
Abstract
To reduce the many adverse health outcomes associated with intimate partner violence (IPV), high-risk groups need to be specifically targeted in the fight against domestic violence in India. This study aims to examine the prevalence and correlates of IPV in HIV-positive and HIV-negative women from India. A convenience sample of HIV-positive and HIV-negative women responded to questionnaires to assess their experience and perception of violence. Multivariate logistic regression analysis was used to model the association between IPV and age, education, employment status, contraception use, age at first marriage, and HIV status. Although adjusting for age, education, employment status, contraception use, age at first marriage, and HIV status, women who are employed were 3.5 times more likely to suffer IPV (confidence interval [CI] = [1.5, 8.5]), women aged 18 or above at first marriage are 0.3 times less likely to face IPV (CI = [0.1, 0.6]), and women who use contraception are 7 times more likely to suffer IPV (CI = [1.4, 30.2]). Also, HIV-positive women are 3 times more likely to face sexual violence compared with HIV-negative women (CI = [1.1, 7.6]).
Introduction
The dual epidemic of HIV and intimate partner violence (IPV) is a global phenomenon affecting millions of women (Aklimunnessa, Khan, Kabir, & Mori, 2007; Babu & Kar, 2009; Koenig, Ahmed, Hossain, & Mozumder, 2003; Naved & Persson, 2005). The World Health Organization (WHO) reports that 15% to 71% of women faced IPV (including both physical and sexual violence) at some point in their lives thus placing them at a high risk of acquiring HIV infection (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). This is a growing public health concern because victims of IPV are at high risk for adverse health outcomes beyond the physical injury caused by the IPV (Babu & Kar, 2009; Chandrasekaran, Krupp, George, & Madhivanan, 2007; Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008; Koenig, Ahmed, et al., 2003; Mahapatro, Gupta, & Gupta, 2012; Martin, Tsui, Maitra, & Marinshaw, 1999; Spiwak, Afifi, Halli, Garcia-Moreno, & Sareen, 2013).
In India, the national adult HIV prevalence has declined from 0.41% in 2000 to 0.27% in 2011 (National AIDS Control Organization [NACO], 2010). The estimated number of new HIV infections has also declined from 270,000 in 2000 to 116,000 in 2011 (NACO, 2010). Although new HIV infections have declined by more than 57% over the past decade, in 2011, women still account for about 39% (.816 million of the 2.09 million) of people living with HIV and AIDS in India (NACO, 2010).
Researchers, clinicians, and public health personnel are increasingly becoming aware that women are more vulnerable to HIV infection partly because of deep-rooted gender inequalities and violence (Aklimunnessa et al., 2007; Boyle, Georgiades, Cullen, & Racine, 2009; Rao, 1997). The male-dominant culture in India severely limits a woman’s ability to negotiate safe sex in an intimate partner relationship and an attempt to negotiate may even incite domestic violence (Decker et al., 2009; Ghosh & Choudhuri, 2011; Go et al., 2003; Mahapatro et al., 2012). The National Family Health Survey–2 (NFHS II) in India has shown that the HIV prevalence was higher among married women indicating physical and sexual abuse within the context of marriage (Decker et al., 2009). In such a setting it is important to understand the intersection of HIV and domestic violence because successful attempts to reduce HIV prevalence must also entail interventions to reduce domestic violence.
There are several community-based studies examining the intersection of HIV and violence comparing HIV-positive and HIV-negative women. Several studies carried out in the United States have consistently failed to find a significant difference in rates of physical, sexual, or emotional abuse by an intimate partner when comparing HIV-positive and HIV-negative women (Burke, Thieman, Gielen, O’Campo, & McDonnell, 2005; Cohen et al., 2000; Laughon et al., 2007). However, many other studies from sub-Saharan Africa have found the risk of IPV to be consistently higher among HIV-positive women (Chin, 2013; Jewkes, Dunkle, Nduna, & Shai, 2010; Kiarie et al., 2006; Maman et al., 2002).
The aim of this study was to examine the prevalence of IPV in HIV-positive and HIV-negative women in a setting where HIV-positive women have undergone informal social support intervention. To the best of our knowledge, this is the first article that links HIV and IPV in a sample of HIV-positive and HIV-negative married women.
