
Abstract
The article presents the results of a study on the relationship between exposure to (i.e., witnessing and experiencing) different patterns and types of family violence during childhood, during adolescence, and during young adulthood, on one hand, and adult post-traumatic stress symptoms (PTSS), on the other. A cross-sectional survey was conducted among 1,969 Palestinian students using a self-administered questionnaire. The results reveal that the more the participants witnessed and experienced psychological aggression (PS) and physical violence (PH) in their families of origin, the more they exhibited PTSS. Furthermore, the results indicate that a significant amount of the variance in the participants’ PTSS could be attributed to their exposure to family violence, over and above the amounts of variance that were explained by their sociodemographic characteristics and by their perceptions of their parents’ psychological adjustment. The limitations of the study and implications for future research are discussed.
Keywords
Introduction
Exposure to family violence occurs in at least three ways: personal experience with various types of abuse and neglect, witnessing various types of aggression and violence, and the exposure to the co-occurrence of family violence, that is, experiencing and witnessing these behaviors. Exposure to family violence is often considered to be a traumatic experience with short-term as well as long-term effects on the family members who are exposed to it (Knight, 2011). This exposure is often perceived by most family members as a non-normative experience, and may exceed the perceived ability of most of them (mainly the children, and sometimes women) to respond to the demands of the situation. The occurrence of family violence upsets the frame of reference of most family members who are exposed to it. Oftentimes, it also upsets the family as a unit and harms many of their needs, with particular harm to their physical and emotional security. These consequences—especially if the exposure to violence is cumulative—intensify the traumatic nature of the occurrence of family violence for the family as a whole and particularly for the children (Barnett, Miller-Perrin, & Perrin, 2011; Kamphuis & Emmelkamp, 2005; Knight, 2011; McCoy & Keen, 2009; Sternberg, Lamb, Guterman, & Abbott, 2006).
In this article, we present the findings of a study on the exposure of young Palestinian adults (university students) to various patterns and types of family violence, during childhood, during adolescence, and during young adulthood, and the psychological consequences of their exposure, with emphasis on post-traumatic stress symptoms (PTSS).
Literature Review
Experiencing Family Violence and Its Impact on the Development of PTSS
The experience of children and adolescents with different types of family violence (physical, psychological, and sexual) and neglect can have various psychological consequences. However, there is a certain consensus that some psychological consequences are common to most types of family violence, and some of them are even common to different age groups. In particular, the personal experiences of children and adolescents with different forms of violence, abuse, and neglect have the potential to lead to the development of internalizing problems (e.g., anxiety, depression, fear, low self-esteem, and withdrawal) and externalizing problems (e.g., acting out, aggressive behaviors, substance abuse, and dropping out of school), as well as to difficulties with interpersonal relationships, negative changes in cognitive processes, the development of feelings of hopelessness and powerlessness, psychological adjustment problems, and PTSS (Fry, McCoy, & Swales, 2012; Haj-Yahia, Musleh, & Haj-Yahia, 2002; Knight, 2011; McCoy & Keen, 2009; Tolin & Foa, 2006; Widom, Schuck, & Raskin-White, 2006).
There is also empirical evidence that when children and adolescents experience multiple types of abuse, the potential impact on psychological adjustment as well as other consequences are significantly greater than in cases of single-type violence (Barnett et al., 2011). For example, Higgins and McCabe’s (2000) study among a self-selected community sample of men and women revealed that participants who experienced “multi-type maltreatment” reported higher levels of adjustment problems than did those who had experienced single-type maltreatment. Similar results were revealed by Arata, Langhinrichsen-Rohling, Bowers, and O’Farrill-Swails (2005), who examined the differential effects of single- versus multi-type maltreatment among college students. Arata et al. (2005) found that all of the types of abuse that were examined (i.e., neglect, emotional, physical, and sexual abuse) were associated with all of the symptoms examined in their study, that is, individuals with a history of abuse and neglect reported lower self-esteem, more depression, and more suicidality (thoughts and attempts), as well as more intended sexual behavior, more drug and alcohol use, and a stronger tendency toward delinquent behavior. Nonetheless, Arata et al. (2005) indicate that experiencing multiple types of abuse and neglect was a more significant predictor of several of these symptoms than experiencing a single type of abuse and neglect.
Regarding the development of PTSS and even post-traumatic stress disorder (PTSD) as a result of experiencing different types of family violence, research has yielded mixed results. McCoy and Keen (2009) argued that being physically abused as a child increases the likelihood of the development of PTSD. However, some research has shown that experiencing sexual and emotional abuse can predict the development of PTSD significantly more than experiencing neglect and/or physical violence (PH; Sullivan, Fehon, Andres-Hyman, Lipschitz, & Grilo, 2006). In a study conducted among a mixed sample of a community group and student group, Kamsner and McCabe (2000) found that victims of “compound abuse” (i.e., child physical abuse and child sexual abuse) had poorer psychological adjustment than victims of child physical abuse or sexual abuse. In addition, they reported that among the community group, levels of family cohesion and experiencing sexual abuse were the best predictors of trauma symptoms and low self-esteem. Nonetheless, among the student group, the findings revealed that the experience of physical abuse alone significantly contributed to predicting trauma symptoms. Other studies also revealed a significant relationship between PTSS, PTSD, and the duration of experiencing abuse and neglect during childhood (e.g., Barnett et al., 2011; Cicchetti & Toth, 2005; Kaysen, Resick, & Wise, 2003). The prediction of PTSS and PTSD is stronger in cases of experiencing multiple types of abuse than in cases of single type of abuse and neglect (Barnett et al., 2011; Grassi-Oliveira & Milnitsky-Stein, 2008).
Witnessing Family Violence and Its Impact on PTSS
Witnessing different types of family violence, includes seeing violence, hearing violence directly, hearing about violence indirectly, or direct involvement in violence at the time it takes place (e.g., trying to separate the perpetrator and victim, calling a member of the extended family or a friend, calling welfare services, and calling the police). Witnessing family violence also includes experience with the aftermath of violence, for example, witnessing the physical consequences, that is, seeing wounds; seeing the victim’s or perpetrator’s depression or tension; and leaving the home and going to a shelter (Barnett et al., 2011; Edleson, 1999; Haj-Yahia, Tishby, & de Zoysa, 2009).
Reviews of available research conducted over the last three decades have revealed numerous effects of children’s witnessing violence in their families in the following areas: (a) emotional functioning (e.g., anxiety, low self-esteem, depression, suicidality, stress and trauma reactions, feelings of loss, hopelessness, sadness, anger), (b) behavior problems (e.g., aggressive behavior, alcohol and drug abuse, delinquency), (c) social competence (e.g., shyness and withdrawal, hostility, low empathy), (d) cognitive abilities (e.g., academic and achievement problems, poor problem-solving and conflict resolution skills, increased vigilance for threat conditions, deficits in information-processing abilities), and (e) physiological problems (e.g., somatic complaints, increased autonomic arousal, hypertension, poor physical health, ailments or physical symptoms; Appel & Holden, 1998; Edleson, 1999; Evans, Davies, & DiLillo, 2008; Holt, Buckley, & Whelan, 2008; Hungerford, Wait, Fritz, & Clements, 2012; Miller-Perrin & Perrin, 2007; Onyskiw, 2003; Wolfe, Crooks, Lee, McIntyre-Smith, & Jaffe, 2003).
Recent research has also examined the possible impact of witnessing family violence on the development of PTSD among children as well as among young adults. A study conducted by Jarvis, Gordon, and Novaco (2005) among battered women and their school-aged children revealed that the mother’s experience with physical assault by her intimate partner correlated positively and significantly with her child’s PTSD. In addition, this study revealed that on the average, children’s scores on the post-stress reaction index were high: 40% of them were classified as exhibiting moderate PTSD, 50% were classified as having severe PTSD, and 10% demonstrated very severe PTSD. Mertin and Mohr’s (2002) study among children of battered women revealed that these children were troubled by distressing thoughts, conscious avoidance, hypervigilance, and sleep difficulties, and 20% of them met the criteria for diagnosis of PTSD. Those who met the full PTSD criteria scored significantly higher on measures of anxiety, depression, and dissociation.
