
Abstract
Sleep disturbance is a significant public health issue that disproportionately affects survivors of interpersonal violence (IPV). This systematic review presents data on the relationship of IPV and sleep. Inclusion criteria for this review were studies that included subjects 18 years of age or older, used an IPV measure and sleep disturbance measure, and were published in a peer-reviewed journal in English. A total of 23 articles met full inclusion criteria and were included in the present review. Studies were largely cross sectional, were conducted in a wide range of clinical and nonclinical samples, and utilized a variety of measures to assess IPV (sexual violence, physical violence, or psychological aggression perpetrated by an intimate partner or sexual or physical violence by any perpetrator in childhood or adulthood) and sleep disturbances (both general sleep disturbance excluding specific sleep disorders and the two specific sleep disorders of insomnia and nightmares). The findings examined the prevalence and association of sleep disturbance in IPV samples from population and community studies, the prevalence and association of sleep disturbance in IPV studies, and the associations between post-traumatic stress disorder and sleep disturbance in IPV samples. All studies identified a relationship between IPV and sleep disturbance. The results of this review provide important information for clinicians, researchers, and policy makers on the prevalence of and relationship between IPV and sleep disturbance.
Approximately 5–10% of the general adult population in industrialized nations meet diagnostic criteria for insomnia, a condition characterized by consistent difficulty initiating or maintaining sleep (Chung et al., 2015; Ohayon, 2002). Sleep disturbance, a broad term encompassing both nondiagnostic sleep complaints (e.g., dissatisfaction with sleep, poor sleep quality [SQ], short duration sleep) and clinical sleep disorders (e.g., insomnia disorder, sleep apnea), is present in one fourth to one third of adults (Ohayon, 2002; Stranges, Tigbe, Gomez-Olive, Thorogood, & Kandala, 2012). Overall, sleep disturbance is a significant public health issue that disproportionately affects survivors of interpersonal violence (IPV). In the United States, nearly one in five women and 1 in 71 men report sexual violence by any perpetrator and one in three women and one in four men have experienced sexual violence, physical violence, or psychological aggression by an intimate partner. Further, 22.3% of women and 4.7% of men report symptoms of post-traumatic stress disorder (PTSD) as a result of intimate partner violence or sexual violence by any perpetrator (Black et al., 2011). Approximately 70% of individuals with PTSD report a sleep impairment (Ohayon & Shapiro, 2000) in the form of either nightmares and/or insomnia with insomnia representing the most common of all PTSD symptoms (McLay, Klam, & Volkert, 2010; Roszell, McFall, & Malas, 1991).
The relationship of sleep and IPV is complex. For instance, physical, psychological, and environmental elements contribute to the development and maintenance of insomnia among IPV survivors (Lalley-Chareczko et al., 2015; Pigeon et al., 2011). Environmental stress has been attributed as the most common precipitant of insomnia (Bastien, Vallières, & Morin, 2004; Pigeon & Cribbet, 2012). PTSD can heighten both physiological and cognitive arousal, which can worsen or maintain preexisting insomnia (Pigeon & Gallegos, 2015). Both disturbed sleep and IPV are associated with deleterious physical and mental health consequences. For example, sleep disturbance is related to increased mortality, obesity, diabetes, cardiovascular disease and hypertension, inflammation, anxiety, and depression (U.S. Institute of Medicine, 2006). The high rates of sleep disturbance and the physical and psychological effects of sleep disturbance among IPV survivors highlight the importance of understanding the relationship of IPV and sleep.
To date, only one review has been conducted examining the physical and mental health consequences of IPV on women that included studies on the impact of IPV on sleep (Dillon, Hussain, Loxton, & Rahman, 2013). The Dillon, Hussain, Loxton, and Rahman’s (2013) systematic review of 75 papers found that IPV was associated with a range of mental health issues, including PTSD, depression, anxiety, and sleep disorders, and poor physical health outcomes, including somatic disorders, chronic pain, and gynecological problems. The purpose of this article is to present an updated and systematic literature review specifically on the relationship of IPV and sleep. We examined the prevalence and association of sleep disturbance (both general sleep disturbance excluding specific sleep disorders and the specific sleep disorders of insomnia and nightmares) in IPV samples (e.g., exposure to sexual violence, physical violence, or psychological aggression perpetrated by an intimate partner or sexual or physical violence by any perpetrator in childhood or adulthood) from population and community studies, the prevalence and association of sleep disturbance in IPV studies, and the associations between PTSD and sleep disturbance in IPV samples.
Method
Data Sources and Searches
Based upon peer-reviewed guidelines to conduct systematic reviews established by the independent, nonfederal Task Force on Community Preventive Services (Zaza et al., 2000), we conducted a systematic review of the literature using PubMed (from 1946) and PsycINFO (from 1967) databases to May 31, 2017. Boolean search logic and medical subject headings (MeSH) terms were used to create the following a priori search term: [(interpersonal violence or intimate partner violence or domestic violence or domestic abuse) and (sleep disturbance or sleep or insomnia) and (posttraumatic stress disorder or traumatic stress or psychological trauma)].