Method
Between January and June 2010, 100 married couples with at least one HIV-positive partner and 100 married couples in which neither partner was HIV-positive were asked to complete a questionnaire regarding household characteristics, history of violence, attitude toward violence, and consequences of violence. The survey was conducted in Belgaum, Karnataka, India.
The HIV-positive couples were recruited from Spandana, a Non-Governmental Organization (NGO) group catering to people affected with HIV, and the uninfected couples were recruited from the Outpatients Department at Karnatak Lingayat Education (KLE) Society Dr Prabhakar Kore Hospital. All the couples were informed about the survey and were told that their participation is completely voluntary and that their refusal will not affect the treatment and care they receive at the center. They were assured complete privacy and confidentiality regarding the personal information shared by them. The participants spend 30 to 40 min to complete the survey. Three couples in HIV-positive group and 10 couples in the HIV-negative group refused to participate in the survey. The Study was approved by the local institutional ethics committee at KLE University.
The questionnaire included sections on demographic information, partner and household characteristics, history of violence, attitude toward violence, and consequences of violence. The questionnaire also explored decision making in the family, the respondents’ opinions regarding a wife’s rights, and reasons for quarrels in the family. Respondents had the option not to answer any question if it made them uncomfortable. Unanswered questions were counted as missing data in our analysis and as such some of the variables in our tables do not add up to 100%. Respondents routinely did not answer questions on level of income, drug-related questions, and questions asking about violence faced in the past 6 months. These variables were excluded from the analysis due to lack of sufficient data.
After obtaining consent from the participants, the husband and the wife were each taken individually to a private room for the questionnaire to ensure that the answers provided by the wives are not biased as a result of the presence of their husbands. The questionnaire was administered verbally in the local language. After completion of the questionnaire similar counseling was again provided to each couple. The analysis for this investigation focuses only on the responses from the wives. For the purpose of this study, a woman in an HIV-positive couple was analyzed in the HIV-positive group and will be referred to as an HIV-positive woman, whether or not the woman was the HIV-positive partner.
Demographic data collected from the wives includes age, employment status, religion, family structure (joint or nuclear and the number of family members in the household), number of marriages, education level, contraception use, and exposure to media. We compared the women in the HIV-positive group and the HIV-negative group to determine if there were significant differences in socio-demographic profile. We also looked for significant differences in the percentage of women who have had quarrels with their partners, their reason for these quarrels and the nature of assault (if any) faced by the women in these two groups.
To indicate the level and type of domestic violence experienced by the wives in this sample, three dependent variables (Physical Violence, Sexual Violence, and Lifetime IPV) were created based on previous studies (Aklimunnessa et al., 2007; Chin, 2013; Decker et al., 2009) The questionnaire asked “Were there any circumstances or family disagreement which caused your husband to do any of the following?” Possible responses were “Push or shake you; Throw something at you; Punch you with his hand; Kick you or drag you; Slap you or twist your arm; Attempt to strangle, kill, or burn you.” A woman who answered “yes” to any one of these questions was categorized as having faced physical violence (Aklimunnessa et al., 2007; Chin, 2013). A woman who was physically forced to have sexual intercourse even when she did not want to was categorized as having faced sexual violence (Aklimunnessa et al., 2007; Chin, 2013). A woman was identified as being a victim of lifetime IPV if she has ever faced any form of violence, including physical violence and sexual violence (Aklimunnessa et al., 2007; Decker et al., 2009). Recent physical violence was defined as reporting at least one type of physical assault in the last 12 months prior to the questionnaire.
In addition to the history of violence, we also explored the perception of violence in the HIV-positive and HIV-negative groups. We also compared what the two groups perceived as appropriate husband–wife behavior in relation to domestic violence and negotiating safe sex practices.
Three multivariate logistic regression models were used to model physical violence, sexual violence, and lifetime IPV with the wives age (<30 years, ≥30 years), education level (none, primary school, secondary school, tertiary education), employment status (currently working or not working), age at first marriage (<18 years, ≥18 years), contraception use (yes/no), and HIV status (yes/no).