Evans et al. (2008) maintained that coping skills and perceptions of domestic violence may vary among children at different ages and developmental stages. Hence, the impact of witnessing interparental violence may be manifested differently among children at different ages and developmental stages. However, findings indicate that no clear pattern of symptoms has emerged among children at different ages as a result of their witnessing domestic violence. In addition, several studies have revealed that witnessing interparental violence may affect boys and girls differently. Specifically, boys were found to manifest more externalizing symptoms, whereas girls tended to demonstrate more internalizing symptoms (Edleson, 1999; Evans et al., 2008; Hungerford et al., 2012; Onyskiw, 2003). Nonetheless, some studies of moderating variables have not pointed to age and gender as significant factors in the development of PTSD among children who have witnessed interparental violence (Kilpatrick & Williams, 1998; Wolfe et al., 2003). Previous research has also revealed that maternal psychological functioning and parenting behavior affect children’s psychological responses to witnessing interparental violence, in part because violence against the mother influences her parenting behavior (Edleson, 1999; Evans et al., 2008; Hungerford et al., 2012). For example, some studies have indicated that mothers who experience violence from their partner are at augmented risk for emotional and behavioral difficulties (e.g., Huth-Bocks, Levendosky, & Semel, 2001; Ybarra, Wilkens, & Lieberman, 2007), and this may negatively affect their maternal psychological functioning and the quality of their parenting (Gewirtz, DeGarmo, & Medhanie, 2011). These negative effects may intensify psychological adjustment problems among children who witness their mother’s experience with intimate partner violence (IPV) (Edleson, 1999; Evans et al., 2008; Holt et al., 2008).
The Co-Occurrence of Experiencing and Witnessing Family Violence and Its Impact on PTSS
Research has shown that alarming proportions of children who witness violence in their families also experience abuse and violence from either one or both parents. The first national survey of American families conducted by Straus, Gelles, and Steinmetz (1980) revealed that violence against children increased as a function of increased frequency of violence between spouses. The survey also revealed that 28% and 77% of children in high-violence families had been abused over the last year and during their lifetime, respectively. The second national survey of American families conducted by Straus and Gelles (1990) revealed that 22.8% of men who had been violent against their women partners, and 23.9% of women who had been physically violent against men partners also physically abused a child. A study conducted among male and female university students revealed that 42.9% and 51.7% of men and women who witnessed parental abuse also reported experiencing physical abuse during childhood, respectively (Silvern et al., 1995).
Research on the impact of children’s and young adults’ witnessing and experiencing domestic violence during childhood has revealed a wide range of health and mental health consequences, similar to those found in studies on the consequences of either one of these patterns of family violence (Herrenkohl, Sousa, Tajima, Herrenkohl, & Moylan, 2008). Research evidence indicates that children who have been exposed to both of these patterns of family violence are more severely affected than children who either witness violence or directly experience it (McCloskey & Walker, 2000; Wolfe et al., 2003). Nonetheless, there is no clear-cut evidence regarding which of these two patterns of exposure has a more significant impact, over and above the impact of other patterns of exposure to family violence.
In a study conducted among college students, Marmion and Lundberg-Love (2008) revealed significant relationships between three patterns of exposure to family violence (childhood physical abuse, childhood sexual abuse, and witnessing interparental violence) during childhood and most of the six PTSD subscales that they measured (i.e., anxious arousal, anger/irritability, intrusive experiences, depression, tension reduction behaviors, and defensive avoidance). Their study also revealed that each of the above-mentioned patterns of exposure to family violence contributed significantly to predicting each of the six PTSD subscales. Nonetheless, witnessing interparental violence was found to be the strongest predictor out of all three of the patterns measured.
A study conducted among Sri Lankan university students revealed that the more frequently they witnessed and experienced family violence, the more they demonstrated dissociation, anxiety, depression, and sleep disturbance (Haj-Yahia & de Zoysa, 2008) as well as PTSD (Haj-Yahia et al., 2009). Both patterns of exposure significantly predicted each of these five symptoms over and above their predictability by several sociodemographic variables (e.g., age, gender, parents’ levels of education, and socioeconomic status [SES]) and family environment.
Family Violence, Parents’ Mental Health, and Children’s Mental Health
Although extensive research has been conducted over the last seven decades on the association between parents’ (mainly mothers’) mental health and the mental health of their offspring, this relationship has only been examined in recent years in light of exposure to family violence. Most research has examined mothers’ mental health as victims and fathers’ mental health as perpetrators, rather than examining both dimensions (i.e., both parents as victims and as perpetrators). It has been found that the most prevalent mental health sequelae among women who are victims of IPV include depression, anxiety, low self-esteem, anger, stress, psychological distress, PTSD, and suicidal thoughts as well as many other effects (Haj-Yahia, 1999, 2000a, 2000c; Kim & Lee, 2013; Miranda, Osa, Granero, & Ezpeleta, 2013; Pico-Alfonso et al., 2006). It has been argued that in violent families, the mothers’ mental health may influence the mental health of her children, particularly if mothers have a history of violence during childhood and in their intimate relations. Several studies have shown that children’s mental health problems that develop as a result of their exposure to family violence are significantly associated with the deteriorating psychological well-being and mental health of their mothers, who are also victims of IPV (e.g., Collishaw, Dunn, O’Connor, & Golding, 2007; Evans et al., 2008; Miranda et al., 2013). In a study of traumatic stress symptoms among children following exposure to IPV, Graham-Bermann, DeVoe, Mattis, Lynch, and Thomas (2006) found that among Caucasian children, these symptoms were best predicted by mothers’ mental health and low self-esteem. The best predictors of these symptoms among minority children were the amount of violence against mothers to which they were exposed, mothers’ low self-esteem, and mothers’ monthly income. Nonetheless, McCloskey, Figueredo, and Koss (1995) revealed that although mothers who had experienced IPV exhibited mental health problems, these problems did not mediate the implications of IPV on psychopathology among their children.
The vast majority of research on mental health sequelae among men in violent families refer to these men as perpetrators of IPV, as abusive fathers, and as victims of abuse and neglect during their childhood rather than as victims of IPV. It is beyond the scope of this article to discuss the mental health of men from these different perspectives. Nonetheless, these men are usually depicted as having problems with anger control, deficits in empathy, low levels of tolerance for frustration, and low self-esteem, as well as rigidity, hostility, depression, severe levels of different patterns of anxiety (mainly social anxiety and abandonment anxiety), life stress, personal distress, irritability, and substance abuse and dependence. In addition, these men are described as demonstrating some intellectual impairment and deficits in problem-solving skills (Barnett et al., 2011; Miller-Perrin & Perrin, 2007). There is a lack of research dealing with the possible impact of fathers’ mental health on the association between their offspring’s exposure to family violence and their PTSS. In this study, the participants’ perceptions of their fathers’ and mothers’ psychological adjustment were examined as moderating variables in the possible association between their exposure to different patterns of family violence and PTSS.
Critique of Previous Research
As shown, extensive research has been conducted in recent decades on the mental health consequences of children’s and adolescents’ exposure to family violence. Most of the available research on the impact of witnessing interparental violence has focused on witnessing father-to-mother PH, but has rarely examined the impact of witnessing mother-to-father and parents-to-siblings violence. Similarly, although extensive research has been conducted on the effects of experiencing parental abuse and violence, there is a lack of research on the impact of siblings-to-children violence. In addition, most existing studies have been conducted among samples known to health and mental health services, that is, among clinical samples of children and adolescents who have been exposed to severe patterns of PH in the family. However, it is only in recent years that a few studies have been conducted among random or convenient community samples, which consisted mainly of university students and may include participants who have been exposed to a wide range of frequencies and severities of violence in their families.
Furthermore, there is a serious dearth of research on the mental health consequences of cumulative exposure to family violence throughout the life span, and most of the available research has examined the effects of this exposure during childhood and/or adolescence, with special emphasis on the occurrence of family violence over the past year. Only in recent years, research has begun to address the possible effects of such exposure during adulthood, and the effects of cumulative exposure during childhood, adolescence, and young adulthood. To overcome some of these shortcomings, our study was conducted among a random sample of Palestinian university students, from the West Bank and East Jerusalem. We examined witnessing three patterns of violence in the family of origin among the participants (i.e., father-to-mother, mother-to-father, and parents-to-siblings) as well as experiencing three patterns of violence in the family (i.e., from fathers, mothers, and siblings). In their reports about each one of these six patterns of family violence, participants were requested to refer to two types of violence, that is, psychological aggression (PS) and PH, during each one of the following developmental stages: childhood, adolescence, and young adulthood. In addition, besides examining levels of PTSS among participants, they also reported on their perceptions of their fathers’ and mothers’ psychological adjustment during each one of the three developmental stages.