Eligibility Criteria
Full-text articles were retrieved and evaluated for eligibility by all investigators. A priori inclusion criteria to determine study eligibility included: (1) study samples were adults ≥18 years of age, (2) the use of an IPV measure, (3) the use of a sleep disturbance measure, and (4) the article was published in a peer-reviewed journal in English (see Figure 1 for flow diagram of selection process). IPV was defined as sexual violence, physical violence, or psychological aggression perpetrated by an intimate partner or sexual or physical violence by any perpetrator in childhood or adulthood. This was based on the World Health Organization (WHO) definition and typology of violence that refers to IPV as violence between individuals and is subdivided into family and intimate partner violence (e.g., child, partner, elder) and community violence (e.g., acquaintance, stranger; Krug, Mercy, Dahlberg, & Zwi, 2002). Sleep disturbance was defined as general sleep disturbance excluding specific sleep disorders and the specific sleep disorders of insomnia and nightmares.

Flow diagram of study selection process.
Data Abstraction and Selection Process
The lead author reviewed all identified titles and abstracts to determine eligibility using the above criteria. Another study author reviewed the abstracts to determine inclusion for this review. Any discrepancies were brought to other study authors for consensus. We extracted information on population, gender, IPV type, sleep measure(s), sleep outcomes, and PTSD measure(s), and outcomes when available.
We utilized a standard data abstraction format as recommended by Zaza et al. (2000) to extract information from each article to promote consistency, reduce bias, and improve reliability and validity. Specifically, we entered information into a table format addressing four key areas: (1) classification information (design features, intervention characteristics), (2) descriptive details (sample, study eligibility, and setting), (3) quality assessment (i.e., descriptions, sampling, measurement, analysis, and interpretation of results), and (4) outcomes. This process allowed the authors to monitor and review articles, make comparisons across studies, and determine study validity.
Results
The literature search yielded a total of 415 abstracts. An initial review identified 56 abstracts as potentially relevant for this review. Of these 56 abstracts, 31 were identified for further full-text review. Subsequently, 23 articles met full inclusion criteria and were included in the present review. Studies were largely cross sectional, were conducted in a wide range of clinical and nonclinical samples, and utilized a variety of measures to assess sleep disturbances (see Tables 1 –3). Following the quality assessment guidelines recommended by Zaza et al. (2000), we assessed threats to validity using categories on descriptions, sampling, measurement, analysis, and interpretation of results. We found that the majority of studies were in the moderate-quality (30%) to high-quality (65%) range; one study (Rasmussen, 2007) was rated as low quality. The majority of studies examined the relationship between sleep and sexual violence, physical violence, or psychological aggression perpetrated by an intimate partner (n = 19). The relationship between sleep and sexual or physical violence by any perpetrator in childhood or adulthood was examined in four studies (Galovski, Monson, Bruce, & Resick, 2009; Galovski et al., 2016; Gutner, Casement, Stavitsky Gilbert, & Resick, 2013; Kelly, Skelton, Patel, & Bradley, 2011). We discuss the measures used to assess IPV and sleep, the prevalence and association of sleep disturbance in IPV samples from population and community studies, the prevalence and association of sleep disturbance in IPV studies, and the associations between PTSD and sleep disturbance in IPV samples.
Prevalence and Association of Sleep Disturbance in IPV Samples From Population and Community Studies.

Note. BRFSS = Behavioral Risk Factor Surveillance System; CTS = Conflict Tactics Scale; FIRST = Ford Insomnia Response to Stress Test; GSS = General Social Survey; IPV = interpersonal violence; PSQI = Pittsburgh Sleep Quality Index; SVAWS = Severity of Violence Against Women Scales; WAST = Women Abuse Screening Tool.
Prevalence and Association of Sleep Disturbance in IPV Studies.
