
Abstract
Child maltreatment contributes to depression in adults. Evidence indicates that such experiences are associated with poorer outcomes in treatment. Mothers in home visiting programs display high rates of depression and child maltreatment histories. In-Home Cognitive Behavioral Therapy (IH-CBT) was developed to treat maternal depression in home visiting. The purpose of this study was to examine the moderating effects of child maltreatment history on depression, social functioning, and parenting in mothers participating in a clinical trial of IH-CBT. Ninety-three depressed mothers in home visiting between 2 and 10 months postpartum were randomly assigned to IH-CBT (n = 47) plus home visiting or standard home visiting (SHV; n = 46). Mothers were identified via screening and then confirmation of major depressive disorder diagnosis. Measures of child maltreatment history, depression, social functioning, and parenting were administered at pre-treatment, post-treatment, and 3-month follow-up. Results indicated high rates of maltreatment in both conditions relative to the general population. Mixed model analyses found a number of main effects in which experiences of different types of trauma were associated with poorer functioning regardless of treatment condition. Evidence of a moderating effect of maltreatment on treatment outcomes was found for physical abuse and parenting and emotional abuse and social network size. Future research should focus on increasing the effectiveness of IH-CBT with depressed mothers who have experienced child maltreatment.
Keywords
Maternal depression is prevalent postpartum. In a meta-analysis, Bennett, Einarson, Taddio, Koren, and Einarson (2004) found that between 7.4% and 12.8% of pregnant women reported significant levels of depression across each trimester. Between 13% and 19% of new mothers develop major depressive disorder (MDD) postpartum, a rate that at least doubles among mothers at high risk due to poverty (O’Hara & McCabe, 2013). The public health implications of maternal depression are profound given its negative impact on maternal life course and child development, especially during the first years of life during which foundational biological and psychological processes occur (Goodman et al., 2011). Mayberry, Horowitz, and Declercq (2007) found that financial hardship, age, unemployment, and educational underachievement predicted elevated depressive symptoms over the first 2 years postpartum. Trauma history and violence are also strongly associated with the occurrence and persistence of depression (Ammerman et al., 2009). Child maltreatment undermines the development of emotional and behavioral regulatory systems and contributes to the emergence of MDD in young adulthood (Institute of Medicine and National Research Council, 2014).
The insidious impact of violence and maltreatment on functioning in depressed mothers has implications for treatment. Among depressed adults, there is a diminished response to antidepressants in those who have experienced trauma (Klein et al., 2009). There is also evidence that depressed adults who have experienced maltreatment in childhood do not benefit to the same extent as their counterparts when receiving cognitive behavioral therapy (CBT; Nanni, Uher, & Danese, 2012). Yet, other research has found that child maltreatment history does not moderate response to treatment (Harkness, Bagby, & Kennedy, 2012).
There are few studies of child maltreatment history and treatment in perinatally depressed women. Grote et al. (2012) reported that child maltreatment history did not moderate response to treatment in a clinical trial of interpersonal psychotherapy in perinatally depressed women. Moreover, much of the research on child maltreatment history and response to treatment in depressed women has conceptualized maltreatment as a general construct, using summative indicators rather than breaking out specific types of abuse and neglect. Here, too, findings are mixed, with some studies showing that adversity broadly contributes to poorer outcomes (L. R. Cohen, Hien, & Batchelder, 2008), and others suggesting differential outcomes based on types of maltreatment (Putnam, Harris, & Putnam, 2013).
Mothers participating in home visiting are an especially important population in which to examine depression. Home visiting is a voluntary early prevention program for mothers and children designed to optimize child outcomes and prevent child abuse and neglect. There is increasing interest in home visiting models that target demographically at risk mothers, seek to enroll mothers during pregnancy or shortly after birth, and provide frequent services over the first years of the child’s life (Adirim & Supplee, 2013). Mothers participating in home visiting have high rates of depression and trauma (Ammerman, Putnam, Bosse, Teeters, & Van Ginkel, 2010). Depression undermines home visiting outcomes. For example, Easterbrooks et al. (2013) found that depressed mothers failed to receive the benefits of lowered rates of abuse and neglect relative to their nondepressed counterparts.