Research Hypotheses and Questions
The following were the two main research hypotheses:
The following were the main five research questions:
Method
Participants
A cross-sectional survey was conducted among 1,969 Palestinian undergraduate students (64.2% females, and 35.8% males) at three Palestinian universities in the West Bank and East Jerusalem. The participants were enrolled in different disciplines and fields of specialization, from all 4 years of study. They ranged from 18 to 37 years of age (M = 20.37, SD = 2.24); 83.8% were Muslim, and the remaining 16.2% were Christian; 72.9% lived in the West Bank, 25.8% lived in East Jerusalem, and 1.3% were originally from the Gaza Strip; 42.5% lived in rural localities, 49.5% lived in urban localities, and 8% lived in refugee camps.
Instrument Package
A self-administered Arabic-language instrument package was utilized in this study, and consisted of the following items and measures.
Background and sociodemographic information
The measure consisted of several items relating to the sociodemographic characteristics of the participants, their parents, and their families such as participant’s age, gender, year of study at the university, religion, type of locality of residence (i.e., rural, urban, and refugee camp), area of residence (i.e., West Bank, East Jerusalem, and Gaza Strip), father’s and mother’s age and level of education, number of siblings, family size, family’s socioeconomic status (as assessed by the participant), and quality of housing (measured by the availability of durable goods such as a television, computer, dishwasher, washing machine, dryer, car, and more).
Exposure to family violence
Revised forms of two subscales—PS and PH—of the Conflict Tactics Scale (CTS; Straus, 1979) were utilized in this study. These subscales included 18 items, which measured the participants’ exposure to two types of violence, that is, PS (e.g., “sulked and/or refused to talk about a conflict,” “threatened to hit or throw something”) and PH (e.g., “slapped,” “kicked, bit, or hit,” “beat up”) in their families, during each of the following three periods: (a) in elementary school (i.e., in childhood), (b) in junior high and secondary schools (i.e., in adolescence), and (c) from high school graduation until the date of filling out the questionnaire (i.e., in early adulthood). This measure was used to evaluate the extent to which participants had witnessed each of the following three patterns of family violence: (a) father-to-mother, (b) mother-to-father, and (c) parents-to-siblings. In addition, we used this measure to examine the extent to which the participants had experienced each of the following three patterns of family violence: (a) father-to-participant, (b) mother-to-participant, and (c) siblings-to-participant. As indicated, participants reported on two types of violence (i.e., PS and PH) when referring to each of the six patterns of exposure to family violence. Exposure to different patterns and types of family violence, during different developmental ages, are treated as the main predictors of this study.
Responses to the items on the CTS examined in this study were based on an 8-point scale, as follows: 0 (never), 1 (once a year), 2 (two to three times a year), 3 (often, but less than once a month), 4 (about once a month), 5 (more than once a month, but not weekly), 6 (weekly, but not daily), and 7 (daily). This measure is widely used in family violence research, and is considered to have reliable and valid subscales. The instrument used in this study was a revised version of the Arabic-language CTS, which has been used in previous research among Arab participants (e.g., Haj-Yahia, 1997, 2001). Notably, the nature of the measured pattern of family violence as well as the developmental stage that the participants were asked about were emphasized in the introduction preceding each group of 18 items of PS and PH. Hence, it is assumed that this prevented any potential for confusing that pattern with other patterns of family violence and/or with other sources of violence and/or traumas during any developmental stage. In this study, the Cronbach’s alpha values of the measures of witnessing different patterns of PS and PH during all three periods ranged from .900 to .936, and from .888 to .960, respectively. In addition, the Cronbach’s alpha values of the measures of experiencing different patterns of PS and PH during the three above-mentioned periods ranged from .907 to .935 and from .865 to .936, respectively (for detailed data on the reliability of the CTS used in this study, see Table 1).
Cronbach’s Alpha Values of the Conflict Tactics Scales.
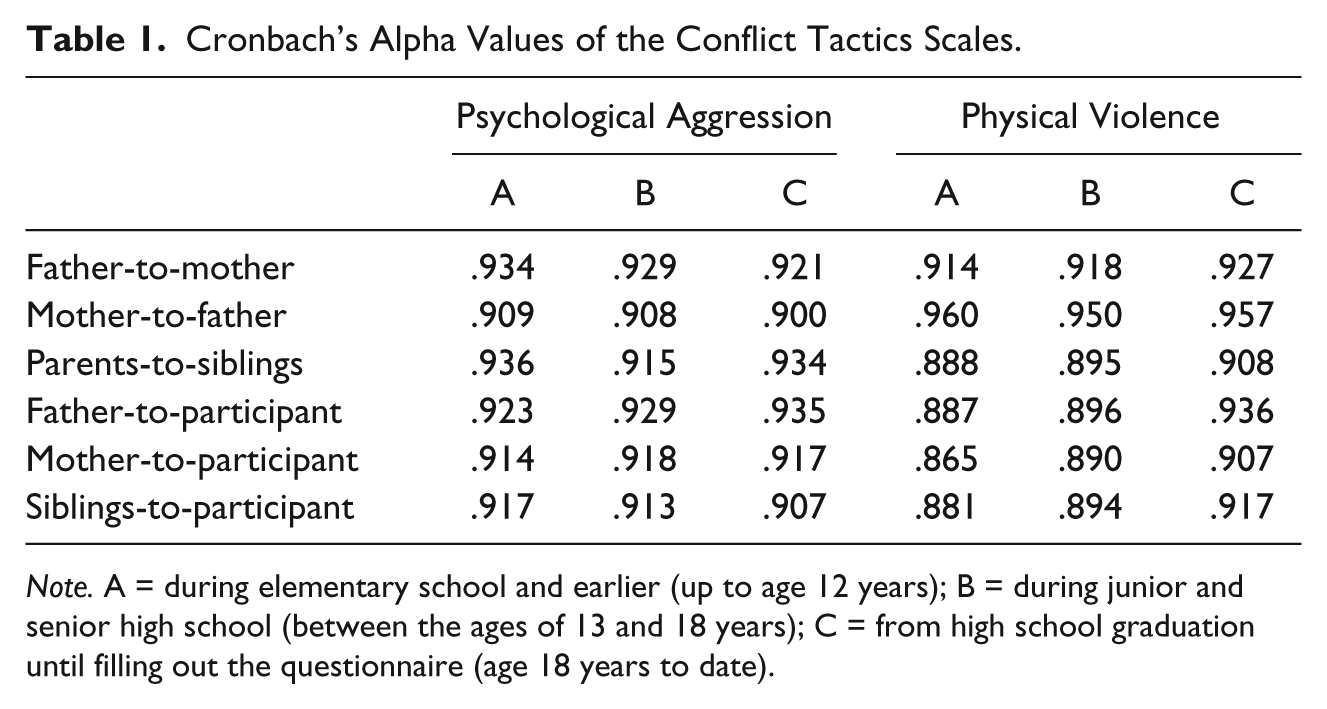
Note. A = during elementary school and earlier (up to age 12 years); B = during junior and senior high school (between the ages of 13 and 18 years); C = from high school graduation until filling out the questionnaire (age 18 years to date).
Participants’ perceptions of parents’ psychological adjustment
The Psychological Adjustment Scale (PAS) was utilized to measure participants’ perceptions of their mothers’ and fathers’ psychological adjustment during each of the three developmental stages mentioned above. The PAS consists of seven items (e.g., “feeling sad, lonely,” “tired and worn,” “pressured”), and the scale of responses ranged from 1 (often) to 4 (never). The average internal reliability reported for the PAS was Cronbach’s α = .66 (National Commission on Children, 1991; Voydanoff & Donnelly, 1999). The Cronbach’s alpha values of the Arabic version used in this study during childhood, adolescence, and young adulthood were .886, .859, and .856, respectively, for mothers, and .886, .869, and .873, respectively, for fathers. Perceived fathers’ and mothers’ psychological adjustment were treated as moderator variables in this study.
