
Abstract
Mobbing is a type of violence which occurs in workplaces and is classified under the community violence subgroup of interpersonal violence. The aim of this study is to examine health care workers who work in primary health care in the city of Mugla and to determine whether there is a relationship between sociodemographic characteristics, work conditions, and their level of mobbing. A cross-sectional analysis has been conducted in which 130 primary health care workers were selected. Of the 130, 119 health workers participated, yielding a response rate of 91.5%; 83.2% of health workers are female, 42.9% are midwives, 27.7% are nurses, and 14.3% are doctors. In all, 31.1% of health workers have faced with “mobbing” in the last 1 year, and the frequency of experiencing “mobbing” of those 48.6% of them is 1 to 3 times per year. A total of 70.3% of those who apply “mobbing” are senior health workers, and 91.9% are female. The frequency of encountering with “mobbing” was found significantly in married health workers, in those 16 years and above according to examined total working time, in those who have psychosocial reactions, and in those who have counterproductive behaviors. It has been discovered that primary health care workers have high prevalence of “mobbing” exposure. To avoid “mobbing” at workplace, authorities and responsibilities of all employees have to be clearly determined.
Introduction
Violence has been defined by the World Health Organization (WHO) as the intentional use of physical force or power, threatened or actual, against oneself, another person or against a group or community that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment, or deprivation (Krug, Dahlberg, Mercy, Zwi, & Lozano, 2002). Mobbing is a type of violence which occurs in workplaces and is classified under the community violence subgroup of interpersonal violence (Krug et al., 2002). The concept of workplace mobbing was defined for the first time in the 1980s by Leymann (Leymann, 1990). Leymann defined mobbing as “a type of psychological terror of antagonistic behaviors with unethical communication directed systematically at one individual by one or more other individuals (Leyman, 1996)”. Leymann (1996) established two criteria for considering these actions as mobbing: (a) They must occur on a very frequent basis, at least once a week; and (b) over a long period of time, with at least a 6-month duration. Mobbing affects the individual mental health and sense of well-being, and it has a negative impact on the organization where it takes place (Figueiredo-Ferraz, Gil-Monte1, & Olivares-Faúndez, 2015). According to the European Agency for Safety and Health at Work (2007), mobbing has been identified as one of the emerging risks for occupational health. Mobbing has been defined as interpersonal workplace aggression and efforts by individuals to harm others with whom they work (Neuman & Baron, 2005). In addition, this form of aggression is not necessarily related to discriminatory behaviors based on gender, race, or social group. In the case of aggression, some authors, such as Einarsen, Hoel, Zapf, and Cooper (2003), have emphasized the question of whether or not there is an intention to do harm. The mobbing process begins by attacking the honor, honesty, reliability, and professional ability of an employee. Mobbing victims are then exposed to attitudes and behaviors that can be the cause of psychological violence such as frightening, excluding, being excluded from some organization resources, isolating, injustice in the use of organizational resources, or delaying or interfering with benefiting from rights (Cowie, Naylor, Rivers, Smith, & Pereira, 2002; Einarsen, 2000; Leymann, 1990). These behaviors can be directed toward an individual by facility managers, supervisors, coworkers in the same position, or subordinates (Einarsen, 2000; Fox & Stallworth, 2003; Leymann, 1996). The person or people in the institution who use psychological violence over a long period of time also affect others, organize systematic and frequent bullying behavior, and develop a front against the victim. Others in the institution act as if they do not see these behaviors, close their eyes to them, or even provoke them; the victim feels helpless facing so many powerful people (Cowie et al., 2002; Einarsen, 2000; Leymann, 1990).
During mobbing, the victim is most affected by its frequency, repetitiveness, and length. As psychological violence and its duration increase, its effect also increases (Einarsen, 2000; Salin, 2003a, 2003b). Everyone has a different limit of endurance for psychological violence. A situation that one person could tolerate may seriously damage another person, who may be psychologically injured. Psychological violence that continues for a long period of time has negative psychological, physiological, and social effects on the victim (Björkqvist, 2001; Einarsen, 2000; Salin, 2003a). It has been reported in the literature that individuals who are exposed to long-term and continuous mobbing in the workplace have decreased self-respect (Leymann, 1996) and experience anxiety, depression, and aggression (Bilgel, Aytac, & Bayram, 2006; Quine, 1999). Some mobbing victims show symptoms of posttraumatic stress disorder (Bilgel et al., 2006; Fox & Stallworth, 2003; Leymann, 1996) and some even attempt to commit suicide (Leymann, 1990, 1996). To balance and decrease the pressure exerted on individuals exposed to mobbing, they begin to call in sick to work, resign either by their own choice or by force, are fired, or are forced into early retirement (Davenport, Schwartz, & Elliott, 1999; Jackson, Clare, & Mannix, 2002; Tinaz, 2006). Experts have stated that the result of terrorizing causes the loss of more than a year’s wages to society from individuals who become ill (Chappell & Di Martino, 2000). In addition, there are many people who face terrorizing activities and are treated for illnesses from the stress that they experience (Fox & Stallworth, 2003).
The number of research studies conducted on the issue of mobbing and the damage caused to individuals in every area of work and social life are increasing (Bilgel et al., 2006; Björkqvist, 2001; Ferrinho et al., 2003; Fox & Stallworth, 2003; Hoel & Cooper, 2000), and the importance of this issue in health care facilities has begun to be recognized. Surveys have shown that the current figures represent only the tip of the iceberg (Di Martino, 2002; El-Gilany, El-Wehady, & Amr, 2010; Schat, Frone, & Kelloway, 2006). In country case studies, Di Martino reported high rates of psychological assaults ranging from 32.2% in Bulgaria to 67.0% in Australia, and the rate of physical violence ranged from 3% in Lebanon to 17% in South Africa (Di Martino, 2002). A study conducted in the health care sector in Portugal determined that 60% of health care professionals were exposed to workplace mobbing during 2003 (Ferrinho et al., 2003). A study in Saudi Arabia showed that about 89.3% of primary health care workers had been exposed to psychological violence event at their workplace (El-Gilany et al., 2010). In a study conducted in the health sector in Iran 29% of health workers were exposed to mobbing (Teymourzadeh, Rashidian, Arab, Akbari-Sari, & Hakimzadeh, 2014). Studies carried out in the United States, Canada, Australia, and New Zealand revealed the importance of this problem and the need for immediate action (Di Martino, 2002; Gascón et al., 2009; Schat et al., 2006). The developed world is aware of the problem and tries to solve it by taking the necessary preventive measures or interventions that are based on scientific studies. However, in the developing world, workplace violence is a neglected phenomenon, and studies investigating this subject are limited.