Ammerman et al. (2011) adapted cognitive behavioral therapy to address depression in mothers receiving home visiting. In-Home Cognitive Behavioral Therapy (IH-CBT) is implemented concurrently with home visiting. IH-CBT combines the principles and techniques of CBT with strategies that promote engagement, make content relevant to the needs of mothers in home visiting, facilitate delivery in the home, and engender a collaborative relationship between the therapist and home visitor. Empirical support for IH-CBT was obtained in a clinical trial comparing mothers who received IH-CBT and concurrent home visiting with those who received home visiting alone (Ammerman, Putnam, Altaye, Stevens, et al., 2013; Ammerman, Putnam, Altaye, Teeters, et al., 2013). Results indicated that mothers receiving IH-CBT were less likely to meet diagnostic criteria for MDD at post-treatment, reported fewer depressive symptoms, and obtained lower scores on clinician ratings of depression severity. Additional improvements were noted in social support and overall psychological distress. While these findings demonstrate the benefits of treatment to mood and social functioning in mothers in home visiting, it is unclear whether impacts were moderated by maternal histories of child maltreatment.
The purpose of this study was to examine the moderating effects of child maltreatment history on depression, social functioning, and parenting in depressed mothers participating in home visiting and receiving IH-CBT treatment. Specifically, new mothers enrolled in a community-based home visiting program were identified using a two-step process comprising a screen and subsequent confirmation of MDD diagnosis. Mothers were 16 years of age or older and were identified at 3 months postpartum. Mothers were randomly assigned to IH-CBT + home visiting or standard home visiting (SHV). Child maltreatment history was measured using the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 2003). Measures of depression, social functioning, and parenting were administered at pre-treatment, post-treatment, and 3-month follow-up. It was hypothesized that child maltreatment history would adversely affect depression, social functioning, and parenting over time in the control condition but not in mothers receiving IH-CBT.
Method
Sample
Participants were 93 new mothers aged 16 or older who participated in a home visiting program and were diagnosed with MDD. Mothers were enrolled in Every Child Succeeds, a community-based home visiting program serving Southwestern Ohio and Northern Kentucky (USA). Two models of home visiting were used: Nurse–Family Partnership (NFP; Olds, 2010) and Healthy Families America (HFA; Holton & Harding, 2007). Eligibility for the home visiting program required at least one of the following risk characteristics: unmarried, low income, ≤18 years of age, inadequate prenatal care. Mothers were enrolled in home visiting prior to 28 weeks gestation in NFP as per model parameters and from 20 weeks gestation through the child reaching 3 months of age for HFA. In the NFP, home visits were provided by nurses, while in HFA, home visits were provided by social workers, related professionals and paraprofessionals.
Design
A randomized clinical trial design was used with assessments at pre-treatment, post-treatment, and 3-month follow-up. Participants were randomized to IH-CBT (IH-CBT + home visiting) or SHV (home visiting alone) following the pre-treatment assessment. Randomization was stratified by race and home visiting model (HFA, NFP). There were no differences in the rate and type of maltreatment between models and the model was not significant in the statistical models and as a result these are not shown.
Of 151 referred mothers, 115 subsequently received a pre-treatment assessment (more detailed information about recruitment can be found in Ammerman, Putnam, Altaye, Stevens, et al., 2013). Twenty-seven mothers were not interested in participating after referral, and 9 mothers were unreachable. There were no differences between assessed and nonassessed participants on demographics or baseline clinical features. Ninety-four of 115 participants were found to be eligible. One mother was disinterested in participating following the assessment but prior to randomization. The remaining 93 mothers were randomized to IH-CBT (n = 47) or SHV (n = 46) and comprised the intent-to-treat sample. Thirteen mothers dropped out of the study between assessment points. There were no differences in dropout rate between conditions, and dropout was unrelated to initial demographic and clinical features.
IH-CBT
Mothers in the IH-CBT condition received IH-CBT + home visiting (see SHV condition for description). IH-CBT was implemented by two licensed master’s level social workers. Treatment consisted of 15 sessions that were scheduled weekly and lasted 60 min plus a booster session 1-month post-treatment. Adaptations to CBT were made to address setting, population, and context to maximize engagement and outcomes. First, IH-CBT was delivered in the home. The second adaptation involved addressing the primary concerns of young, low income, new mothers who were socially isolated (Levy & O’Hara, 2010). The third adaptation sought to facilitate close collaboration with home visitors through written communication, telephone contact, and a joint 15th session with the mother, home visitor, and therapist.