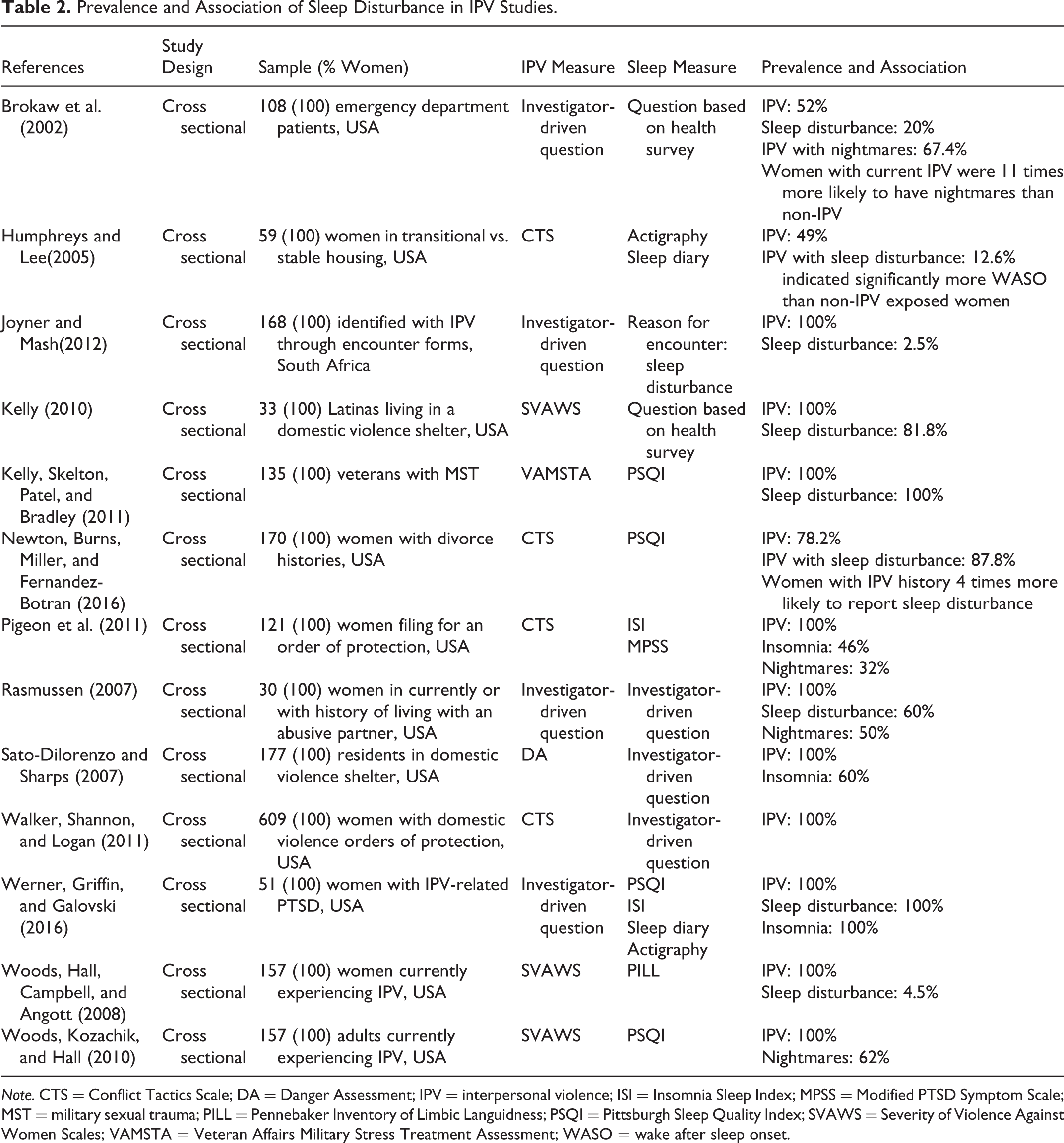
Note. CTS = Conflict Tactics Scale; DA = Danger Assessment; IPV = interpersonal violence; ISI = Insomnia Sleep Index; MPSS = Modified PTSD Symptom Scale; MST = military sexual trauma; PILL = Pennebaker Inventory of Limbic Languidness; PSQI = Pittsburgh Sleep Quality Index; SVAWS = Severity of Violence Against Women Scales; VAMSTA = Veteran Affairs Military Stress Treatment Assessment; WASO = wake after sleep onset.
Associations Between PTSD and Sleep Disturbance in IPV Samples.
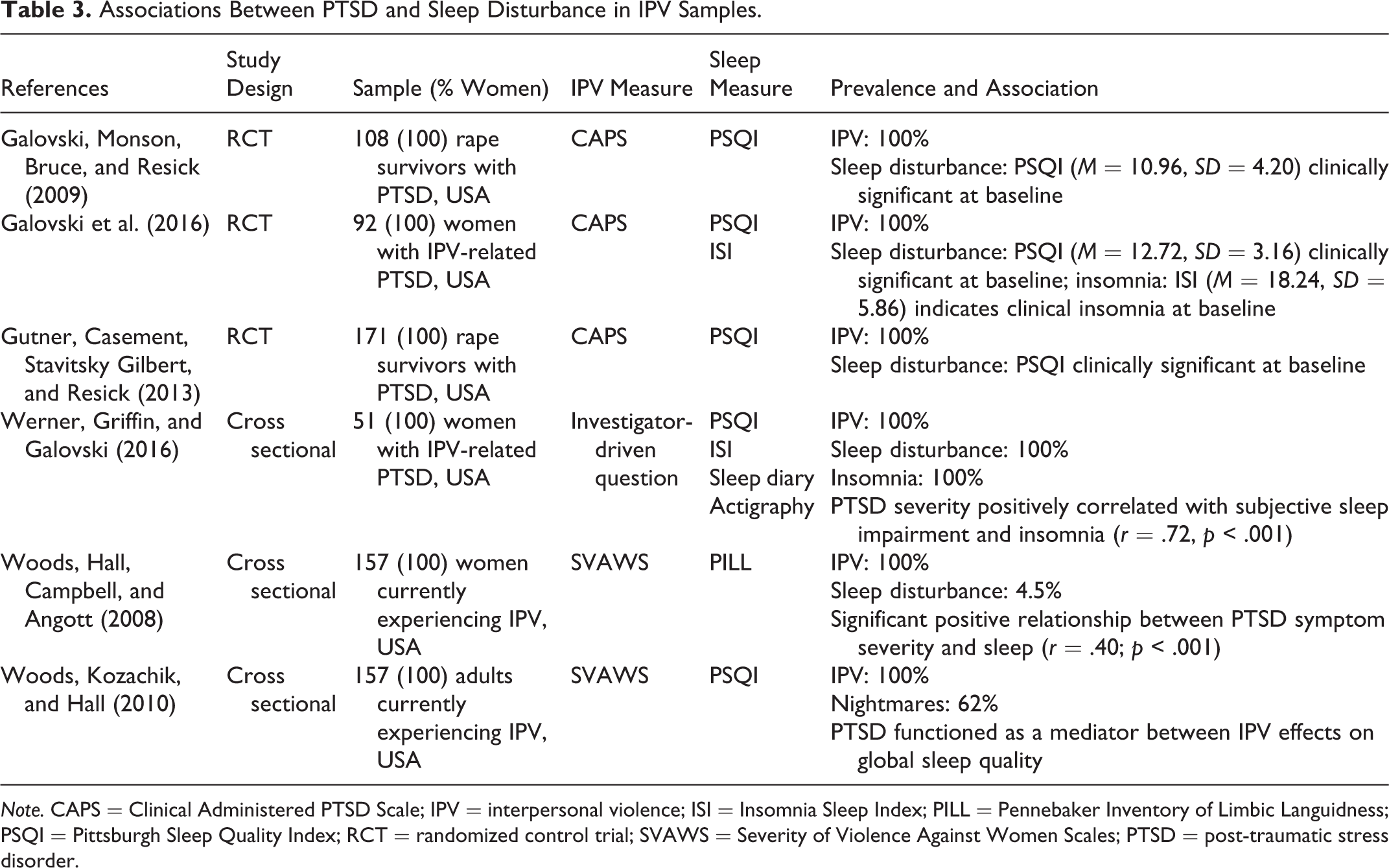
Note. CAPS = Clinical Administered PTSD Scale; IPV = interpersonal violence; ISI = Insomnia Sleep Index; PILL = Pennebaker Inventory of Limbic Languidness; PSQI = Pittsburgh Sleep Quality Index; RCT = randomized control trial; SVAWS = Severity of Violence Against Women Scales; PTSD = post-traumatic stress disorder.
Measures of IPV and Sleep
IPV
IPV measures and conceptualizations varied across studies, with 12 studies using validated measures, either adapted or in full (Ansara & Hindin, 2011; Humphreys & Lee, 2005; Kelly, 2010; Newton, Burns, Miller, & Fernandez-Botran, 2016; Pigeon et al., 2011; Rauer, Kelly, Buckhalt, & El-Sheikh, 2010; Romans, Cohen, Forte, Du Mont, & Hyman, 2008; Sato-DiLorenzo & Sharps, 2007; Svavarsdottir & Orlygsdottir, 2009; Walker, Shannon, & Logan, 2011; Werner, Griffin, & Galovski, 2016; Woods, Hall, Campbell, & Angott, 2008; Woods, Kozachik, & Hall, 2010), and seven studies using investigator-driven questions (Brokaw et al., 2002; Hathaway et al., 2000; Joyner & Mash, 2012; Kelly et al., 2011; Lalley-Chareczko et al., 2015; Rasmussen, 2007; Sanchez, Islam, Zhong, Gelaye, & Williams, 2016). The Conflict Tactics Scale (CTS/CTS-2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) was used with the highest frequency (n = 4), followed by