In Turkey, workplace violence has become an important issue in recent years, and some descriptive studies have been done. There are a limited number of researches on the subject of mobbing in Turkey. Most studies dealt with workplace mobbing in the secondary health care, and the morbidity was found to be high. Studies among workers in hospital emergency services showed that 69.5% of the workers had been exposed to psychological violence (Ayranci, 2005). Another study performed in secondary health care settings in Turkey found that 55% of the health care workers had experienced psychological violence (Krug et al., 2002). A study in Turkey showed that about 30.3% of secondary health care workers had been exposed to psychological violence at workplace (Aytac, Bozkur, Bayram, Yildiz, & Aytac, 2011). All these studies in health care settings revealed that the morbidity of the workplace violence in that sector is high. Despite the recent studies in the secondary health care, the level and type of workplace mobbing in primary health care in Turkey remain unclear. It is necessary to state that there are not enough measurement instruments specific to mobbing in Turkey. To the best knowledge of authors, there is no published research on the problem of workplace mobbing in primary health care in Turkey. Furthermore, there is neither statistics on workplace mobbing in its different forms nor even a formal acknowledgment of its existence. More studies should be done to reflect the cultural difference of Turkey in identification of mobbing behaviors. The aim of this study is to examine health care workers who work in primary health care in the city of Mugla and to determine whether there is a relationship between sociodemographic characteristics, work conditions, and their level of mobbing.
Method
Study Population
This study was conducted in Mugla, a city of 838,324 residents, located in southwestern Turkey. The city is a center for energy production and tourism (Turkey Statistical Information Services, 2014). One hundred thirty primary health care workers were practicing in the Mugla city center at the time of this study and were the study’s population (Public Health Directorate, 2014).
A cross-sectional analysis has been conducted in which 130 primary health care workers were selected. No sampling was carried out; this study aimed to reach all of the primary health care centers and health care workers in the city center. Of the 130, 119 health workers participated, yielding a response rate of 91.5%. In this study, a questionnaire which contains the variables of the characteristics of sociodemographic, work conditions, the selected behaviors from mobbing, reaction to mobbing incidents, and action taken to mobbing behaviors has been used. Four health workers did not want to attend the study due to work intensity. The remaining 7 health workers who were not contacted were either taking their yearly leave or permitted to take a leave. A questionnaire form was used during office visits to health care workers. The research found that the healthcare workers face-to-face interviewed. Data were collected between January 9, 2010, and February 26, 2010, during face-to-face 15- to 20-min interviews.
The Questionnaire
A four-section questionnaire prepared after a literature review was used for data collection. In the first section, the participants’ sociodemographic variables were requested. Sociodemographic variables were gender, age, educational level, and marital status. In the second section, the participants’ working conditions were requested. Working condition variables were the presence of income other than salary, occupational status, total working time (year), and daily working time (hours). In the third section, questions were asked about mobbing behaviors; the third concerned emotional, physiological, and organizational behaviors experienced in reaction to mobbing. Preparation of mobbing behaviors; 28 types of mobbing behavior were culled from the literature. The first researcher was Leymann (1996) who identified indicators or the behaviors of mobbing, but these behaviors and activities can be gathered into five categories according to type of behavior and their effects on victim (Davenport, Schwartz, & Elliott, 2003). The exposure to mobbing is assessed subjectively based on participants’ views and perceptions, but because the instrument had been used in several previous studies, and its validity and reliability had been assessed (Davenport et al., 1999; Fox & Stallworth, 2003; Leon-Perez et al., 2014; Leymann, 1990; Niedl, 1996; Tinaz, 2006; Zapf, Knorz, & Kulla, 1996), it was deemed suitable for the purposes of this study. In this study, Leymann’s definition of mobbing was taken as a reference, and this study focused on the experiences of primary health care workers exposed to mobbing in public sectors in Turkey, and how they perceive, experience, and are affected by mobbing behaviors. Referencing Leymann’s definition can be explained by several justifications. First, Leymann is the first scholar to introduce this phenomenon, providing essentials of mobbing which are duration and frequency. Second, Leymann identified mobbing behaviors, which are more than other identifications. Finally, most of the studies depend on Leymann’s work, and there has not been another definition of mobbing that goes beyond Leymann’s definition. The reliability and validity of the instrument have been assessed for the Turkish version. The findings showed that the instrument is valid and reliable within the acceptable limits (Yildirim, Yildirim, & Timucin, 2007). The categories were isolation (8 items), attack on personality (6 items), attack on professional status (10 items), and direct negative behaviors (4 items). Staff were asked to indicate whether they had been persistently subjected to any of these behaviors in the workplace in the last 12 months. Because the commissioning trust was concerned to establish the prevalence of each type of mobbing behavior since trust status had been granted, we used a time period of 12 months and a simple yes/no response so that we could report the results as percentages. The fourth section asked about what the participants did to escape from mobbing.
Dependent variable
The dependent variable is encounter with mobbing in the workplace situation. The encounter with mobbing in the workplace situation is discussed under the subheadings of; exposure to mobbing (exposed, not exposed).
Statistical Analyses
Means and percentage distributions were calculated using SPSS for Windows version 17.0. The compatibility of the mean scores from the questionnaire with a normal distribution was measured by the Kolmogorov–Smirnov test and Lilliefors test. The characteristics of the health care workers were evaluated by percent distribution. The parameters affecting the presence of mobbing were determined by chi-square test in univariable analysis. The data were examined by using Fisher’s exact test, Pearson’s chi-square test, and logistic regression, p < .05 was considered as statistically significant. Logistic regression analysis was also applied to distinguish between exposure to mobbing and baseline variables. Among the groups, variables which were found to be statistically significant and variables that are not conceptually compatible were added to the logistic regression model. Exposure to mobbing (exposed, not exposed) has been grouped and added to the logistic regression model as a dependent variable. Variables with a p value of <.10 per univariate regression analyses were included in the multiple logistic regression analysis using the conventional method of maximum likelihood and variable selection using backward elimination. A p value of <.10 was used as a criterion for retaining variables in the final model.