SHV
In SHV, mothers received services from home visitors as per the HFA and NFP model directives. Both models call for regular home visits during the intervals covered during the trial, and home visitors were given discretion to increase frequency of visits if needed. Curricula for both models are distinct but emphasize child health and development, nurturing mother–child relationship, maternal health and self-sufficiency, and linkage to other community services. Consistent with standard of care, mothers in the SHV condition were permitted to receive treatment for depression in the community.
Measures
The Edinburgh Postnatal Depression Scale (EPDS; Cox, Holden, & Sagovsky, 1987) is a 10-item self-report measure of depressive symptoms. Items are endorsed on a four-point scale indicating occurrence and severity over the past week, yielding a total score. The EPDS was used to screen mothers for referral to the study using a cutoff of ≥11.
The Structured Clinical Interview for DSM-IV Axis 1 Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) Axis 1 Disorders (SCID, January 2007 Version; Spitzer et al., 1992) is a semistructured psychiatric interview that is widely used in research and clinical practice. Interviews were audio-recorded and 25% were rated by a second rater yielding a kappa coefficient of .89. The SCID was administered at pre-treatment to confirm MDD diagnosis.
The CTQ (Bernstein et al., 2003) is a 28-item version of the larger CTQ. Items describe maltreatment experiences in childhood and are endorsed on a 5-item Likert-type scale reflecting how true they are. Raw scores are derived and these were also used to categorize (none, mild, moderate, severe) severity of physical abuse, sexual abuse, emotional abuse, physical neglect, and emotional neglect for descriptive purposes. The CTQ was administered at pre-treatment.
The Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996) is one of the most widely used self-report screens of depressive symptoms, with strong reliability and validity properties. It consists of 21 items indicating presence and severity of symptoms over the past 2 weeks by endorsing one of four statements reflecting severity, yielding a total score. The BDI-II was administered at pre-treatment, post-treatment, and follow-up.
The Interpersonal Support Evaluation List (ISEL; S. Cohen & Hoberman, 1983) is a widely used self-report of social support that has been utilized with multiple clinical and nonclinical populations. This 40-item measure consists of statements regarding the availability and use of tangible and emotional support from others that are endorsed using a 4-point scale reflecting the degree to which they are true. The total score was used as the primary indicator in the current study and was administered at pre-treatment, post-treatment, and follow-up.
The Social Network Index (SNI; S. Cohen, Doyle, Skoner, Rabin, & Gwaltney, 1997) consists of 12 items that document the size of the mother’s social network and this was used as the study variable. The social network number (SNN) reflects the number of people (e.g., parents, close friends, coworkers) with whom the mother has had contact in the prior 2 weeks. The SNI was administered at pre-treatment, post-treatment, and follow-up.
The Parenting Stress Index–Short Form (PSI-SF; Abidin, 1995) is a 36-item parent report measure of child and parent functioning/coping. This widely used measure yields a standardized score for Total Stress. The PSI-SF was administered at pre-treatment, post-treatment, and follow-up.
The Home Observation for Measurement of the Environment Inventory (HOME; Caldwell & Bradley, 1984) is a standardized observational measure of features in the home consistent with a stimulating, nurturing, and safe environment. It yields a Total Score and was administered at pre-treatment, post-treatment, and follow-up.
Results
Overview of Analyses
The SPSS MIXED procedure was used to examine the moderating relationship of each of the five child maltreatment categories for IH-CBT and SHV groups across three time points. Mixed model analyses first estimated fixed and random effects to determine the best descriptive form of change over time. Analyses then estimated main effects (M) of emotional abuse, physical abuse, sexual abuse, emotional neglect and physical neglect, followed by the two-way interaction of maltreatment type by time (M × T) interaction and the three-way interaction of maltreatment type by time by condition (IH-CBT or SHV). An intent-to-treat approach was used such that all participants were included in analyses. Missing data were minimal (range: 0.39%-3.15%) and were handled with multiple imputation using all analysis variables, plus an additional 185 auxiliary correlate variables in the imputation model to produce I = 100 imputed data sets (Enders, 2010). The False Discovery Rate (FDR; Benjamini & Hochberg, 1995) was used to control for Type 1 error inflation across all analyses.
Sample Characteristics and Child Maltreatment Experiences
Table 1 shows the demographics of the two groups. No differences were found between treatment and control groups on these variables. There were no differences between groups on the risk variables used to determine eligibility for the home visiting program. In terms of home visiting model, 81 mothers were in the HFA model and 12 in the NFP model. Eighty-five mothers were primiparous and 8 had more than one child (all of these were in the HFA model). No differences were found on number of children or number of home visits received (p > .05).