the Severity of Violence Against Women Scale (n = 3; Marshall, 1992). Finally, the Women Abuse and Screening Tool (Brown, Lent, Brett, Sas, & Pederson, 1996) and the Danger Assessment (Campbell, Webster, & Glass, 2009) were each used once (Sato-DiLorenzo & Sharps, 2007; Svavarsdottir & Orlygsdottir, 2009). Investigator-driven questions were derived by the study authors or taken/adapted from larger epidemiological studies such as the Behavioral Risk Factor Surveillance System (BRFSS). The assessments measured physical violence (n = 16; Ansara & Hindin, 2011; Brokaw et al., 2002; Hathaway et al., 2000; Humphreys & Lee, 2005; Kelly, 2010; Kelly et al., 2011; Lalley-Chareczko et al., 2015; Newton et al., 2016; Pigeon et al., 2011; Romans et al., 2008; Sanchez et al., 2016; Svavarsdottir & Orlygsdottir, 2009; Walker et al., 2011; Werner et al., 2016; Woods et al., 2008), sexual violence (n = 12; Ansara & Hindin, 2011; Humphreys & Lee, 2005; Kelly, 2010; Kelly et al., 2011; Lalley-Chareczko et al., 2015; Pigeon et al., 2011; Romans et al., 2008; Sanchez et al., 2016; Svavarsdottir & Orlygsdottir, 2009; Walker et al., 2011; Werner et al., 2016; Woods et al., 2008), and psychological aggression (i.e., verbal abuse, coercive control; n = 9; Ansara & Hindin, 2011; Hathaway et al., 2000; Kelly, 2010; Kelly et al., 2011; Lalley-Chareczko et al., 2015; Pigeon et al., 2011; Rauer et al., 2010; Romans et al., 2008; Sanchez et al., 2016; Svavarsdottir & Orlygsdottir, 2009; Walker et al., 2011; Woods et al., 2008). Abuse generally defined and specifically by an intimate partner was measured by three studies (Joyner & Mash, 2012; Rasmussen, 2007; Sato-DiLorenzo & Sharps, 2007) and three studies measured IPV specific to military sexual trauma or rape by an unknown perpetrator (Galovski et al., 2009; Gutner et al., 2013; Kelly et al., 2011).