Ethical Considerations
The research was conducted within the framework of ethical rules. Written permission was taken before the study from the Director of Mugla City Health, Mugla Governorship, and Muğla Sıtkı Koçman University Verbal permissions were taken form health care workers before applying the survey, and the aim of the study was explained to health care workers.
Results
The mean age of health workers working in primary health care is 37.6 ± 5.6. The distribution of sociodemographic characteristics and working conditions of health workers who participated in the study are presented in Table 1.
The Distribution of Sociodemographic Characteristics and Working Conditions of Primary Health Care Workers.

In all, 83.2% of the health workers were female and 70.6% of them were 35 years old and more than 35 years old age group, 52.1% of them had graduate degree, 95.8% of them were married, and 58.8% of them did not have an presence of income other than salary. The distribution of academic titles was 42.9% midwife, 27.7% nurse, 14.9% doctors, 5.9% civil servant, 5.0% health officer, 3.4% laboratory officer, and 0.8% dentist. In total, 50.5% of the health workers have 11- to 20-year term of work experience, all of them (100.0%) work 9 hr a day (Table 1).
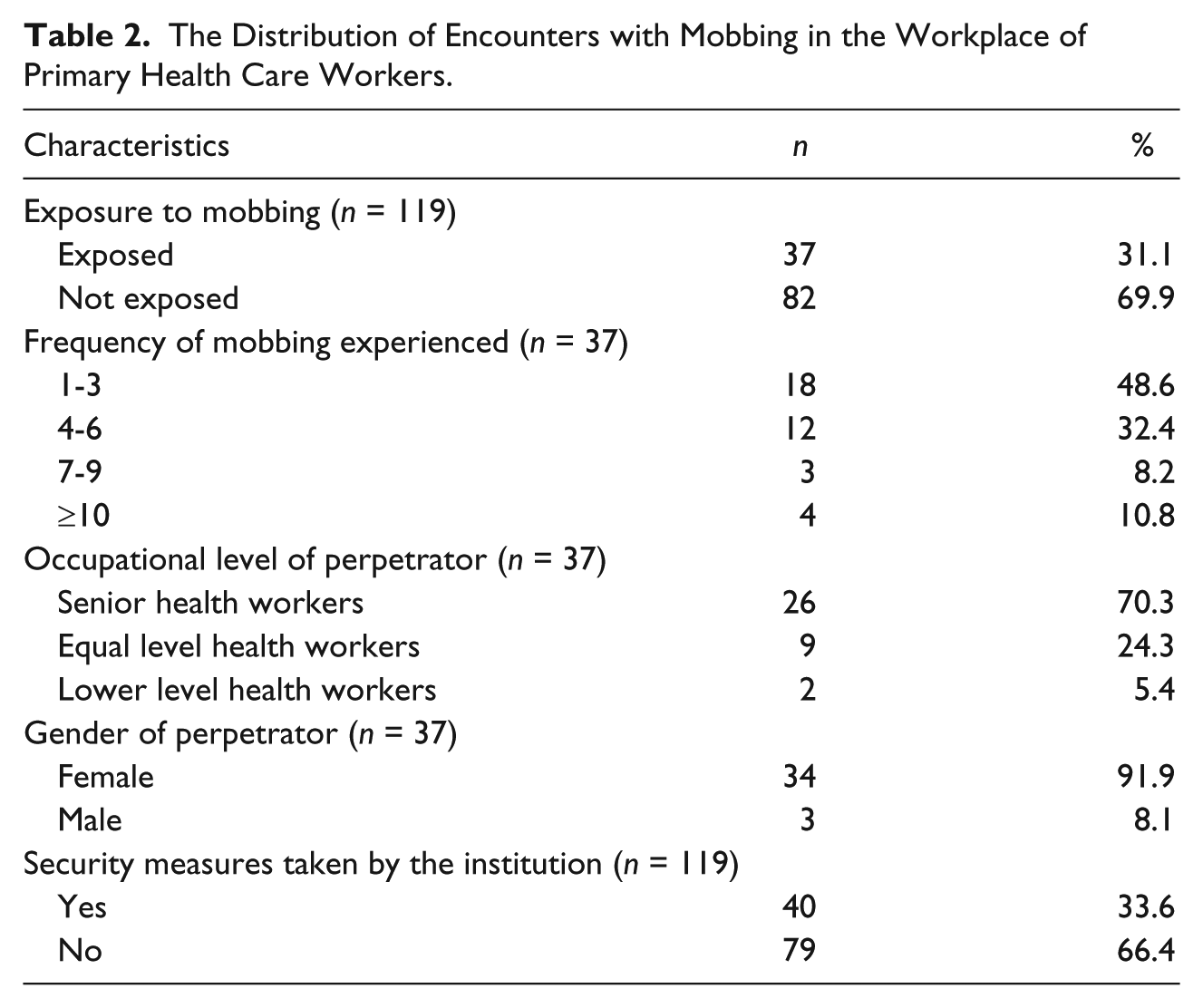
A total of 31.1% of the health workers encountered with “mobbing” in the last 1 year, and the frequency of experiencing “mobbing” of those 48.6% of them is 1 to 3 times per year. A total of 70.3% of those who apply “mobbing” are senior health workers, and 91.9% are female. In all, 66.4% of the health workers who were exposed to violence expressed that no prevention has been placed by the institution (Table 2).
The Distribution of Encounters with Mobbing in the Workplace of Primary Health Care Workers.