PTSS
A 28-item inventory of Crime-Related PTSD (CR-PTSD; e.g., “repeated unpleasant thoughts that won’t leave your mind,” “feeling uneasy in crowds, such as shopping or at a movie”; Saunders, Mandoki-Arata, & Kilpatrick, 1990) was used to measure levels of PTSS among the participants as the main dependent variable in this study. Saunders et al. (1990) developed the CR-PTSD by testing the ability of the items contained in the Symptom Checklist-90–Revised (SCL-90-R), which is a widely used psychological symptom assessment instrument, to “effectively screen for and assess CR-PTSD among women” (Saunders et al., 1990, p. 440). In that test, the inventory was found to be reliable and valid, and the Cronbach’s alpha value of the Arabic-language version of the measure used among the Palestinian students in the present study was .931. Responses to the items in this inventory were based on a 4-point scale ranging from 0 (never) to 3 (very often).
Procedure
In the first stage, Arabic versions of the PAS and the CR-PTSD measures were prepared. To ensure valid and robust procedures in translating and adapting the measures, they were translated from English to Arabic by three Palestinian professionals who had an excellent command of English, and who specialize in the social, behavioral, and mental health sciences. Each of these professionals was asked to translate the measures into Arabic independently, taking into consideration the cultural context of their concepts in Palestinian society. Afterward, they worked together with one of the authors to prepare unified Arabic versions of all three translations of the measures. To ensure the comparability of the measures in both languages, the unified Arabic versions were back-translated into English by a professional translator, in cooperation with one of the authors of this article.
The study was approved by the ethics committee of the school that the authors are affiliated with. In addition, an informed consent form was obtained from each individual participant. The study was conducted in cooperation with the registrar offices of three major Palestinian universities in the West Bank and East Jerusalem, who helped in the process of random selection of at least 30 courses with an enrollment of at least 20 students from different faculties and departments, in all years of study (first to fourth year) at the undergraduate level. Following this process, 92 courses with an official enrollment of 2,220 students were selected. About a week before the distribution of questionnaire, all 86 of the instructors who taught these courses were informed by the registrar of their university and by one of the authors about the nature and purpose of the study, as well as about the data collection procedures. In addition, the instructors were asked to cooperate in distributing the questionnaires among their students, and to inform the students that the questionnaires would be distributed in one of the classes within the next 3 weeks. All of the instructors agreed to cooperate in implementing these procedures. During the 3 weeks that followed, the students attending all 92 of the courses selected for the sample were approached in class by one of the authors together with a research assistant. The students were given explanations about the nature and purpose of the study, and were told that their participation in the study is voluntary. Questionnaires were distributed to all of the students who were present in class (a total of 2,196 students were present when the questionnaires were distributed, i.e., 98.9% of the students who were officially registered in the selected courses). The students were asked to fill out the questionnaire during the class session, and return it in a sealed envelope which was provided together with the questionnaire. Of the students who were present in class, 2,098 returned the questionnaires (a 95.5% response rate), which were placed in a special box provided by the research team.
The participants were assured that all of the information they provided would remain strictly confidential, and they were instructed to refrain from disclosing any information that would reveal their identity. The time required to fill out the questionnaires was 35 to 45 min. A short debriefing session (about 10-15 min) was conducted in each class after the students finished filling out the questionnaires, and contact information was provided for one of the authors as well as for the University’s Student Counseling Center, in the event that they had questions about any issue pertaining to the study, or in the event that they experienced any discomfort as a result of their participation.
In the data entry phase, 129 questionnaires (6.1%) were eliminated because responses to over 20% of the questions were missing. Hence, questionnaires were coded for a total of 1,969 participants (88.7% of the original sample, and 93.9% of those who were present at the time of data collection), using SPSS software.
Statistical Analysis
Several types of statistical analyses were conducted to examine the research hypotheses and questions. First, with regard to rates of students’ exposure to the six above-mentioned patterns of family violence during each of the three periods of the study, descriptive statistics were examined for each of the items that measured PS and PH. (Due to space limitations, the results of these analyses are not presented in this article, but they can be obtained from the authors.) Second, zero-order correlations were calculated among several of the sociodemographic characteristics, as well as among all 36 of the variables that measured exposure to family violence (i.e., the six patterns of experiencing and witnessing violence × the two types of violence × the three time periods), and among the measure of PTSS (which are not fully presented here due to space limitations). Third, because the previous analysis revealed very high and significant correlations among all 36 patterns of exposure to PS and PH during all three periods, and to overcome the potential for multicollinearity, one PS score and one PH score were calculated for all three periods together, for each of the six above-mentioned patterns of exposure to family violence. Hence, this procedure enabled us to aggregate the 36 patterns of exposure into 12 patterns of cumulative witnessing and experiencing of family violence. Afterward, to examine both hypotheses of the study, zero-order correlations were calculated among participants’ all 12 patterns of exposure to violence, perceived fathers’ and mothers’ psychological adjustment, and PTSS (see Table 2). Notably, all three scores for participants’ perceptions of fathers’ psychological adjustment were aggregated to produce one score, as were all three scores for participants’ perceptions of mothers’ psychological adjustment. Fourth, to examine the first research question, partial correlations were examined between all 12 patterns of exposure to family violence and PTSS, where perceived fathers’ and mothers’ psychological adjustment were held constant (see Table 3). The purpose of this analysis is to partial out the possible influence of perceived parents’ psychological adjustment on the correlations between all patterns of exposure to family violence and PTSS.
Zero-Order Correlations Among All Patterns of Exposure to Family Violence and PTSS and Perceived Parental Psychological Adjustment (N = 1,969).
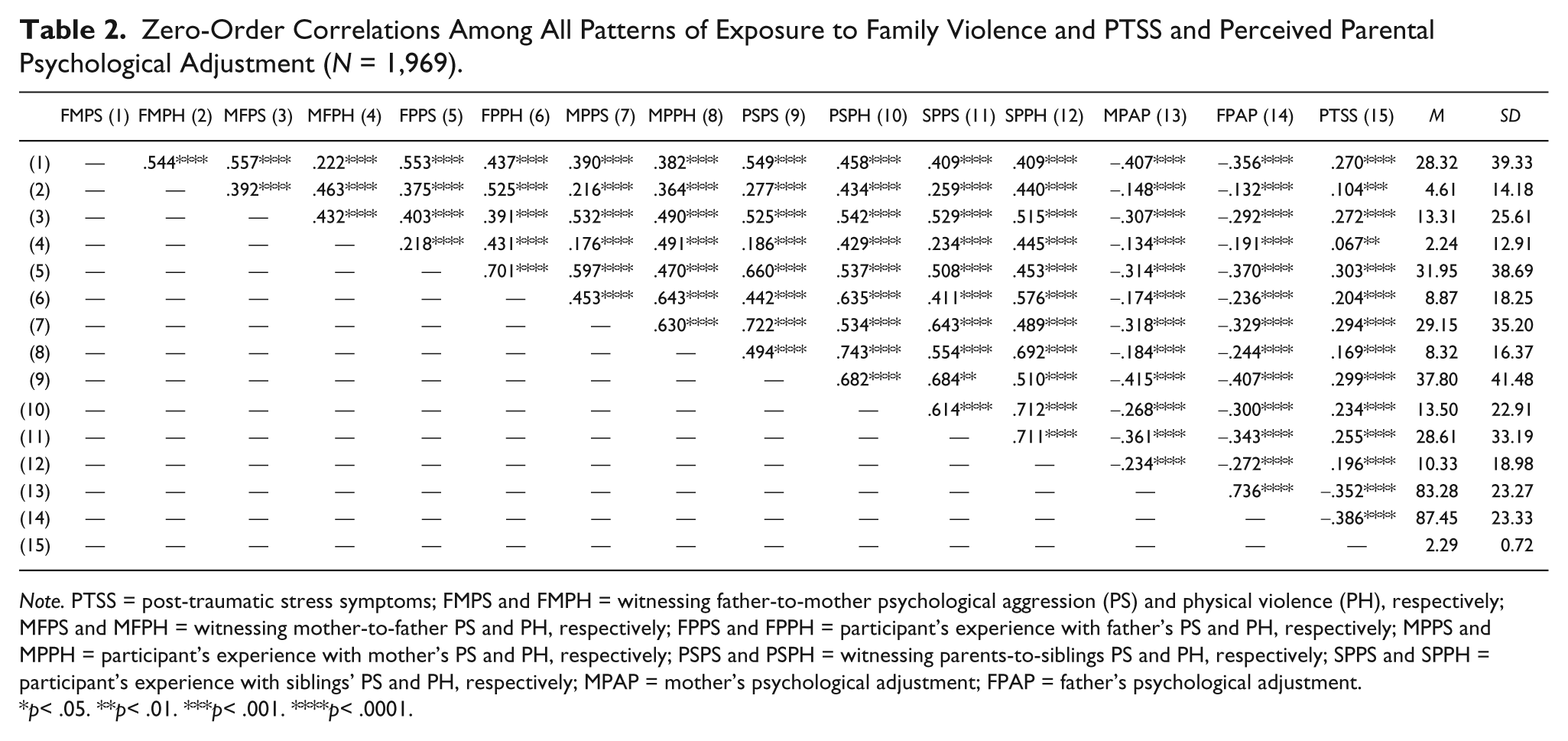
Note. PTSS = post-traumatic stress symptoms; FMPS and FMPH = witnessing father-to-mother psychological aggression (PS) and physical violence (PH), respectively; MFPS and MFPH = witnessing mother-to-father PS and PH, respectively; FPPS and FPPH = participant’s experience with father’s PS and PH, respectively; MPPS and MPPH = participant’s experience with mother’s PS and PH, respectively; PSPS and PSPH = witnessing parents-to-siblings PS and PH, respectively; SPPS and SPPH = participant’s experience with siblings’ PS and PH, respectively; MPAP = mother’s psychological adjustment; FPAP = father’s psychological adjustment.
