
Abstract
The abuse of individuals with disabilities is a widespread problem that has received minimal attention in scholarly research on intimate partner violence (IPV). As a result, the literature offers neither a general demographic profile of IPV survivors with disabilities nor an examination of the relationships between IPV and individuals with specific types of disabilities. This article addresses these gaps by reporting the results of a retrospective case study review of 886 client files, covering an 8-year service period in a non-residential domestic violence disability program. The study examined key demographics along with familial, social, and contextual aspects of IPV among women with disabilities, and provides crucial information for service providers who must understand the multifaceted and unique needs of survivors. Findings are discussed in terms of their relevance to abuse-related outcomes and corresponding best practices with this population.
Intimate partner violence (IPV) affects women and men of varying cultural, ethnic, socioeconomic, and familial backgrounds. These identifying factors shape both the resources available to address IPV and the actions a survivor takes in response to abuse. Effective service provision requires a thorough understanding of these factors and their unique presentation for each survivor. This study examined the diverse demographic backgrounds of women with disabilities who sought assistance for issues related to their experiences of IPV from an agency working exclusively with this population.
Early research on IPV against women with disabilities established prevalence rates, risk factors for abuse, types of disability-related abuse, and the range of perpetrators (e.g., Milberger et al., 2003; Nosek, Howland, Rintala, Young, & Chanpong, 2001; Saxton et al., 2001; Young, Nosek, Howland, Chanpong, & Rintala, 1997). For example, it is now well established that women with disabilities are more likely to be abused than both women without disabilities and men with disabilities, and for longer periods of time (R. B. Hughes, Lund, Gabrielli, Powers, & Curry, 2011; Nosek et al., 2001; Smith, 2008). Furthermore, women with disabilities are more often subject to severe forms of physical abuse, including being kicked, punched, or bitten (Brownridge, 2006), yet also experience subtle forms of abuse exploiting aspects of disability, such as withholding medication or denying needed supports (Lund, 2011). The most common perpetrators of violence are former or current intimate partners (Young et al., 1997), but family members, caregivers, personal assistants, and medical providers also may be perpetrators (Curry et al., 2009; Milberger et al., 2003).
An important limitation of the current literature on IPV and disability is the absence of data from diverse samples of women. A literature review of 21 major studies on this topic noted the underrepresentation of women of color (R. B. Hughes et al., 2011). While demographic characteristics do vary geographically, and sample populations are often reflective of the areas in which research is conducted, their significance has nonetheless been largely unexplored. Acknowledging diversity further entails exploring the range of similarities and differences among women based on disability type. Literature on violence and women with disabilities has included a range of disabilities in study samples, yet generally fails to examine abuse among specific disability groups (R. B. Hughes et al., 2011), particularly among women with physical or sensory disabilities (K. Hughes et al., 2012). In general, women with disabilities are often further disadvantaged by structural inequalities related to race, gender, socioeconomic status, sexual orientation, and age (Ortoleva & Lewis, 2012). Explorations of the ways diversity and disability-specific factors may affect the experience of abuse for women with disabilities are essential for ongoing knowledge and skill development. A critical first step is the determination of a demographic profile of women with disabilities who were able to access support services for IPV.
Method
This retrospective study examines the client files of female survivors of IPV with disabilities who received services from Barrier Free Living, Inc.’s disability-specific non-residential domestic violence program, the Secret Garden.
Definition of IPV and Disability
The criteria used to determine disability and the definition of IPV are based on those utilized at the agency. At the time of agency intake, clients provided medical documentation and/or self-reported a disability diagnosis. Using standards set by the Americans With Disabilities Act (1990, P.L. 101-336), the agency defines disability as “a physical or mental impairment that substantially limits a major life activity” (Sec. 12102, para. 1). Beginning with this umbrella definition of impairment, the Secret Garden further categorizes disability as physical, psychiatric, developmental, or sensory. For the purposes of this study, physical disabilities encompass mobility disabilities and illnesses affecting physical functioning, such as a heart condition; mental illness is categorized as psychiatric disability; developmental disabilities include chronic physical and/or mental conditions affecting an individual prior to the age of 22, such as autism or mental retardation (Developmental Disabilities Assistance and Bill of Rights Act of 2000, P.L. 106-402); sensory disabilities comprise those disabilities affecting the sensory functions of hearing and seeing.