The p values in the tables were calculated using t tests to compare average age, hours of work, and number of people in household. Mantel–Haenszel tests were utilized for comparing HIV status with the variables education, exposure to media, and contraception use. We used chi-square tests to see if there are any differences between the HIV groups in relation to employment status, religion, family type, contraception use, access to electricity, access to running water, whether a couple has quarrels, forced sex, opinion about situations in which a wife deserves to be beaten, and whether it is acceptable to ask for condoms or refuse sex in certain situations. Fisher’s exact test was applied to compare the number of marriages to HIV status. For the reasons for quarrels and nature of assault (both overall and in the past 12 months), chi-square tests were applied when expected frequencies were above five and Fisher’s exact test was used when expected frequencies were less than five.
Results
A total of 199 married couples participated in the survey, among them 99 were HIV-positive couples and 100 were HIV-negative couples. Out of the 99 HIV-positive couples, 80 of the wives were HIV-positive. The mean age of the women in the HIV-positive couples was 29.9 years compared with 34.7 years for the HIV-negative couples which was found to be statistically significant (p = .001). More than 85% of the women identify as Hindu. The family structure did not differ significantly between the two groups. About 7.1% of HIV-positive women had formal education beyond secondary school as did 12% of HIV-negative women (p = .228). About 9.1% of HIV-positive women had been married more than once, whereas all the HIV-negative women were married only once. Twelve of the women in the HIV-positive group reported using some form of contraception, of these women the majority used condoms or intra-uterine device (IUD; 83.3%). In the HIV-negative group, only 3% reported using contraception with oral contraceptive (66.7%) being the most common form of contraception used. This demographic data are displayed in Table 1.