Sleep
Sleep measurement varied across studies. Many studies used health questionnaires that included a sleep item (n = 6; Ansara & Hindin, 2011; Brokaw et al., 2002; Hathaway et al., 2000; Lalley-Chareczko et al., 2015; Romans et al., 2008; Svavarsdottir & Orlygsdottir, 2009) or investigator-driven survey questions (n = 6; Joyner & Mash, 2012; Kelly, 2010; Newton et al., 2016; Rasmussen, 2007; Sato-DiLorenzo & Sharps, 2007; Walker et al., 2011). Validated sleep measures, the Insomnia Severity Index (ISI; Bastien, Vallières, & Morin, 2001), the Pittsburgh Sleep Quality Index (PSQI; Buysse, Reynolds, Monk, Berman, & Kupfer, 1989), and the Ford Insomnia Response to Stress Test (FIRST; Drake, Richardson, Roehrs, Scofield, & Roth, 2004) were used by seven studies (Galovski et al., 2016; Gutner et al., 2013; Newton et al., 2016; Pigeon et al., 2011; Rauer et al., 2010; Sanchez et al., 2016; Werner et al., 2016). The objective sleep measure included in two studies was wrist actigraphy (Humphreys & Lee, 2005; Werner et al., 2016). Humphreys and Lee (2005) and Werner, Griffin, and Galovski (2016) also used a sleep diary as a self-report measure.
Prevalence and Association of Sleep Disturbance in IPV Samples From Population and Community Studies
Data on the prevalence of sleep disturbance in IPV were assessed in large population-based and nationally representative samples from the United States, Canada, and Iceland (Ansara & Hindin, 2011; Hathaway et al., 2000; Lalley-Chareczko et al., 2015; Romans et al., 2008; Svavarsdottir & Orlygsdottir, 2009; Table 1). In the United States, data assessing 2,043 women from the 1998 Massachusetts BRFSS found that among the 6.3% of women reporting exposure to IPV, 53% reported “not getting enough sleep,” nearly double that of women without IPV exposure (Hathaway et al., 2000). Using data from the 2006 BRFSS (n = 34,975) wherein 20% had a lifetime prevalence of IPV, Lalley-Chareczko and colleagues (2015) found that all IPV variables were associated with sleep disturbance with rates of sleep disturbance 7–8 times higher among those reporting IPV in the past year, compared to those with no such exposure. Further, sleep disturbance partially mediated all relationships between IPV and mental and physical health. In the 1999 Canadian General Social Survey (GSS) of 25,876 respondents, the 21.2% of females reporting IPV indicated more medication use for sleep as compared to men (17.3% vs. 9.4%; Romans et al., 2008). Similarly, in the 2004 Canadian GSS of 23,766, of the 19.31% of respondents who reported IPV, women were more likely to take psychotropic medication to address sleep disturbances as compared to men (Ansara & Hindin, 2011). Using an investigator-driven questionnaire, Svavarsdottir and Orlygsdottir (2009) conducted a population-based survey among 2,746 Icelandic married and cohabitating women and asked IPV-related questions regarding their current partner or husband. The researchers found that sleep disturbance and current IPV (5.3% reported physical abuse, 34.9% reported psychological abuse, and 2.5% reported sexual abuse) predicted overall psychological (β = .23, p < .001) and physiological health status (β = .16, p < .001).
In a cohort study of pregnant Peruvian women (N = 634), lifetime exposure to IPV (33% of the sample) was associated with a 1.54-fold increased odds of stress-related sleep disturbance (as measured by the FIRST) and a 1.93-fold increased odds of poor sleep quality (as measured by the PSQI) as compared to women who had not experienced IPV (Sanchez et al., 2016). In a longitudinal, community sample of 241 married couples in which a large majority of husbands and wives reported receiving psychological abuse from their partner. The PSQI identified that 50% of husbands and 52% of wives reported significant sleep disturbance. The researchers found that sleep disturbances increased for both men and women relative to the amount of psychological abuse (Rauer et al., 2010).