The Secret Garden uses standards established by the New York State Coalition Against Domestic Violence (2011) to define IPV which states that domestic violence entails “physical, sexual, psychological, disability-related, and economic abuse, and is perpetrated by one person against their intimate partner. Domestic violence can also be perpetrated by and/or against a member of the same family or household” (para. 1). Because some individuals with disabilities utilize personal assistance services or require aid from medical professionals on an intimate basis, we included these providers as potential perpetrators of IPV. This is consistent with several empirical studies (Curry et al., 2009; Milberger et al., 2003; Nosek, Hughes, Taylor, & Taylor, 2006) and more accurately reflects a comprehensive definition of IPV against individuals with disabilities.
Study Population and Setting
Secret Garden, located in New York City, is one of few programs nationwide dedicated exclusively to serving survivors of domestic violence with disabilities. Clients may be self-referred or referred from outside service agencies. Client eligibility criteria include the following: (a) current or previous experience of domestic violence, (b) a diagnosed or self-identified disability, and (c) a minimum age of 16 years.
Data Collection
Data collection commenced in January 2010 upon receipt of Columbia University Institutional Review Board approval. In adherence with the Health Insurance Portability and Accountability Act of 1996 (P.L. 104-191), the Secret Garden destroys client files after a case has been closed for 7 years. Therefore, client files opened during the service period spanning January 2002-December 2009 (N = 1,056) were included for review. Of these client files, 81 were damaged during a series of floods at the facility over the study period, 70 addressed male survivors of IPV with disabilities, 1 referred to an individual who identified as transgender, and 18 did not include information on the client’s gender. The aforementioned cases were excluded from analysis; this study focuses on the remaining client files of female survivors of IPV with disabilities (n = 886).
Relevant information covering nearly 100 variables was extracted from various records within client files (e.g., psychosocial intakes, mental status exams, progress notes, hospital records, police reports). Variables included in the current analysis are as follows: age; race/ethnicity; country of origin; type of disability; marital status; employment status; whether client had children, and if so, with whom; history of physical and sexual abuse; utilization of police, medical services, and order of protection; and relationship with the abuser.