Socio-Demographic Profile.

Reasons for quarrels within the couples and the nature and extent of any violence experienced by these women were explored. Compared with the HIV-negative women, a significantly higher proportion of HIV-positive women had quarrels with their spouse (79.8% compared with 67%). More than one quarter (28.3%) of the women in the HIV-positive group reported HIV/AIDS as a major reason for their quarrels. When asked about the types of physical assaults experienced, there was no significant difference between the two groups (Table 2). However, we did find that the HIV-positive group women reported significantly higher recent physical assault compared with the HIV-negative group women (p value = .014). Figure 1 displays the proportion of women in each group (HIV-positive group and HIV-negative group) who have ever experienced various types of domestic violence, including forced sex.
Reasons for Quarrels and Nature of Assault Faced by HIV-Positive and HIV-Negative Women.
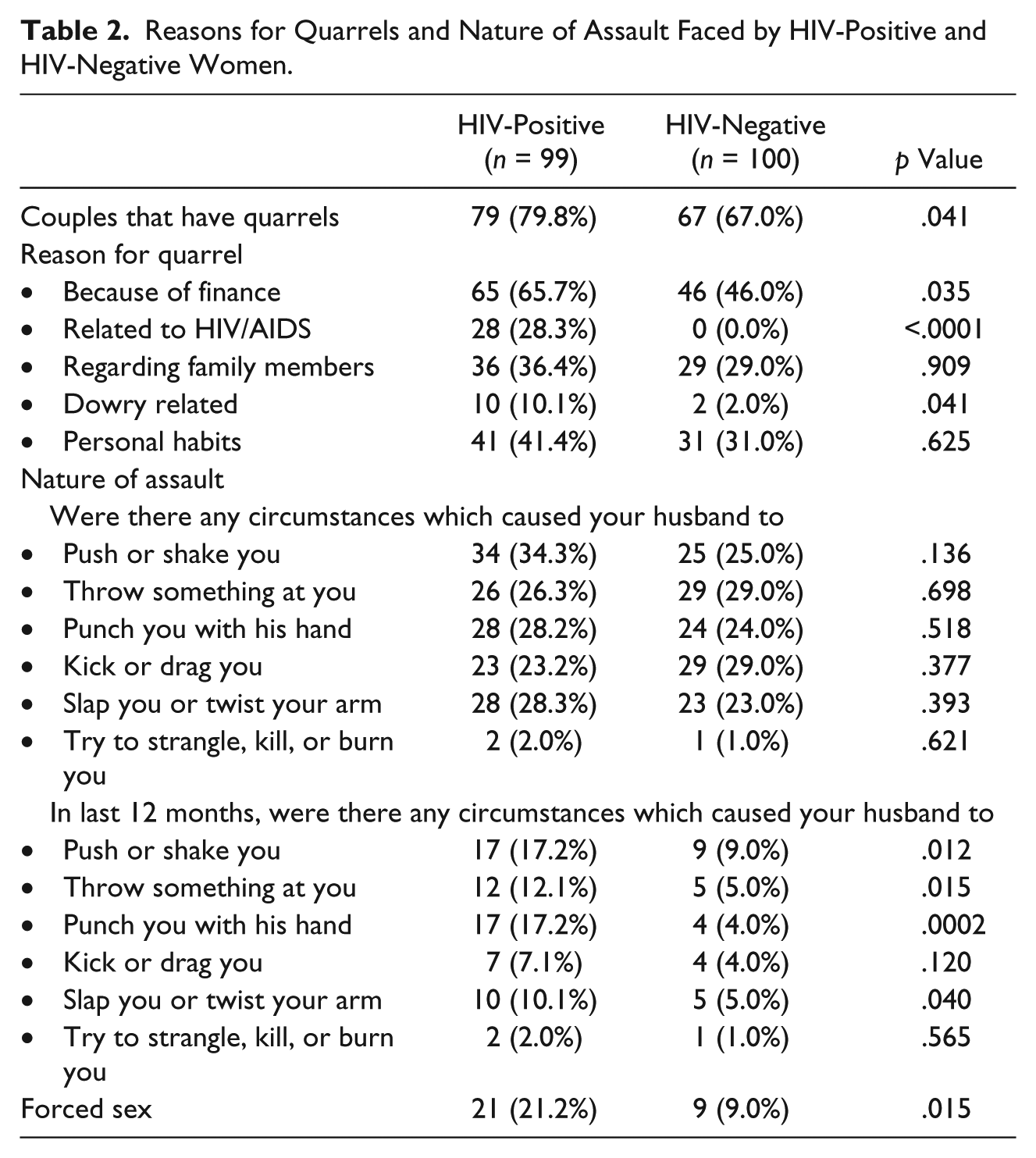
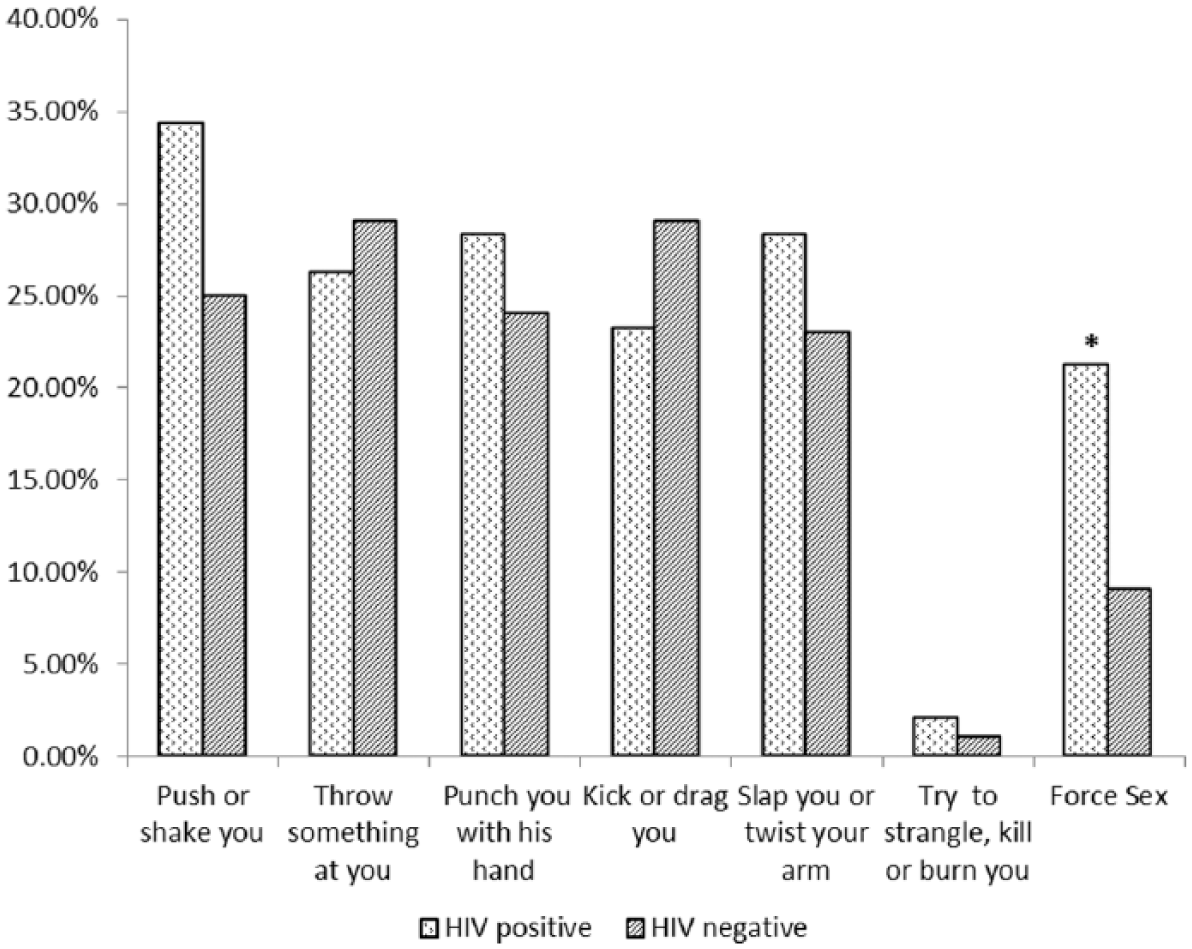
Nature of domestic violence experienced by HIV-positive and HIV-negative women.
Forced sex by the spouse was significantly higher in HIV-positive group women compared with the HIV-negative women (21.2% vs. 9.0%, p value = .015). One third (n = 7) of the women in the HIV-positive group who reported forced sex had retaliated, whereas the remaining two thirds surrendered to their partner’s wishes. Of the seven HIV-positive group women who opposed forced sex by their spouses, three were assaulted and suffered physical injuries. Two of these women sought medical care and required medical treatment. Of the nine HIV-negative women who experienced forced sex, none of them retaliated to this violence and did not experience any physical injuries.