Prevalence and Association of Sleep Disturbance in IPV Studies
General sleep disturbance
Among IPV samples from shelters, community health centers, and veteran cohorts, seven studies found general sleep disturbance, ranging from poor SQ to symptoms of insomnia (e.g., difficulty falling or staying asleep) in the absence of an insomnia diagnosis or measure of insomnia severity. Humphreys and Lee (2005) compared sleep using a convenience sample of female IPV survivors living in shelters to healthy controls living in a stable home environment (Humphreys & Lee, 2005). Using wrist actigraphy and subjective sleep measures, they found that IPV survivors needed significantly more time to fall asleep (15 min) and spent significantly more time awake in bed (12%) as compared to healthy controls (7%). Joyner and Mash (2012) examined medical records of women with IPV histories (N = 114) from community health centers in South Africa. Their findings indicated that 2.5% of the women presented with sleep disturbance. In a sample of Latina women living in an emergency shelter for IPV (N = 33), 81% reported difficulty falling or staying asleep (Kelly, 2010). Using the PSQI, Kelly, Skelton, Patel, and Bradley (2011) found clinically significant sleep disturbance in a sample of veteran women exposed to military sexual trauma. Of note, 95.4% of the veterans reported lifetime exposure to at least one non-military-related IPV-related trauma, the majority reporting sexual abuse as an adult civilian (77%). Another study also used the PSQI to determine sleep disturbance in divorced women from marriages with and without IPV (N = 170; Newton et al., 2016). They found that women with IPV histories were 4 times more likely to have disturbed sleep than women without IPV histories. Walker, Shannon, and Logan (2011) found that women with domestic violence orders of protection against male intimate partners (N = 609) slept an average of 5.5 hr per night. Using the Pennebaker Inventory of Limbic Languidness, Woods, Hall, Campbell, and Angott (2008) interviewed a sample of women currently experiencing IPV (N = 157) and found that 70.1% endorsed difficulty staying asleep or poor sleep, 73.9% endorsed difficulty falling asleep, and 63.7% endorsed waking early. In the sample, 88% of the women in the sample had a PSQI global score >5, indicating significant sleep disturbance (Woods et al., 2010). Woods et al. (2008) found a significant positive relationship between IPV and sleep disturbance, ranging from r = .23, p < .01, to r = .35, p < .001, with risk of homicide in their current intimate relationships as the highest correlation.
Insomnia
Using the ISI, Pigeon and colleagues (2011) examined a court sample of women exposed to IPV and found that 46% endorsed clinically significant insomnia and 53% had some form of insomnia. A total of 60% of residents in a domestic violence shelter endorsed insomnia (Sato-DiLorenzo & Sharps, 2007). Werner et al. (2016) found that female IPV survivors with PTSD endorsed moderately severe insomnia on the ISI.
Nightmares
Studies that reported on nightmares indicated a prevalence of weekly symptoms in 32–62% of IPV survivor respondents in samples from medical (Brokaw et al., 2002), transitional housing (Rasmussen, 2007), and court-based settings (Pigeon et al., 2011). An emergency department survey of IPV and nightmares among 108 women with a history of or current IPV exposure found that women with current IPV (n = 22) were 11 times more likely to have nightmares and women with IPV history (n = 34) were 5 times more likely to have nightmares as compared to women with no IPV history (n = 52; Brokaw et al., 2002). Using the Modified PTSD Symptom Scale (Falsetti, Resnick, Resick, & Kilpatrick, 1993) nightmare frequency and severity items, Pigeon and colleagues (2011) examined a court sample of women exposed to IPV and found that 32% endorsed moderate to severe nightmares at least one night per week. In sample of IPV-exposed women (N = 30) living in transitional housing or receiving services from a family counseling center, 50% of the sample experienced nightmares on a weekly basis (Rasmussen, 2007). This study, using an investigator-driven survey, found severe nightmare content containing graphic depictions of torture, falling, being chased, running, and murder (Rasmussen, 2007). Using the PSQI, Woods, Kozachik, and Hall (2010) found that 62% of a sample of women, primarily living in crisis shelters, endorsed nightmares at least 1–2 times per week.