Data Analysis
Data analysis was conducted using SAS 9.2. We report frequencies and percentages for all outcomes. Percentages represent the percentage of available responses for each reported item. Because the amount of missing data varied across items, we report the frequency representing each percentage for each response. For tests of association between two categorical variables, Pearson’s χ2 test of independence was used to examine whether the variables were independent of each other.
Results
Please refer to Tables 1 and 2 for detailed results. Main results and their implications are highlighted in the discussion section. Notable findings regarding demographic characteristics, marital status, children, past history of abuse, and additional psychosocial factors are discussed. The impact of disability type is explored for relevant variables.
Sample Demographic and Psychosocial Characteristics.
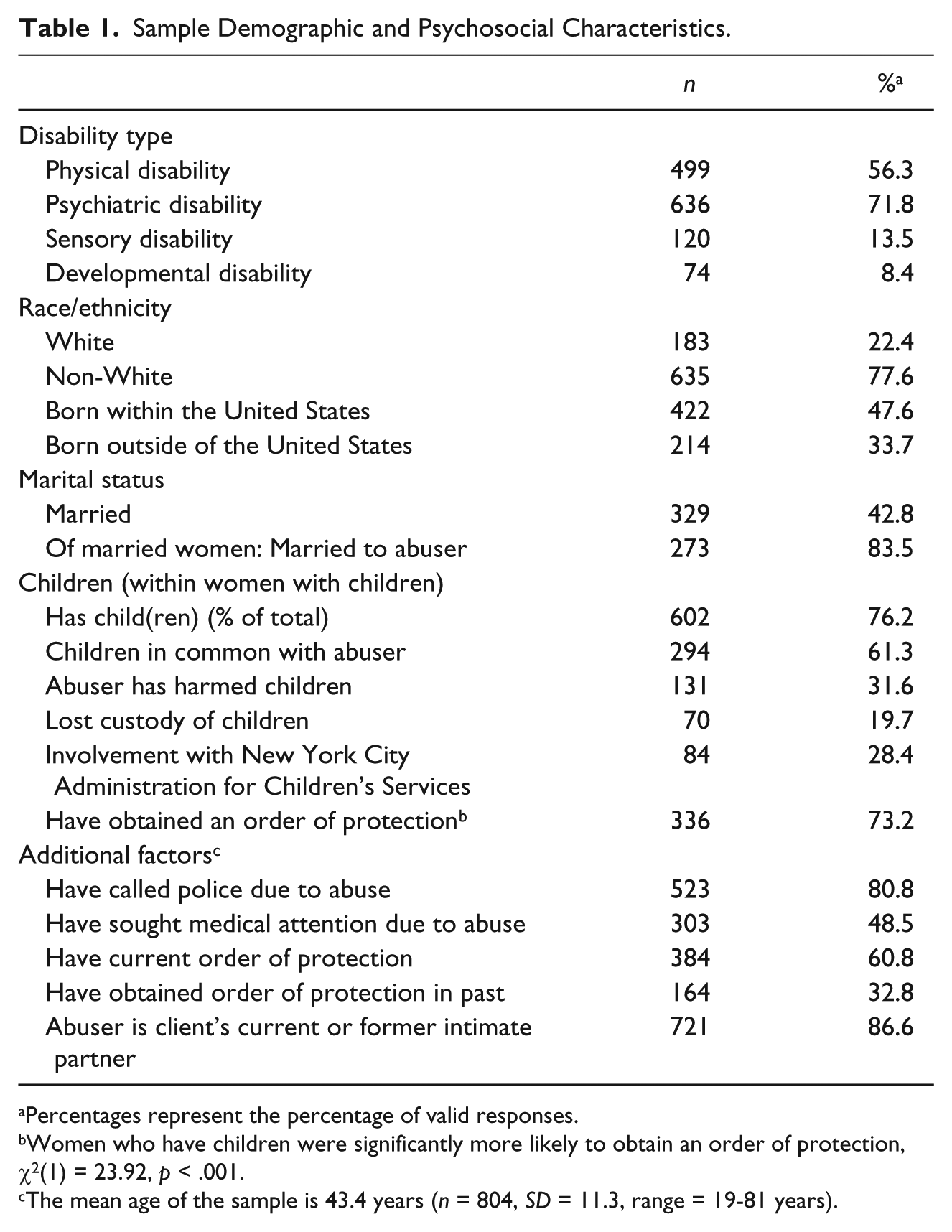
Percentages represent the percentage of valid responses.
Women who have children were significantly more likely to obtain an order of protection, χ2(1) = 23.92, p < .001.
The mean age of the sample is 43.4 years (n = 804, SD = 11.3, range = 19-81 years).
Shared Similarities and Differences Within Disability Type.
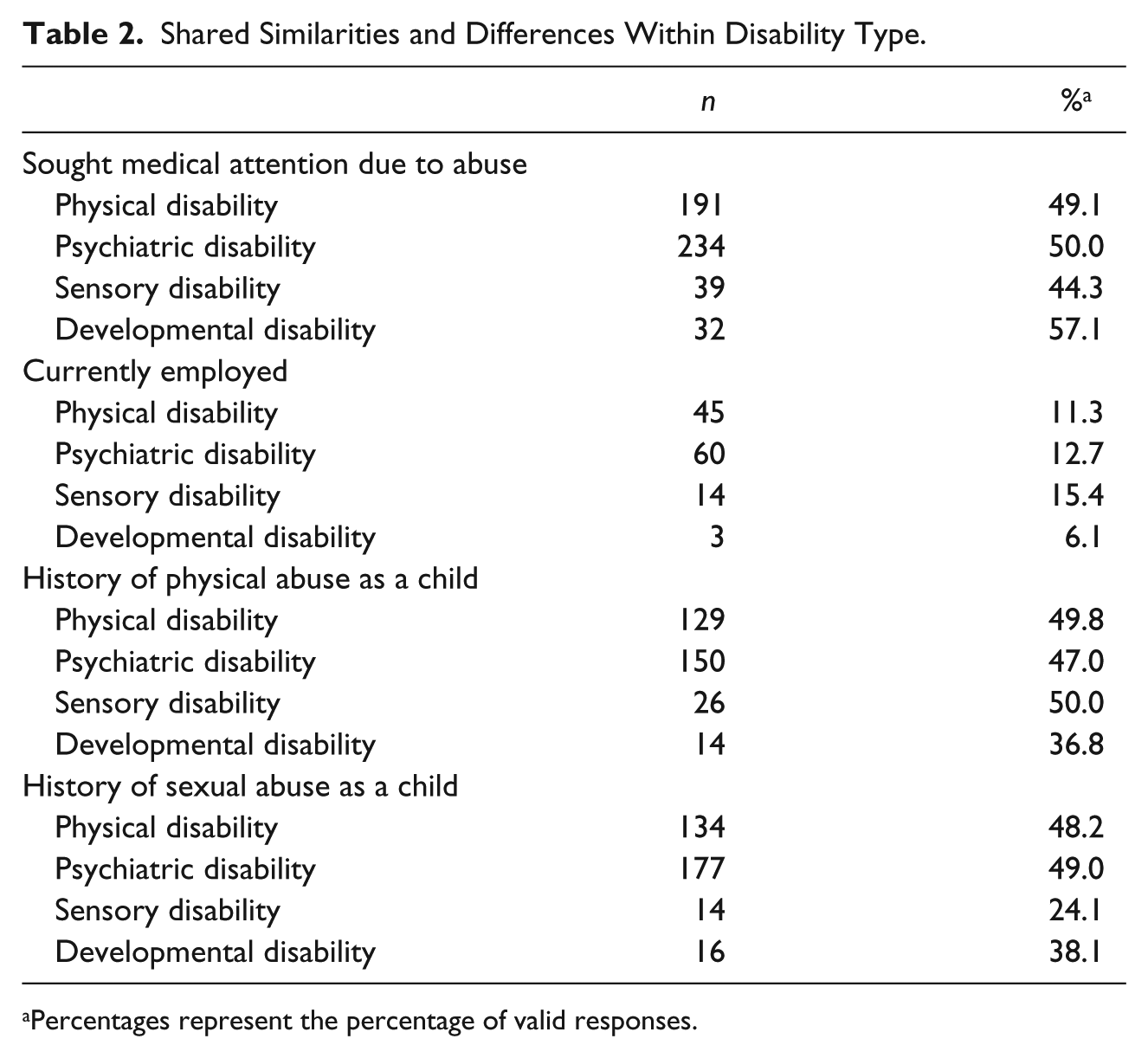
Percentages represent the percentage of valid responses.
Discussion
The findings illustrate the extent to which women with disabilities are diverse socially, culturally, and demographically. Each woman’s assessment, intervention, outreach, safety planning, and criminal justice needs are shaped by her disability profile. Accordingly, meaningful social work-related services must consider not only aspects of identity that have been long recognized for their importance (e.g., race/ethnicity, sexual orientation, immigration status) but also the full range of modifications required to ensure equal access across disability types.
Women of color comprised the majority of this sample. Previous research focusing on Caucasians with disabilities likely excludes countless women who have sought assistance. Furthermore, a significant proportion of the sample was born outside of the United States. This diversity reflects the larger population of New York City from which the sample was drawn. For instance, 36.9% of New York City’s residents are foreign born, and 56% are non-White (United States Census Bureau, 2010). In areas with diverse international populations like New York City, women with limited experience in the United States may need assistance with a range of issues, such as immigration, navigating a foreign criminal justice system, and contending with cultural bias.