Prevalence of IPV and sexual violence in our sample was 49.3% and 15.1%, respectively. Compared with women in the HIV-negative group, a higher proportion of women in the HIV-positive group experienced physical, sexual, and lifetime IPV. However, only sexual violence was significantly different between the two groups. Figure 2 displays the proportions of HIV-positive and HIV-negative groups who have ever faced physical violence, sexual violence, and lifetime IPV.

Types of domestic violence experienced by HIV-positive and HIV-negative women.
More than half of the women in both HIV-positive and HIV-negative groups believed that neglecting their children or arguing with their spouse is justification for their husband beating them. About 41.4% of HIV-positive women and 24% of HIV-negative women believe that if a woman refuses her husband sex, her husband is justified in reprimanding her. The top two methods of punishment reported in both groups are forced sex and hitting/beating. About 79.4% of all women in this study feel that there are situations when a man is justified in slapping their wife in the face, but only 7% of women feel that there are situations where a woman is justified in slapping her husband in the face (Figure 3). The majority (78.8%-79.8%) of HIV-positive women feel that it is acceptable to ask their husband to use condoms or refuse sex when it is known that the husband is having sex with other women, whereas the majority (67%) of HIV-negative women either disagree or are not sure (p ≤ .0001). Table 3 shows the distributions of responses.