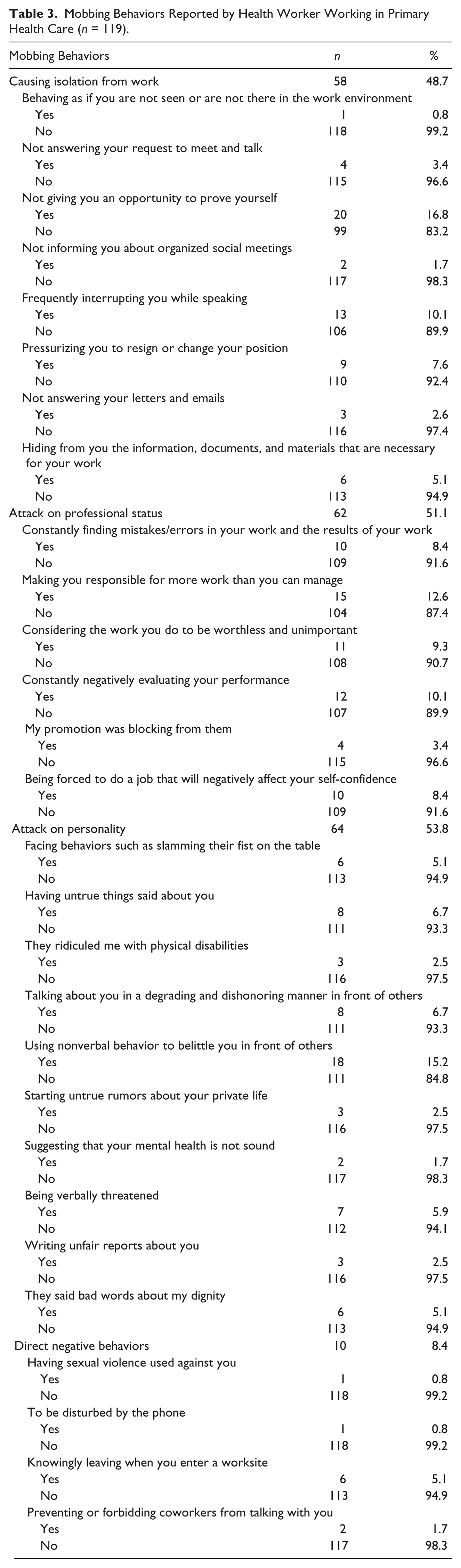
The health workers’ experiences with “mobbing behaviors” are shown in Table 3. These findings are regarding the categories of behavior: The most common behaviors included attacks on personality (53.8%) and professional status (52.1%); the most frequently encountered behavior (16.8%) was “not giving you an opportunity to prove yourself.” The second most common mobbing behavior experienced by the employees (15.2%) was “using nonverbal behavior to belittle you in front of others.” The third most common mobbing behavior experienced by the participants (12.6%) was “making you responsible for more work than you can manage.” Other mobbing behaviors that were experienced by the majority of health workers included the following: frequently interrupting you while speaking, constantly negatively evaluating your performance, and considering the work you do to be worthless and unimportant, and constantly finding mistakes/errors in your work and the results of your work.
Mobbing Behaviors Reported by Health Worker Working in Primary Health Care (n = 119).
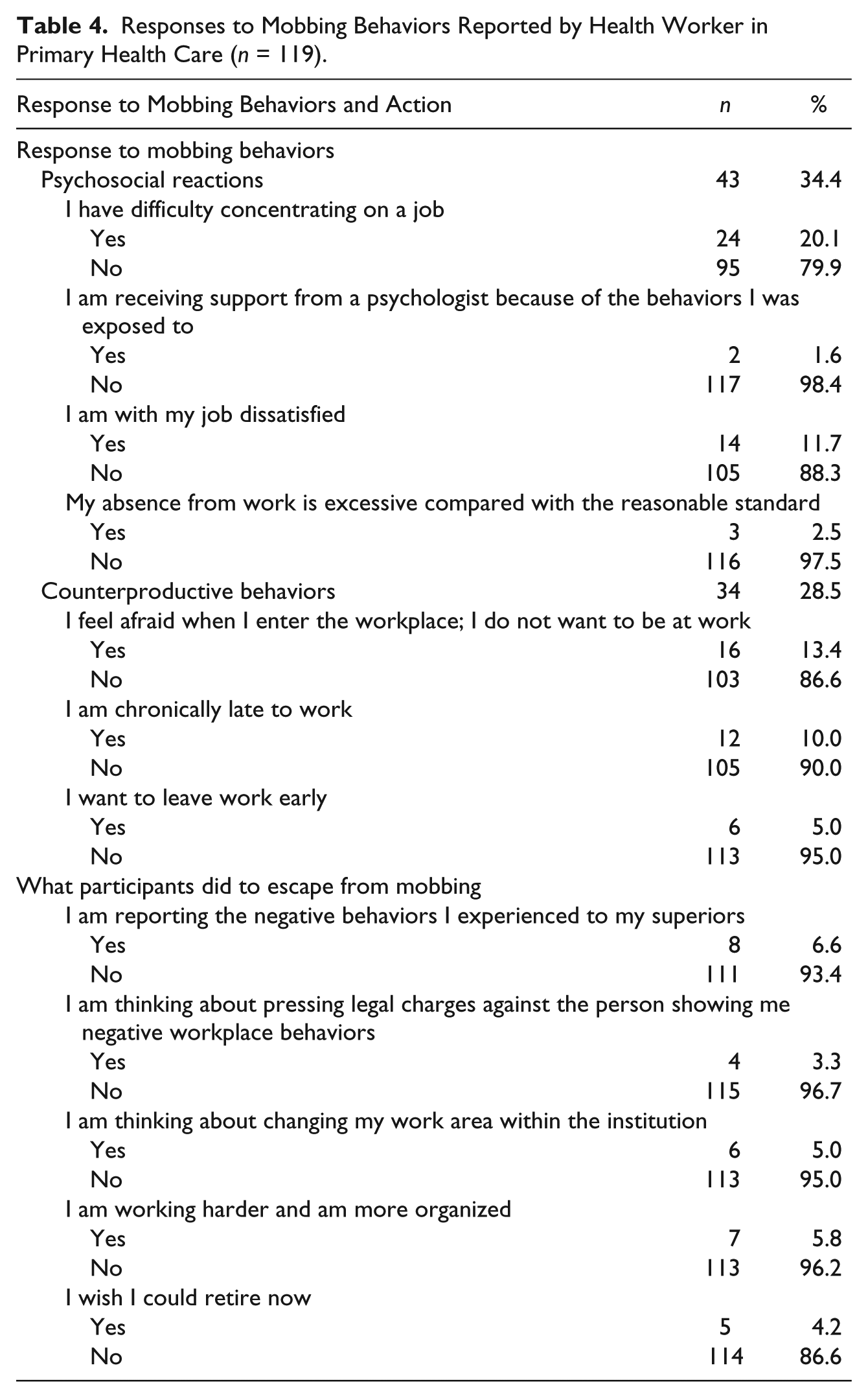
The frequencies of psychosocial and counterproductive work behaviors and action-based responses given by the employees to mobbing behaviors are shown in Table 4. The responses given concerning mobbing behaviors were intense in every respect. The most common responses were that they had difficulty concentrating on a job (20.1%), frightened when they came to work and did not want to be at work (13.4%), and had job dissatisfaction (11.7%). The most frequent behaviors used by these health workers to escape from mobbing behaviors were “I am reporting the negative behaviors I experienced to my superiors” (6.6%), “I am working harder and am more organized” (5.8%), and “I am thinking about changing my work area within the institution” (5.0%).