In this sample, the most common perpetrators of abuse were intimate partners. This finding debunks the stereotype that women with disabilities are asexual or undesirable as intimate partners, a belief that has fueled the failure of IPV service agencies and researchers to acknowledge IPV among women with disabilities (Mays, 2006), and offers a clear direction for improving IPV interventions. If a woman is dependent on her intimate partner for assistance with activities of daily living (ADLs), reporting abuse could result in the loss of the individual responsible for helping her meet her most basic needs. In addition, a woman’s fear that leaving the relationship will lead to further isolation is an obstacle to successful separation and safety planning. A practitioner may assist survivors in establishing plans for backup care, provide guidance on hiring and managing those who assist them, or facilitate achievement of new skills or skill levels (e.g., using adaptive equipment for cleaning and cooking) that will decrease their need for support from others for ADLs (Saxton et al., 2001).
The number of women in the sample who were married or had children also challenges stereotypical portrayals of women with disabilities as single and childless (Mays, 2006). Almost half were married, and two thirds had children. IPV interventions must consider the needs of these women as spouses and mothers. Legal advocacy may be warranted to assist with divorce or custody proceedings. The possibility of losing custody of one’s children is a great deterrent to reporting abuse among women with disabilities, as perpetrators may erroneously claim that disability negatively affects parenting ability (Ortoleva & Lewis, 2012). On the other hand, having children may prompt a woman with disabilities to take steps to address abuse she is experiencing. The finding that women with children were significantly more likely to obtain an order of protection than women without children raises the possibility that mothers may be moved to seek assistance to protect their children. Practitioners should comprehensively address various options and potential outcomes with clients.