Demographic Characteristics of IH-CBT (n = 47) and SHV (n = 46) Participants.
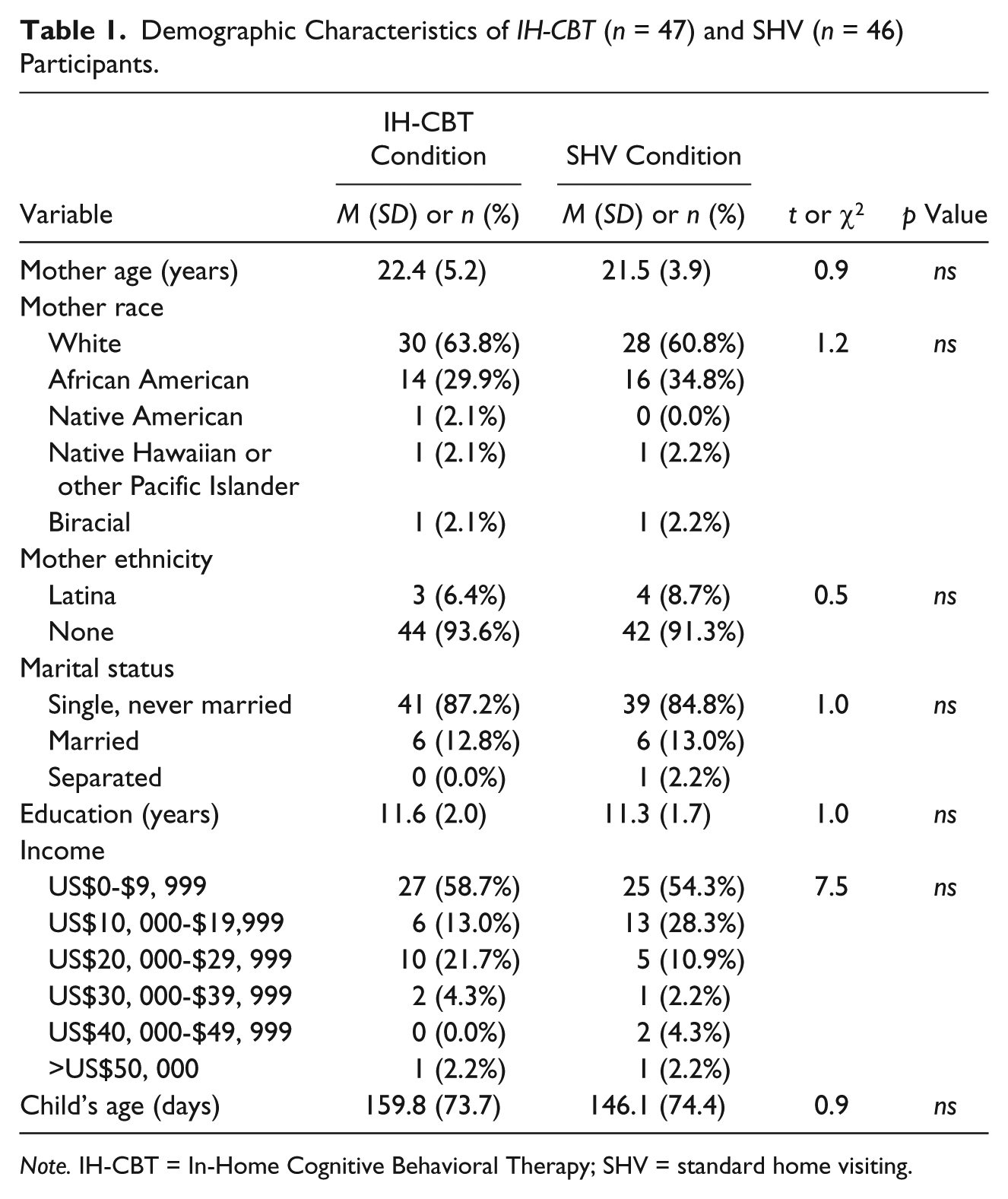
Note. IH-CBT = In-Home Cognitive Behavioral Therapy; SHV = standard home visiting.