Responses to Mobbing Behaviors Reported by Health Worker in Primary Health Care (n = 119).
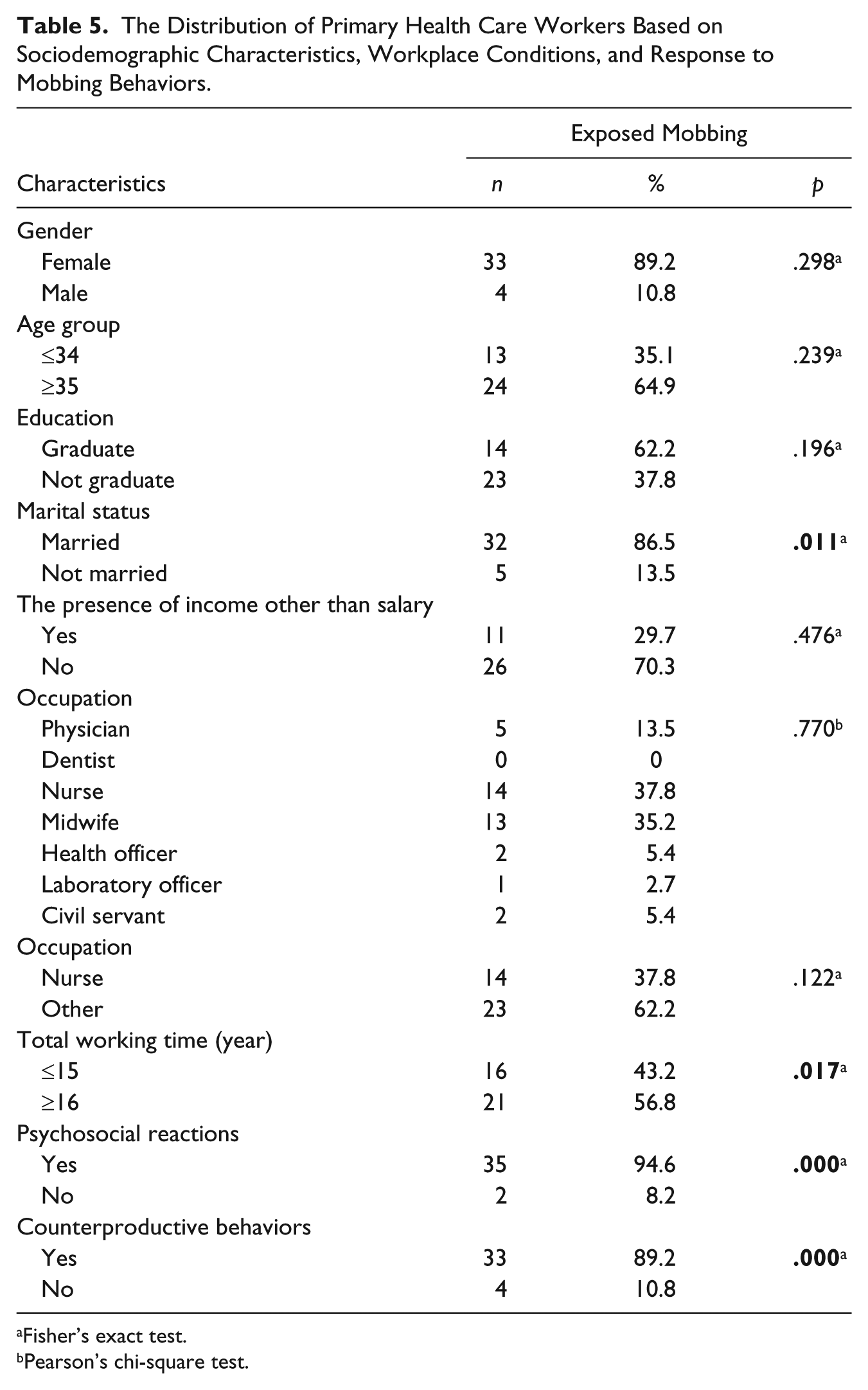
There has not been a significant difference among those with a different gender, age group, educational level, and the presence of income other than salary and occupation, when the encountered with “mobbing” in the workplace was evaluated (Table 5).
The Distribution of Primary Health Care Workers Based on Sociodemographic Characteristics, Workplace Conditions, and Response to Mobbing Behaviors.
Fisher’s exact test.
Pearson’s chi-square test.
The frequency of encountering with “mobbing” was found significantly meaningful in married health workers (p = .011), in those with 16 years and above according to examined total working time (p = .017), in those who have psychosocial reactions (p = .000), and in those who have counterproductive behaviors (p = .000; Table 5).
In univariate analysis results, the multivariate analysis results that include effecting varieties of encountering with “mobbing” are presented in Table 6.
According to Logistic Regression Results, the Features That Affect Frequency of Encounter With Mobbing of Primary Health Care Workers.