p< .05. **p< .01. ***p< .001. ****p< .0001.
Zero-Order Correlations and Partial Correlations Between Exposure to Family Violence and PTSS.
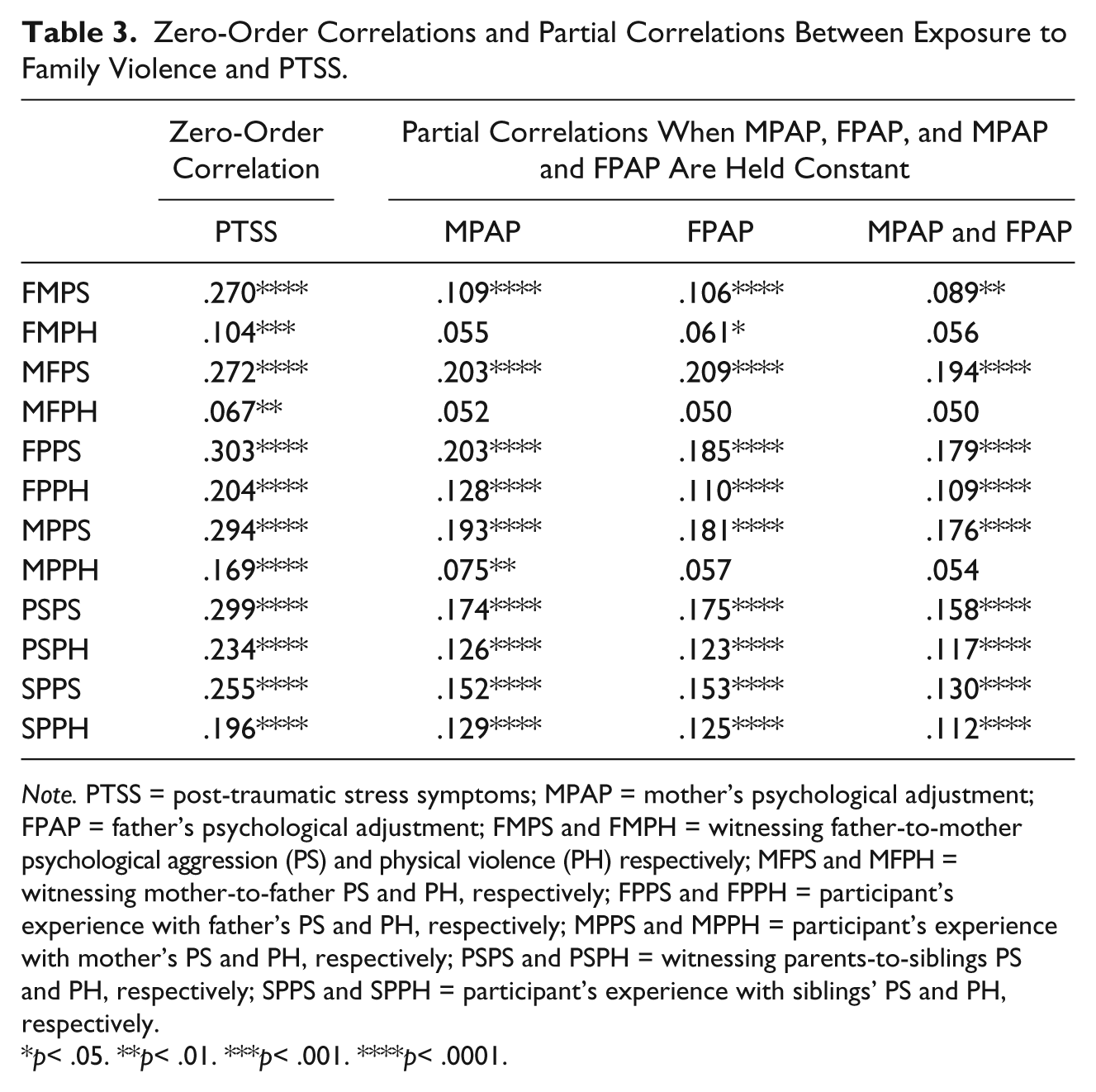
Note. PTSS = post-traumatic stress symptoms; MPAP = mother’s psychological adjustment; FPAP = father’s psychological adjustment; FMPS and FMPH = witnessing father-to-mother psychological aggression (PS) and physical violence (PH) respectively; MFPS and MFPH = witnessing mother-to-father PS and PH, respectively; FPPS and FPPH = participant’s experience with father’s PS and PH, respectively; MPPS and MPPH = participant’s experience with mother’s PS and PH, respectively; PSPS and PSPH = witnessing parents-to-siblings PS and PH, respectively; SPPS and SPPH = participant’s experience with siblings’ PS and PH, respectively.
p< .05. **p< .01. ***p< .001. ****p< .0001.
Fifth, to examine the second question of this study, hierarchical regression and multiple regression analyses were conducted for PTSS. At the first stage of these analyses, that is, the first block of predictors, several sociodemographic characteristics were entered into the regression and multiple regression formula (e.g., age, gender, place of residence, parents’ levels of education, and family SES as assessed by a by-proxy of quality of housing). Because of the very high and significant relationship between fathers’ and mothers’ levels of education (r = .634, p< .0001), and to prevent any potential multicollinearity, an average of both levels of education was calculated and then entered into this formula as one variable. At the second stage, that is, the second block of predictors, participants’ perceptions of mothers’ and fathers’ psychological adjustment were entered into the hierarchical regression and multiple regression analyses. The third and fourth stages of this analysis included the main predictors of this study, that is, the three patterns of cumulative witnessing of family violence and the three patterns of cumulative experiencing of family violence, respectively, which comprised the third and fourth blocks of predictors. In so doing, we aimed to examine the power of these variables to predict PTSS, over and above the variance that was explained by the previous two blocks of predictors (see Table 4). In addition, hierarchical regression and multiple regression analyses were carried out to examine the third research question presented earlier. Hence, the first two stages included the first two blocks of predictors in the above-mentioned analyses, and the third block included three main predictors of PTSS: exposure to family violence during childhood, exposure to family violence during adolescence, and exposure to family violence during young adulthood. Each one of these three predictors was produced by compiling all acts of witnessing and experiencing PS and PH during each one of the three periods separately, namely, all acts of witnessing and experiencing PS and PH during each of these three periods were summed up as one new variable, regardless of who the victims and perpetrators were (see Table 5). Furthermore, to examine the fourth question of this study, hierarchical regression and multiple regression analyses were carried out, which included the first two blocks of predictors indicated earlier, as well as the third block with the following two predictors: cumulative exposure to PS and cumulative exposure to PH. Accordingly, each one of these predictors was calculated by summing all acts of witnessing and experiencing PS (as one predictor) and witnessing and experiencing PH (as another predictor), during the life span, regardless of who the perpetrators and victims were (see Table 6). In addition, to test the fifth question, we examined the interactions of gender and perceived fathers’ and mothers’ psychological adjustment with each of the main predictors in the previous three hierarchical regression and multiple regression analyses (i.e., the predictors of exposure to family violence presented in Tables 4-6). However, because none of the interaction variables were found to contribute significantly to predicting PTSS and to explaining its variance over and above the predictability of PTSS by the blocks indicated earlier, the results of the interaction analyses are not included in these three tables (see Tables 4-6).