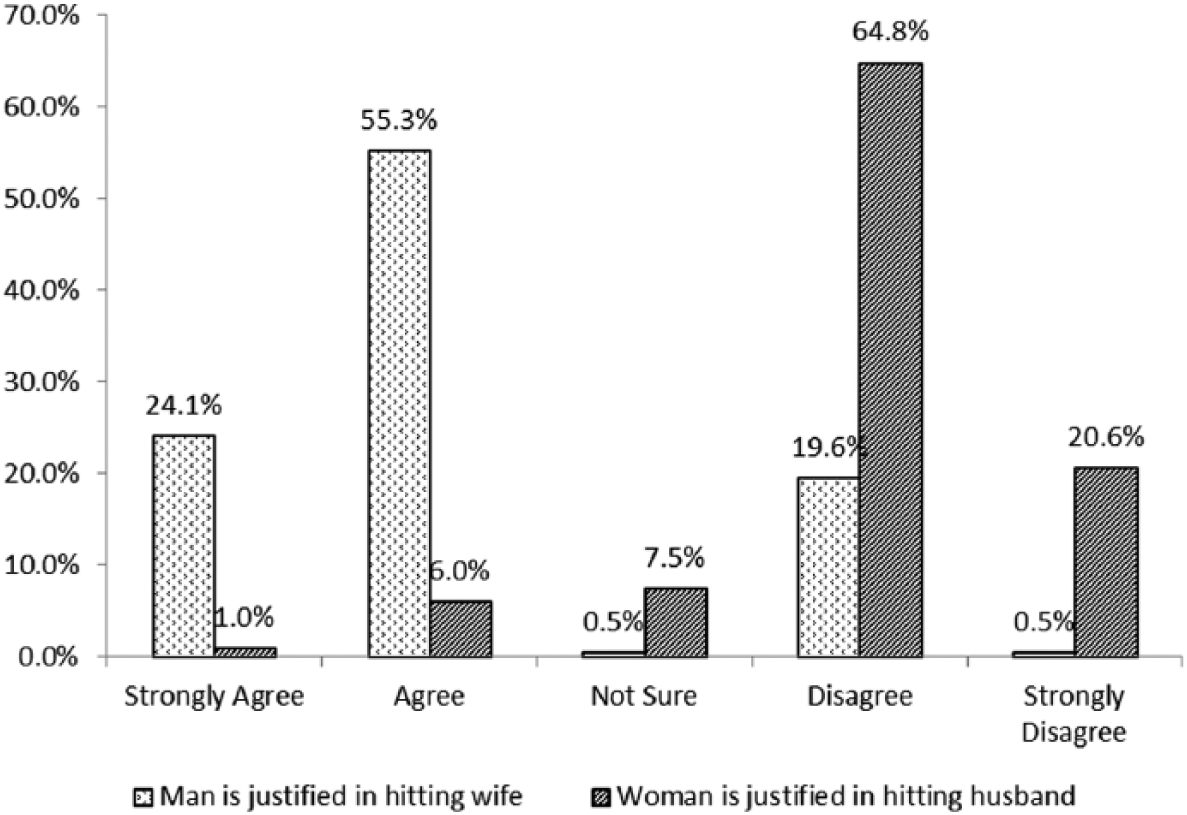
Women’s perception of justified violence between married couples.
Perception of Acceptable Behavior by HIV Status.

Multivariate logistic regression results are shown in Table 4. In our model, women who are employed are 3.3 times more likely to suffer physical violence (confidence interval [CI] = [1.4, 7.9]; p = .007) and 3.5 times more likely to suffer lifetime IPV (CI = [1.5, 8.5]; p = .005). Women who were 18 or above when they first got married were less likely to face any physical violence (odds ratio [OR] = 0.3; CI = [0.1, 0.6]; p = .001) or lifetime IPV (OR = 0.3; CI = [0.1, 0.6; p = .001). It is interesting to note that women who use contraception appear to be at higher risk of physical violence (OR = 7.7; CI = [1.8, 33.1; p = .011) and lifetime IPV (OR = 7.0; CI = [1.6, 30.2]; p = .019). HIV-positive women are 3 times more likely to face sexual violence compared with the HIV-negative women (CI = [1.2, 7.6]; p = .023).
Adjusted Multivariate Logistic Regression Models.

Note. IPV = intimate partner violence; OR = odds ratio; CI = confidence interval.
Highlighted in bold are significant associations at α=.05 level.
ORs are adjusted for age, education, employment status, age at first marriage, contraception use, and HIV status.
p < .05. **p < .01. ***p < .001.
Discussion
In this study, married women in couples where at least one of the partners is HIV-positive were younger and more likely to use contraception (especially barrier contraception) compared with married women in couples in which neither partner was HIV-positive. There was no difference in other individual or household characteristics, particularly education, employment, religion, exposure to media, and access to electricity and running water. Nevertheless, HIV-positive women were more likely to experience couples quarrels, recent physical violence, and forced sex.
Women who were age 18 years or above when married are much less likely to face physical violence compared with women who were less than 18 years of age when they got married. It appears that being older has a protective effect on IPV. One reason for this could be that women who are less than 18 years of age when they are married are more vulnerable to abuse as they have less control/power within their marriage and have little to no negotiation skills (Silverman, Decker, Saggurti, Balaiah, & Raj, 2008; Yount & Li, 2010).