Associations Between PTSD and Sleep Disturbance in IPV Samples
All of the clinical intervention studies examining a relationship between PTSD-related sleep disturbance in IPV, with varied clinical and community samples, reported a correlation between PTSD and poor sleep or that PTSD predicted poor SQ, insomnia, and/or nightmares (Table 3). The three randomized clinical trials included in this systematic review examined the effects of PTSD interventions on PTSD and sleep outcomes among female sexual assault survivors (Galovski et al., 2009, 2016; Gutner et al., 2013). Galovski, Monson, Bruce, and Resick (2009) examined sleep impairment in a sample of female rape survivors with PTSD (N = 108) who received cognitive processing therapy (CPT), prolonged exposure (PE), or minimal attention. Relative to the minimal attention group, sleep improved for women in the CPT and PE groups. Using the same study data (N = 171), Gutner, Casement, Stavitsky Gilbert, and Resick (2013) expanded upon Galovski and colleagues’ (2009) findings by assessing the long-term impact of CPT and PE on sleep efficiency, sleep onset latency (SOL), total sleep time (TST), and SQ changes. Both CPT and PE had large effects on insomnia and nightmare severity (Cohen’s d > .80, p < .001), moderate effects on perceived SQ (Cohen’s d > .50, p < .001), and small effects on SOL, TST (Cohen’s d > .20, p < .001). Treatment gains in sleep were maintained through the long-term follow-up (an average of 6 years posttreatment). Galovski et al. (2016) examined sleep-directed hypnosis as an augmentation prior to the delivery of CPT among women with PTSD related to IPV (N = 108). The augmentation of CPT with hypnosis improved sleep, but there were no differences with PTSD symptoms relative to the control condition.
Woods et al. (2008) examined PTSD and sleep among women currently experiencing IPV and living in crisis shelters (N = 157). They found a significant positive relationship between PTSD symptom severity and sleep (r = .40; p < .001). Further, PTSD avoidance was a significant predictor of sleep disturbance in this sample. Using the same sample, Woods et al. (2010) found that PTSD functioned as a mediator between IPV effects on global SQ. Walker et al. (2011) examined predictors of sleep disturbance among a sample of women with orders of protection against violent partners (N = 609). Their findings indicated that PTSD symptoms were a significant predictor of sleep disturbance. Werner et al. (2016) examined the consistency of subjective (PSQI, ISI) and objective (wrist actigraphy) sleep measures in a cohort of female IPV survivors with PTSD (N = 51) and found that PTSD severity was positively correlated with subjective sleep impairment and insomnia (r = .72, p < .001). However, no significant correlations between subjective and objective reports were found.
Discussion
Overall, the current review identified that sleep disturbance is widely prevalent among individuals exposed to IPV and strongly associated with IPV and related morbidity across a variety of study designs and study populations. There is, however, great heterogeneity in how clinicians and researchers define IPV and assess abuse within clinical and research settings. Not surprisingly, the current review revealed that studies vary widely on their assessment of IPV. It is possible that with consistent definitions and assessments across settings, we might find more consistent patterns regarding the intersections between sleep and abuse. Some of these studies include convenience samples found in specialty settings among help-seeking survivors, who may be at a different point in their abuse trajectories. For example, an individual living in a domestic violence shelter may have decreased safety concerns, which could possibly decrease disturbed sleep over time. While the last decade has seen a proliferation on studies which explore the impact of violence in the lives of both men and women, most studies on IPV and sleep have been conducted on cohorts of women, perhaps due to these convenience samples. Nonetheless, estimates from large samples suggest that among all individuals exposed to IPV, 28.5% of men have experienced sexual violence, physical violence, or psychological aggression by an intimate partner and 1.4% of men have experienced sexual violence by any perpetrator (Black et al., 2011). In the studies we reviewed, four studies assessed gender differences (Ansara & Hindin, 2011; Lalley-Chareczko et al., 2015; Rauer et al., 2010; Romans et al., 2008). Among these studies, greater sleep disturbances were reported among women as compared to men (Ansara & Hindin, 2011; Romans et al., 2008), but when present, sleep disturbance was associated with increases in intensity and severity of violence for both men and women. In addition, although some studies included in this review studied racially and ethnically diverse samples, no study compared outcomes based on race or ethnicity. Therefore, we cannot glean from these studies how sleep and IPV may impact those who self-identify as coming from underrepresented minorities.
Implications for Practice
This review supports the necessity and importance of a holistic approach to delivering mental and physical health care for IPV survivors. Specifically, for clinicians working with survivors of IPV, routinely assessing for sleep disturbance can guide clinical referrals for patients dealing with chronic or acute sleep disruptions that are likely to adversely affect their health, well-being, and capacity to cope. Conversely, clinicians treating sleep disturbance must be aware of potential IPV concerns, routinely screen and assess for IPV, and be prepared to appropriately provide resources to address IPV concerns such as safety or legal issues. The results further suggest the adoption of a trauma-informed model of care for clinicians who work with individuals with sleep disturbances. Having a trauma-informed approach might facilitate engagement of individuals with IPV and help them understand how exposure to IPV and sleep disturbance are interconnected (Elliott, Bjelajac, Fallot, Markoff, & Reed, 2005), leading to improved treatment outcomes. It has been suggested, for instance, that managing sleep problems may improve adherence to and retention in trauma-focused therapies (Galovski et al., 2016; Pigeon et al., 2015). Given the science emerging around the intersections of sleep and IPV, it is advisable to consider how providers in clinical practices and social service agencies can work collaboratively to deliver best care practices. Organizations might consider cross-agency waivers of confidentiality so sleep providers and safety advocates can work together to create safety plans, offer protection orders, and help survivors navigate their sleep behaviors. In that way, the survivors are treated in a holistic way, offering them biopsychosocial responses to their violence experiences. Integrated care, often called collaborative care, is a new approach that might benefit from considering sleep assessments (and provide either direct care for or appropriate referrals for sleep treatment) in the context of lived violence experiences.