Table 2 presents the breakout of severity of child maltreatment experience in each group for each type of maltreatment using the four categories (none, mild, moderate, severe). The CTQ was missing for one participant in the SHV condition so the table reflects n = 92. Results indicate a high proportion of child maltreatment experiences in both groups. Emotional abuse was the most commonly reported experience, endorsed as at least mild in 80.4% of the sample. Mothers reported high rates of severe levels of maltreatment in both the IH-CBT (range: 14.9%-48.9%) and SHV (range: 22.2%-44.4%) conditions.
Number and Percentage in Maltreatment History Categories From the Childhood Trauma Questionnaire in IH-CBT (n = 47) and SHV (n = 45) Participants.

Note. ps > .05. IH-CBT = In-Home Cognitive Behavioral Therapy; SHV = standard home visiting.
Mixed Model Analyses
Fixed effect analysis results (not shown) showed that linear growth best described the average form of change across participants for the HOME, PSI-SF, and SNN response variables, while quadratic change best described the average form of change across participants for the BDI-II and ISEL response variables. Furthermore, the PSI-SF, ISEL, and SNN response variables showed significant intercept (T = 1) and linear slope variation across participants, while the BDI and HOME response variables showed significant intercept variation only.
Results from adding the main effects (M) for each maltreatment type, the maltreatment by time interactions (M × T), and the maltreatment by time by group three-way interactions (M × T × G) to each longitudinal mixed model are summarized in Table 3. Statistically significant effects (p < .05 or .01) and effects that approached significance (p < .10) are shown.
Mixed Model Analyses of Types of Childhood Maltreatment From the Childhood Trauma Questionnaire on Maternal Depression, Social Functioning, and Parenting.
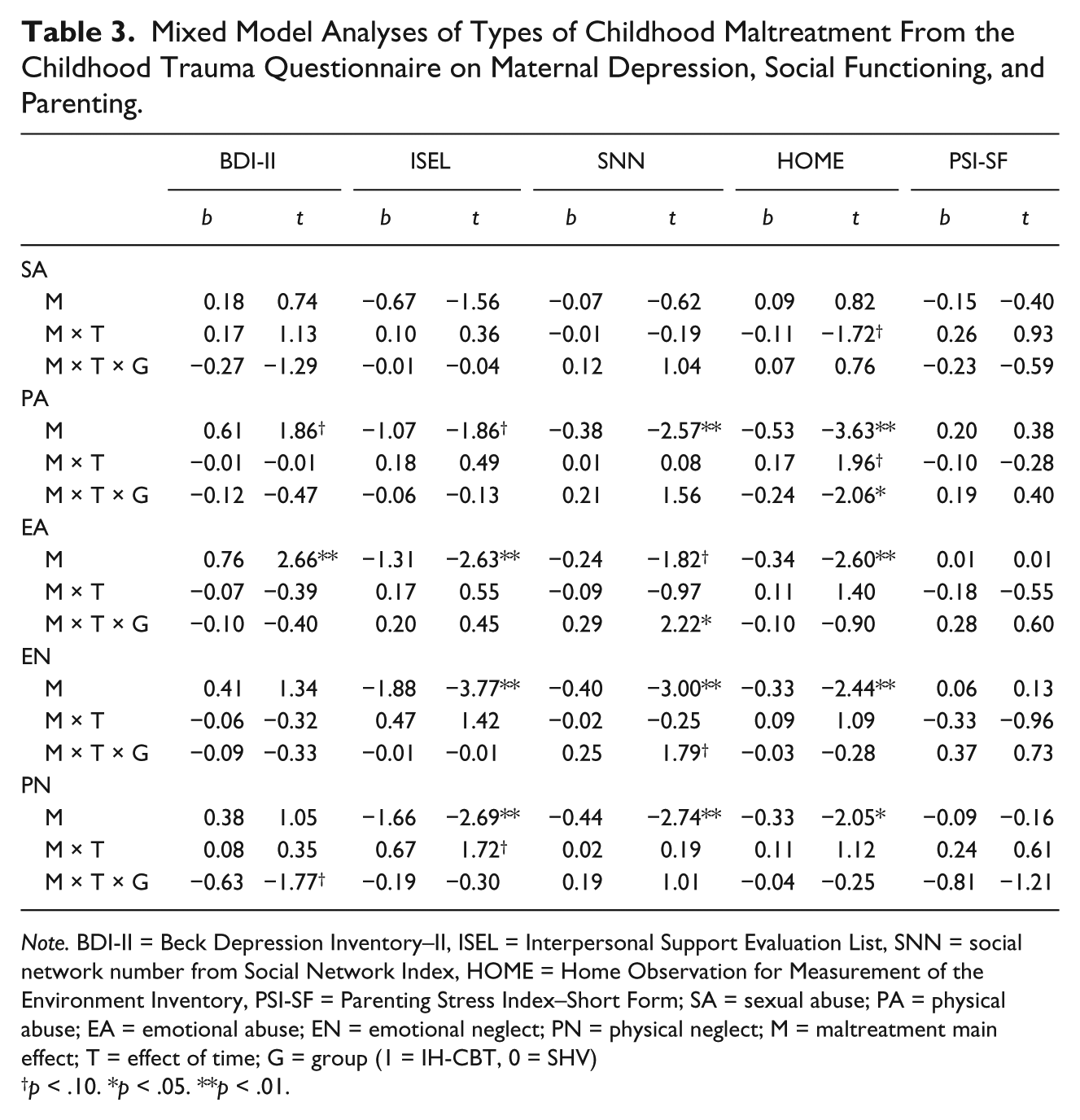
Note. BDI-II = Beck Depression Inventory–II, ISEL = Interpersonal Support Evaluation List, SNN = social network number from Social Network Index, HOME = Home Observation for Measurement of the Environment Inventory, PSI-SF = Parenting Stress Index–Short Form; SA = sexual abuse; PA = physical abuse; EA = emotional abuse; EN = emotional neglect; PN = physical neglect; M = maltreatment main effect; T = effect of time; G = group (1 = IH-CBT, 0 = SHV)