Significant associations were also found between employment status and lifetime IPV Women who are employed are significantly more likely to face domestic violence. This finding is consistent with other studies (Babu & Kar, 2009; Chin, 2013; Koenig, Ahmed, et al., 2003; Mahapatro et al., 2012). One reason is that women who work tend to come into contact with men who are unrelated, which in societies such as India can be seen as provocative, hence these women may face more abuse from their spouses at home (Koenig, Ahmed, et al., 2003; Naved & Persson, 2005). In some cases, these women work only due to financial stress in the household which could be the underlying cause of tension and abuse. Another theory is that a woman earning an income changes the power dynamics in a marriage which increases stress in the relationship, leading to possible abuse.
Several studies have reported an association between education and domestic violence (Aklimunnessa et al., 2007; Boyle et al., 2009; Koenig, Ahmed, et al., 2003; Yount & Li, 2010); however, our study did not find any significant trends. One reason for this is our non-random selection of participants which means that our sample is non-representative of all couples in India. Hence, the distribution of level of education among HIV-positive and HIV-negative respondents would differ leading to an inability to detect any associations.
Previous research has shown that IPV significantly increases risk of HIV infection among women (Bauer et al., 2002; Decker et al., 2009; Molitor, Ruiz, Klausner, & Mcfarland, 2000; Sareen, Pagura, & Grant, 2009; Silverman et al., 2008), but the reverse also appears to be true. Our study found that HIV-positive women have an increased odds (OR = 3.0; CI = [1.2, 7.6]) of being sexually abused by their spouses compared with women who are HIV-negative, which is consistent with studies undertaken in sub-Saharan countries (Chin, 2013; Koenig, Lutalo, et al., 2003; Maman et al., 2002; van der Straten et al., 1998). One possible explanation is that HIV/AIDS can initiate arguments between couples which could in turn lead to physical and even sexual violence (Chin, 2013; Hoffman, Demo, & Edwards, 1994; Hurtado, Ciscar, & Rubio, 2004). About 28% of HIV-positive women reported HIV/AIDS as a major reason for quarrels with their spouse, 44% of whom also reported forced sex by their spouse.
A limitation of this study is disclosure-related bias leading to an underestimation of the true prevalence of domestic violence. The results from this study show that 79.4% of women feel that there are situations where their husband is justified in beating their wife for perceived bad behavior. Other studies from many different countries report similar perception of domestic violence (Aklimunnessa et al., 2007; Garcia-Moreno et al., 2006; Kim & Motsei, 2002; Maman et al., 2002; Yount & Li, 2010). As such, the women in this study may not have reported violence they felt they deserved. If the women overlooked everyday behavior resulting in less severe forms of assault, this could result in our data underestimating the true prevalence of IPV (Ellsberg et al., 2008; Mahapatro et al., 2012). The sensitive nature of our questions may also add to this underestimation as the women may not be willing to disclose violence for fear that their husband will beat them for speaking out. Hence, the data presented in this article should be viewed as the minimum level of violence actually experienced when planning health promotion and prevention strategies.
Another important consideration is the cultural context in which prevention programs are targeted. In India, the cultural and societal structures oppress women from being able to negotiate safe sex even when it is known that their husband is having sexual relations with other women (Babu & Kar, 2009; Go et al., 2003; Silverman et al., 2008). This perception appears to differ according to HIV status. Our study found that the majority (67%) of HIV-negative women are either unsure or disagree that it is acceptable to negotiate safe sex practices compared with 20% of HIV-positive women. This mind-set may make it difficult to establish safe sex practices in non-infected domiciles.
To reduce the prevalence of IPV in India, there is a need for counseling and support services for HIV-positive women who are at high risk for experiencing IPV. It is also important to consider a wide-scale program targeting men to alter gender norms in a culture which encourages domestic abuse. The social structures in India create an environment where husbands feel that beating their wives is justified, sometimes even encouraged (Go et al., 2003; Jewkes et al., 2010). Meanwhile, there is no community support for wives who do face IPV (Boyle et al., 2009). Changing the mind-set of the people in India would not only allow women to speak openly to their husbands about safe sex practices but could also reduce domestic violence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.