Nearly half the sample had histories of childhood physical or sexual abuse. Women with physical and sensory disabilities were more likely to be survivors of childhood physical abuse; women with psychiatric disabilities were more likely to be survivors of childhood sexual abuse. The disparity of abuse rates across disability groups in this sample suggests the extent to which a woman’s experience of IPV may be shaped by disability status and highlights an important area of further inquiry. Many worthwhile questions remain unexplored. For instance, are women with physical and sensory disabilities more likely to experience childhood physical abuse because the barriers to reporting abuse made it difficult to access help? Did abusers target these groups because of their perceived vulnerability? Likewise, do women with psychiatric disabilities develop mental health conditions such as post-traumatic stress disorder as a result of childhood sexual abuse, or does psychiatric disability precede the childhood abuse? Discovering answers to these critical questions is impossible when women with disabilities are treated as a homogeneous group in research on IPV.
Almost 72% of this sample was diagnosed with a psychiatric disability of some type, and the majority of women with physical disabilities also had a psychiatric disability. However, less than half of all safe homes, shelters, and transitional housing services in the United States provide mental health services to survivors of IPV (Douglas & Hines, 2011). Agencies addressing IPV, particularly those serving women with disabilities, must offer comprehensive mental health services. This unmet need warrants immediate attention. Untreated mental illness further compromises a woman’s ability to respond effectively to abuse and other unsafe situations (Hoog, 2004). Likewise, a woman’s ability to respond effectively to abuse is influenced by her economic status, which is often connected to employment status (Smith & Strauser, 2008). Few women in the sample were employed, with a range of only 6% to 15% reporting current employment at the time of contact with the Secret Garden. Findings are consistent with research indicating women with disabilities who have experienced physical and sexual abuse are more likely to be unemployed (Smith & Strauser, 2008). While the direction of the relationship between past abuse and unemployment is not clear, this finding indicates the need for vocational and financial assistance for survivors of IPV with disabilities. Moreover, it guides practitioners to consider the additional needs such as permanent housing and accessible affordable health care accompanying unemployment and low socioeconomic status among women with disabilities who have experienced IPV.
Limitations
The data examined in this study were originally collected by social workers at client intake and were intended for internal agency monitoring of clients’ service needs. As is the case with all secondary analyses, we had to contend with the limitations of the original data including incomplete case notes and psychosocial assessments. Variables were sometimes defined or categorized differently than the researchers would have chosen, thereby altering the questions we sought to answer. Missing information within client files for certain variables was the largest limitation. A number of potentially informative variables had to be dismissed due to missing information across a large number of files. These included variables such as the individual’s highest level of education, duration of IPV, and frequency of various types of IPV. Such variables would have enhanced our understanding of survivors of IPV with disabilities and added to our recommendations for best practices with this population. Finally, our sample included only the client files of women with disabilities who had sought assistance for IPV. Information about women who are unable or choose not to access such services is also worthy of exploration.
Directions for Future Research
The study findings present a multicultural profile of women with disabilities who have sought services for issues related to their experiences of IPV. Additional research should use diverse samples to develop and empirically validate interventions for survivors with disabilities. Currently, IPV interventions used with the general population include crisis intervention, safety skills promotion, connection to information and resources, and long-term individual and group counseling. Despite assertions that intervention methods should address the interplay of disability, abuse, and related psychosocial dimensions (Copel, 2006), the potential utility of these interventions with women with disabilities remains unexplored.
Conclusion
Women with disabilities are a population of unique individuals with multifaceted needs, desires, and strengths. Research that does not recognize and explore this heterogeneity will yield practices and programs that fail to address important social, environmental, and political implications of race, marital and parental status, and disability type. This study is the first step in a line of research aimed at uncovering the demographic and disability-specific factors influencing the needs and actions of survivors of IPV with disabilities. These findings, in turn, can be used to inform the development of culturally sensitive, evidence-based interventions for this vulnerable population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The Loreen Arbus Foundation has generously provided funding to assist with the analysis and dissemination of the research detailed in this article.