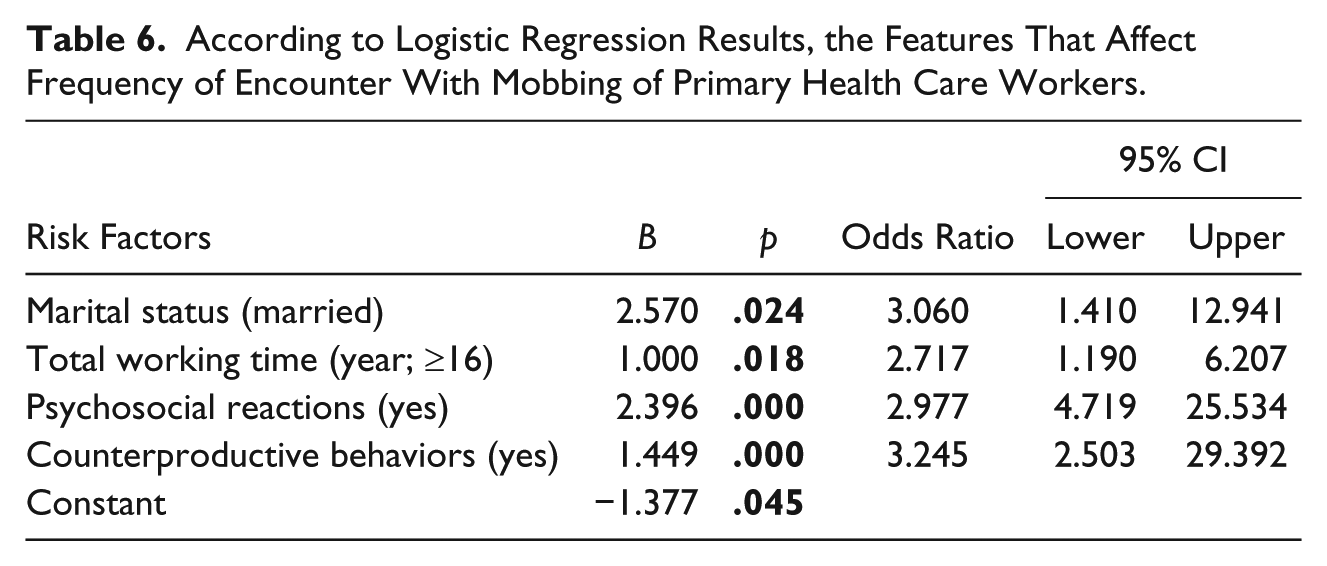
According to logistic regression analysis, 16 years and above according to examined married, total working time, psychosocial reactions, and counterproductive behaviors significantly increase the frequency of encountering with “mobbing” of health workers (odds ratios [ORs] = 3.0, 2.7, 2.9, and 3.2, respectively; Table 6).
Discussion
A significant percentage of the health workers who work in primary health care and took part in this study had encountered mobbing behaviors one or more times in the previous 12 months; 31.1% had been directly exposed to mobbing, the majority of which came from their own supervisors.
These percentages revealed that mobbing is common among health workers. In Europe (Krug et al., 2002) in 20 (5%) workers reported having been subjected to bullying and harassment in the workplace in 2005 (Parent-Thirion, Macias, Hurley, & Vermeylen, 2007). However, this low average figure conceals wide variations between countries, ranging from 17% in Finland and 12% in the Netherlands to 2% in Italy and Bulgaria, and such differences may reflect different levels of cultural awareness of and sensitivity to the issue as much as differences in actual incidence (Parent-Thirion et al., 2007). Many studies performed in both developed and developing countries showed that workers in the health care sector are at a high risk of being exposed to workplace violence (Ayranci, 2005; Ayranci, Yenilmez, Balci, & Kaptanoglu, 2006; Boyle, Koritsas, Coles, & Stanley, 2007; Canbaz et al., 2008; Di Martino, 2002; El-Gilany et al., 2010; Gascón et al., 2009; Hesketh, Duncan, & Estrabrooks, 2003; Kisa, 2008; Krug et al., 2002; Ng, Yeung, Cheung, Chung, & White, 2009; Parent-Thirion et al., 2007; Picakciefe et al., 2012; Schat et al., 2006; Senuzun-Ergun & Karadakovan, 2005; Yildirim & Yildirim, 2010). A study found that health care workers faced 16 times the risk of violence that other workers faced (Einarsen, 2000). Most violent acts occurred in hospitals, nursing and personal care facilities, and residential care services with most incidents in the form of verbal abuse or bullying/mobbing (Ayranci, 2005; Ayranci et al., 2006; Boyle et al., 2007; Canbaz et al., 2008; Di Martino, 2002; El-Gilany et al., 2010; Elliott, 1997; Gascón et al., 2009; Hesketh et al., 2003; Kisa, 2008; Ng et al., 2009; Picakciefe et al., 2012; Schat et al., 2006; Senuzun-Ergun & Karadakovan, 2005). Most previous Turkish studies on workplace violence took place in the health care sector and showed a high prevalence of psychological violence (Ayranci et al., 2006; Canbaz et al., 2008; Kisa, 2008; Picakciefe et al., 2012; Senuzun-Ergun & Karadakovan, 2005). A study in primary health care settings found that half of the primary health care workers had experienced violence at their workplaces (Ayranci et al., 2006).
WHO particularly stressed the importance of psychosocial aspects of work and work-related psychosocial factors while determining the strategies of “Working People’s Health” (World Health Organization Regional Office for Europe, 1990). Psychological violence (mobbing) is one of the psychosocial factors that employees often face. It has been found that 54% of U.K. employees, 11% of German employees, and 8% of EU employees were exposed to mobbing (Chappell & Martino, 1996). Also 8.3% of employees in Denmark and 28% of employees in Spain were exposed to mobbing (Ortega, Hogh, & Pejtersen, 2009; Pedro, Sanchez, Navarro, & Izquierdo, 2008). According to the National Institute for Occupational Safety and Health at Work in Germany, 11.3% of all employees were victims of mobbing in their working lifetime, and women are under risk 75% more than men (Pasquale, 2002). Mobbing more often is seen in Health employees than other employees. According to Synthesis Report 2002, mobbing/bullying is seen as often as 30% in Bulgaria, 22% in Lebanon, 21% in South Africa, 15% in Brazil, 11% in Thailand, and 10% in Australia in the health sector (International Labour Organization (ILO), 2005). The frequency of mobbing was 28.8% at the two public service hospitals in Kutahya, Turkey (Yener, 2008). It has been found that 55% of employees of health and education organization sectors are exposed to mobbing in Bursa, Turkey; health care workers were under the most risk (Kirel, 2007). While the annual rate of physical violence was 13.2% per 100 nurses, annual rate of mobbing was 38.8% in the United States (Nachreiner, Gerberich, Ryan, & Mcgovern, 2007). It has been found in our study that the frequency of encounter with mobbing for primary health care workers (31.1%) is higher than in other studies.