Hierarchical Multiple Regression Analysis on PTSS, by Different Patterns of Witnessing and Experiencing Family Violence.
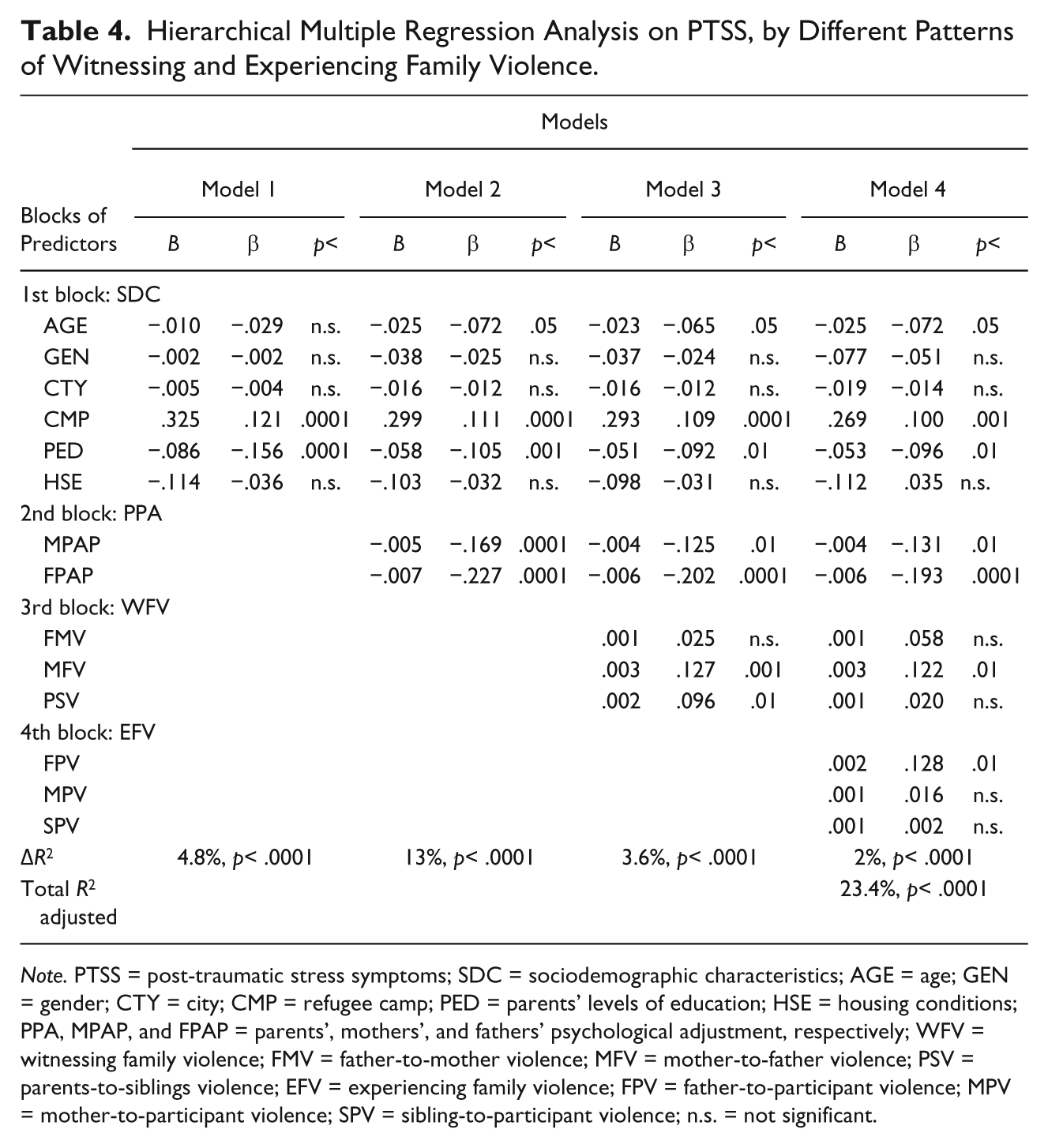
Note. PTSS = post-traumatic stress symptoms; SDC = sociodemographic characteristics; AGE = age; GEN = gender; CTY = city; CMP = refugee camp; PED = parents’ levels of education; HSE = housing conditions; PPA, MPAP, and FPAP = parents’, mothers’, and fathers’ psychological adjustment, respectively; WFV = witnessing family violence; FMV = father-to-mother violence; MFV = mother-to-father violence; PSV = parents-to-siblings violence; EFV = experiencing family violence; FPV = father-to-participant violence; MPV = mother-to-participant violence; SPV = sibling-to-participant violence; n.s. = not significant.
Hierarchical Multiple Regression Analysis on PTSS, by Exposure to Family Violence During Childhood, Adolescence, and Young Adulthood.
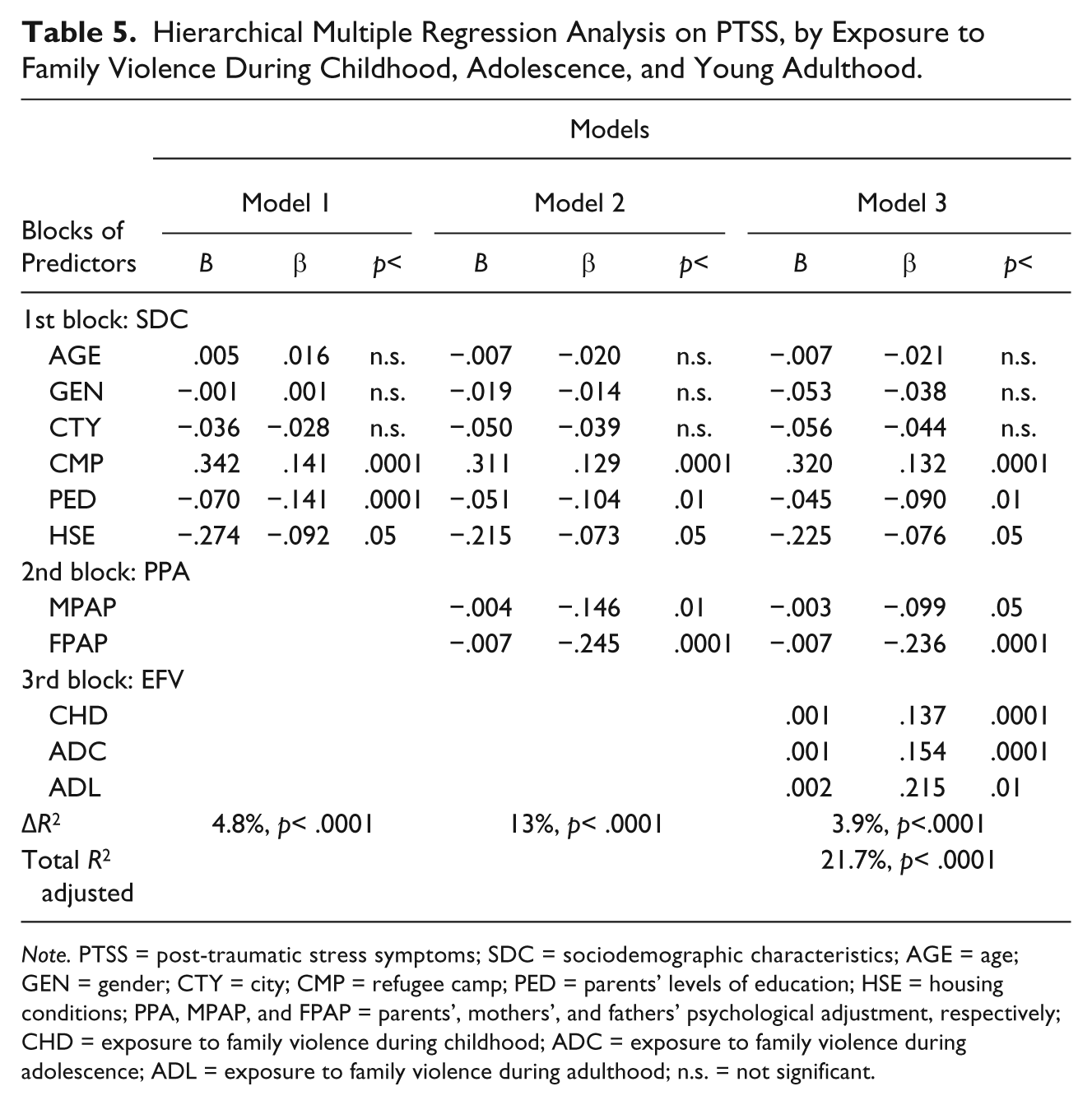
Note. PTSS = post-traumatic stress symptoms; SDC = sociodemographic characteristics; AGE = age; GEN = gender; CTY = city; CMP = refugee camp; PED = parents’ levels of education; HSE = housing conditions; PPA, MPAP, and FPAP = parents’, mothers’, and fathers’ psychological adjustment, respectively; CHD = exposure to family violence during childhood; ADC = exposure to family violence during adolescence; ADL = exposure to family violence during adulthood; n.s. = not significant.