Implications for Policy
For many years, research on IPV and sleep have been largely disconnected. Recently, funding agencies recognize the need for team science and the social determinants of health approach promulgated by the WHO. This model suggests that health is grounded on a number of areas of one’s life: individual needs, interpersonal relationships, community surroundings, and state and federal statutes around basic needs such as housing, food, and safety. While the Affordable Care Act recommends screening for all women in childbearing years, legislators might consider amendments that recommend screening all patients for IPV, including men and women across the life span. Whereas both public and private health-care systems that provide mental health care may more routinely or readily screen for IPV, a focus on screening in other health-care settings is important. This is increasingly implemented in primary care settings. Here, we suggest that specialty care settings, especially those providing sleep medicine services, may be enlisted to help realize universal screening. At the same time, sustainable mechanisms for providers to bill for necessary clinical assessments of those who screen positive for IPV currently falls outside many organizations’ routine billable services and thus requires modifications to existing systems. Further, sleep improvement providers would need training in how to screen, assess, and refer for IPV services to be sure they are doing so in a safe manner. For example, a survivor receiving an explanation of benefits at home that includes screening and safety planning may be at risk if the perpetrator is either the enrolled benefit subscriber and/or the monitoring mail.
Implications for Research
The majority of studies in the current review were cross sectional underscoring the need for longitudinal, observational studies to further elucidate the relationship between IPV and sleep. For example, does the type of IPV exposure (e.g., sexual, physical) or the perpetrator (e.g., any perpetrator or intimate partner) predict the type of sleep disturbance? Further, does one’s level of danger predict sleep patterns? Similarly, it is unknown to what extent the relationships observed in the current review are mediated or moderated by mechanisms that are similar or different than those posited to exist between PTSD and sleep more broadly such as abnormal rapid eye movement (REM) sleep processes, fear-enhanced memory processes, and maladaptive stress responses at the level of behaviors, cognitions, and/or psychobiologic processes (Germain, 2013). Clinical trials are also needed to determine how to best treat IPV survivors who may present with some combination of insomnia, nightmares, depression, anxiety, and/or PTSD.
Conclusion
IPV is a pervasive public health problem that has many implications for the physical and mental health of survivors. This review sheds new light on the magnitude of the co-occurrence of IPV and various sleep disturbances. Additional research is needed to disseminate evidence-based or evidence-informed, interventions, and policies which can improve sleep and health, thus improving survivors’ qualities of life.
Implications for Practice, Policy, and Research
Practice
Clinicians treating sleep disturbance must be aware of potential interpersonal (IPV) concerns, routinely screen and assess for IPV, and be prepared to appropriately provide resources to address IPV concerns such as safety or legal issues.
For clinicians working with victims/survivors of IPV, routinely assessing for sleep disturbance can guide clinical referrals for victims dealing with chronic or acute sleep disruptions.
Patients may be better able to adhere to sleep medications and routines if their safety issues are addressed.
Policy
Sleep providers may determine it is beneficial to create memorandums of understanding to work with IPV providers locally, including waivers for providers to be able to talk together using case conferencing.
Providers may want to explore the Affordable Care Act to understand how to effectively screen for IPV in an affordable way that offers staff ample time to conduct routine inquires that are using best practice guides.
Research
There is a need for longitudinal, observational studies to further elucidate the relationship between IPV and sleep.
It is unknown to what extent the relationships observed in the current review are mediated or moderated by mechanisms that are similar or different than those posited to exist between PTSD and sleep more broadly.
Clinical trials are also needed to determine how to best treat IPV survivors who may present with some combination of insomnia, nightmares, depression, anxiety, and/or PTSD.
Critical Findings
All of the studies in this review reported a relationship between IPV and a broad range of sleep disturbance. In epidemiological samples, prevalence of IPV exposure ranged from 6.3% to 35%. In epidemiological samples, sleep disturbance was found in up to 29% of respondents and 53.1% of respondents with IPV exposure. Studies examining insomnia and IPV found that 46–100% of respondents endorsed moderate to severe insomnia. Studies that reported on nightmares among IPV survivors indicated a prevalence of weekly symptoms in 32–62% of respondents.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official view of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Autumn M. Gallegos was supported by the University of Rochester CTSI Award KL2 TR001999 from the National Center for Advancing Translational Sciences of the National Institutes of Health. Nicole Trabold was supported by a U.S. Department of Health and Human Services, National Institutes of Health, National Research Service Award T32MH20061 (Dr. Conwell, Private Investigator) and University of Rochester CTSI Award (KL2 TR001999).