In studies about violence to which nurses have been exposed, it has been shown that they have a higher risk of workplace violence than other health care staff, and that the source of this violence is patients, patients’ relatives, physicians, and other health care personnel (Alcelik, Deniz, Yesildal, Mayda, & Serefi, 2005; Ayranci, 2005; Callaghan, Palmstierena, Hijman, & Oud, 2007; Jackson et al., 2002; Rowe & Sherlock, 2005; Yesildal, 2005). Although there are a few international studies about violence inflicted by nurses against other nurses, there is only one in Turkish national literature. In Bilgel et al.’s (2006) study, 75% of the participating health care personnel had been exposed to bullying one or more times in the previous year. Cox (1998) studied a group of 1,100 nurses in 1987 and found that 97% of those who were surveyed had faced verbal violence. In a study conducted in Norway, 20% of the nurses had been exposed to workplace bullying behaviors, the sources of which were frequently other nurses, assistant nurses, and head nurses in their own departments (Einarsen, Matthiesen, & Skogstad, 1998). Niedl (1996) reported that 26.6% of nurses face hostile actions in the workplace one or more times a week. In a study by Quine (Salin, 2003b), 38% of health care personnel had faced bullying one or more times in the last year, and the source of these behaviors, similar to our study, was frequently their own supervisors. In a Portuguese study, 60% of health care professionals had been exposed to bullying behaviors in the previous year (Ferrinho et al., 2003). It is quite possible that, similar to our study (70.3%), these behaviors were frequently displayed by managers.
Violence against women in the workplace is increasing each passing day. It has been reported that especially female workers who work in household professions and in the entertainment business encounter with workplace violence in the Philippines, and an average of 20 workers were killed and 18,000 were attacked in a week in the United States (Chappell & Di Martino, 1999. According to Salin (2003a) and Björkqvist, Österman, and Hjelt-Back (1994), women encounter more mobbing in the workplace than men. Ferrinho et al. (2003) determined that women experience more of every kind of violent behavior in health care facilities than men. In a study conducted with 7,986 Norwegian workers in 13 different organizations, no difference was found between men and women for exposure to bullying; however, 49% of the individuals displaying these types of behaviors were men and 30% were women (Einarsen & Skogstad, 1996). In addition, while men are frequently harassed by men, women are harassed by both men and women (Bilgel et al., 2006; Di Martino, 2002; Einarsen & Skogstad, 1996). Björkqvist (2001) reported that women frequently face mobbing from women and that women try to hurt their enemies psychologically, rather than physically, and prefer to display passive/aggressive behaviors. Similarly, when opportunity arises for bad behaviors to be covered up, pleasant and thoughtful behaviors are displayed, which is a characteristic of passive/aggressive personality (Buzlu, 1999). It is very frightening that, in the midst of all the work being done today to stop violence against women in all societies, there is the presence of this kind of violence between women. It has been found in our study that the frequency of encounter with mobbing for nurses (37.8%) is higher than other health care staff workers. The majority of the health workers (89.2%) were women, and all of the nurses were women in our study; this situation may have increased the ratio of mobbing in our study. In our country, because of legal regulations, only women can work in the nursing profession. In addition, generally the causes of higher frequency of encounter with mobbing according to all health workers are that all staff nurses are women, being in close relationship with patients and their relatives and more time allocation to patients.
In this study, the participants frequently encountered behaviors directed against their personality and professional status and which isolated them. In the study by Bilgel et al. (2006), the participants were frequently exposed to overwork, destabilization, and professional and personal threatening behaviors. Einarsen, Raknes, and Matthiesen (1994) reported results similar to our study. These victims of workplace mobbing most frequently experienced negative behaviors such as social isolation and exclusion, not valuing their work, talking about them in front of others in a belittling and dishonoring way, and making fun of them. Adams (1992) emphasized that the behaviors that include continuous unfair criticism and attacks on personality and on professional status were carried out in the presence of others. However, this tactic was difficult to establish precisely, and determined whether there was a relationship between this behavior and the perception of the individual exposed to it. It is this reason, more than the negative behavior the victim encounters, that renders the experience difficult for the person.
Psychological abuse has become more widespread because of legal regulations against physical violence, particularly in public facilities. Negative effects on victims of psychological violence are long lasting and systematic (Davenport et al., 1999; Einarsen, 2000; Leymann, 1996; Salin, 2003a). Leymann (1990, 1996) who is well known for conducting studies on mobbing has determined that mobbing victims’ emotional health is significantly affected and that serious psychiatric, psychosomatic, and psychosocial problems can occur. Studies on this subject show that there is a strong relationship between individuals being exposed to workplace psychological violence and victims’ complaints of both psychological and physical health problems (Adams, 1992; Björkqvist, 2001; Einarsen, 2000; Hansen et al., 2006; Leymann, 1990; Zapf, 1999). In addition to this, it has been emphasized frequently that there are differences in individuals’ perception of similar behaviors and there is variation in the effect of these behaviors from person to person (Björkqvist, 2001; Davenport et al., 1999; Hansen et al., 2006; Leymann, 1990; Zapf, 1999). The responses of individuals to mobbing behavior also guide us in determining the degree of mobbing (Einarsen, 2000). Davenport et al. (1999) reported that individuals who experience first-degree mobbing (lowest form) frequently experience difficulty with concentration. In our study, 20.1% had difficulty with concentration. Individuals who experience second-degree mobbing (medium form) in addition to the above, frequently exhibit symptoms of absenteeism from work. In our study also, 2.5% of the health care workers stated that they had symptoms of absenteeism from work. Individuals who are subjected to the highest form (third degree) of mobbing, in addition to the above behaviors, experience fear on entering the workplace and are not able to stay still at work. We found that 13.4% were frightened when they came to work and did not want to be at work. A significant percentage of the health personnel participating in our study had been exposed to workplace mobbing behaviors including those that can be considered to be second- and third-degree mobbing.