p < .10. *p < .05. **p < .01.
For sexual abuse, there were no significant main effects. There was a trend (p < .10) for a two-way interaction between time and sexual abuse for the HOME such that scores on this measure decreased over time across groups. No significant three-way interactions were found.
Main effects for physical abuse were observed with the SNN and HOME. Mothers reporting childhood physical abuse had smaller social networks and had lower scores reflecting nurturing and stimulating parenting. A trend (p < .10) was found for the main effects of physical abuse on the BDI-II and ISEL. These were in the direction of increased depressive symptoms and lower levels of social support for mothers reporting higher levels of physical abuse. A three-way interaction was observed between physical abuse, time, and group with the HOME. Mothers in the SHV group who reported higher levels of physical abuse had lower HOME scores at pre-treatment, and these increased over time to reach equivalent levels as their counterparts at follow-up.
Three main effects were found for emotional abuse: BDI-II, HOME, and ISEL. Mothers reporting histories of emotional abuse had higher levels of depression, lower HOME scores, and reported less social support that those without these experiences. A trend (p < .10) was found for the main effect of emotional abuse and the SNN, reflecting decreased network size in mothers experiencing more emotional abuse. This was further elucidated by a three-way interaction between emotional abuse, time, and group and the SNN. This finding is presented in Figure 1. Mothers in the IH-CBT group reporting emotional abuse started the trial with the smallest level of social network size, increasing over time to be equivalent to those in the treatment group with lower levels of emotional abuse.
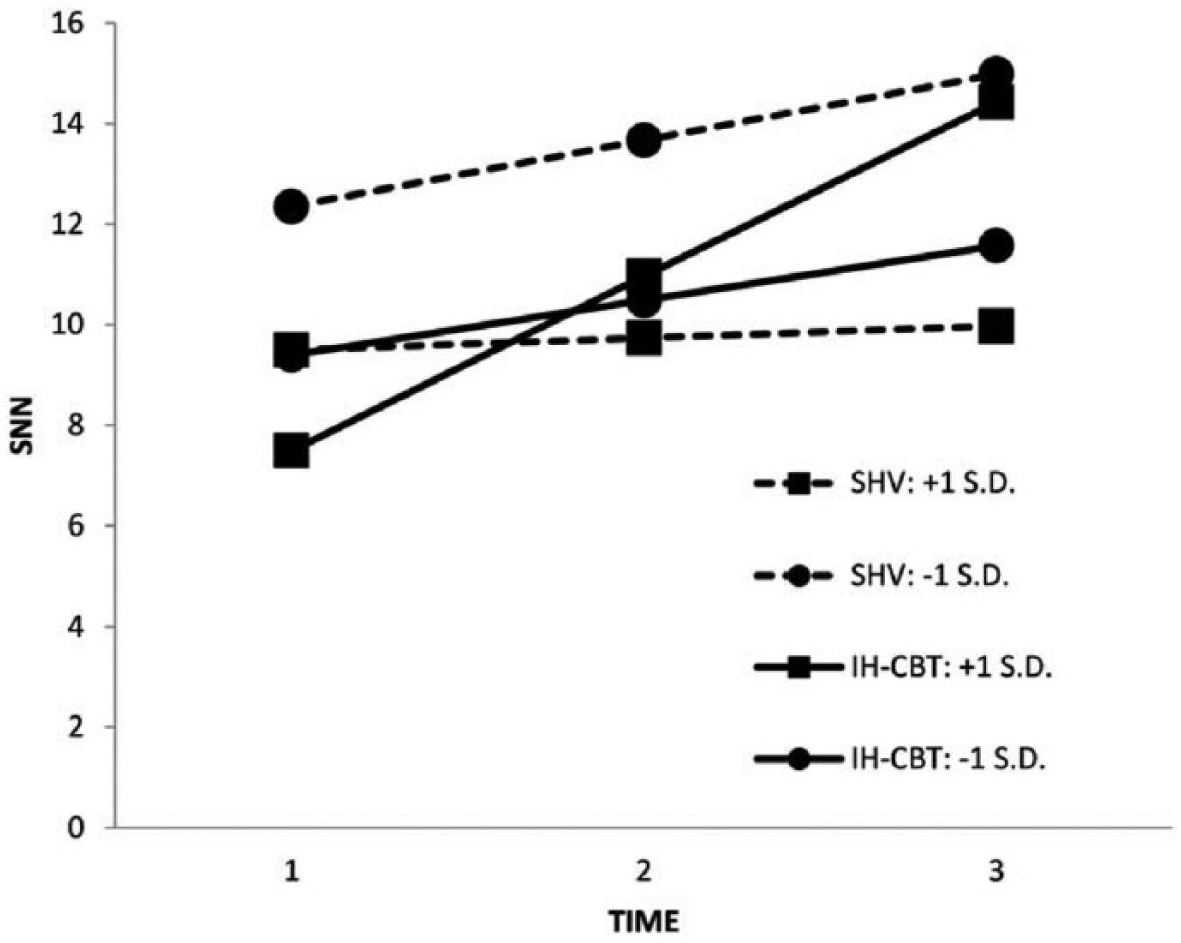
Three-way interaction between emotional abuse, time, and condition.
Significant main effects were found for emotional neglect for the ISEL, SNN, and HOME. Mothers’ report of experiencing emotional neglect was associated with lower levels of social support, smaller social networks, and less nurturing and stimulating parenting. A trend (p < .10) emerged for the three-way interaction with social network number.
