trauma in childhood and in many cases also during adulthood. Analysis of their answers indicated that the way to recovery was a complex, time-consuming process that took place both internally and in external relational interaction between the self and others. An important finding is that safe relationships comprise an important condition for recovery.
The concept of dissociation has in recent years been used in a more expanded way than in the past. A number of authors in the psychoanalytic-relational tradition have used the concept as an alternative to the traditional intrapsychic conflict model, in which conscious experiencing is contrasted with dynamically repressed psychic content. This usage opens the way for a more detailed understanding of complications in the interplay of different self-states. Bromberg (2006, 2009), for instance, argues that in the process of increasing the individual’s self-reflective stance, a dialectical process may develop between dissociated and nondissociated mental content, leading to an increased capacity for a secure experience of what was before too painful to revisit.
The relational view of recovery from dissociation emphasizes the importance of the therapeutic relationship (Chefetz, 2009; Herman, 1992). The women in this study stressed the central function that secure relationships with others had in their recovery processes. Significant others and therapists were crucial in this process. The women needed trust others to develop their own inner trust and capacity for interaction. This trust also made it possible for them to approach painful memories.
Pearlman and Courtois (2005) emphasize the therapist’s contribution to building an adequately safe relationship. They argue that the therapist, through affect attunement and by engaging with the patient in relational repair, can contribute to an intersubjective growth in the long term. Through a relationship with the therapist, the work on dissociation can become a vehicle for experiencing and developing ways of naming feelings, for understanding them and tolerating them. The individual experiences less chaos when he or she understands and develops the capacity to differentiate emotions and reactions. This facilitates understanding the context of what was previously impossible to understand because it was fragmented and dissociated.
The importance of being human in the face of trauma and of being relieved of the feeling of being an object, described by Togashi and Kottler (2012), became obvious in this study. The women described their gradually increasing sense of subjectivity.
The concept of “mentalized affectivity” (Fonagy, Gergely, Jurist, & Target, 2002; Jurist, 2005, 2010) involves the way that an individual not only experiences the affect but also integrates it into his or her life history. Learning to mentalize affects depends on the way key attachment figures model this capacity. One of the study participants, Marit, described the inner change that took place during the therapy process in which affects were revalued, not only modeled. She observed that the affects, especially fear, were transformed and could take on new, adequate, and constructive meanings that better served her own interests. She talked about walls that had become lower and indicated that different inner parts now knew each other and were less afraid. She also mentioned a sense of keeping all the different parts inside, saying that they now existed side by side.
The women expressed ambivalence regarding the recovery process that occurred both internally, between body and mind, and externally, in the relational interaction between self and other. This development seems to have been unpredictable and was dependent on a sense of security in the relationship. Harris (2009) argues that development occurs in an unpredictable fashion, alternating between complexity and simplicity. Like Bromberg (2006, 2009), she argues for a nonlinear system in which development takes place through a progressive integration where complexity is created, shaped, and reorganized at higher levels.
Margot indicated that her inner ambivalence meant that one part of her understood what had happened while another, more frightened part tried to convince her that it had not occurred at all. During the recovery process, the part that understood and knew that the abuse had taken place grew, and at the same time the fearful part was reduced. This process was arduous and unforeseeable. Margot experienced the treatment as both the most difficult and the most rewarding thing she had ever done.
The women did not describe themselves as cured; rather, they expressed an increasing ability to hold their experiences in their consciousness. They were reminded in different ways of past states that occasionally and temporarily came into the foreground, states that were not fully accepted but could be harbored in consciousness. Pathological symptoms returned during their interviews for several women, but it seemed that they had come so far in the recovery process that they were able to reflect on, verbalize, and share what was happening to them. The women’s experiences seem to illuminate an understanding of dissociation shared by Bromberg (2008) and Howell (2005, 2011) as a continuum that stretches from an adaptive and normal dissociation to extreme pathological dissociation.
The women who were interviewed in this study had all lived in abusive relationships, and their dissociation resulted from the relational violations that they had experienced. The psychotherapies that they were offered were predicated on the idea that new relational experiences could in some way compensate for their suffering. It is important that future studies of patients who recover from pathological dissociation incorporate an understanding of both the potential and the limitations of reparative experiences in a therapeutic relationship.
The experience of mental states that are called dissociation in the psychiatric diagnostic literature and recovery from them is a process that is immanently unique for each person. In this study, six women’s voices about such experiences have been described. To summarize these individual women’s ways to more meaningful lives by using nomothetic terms makes in some sense violence to their uniqueness. It is important to emphasize the variation in the ways that they experienced their treatment trajectories.
An important limitation of this study is its generalizability, which as in all qualitative studies should be considered in conceptual terms. The participants’ different abilities to verbalize their experiences and to describe dissociative states can also be seen as potential problems. As always, an IPA study is judged by the reader in terms of the connection between its results and his or her own professional thoughts, theories, and experiences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.