It is not just the mobbing victims’ psychology and physiology that is disturbed, but their social lives are also negatively affected. Researchers have recommended that victims of mobbing receive expert assistance as early as possible to avoid serious negative health problems (Davenport et al., 1999; Leymann, 1990). A small percentage (1.6%) of the participants in our study stated that they received support from a psychologist because they had been exposed to mobbing behaviors. This may be because the health care workers did not consider the work stress they experienced to be an illness.
On examining what the participants did to try to decrease the mobbing behaviors that they were facing or to escape from them, most tried to talk to the individual responsible for the behavior or reported the person to their supervisors. The majority (5.8%) also stated that they were more careful with their work and worked harder and in a more organized way. However, 5.8% of the participants were thinking about changing their job or working in another division to get away from their current workplace. Bilgel et al. (2006) similarly stated that the most frequently reported responses to bullying were talking to colleagues and friends, ignoring the perpetrator, and warning the perpetrator not to do this again. Jealousy, having a different point of view, and success at work were the most commonly reported reasons for being subjected to bullying.
On achieving results similar to our study, Einarsen (2000) found that mobbing victims actively use a problem-solving process, and when they cannot solve the problem they leave the institution. In addition, 3.3% thought about taking legal action. The reason why more individuals did not choose this route in our study may be because in our country, workplace psychological violence has not yet been clearly defined, and appropriate laws do not exist. However, judges have brought cases to occupational courts and have ordered financial penalties for those accused of “abuse of human rights” and “injury with emotional abuse” (Tinaz, 2006). Samanci, who investigated Turkish patients who had problems as a result of pressure they faced in the workplace, emphasized that, particularly in times of economic crisis, they experienced increased emotional abuse. However, this situation may suit employers and nobody complains, which only increases the problem. In this way, terrorizing actions are seen as a way “to be freed of the responsibility to make severance payments,” and “dismissing” an employee through self-resignation has become a primary aim of the process of terrorizing in our country (Tutar, 2004).
No statistically significant relationships were found with the health workers’ age, gender, education, and occupational status. However, in this study, being married was found to be significantly associated with becoming a victim of workplace mobbing. The results of studies in the literature are not clear, in each study were different results (Bilgel et al., 2006; Di Martino, Hoel, & Cooper, 2003; Einarsen & Skogstad, 1996; Quine, 1999, 2003; Yildirim, Yildirim, & Timucin, 2007). According to the results in the literature, we can say, regardless of age, gender, education, marital status, or occupational status, the frequency of meeting with mobbing of health workers increases. More studies are needed on this subject.
We found that job tenure was significantly associated with exposure to workplace mobbing and as the number of years of work experience increased, so did exposure to mobbing. Similar results were obtained from a study among U.S. workforce; there was a positive linear relation for job tenure (Schat et al., 2006). Although some studies in the literature revealed an opposite statement, which suggested that new and, inexperienced workers were especially vulnerable to violence (El-Gilany et al., 2010). The association between job tenure and exposure to workplace mobbing should be further studied.
Study Limitations
This study had several limitations. First, the study was carried out in a single city’s primary health care centers; hospitals and private facilities were not included. The inability to generalize may affect the findings of this study. This situation has created a problem generalizing the interpretation of the study’s results. The survey being implemented during working hours of health care workers has caused a drop in the participation rate. We can show this situation as a difficulty in our study.
In addition, it is very difficult to determine absolutely the mobbing behaviors that have become completely accepted because there is no general definition (Cowie et al., 2002; Einarsen, 2000). Because these negative behaviors can occur continuously or periodically in the workplace and are carried out by a group, it is very difficult to determine particular mobbing strategies (Cowie et al., 2002). For this reason, it is also difficult to compare the results of other studies that have been conducted on the subject of workplace mobbing.
Other limitations of our study were the use of self-report questionnaires and determining mobbing from the different perceptions of individual health workers exposed to negative behaviors. In addition, another factor is that participants had to remember how frequently they had been exposed to these behaviors in the previous 12 months. Cowie et al. (2002) stated that questionnaire formats are not sufficient for determination of the dynamics and process of mobbing situations. Finally, because this study was carried out only in Mugla, Turkey, these results cannot be generalized to all Turkish primary health workers. Future studies are needed using larger samples in several health care centers in different regions of Turkey.
Conclusion
In conclusion, primary health care workers who have undertaken an important task for public health face a high ratio of mobbing in the workplace. The health care workers’ encounters with violence should be avoided. First, health workers should take sufficient amount of and continuous in-service training prior to coping with issues. The relevant state departments should be informed about the risk factors of the working environment of health care workers. The health workers should be monitored continuously and regularly in terms of health outcomes. Follow-up structures should be developed. In the long run, training such as defense training, judicial and administrative reporting, and training related to the legal process (to obtain the rights and protection of possible legal problems) should be given to health care workers. Counseling, moral, mental aspects of protection, and treatment should be provided to health care workers. The cooperation among the institutions (municipalities, police forces, universities, hospitals, etc.) should be established, and coordinated efforts (meetings, seminars, etc.) should be performed.
Footnotes
Acknowledgements
The authors thank all retired health care workers who participated in this study. Thanks to all those who cooperated in this research, including the provincial director of Mugla City Health, Mugla Governorship, and Mugla S.K. University.
Author Contributions
Metin Picakciefe, Gulcihan Acar, Zehra Colak, and Ibrahim Kilic contributed equally to this work; Metin Picakciefe designed research; Metin Picakciefe, Gulcihan Acar, Zehra Colak, and Ibrahim Kilic performed research; Metin Picakciefe, Gulcihan Acar, Zehra Colak, and Ibrahim Kilic contributed new reagents/analytic tools; Metin Picakciefe analyzed data; and Metin Picakciefe, Gulcihan Acar, Zehra Colak, and Ibrahim Kilic wrote the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.