For physical neglect, main effects were found for the HOME, ISEL, and SNN. Mothers reporting this type of maltreatment had lower HOME scores, less social support, and smaller social networks than their counterparts with lower levels of physical neglect. A trend (p < .10) was found for the two-way interaction between time and physical neglect on the ISEL and the three-way interaction between physical neglect, time, and group on the BDI-II.
Discussion
This study examined the moderating influence of child maltreatment history on response to an adapted CBT treatment for depressed mothers in home visiting programs. Each type of maltreatment occurred at elevated levels relative to the general population (Centers for Disease Control and Prevention, 2010), especially emotional abuse, emotional neglect, and physical abuse. For a sizable proportion of mothers reporting child maltreatment, their experiences were in the moderate and severe ranges of severity. These findings underscore the prevalence of maternal maltreatment history in home visiting populations (Ammerman et al., 2009), and the strong association between maltreatment history and depression (Blackmore et al., 2013). The prominence of maltreatment experiences in childhood in this population of mothers is relevant to the presentation and course of depression and associated clinical features.
Maltreatment history was associated with depression and impaired social functioning and parenting regardless of time or treatment condition. These findings mirror Grote et al. (2012) who also found that maltreatment histories did not differentiate outcomes between interpersonal psychotherapy and untreated controls in mothers with perinatal depression. Grote et al. speculated that their findings might be partly attributable to the lesser severity of maltreatment in their sample. In the present study, however, severity levels were high, suggesting that this aspect of maltreatment is not driving findings. Two three-way interactions were found between maltreatment history type, time, and condition. One of these, involving emotional abuse, revealed that mothers experiencing this form of abuse in childhood had greater improvements in social network size in the IH-CBT condition relative to controls. The synergistic influences of IH-CBT treatment and concurrent home visiting may have facilitated accelerated growth of network size in these mothers. Larger social networks provide more resources for emotional and tangible support and may be an important buffer against recurrence of MDD (Balaji et al., 2007).