Hierarchical Multiple Regression Analysis on PTSS, by Cumulative Exposure to Psychological Aggression and Physical Violence.

Note. PTSS = post-traumatic stress symptoms; SDC = sociodemographic characteristics; AGE = age; GEN = gender; CTY = city; CMP = refugee camp; PED = parents’ levels of education; HSE = housing conditions; PPA, MPAP, and FPAP = parents’, mothers’, and fathers’ psychological adjustment, respectively; EFV = exposure to family violence; PSA = exposure to cumulative psychological aggression; PHV = exposure to cumulative physical violence; n.s. = not significant.
Results
Correlations Among Exposure to Family Violence, Perceived Parents’ Psychological Adjustment, and PTSS
Regarding the two research hypotheses, the results in Table 2 reveal significant correlations between the participants’ exposure to each one of the patterns of family violence and levels of PTSS examined in the study: The more the participants witnessed and experienced each of the patterns of PS and PH in their families of origin, the higher their levels of PTSS were (see Table 2). The results also reveal that the more participants witnessed and experienced each of the patterns of PS and PH in their families of origin, the lower they perceived their mothers’ and fathers’ psychological adjustment to be. Furthermore, lower levels of perceived mothers’ and fathers’ psychological adjustment correlated significantly with higher levels of PTSS (see Table 2).
Regarding the first research question, the results of the partial correlations revealed that although all of zero-order correlations between all patterns of exposure to family violence and PTSS slightly decreased, after partialing out the influence of perceived parents’ psychological adjustment on those correlations, the vast majority of the correlation coefficients (i.e., between patterns of exposure to family violence and PTSS) remained significant. Notably, the correlation between mother-to-participant PH and PTSS remained significant (r = .075, p< .01) after holding constant perceived mothers’ psychological adjustment. However, this correlation became insignificant after holding constant the participants’ perceptions of fathers’ psychological adjustment, and after holding constant their perceptions of fathers’ and mothers’ psychological adjustment. In addition, the correlation between mother-to-father PH and PTSS became insignificant after controlling for the participants’ perceptions of mothers’, fathers’, and mothers’ and fathers’ psychological adjustment. Similar results were revealed regarding the correlation between father-to-mother PH and PTSS. Notably, although the zero-order correlations between father-to-mother and mother-to-father PH on the one hand and PTSS on the other were significant, the correlations were weak even before controlling for the participants’ perceptions of parental psychological adjustment (see Table 3).
Predicting PTSS by Exposure to Family Violence
The second research question examined the predictability of participants’ PTSS by witnessing three patterns of cumulative family violence and experiencing three patterns of cumulative family violence, over and above the predictability of PTSS by the participants’ sociodemographic characteristics and by perceptions of their parents’ psychological adjustment. Hence, each of the three patterns of witnessing family violence was calculated by summing all acts of PS and PH that were witnessed for each pattern throughout the life span. Similarly, each of the three patterns of experiencing family violence was calculated by summing all acts of PS and PH by that perpetrator that were experienced throughout the life span. The results in Table 4 reveal that 23.4% of the variance in the participants’ PTSS can be attributed to all four blocks of predictors examined in the analyses. More specifically, the results reveal that 5.6% of the variance in PTSS was significantly explained by the two main blocks of predictors examined in this study, that is, 3.6% and 2.0% of the variance in the participants’ PTSS could be significantly attributed to cumulative witnessing of three patterns of family violence and to cumulative experiencing of three patterns of family violence, respectively. Notably, witnessing mother-to-father violence (β = .127, p< .001), and parents-to-siblings violence (β = .090, p< .001), as well as experiencing father’s violence (β = .128, p<.01) were found to be the three most significant patterns of family violence that contributed to explaining the variance in PTSS out of the six patterns examined in this study. These results are over and above the variance in participants’ PTSS that could be significantly explained by the participants’ sociodemographic characteristics (i.e., 4.8%), and by their perceptions of their parents’ psychological adjustment (i.e., 13%; see Table 4).
The third research question examined the predictability of participants’ PTSS by their exposure to family violence (i.e., witnessing and experiencing family violence as one variable) during each one of the three developmental periods examined, that is, during childhood, during adolescence, and during young adulthood as three separate predictors, over and above its predictability by the participants’ sociodemographic characteristics and by perceived psychological adjustment of parents. Hence, each of these three predictors was calculated by summing all witnessed and experienced PS and PH during each of the above-mentioned developmental periods. The results revealed that exposure to family violence significantly explained 3.9% of the variance in the participants’ PTSS. This amount of the variance is over and above the variance that could be attributed to the participants’ sociodemographic characteristics (i.e., 4.8%) and to their perceptions of their parents’ psychological adjustment (i.e., 13%). Notably, exposure to family violence during each one of the three developmental stages examined in the study was found to significantly explain the variance in PTSS during childhood (β = .137, p< .0001), during adolescence (β = .157, p< .0001), and during young adulthood (β = .215, p< .01; see Table 5).
Furthermore, the fourth research question examined the extent to which participants’ PTSS is predicted by cumulative exposure to PS and cumulative exposure to PH, as two separate predictors, over and above the predictability of PTSS by the participants’ sociodemographic characteristics and perceptions of their parents’ psychological adjustment. These two patterns of violence, that is, cumulative exposure to PS and to PH, were calculated by summing all acts of PS that were witnessed and experienced throughout the life span into one predictor and, similarly, by summing all acts of PH that were witnessed and experienced throughout the life span into another predictor. The results revealed that participants’ exposure to family PS and PH during the life span explained 3.9% of the variance in their PTSS. This variance was significant over and above the variance (i.e., 4.8%) that could be attributed to their sociodemographic characteristics and to their perceptions of their parents’ psychological adjustment (i.e., 13%). It should be noted that exposure to each one of the two types of violence, that is, cumulative PS and cumulative PH, contributed significantly to the explained variance in their PTSS (β = .177, p< .0001, and β = .114, p < .05, respectively; see Table 6).
Discussion
Summary and Conclusions
The results of this study revealed that each of the patterns of witnessing and experiencing family violence examined in this study (i.e., PS and PH) correlated positively and significantly with PTSS among Palestinian university students. Notably, exposure to family violence during each of the periods examined (i.e., during childhood, during adolescence, and during young adulthood) contributed significantly to explaining PTSS among the participants. The results also revealed that the development of PTSS among the participants could be significantly attributed to each of the two forms of exposure to family violence (i.e., witnessing and experiencing) rather than to either form of exposure alone. These findings support the results of earlier research, which showed that exposure to family violence is a traumatic experience that can lead to the development of PTSS (Becker-Blease & Freyd, 2005; Hetzel & McCanne, 2005; Sternberg et al., 2006).