A number of main effects for maltreatment type were identified for social support and social network. Each measure of these constructs yielded significant coefficients for three different types of maltreatment. A fourth coefficient for each approached but did not reach statistical significance (p < .10). The negative impact of child maltreatment in adult social functioning is well documented (Institute of Medicine and National Research Council, 2014), and is evident in this sample of depressed mothers. There was only one significant main effect for depression, involving emotional abuse. In contrast, maltreatment histories were associated with parenting deficits as measured by the HOME Inventory. This measure reflects nurturing and stimulating parenting. Main effects were found for all types of maltreatment except sexual abuse indicating that physical abuse and neglect were associated with overall parenting deficits. No significant findings emerged for parenting stress. It should be noted that all of the outcome variables have been found to be related to maltreatment, and that the analytic strategy in this study sought to characterize the influence of maltreatment on mothers already presenting with depression. Time was not statistically significant (except in the three-way interactions), suggesting that maltreatment history was unrelated to course of functioning during treatment.
In terms of maltreatment type, emotional abuse, emotional neglect, and physical abuse were most associated with impairment. The pattern of findings supports the interrelatedness of maltreatment (Dong et al., 2004). Yet, the lack of significant associations with sexual abuse and differential patterns of results for other types of maltreatment support the value of separating types of maltreatment. As noted by the Institute of Medicine and National Research Council (2014), findings are mixed regarding the utility of defining maltreatment as a global construct versus breaking out specific types of abuse and neglect. Until this becomes more definitive, it is suggested that specific types of maltreatment be considered separately.
IH-CBT is a promising treatment approach with a strong evidence-base (Ammerman, Putnam, Teeters, & Van Ginkel, 2014) that joins other successful efforts to treat low income, perinatally depressed women using cognitive behavioral therapy (O’Mahen, Himle, Fedock, Henshaw, & Flynn, 2013). However, maltreatment history in this population is associated with increased impairments in affective, social, and parental functioning relative to those who have not experienced such childhood adversity. It is possible that depressed mothers with significant trauma histories need more sessions, more booster sessions, or specific treatment approaches that target trauma-related clinical features to obtain the full benefits of treatment. Cuijpers, Huibers, Ebert, Koole, and Andersson (2013) found that, in a meta-analysis, more frequent sessions each week was associated with improved depression outcomes in adults. Such an approach may also be beneficial to perinatally depressed mothers in home visiting who have experienced maltreatment in childhood.
The study had a number of strengths. First, the design provided a rigorous framework within which to examine IH-CBT and the moderating impacts of child maltreatment history. Second, depressed mothers were identified using a standardized diagnostic interview in contrast to reliance on self-report measures that characterize much of the research on maternal depression generally and home visiting in particular. Third, an intent-to-treat strategy was used and retention of the sample was good. Fourth, both maternal functioning and parenting were considered. Fifth, two widely disseminated models of home visiting were represented in the sample. Findings are generalizable to low income, socially isolated mothers, who in turn reflect the largest population enrolled in home visiting programs.
The study also has several limitations that warrant caution in interpreting findings. First, the sample size was relatively small, limiting power. Second, there was no long-term follow-up. Third, child maltreatment histories were determined using retrospective recall. This is subject to bias, although recent research supports the validity of such reports (Fergusson, Horwood, & Boden, 2011). Fourth, although child maltreatment history was documented, more recent experiences of violence were not measured. Fifth, findings may not be generalizable to mothers with higher levels of social resources.
Conclusion
Research has documented high rates of depression in mothers participating in home visiting, although until recently few treatment options were available. Given the sizable public investment in home visiting, and evidence that depression undermines important outcomes sought in these programs, identifying effective treatments is imperative. IH-CBT is an adapted version of cognitive behavioral therapy that is specifically designed for depressed mothers in home visiting. Although IH-CBT is effective in ameliorating depression and associated clinical features, this study revealed that depressed mothers who have experienced child maltreatment display greater impairment in social functioning and parenting over the course of treatment when compared with those without such experiences. Emotional abuse, emotional neglect, and physical abuse were most related to impairments in functioning. Future research should focus on enhancing IH-CBT to more systematically address trauma experiences to optimize outcomes for these mothers.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant R34MH073867 from the National Institute of Mental Health.