The findings of this study are also consistent with previous research on the short-term and long-term consequences of exposure to different and multiple types and patterns of family violence (e.g., Feerick & Snow, 2005; Haj-Yahia et al., 2009). Several studies have demonstrated that children and young adults who have been exposed to more than one form of family violence (i.e., witnessing interparental violence and experiencing parental violence) and to more than one type of family violence (i.e., psychological, physical, or sexual) are at greater risk of developing PTSD (Haj-Yahia et al., 2009; McCloskey & Walker, 2000; Sternberg et al., 2006; Wolfe et al., 2003). This is not only because of the combination of the two types and six patterns of family violence to which the participants were exposed, but also to the general toxic family atmosphere in which this violence occurs. This atmosphere and environment are usually characterized by the intense levels of fear, anxiety, hostility, irritability, anger, tension, willingness for revenge, helplessness, hopelessness, and lack of trust besides many other characteristics that have an impact on individuals in the family as well as on marital and family relations (Barnett et al., 2011; Haj-Yahia et al., 2009; Siegel, 2013). Moreover, in Arab societies, this atmosphere in the nuclear family can have a negative impact on the relationships in extended families, as expressed in the development of interfamilial tensions, hostilities, conflicts, disputes, antagonism, and even the occurrence of violence between the extended families of both partners (Haj-Yahia, 2000c).
Hence, not surprisingly, the results of this study reveal that the more the participants reported being exposed to different types and patterns of family violence, the more negatively they perceived the psychological adjustment of each of their parents. Furthermore, the results indicate that participants with more negative perceptions of each of their parents’ psychological adjustment reported higher levels of PTSS. Nonetheless, it should be noted that despite the relatively high percentages of variance in the participants’ PTSS that was explained by their perceptions of their parents’ psychological adjustment, the findings still revealed that a significant amount of the variance in their PTSS could be attributed to their exposure to family violence, over and above the variance in their perceptions of their parents’ psychological adjustment. Furthermore, no significant interactions were revealed between the effects of the participants’ exposure to any one of the types and patterns of family violence and their perceptions of their fathers’ and mothers’ psychological adjustment on the one hand, and PTSS on the other. Similarly, no significant interactions were revealed between the participants’ exposure to any type and pattern of family violence and their gender on the one hand, and their PTSS on the other. Consequently, the participants’ exposure to any type or pattern of family violence was found to be a significant predictor of PTSS, irrespective of the participants’ perceptions of their parents’ psychological adjustment and irrespective of their gender. Moreover, these results are indicative of the potential detrimental effects of exposure to family violence on PTSS, even after partialing out the possible effects of perceptions of parents’ psychological adjustment and after controlling for several sociodemographic characteristics, including gender. However, only one construct, that is, the participants’ perceptions of their parents’ psychological adjustment, was examined in this study as a possible indication of the negative family atmosphere that might develop as a result of family violence. Hence, on the one hand there is a need to conduct more comprehensive research on the relevance of personal, parental, marital, and family characteristics like those mentioned earlier to exposure to family violence, as well as for research on the extent to which these characteristics can intensify the negative mental health consequences of exposure to family violence. On the other hand, there is a need to examine the extent to which the lack of these characteristics and the existence of positive personal, parental, marital, and family characteristics can mitigate these consequences. In Arab societies, it is especially important to examine the extent to which the development of negative responses between the extended and nuclear families such as those mentioned earlier (e.g., interfamilial disputes, tensions, hostilities, etc.) as a result of the occurrence of violence in the nuclear family can exacerbate the negative mental health consequences that develop as a result of exposure to family violence. In that context, there is also a need to conduct research on the extent to which the positive involvement of extended families (e.g., offering support and protection) in light of violence in the nuclear family can contribute toward mitigating the negative consequences of exposure to family violence (Haj-Yahia, 2000c, 2011).
The results of our study indicate that some of the variance in the participants’ PTSS could be attributed to their sociodemographic characteristics, namely, place of residence (refugee camps), and to their parents’ levels of education. Previous research on Palestinian society has revealed that these two characteristics are significant predictors and risk factors for violence against women (Haj-Yahia, 2000d). Nonetheless, there is a lack of research on the relationship between these characteristics and PTSS in Palestinian society. Palestinian refugee camps are characterized by very high population density and very poor infrastructure in many domains (including quality of housing; educational, health, and welfare services; and sanitation and sewage systems). These difficult life conditions can have negative mental health implications at the personal, family, and community levels (e.g., high levels of stress, frustration, hostility, irritability, anger, hopelessness, helplessness, crime, losses, grief, and PTSS). Similarly, the parents’ low levels of education can be a significant predictor of low income or even poverty and unemployment, which might also lead to mental health consequences similar to those indicated above. Although it has been argued that these conditions and consequences might become significant stressors and risk factors for family violence (e.g., Barnett et al., 2011), there is a serious lack of research on their relevance to PTSS among members of the Palestinian family following exposure to family violence.
All of the blocks of predictors examined in this study explained only between 21.7% and 23.4% of the variance in the participants’ PTSS. This result raises a question about the potential contribution of other predictors such as the family’s history of PTSS (Keane, Marshall, & Taft, 2006), which were not measured in this study or in previous studies conducted in Palestinian society. Another possible predictor is the accumulation of experience with traumatic political events relating to the Arab–Israeli conflict (Haj-Yahia, 2008). This conflict has resulted in several wars, which have had devastating and traumatic consequences for Palestinians as well as for all nations in the region. Finally, in previous research, the participants’ coping styles at different developmental stages, as well as by their appraisals of the current situation and the process of exposure to family violence and similar traumatic events, have been found to influence the development of PTSS in aspects such as the children’s and young adults’ ability to calm themselves down or their cognitive beliefs relating to the traumatic experience (Bowman & Yehuda, 2004).
Strengths, Limitations, and Implications for Future Research
Several strengths of this study are noteworthy. First, the data are based on young adults’ self-reports regarding their exposure to different types and patterns of family violence and regarding levels of PTSS as a consequence of such exposure, rather than based on reports by other parties such as parents, teachers, mental health practitioners, or human service providers. Second, we examined the extent to which the participants witnessed and experienced three patterns of family violence at different levels of frequency and severity during childhood, during adolescence, and during young adulthood, that is, throughout the life span, and the relationship of this cumulative exposure with PTSS. In contrast, most existing studies have examined only one type of abuse (i.e., physical, sexual, or psychological abuse), or have focused specifically on the consequences of witnessing PH against the mother. Third, most existing studies have been conducted among clinical samples of children and adolescents, whereas we examined a random sample of university students in the Palestinian Authority. This enabled us to reach young adults who have never been abused and/or have never witnessed PS and PH in their families, as well as young adults who have been exposed to those types and patterns of family violence at various levels of intensity, frequency, and severity. Moreover, we were able to reach young adults from heterogeneous backgrounds in terms of socioeconomic status, participants’ gender and age, parents’ age and level of education, family size, religious affiliation, type of locality of residence, quality of housing, and so forth.
Despite these strengths, several limitations of the study need to be taken into account. First, the CTS was not used to measure the context in which the participants were exposed to PS and PH. Nor were the participants asked about their interpretation of aggression and violence during their childhood, adolescence, and young adulthood. Thus, the study did not examine the relationship between the participants’ perceptions of different patterns of family PS and PH during each of these three periods of time on the one hand, and their levels of PTSS on the other. Second, it is possible that the participants had forgotten or repressed some of the PS and PH that they were exposed to as children and adolescents or even as young adults, and that they provided only partial reports. This might have influenced the strength of the relationship between exposure to PS and PH and PTSS.
Third, in this study, we relied on scales developed in Western, post-industrial societies as measures of PS, PH, perceived psychological adjustment of parents, and PTSS. This limitation derives from the dearth of measures that originate in Arab societies in the social, psychological, behavioral, and family sciences. Undoubtedly, the availability of such measures would have strengthened the validity of our results. Hence, concerted efforts should be made to ensure that in future studies, such scales will only be used after they have been adapted and adjusted to the sociocultural and sociopolitical contexts of Palestinian society. Fourth, fathers’ and mothers’ psychological adjustment were measured in this study on the basis of the subjective perceptions of the participants (i.e., their offspring), rather than objectively, by asking each of the parents to report their own estimations of their psychological adjustment. Hence, participants’ perceptions of the psychological adjustment of their parents might be confounded by their exposure to family violence. To alleviate this problem, future studies in this field should aspire to involve the parents in measuring their psychological adjustment. Furthermore, the parents should be asked to report on different patterns of their aggressive and violent behavior against each other and against their offspring. This measurement procedure may enhance the reliability and validity of reporting family violence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.