
Abstract
Work-related threats and violence is a major occupational hazard and the consequences for victims may be a range of physical and psychological symptoms. The purpose of this study was to examine the associations between exposure to work-related violence and threats and subsequent risk for depression and to examine whether the associations were modified by social support, organizational justice and safety perceptions. Questionnaire data was collected in 2010, 2011 and in 2015. A total of 5,342 employees from special schools, psychiatric wards, eldercare and the Prison and Probation Services (PPS) participated in the first round in 2010. The analysis was performed by multivariate logistic regression. Staff exposed for work-related threats and violence had an increased risk for depression compared to non-exposed staff. The risk was highest for staff working in PPS. Compared to low levels, there were a tendency for high levels of social support, organizational justice and safety perception to attenuate the associations between work-related threats and violence and depression. However, none of the differences were statistically significant. Many employees working in human service sectors are exposed to work-related threats and violence which increases the risk for depression. The risk for depression following work-related threats and violence may be modified by social support, organizational justice and the perception of safety workplace. It is recommended that workplaces adopt an integrated organizational approach including both prevention of work-related threats and violence and intervention to modify the health consequences of work-related threats and violence.
Introduction
The International Labour Organization (ILO, 2004) defines work-related violence as “any action, incident or behavior that departs from reasonable conduct in which a person is assaulted, threatened, harmed, injured in the course of, or as a direct result of, his or her work” (p. 4). This definition covers a broad range of actions and behaviors that can create a risk to the health and safety of employees (ILO, 2004).
Workplace violence in health care and social services occupations has been recognized globally as a major occupational hazard (Camerino, Estryn-Behar, Conway, van Der Heijden, & Hasselhorn, 2008; McPhaul & Lipscomb, 2004). A study among U.S. nurses found that 54% had verbally been abused by patients during the last year and 76% had experienced violence at work, and a Spanish study among professionals working in senior citizen residences found that 61% had been assaulted at work during the last year (Speroni, Fitch, Dawson, Dugan, & Atherton, 2014; Vidal-Martí & Pérez-Testor, 2015).
Impact on Health Outcomes
Violence and threats at work can trigger a range of physical and psychological symptoms in victims. Most victims report being affected emotionally by the experience, and the consequence can include anger, frustration, shock, annoyance, fear, stress, sleep disruption, and depression (Lanctôt & Guay, 2014). In employees working in prisons, work-related threats, and violence have been found to be related to posttraumatic stress disorders (Boudoukha, Altintas, Rusinek, Fantini-Hauwel, & Hautekeete, 2013; James & Todak, 2018) and sleep disorders (James, Todak, & Best, 2017). Among teachers, studies have that found work-related violence and threats are related to burn-out, fear and posttraumatic stress disorders (Bass et al., 2016; Wilson, Douglas, & Lyon, 2011).
Also among employees working in elder care and psychiatric wards, work-related threats and violence are associated with psychological symptoms such as fear and anxiety (Isaksson, Graneheim, Aastrom, & Karlsson, 2011), posttraumatic stress disorders (Inoue, Tsukano, Muraoka, Kaneko, & Okamura, 2006; Richter and Berger, 2006), and depression (Hanson, Perrin, Moss, Laharnar, & Glass, 2015; McCaughey, DelliFraine, McGhan, & Bruning, 2013).
According to a review, depressed mood, the experience of depressive symptoms, or a state of depression may be a frequent health outcome of work-related threats and violence irrespective of occupation (Lanctôt & Guay, 2014). Depression is a common mental disorder characterized mainly by a significant and constant feeling of being low in spirits. According to the International Classification of Diseases, 10th edition (ICD-10; World Health Organization, 1992), depressive symptoms can include diminished energy and strength, lowered interest in daily activities, feeling of sadness or low spirits, feelings of guilt, worthlessness, feeling that life is not worth living, difficulty in concentrating, trouble sleeping at night, and increased or decreased appetite.
Several studies have found that work-related violence is associated with depressive symptoms (Byun, Jung-Choi, Cho, & Paek, 2009; Choi, Jung, Kim, & Park, 2010; Lipscomb et al., 2012). A study among 6,300 nurses in the United States found that around 15% reported depressive symptoms following nonphysical violence and around 7% reported depressive symptoms following physical violence (Gerberich et al., 2004). Among 441 nurses in Turkey, a study found that found that 7.8% reported depressive symptoms following violence at work (Ünsal Atan et al., 2013), and a study among nurses in Kuwait found that 73% reported depressive symptoms following violence at work (Atawneh, Zahid, Al-Sahlawi, Shahid, & Al-Farrah, 2003). Measuring depression with the use of Beck’s Depression Inventory–Revised, a study found that nearly 10% experienced moderate to severe depression after being exposed to violence at work (Lam, 2002). Based on a larger number of hospital inpatients and outpatients, a study found that employment in occupations involving exposure to work-related threats and violence was a risk factor for the clinical psychiatric diagnosis of an affective disorder. However, in this study only a proxy measure for work-related violence and threats was used, the occupation held the year before hospital treatment being used as exposure proxy.
Thus, several studies have found associations between depressive symptoms and violence and threats at work. However, there are several methodological issues which should lead to caution in interpreting these results. Most studies are based on cross-sectional designs (Hanson et al., 2015; da Silva et al., 2015), and the measurements of depression are often nonspecific and nonvalidated (Atawneh et al., 2003; Gerberich et al., 2004). Furthermore, in some of the studies, the response rates are relatively low (Hanson et al., 2015) or sample sizes are relative small (Atawneh et al., 2003; Lam, 2002). Finally, some of the studies do not compare employees exposed to violence and nonexposed employees regarding the risk for depression following work-related threats and violence (Atawneh et al., 2003; Gerberich et al., 2004; Lam, 2002). Therefore, there is a need for larger, longitudinal studies using more precise measures of depression that examine the risk for depression after work-related threats and violence
Modifying Factors
Despite the traumatic character of work-related threats and violence, not all employees develop depressive symptoms following violence at work. Lam’s (2002) study found that 62% of employees had been exposed to aggressive patients at least once within 4 weeks prior to survey, but only 10% experienced moderate to severe depression, which may indicate the existence of protective factors. However, most studies on work-related violence have focused on the negative consequences for the employees’ health, and only a few studies have identified organizational factors that may protect employees from the adverse consequences of work-related threats and violence. Factors at work that may protect against depressive symptoms are organizational social support, organizational justice, and safety perceptions.
Organizational Social Support
Social support is a major resource for coping with work demands and may provide the practical and emotional support necessary to cope with adverse working conditions (van Emmerik, Euwema, & Bakker, 2007). Social support may most strongly affect social stressors (Cohen & Wills, 1985) such as interpersonal conflicts, threats, and violence. Therefore, social support may play an important role in preventing the development of depressive symptoms among employees who are victims of workplace violence.
Few studies have examined the association between workplace violence, social support, and health outcomes. A study among emergency department nurses found that those who had suffered from workplace violence, but without displaying or reporting depressive symptoms, received more peer support than those who developed depressive symptoms (Hsieh, Chen, Wang, Chang, & Ma, 2016). Some studies have focused specifically on the source of the social support. For instance, studies have found that social support from inside the organization had a moderating effect on stress symptoms following vicariously experienced violence, whereas social support from family and friends did not have any moderating effect (Leather, Lawrence, Beale, Cox, & Dickson, 1998). In the study by Schat and Kelloway (2003), social support was operationalized both as instrumental support provided from coworkers, supervisors, and management following the experience of aggression and violence and informational support in the form of training that could help employees deal with various aggressive and violent acts. In the study by Leather et al. (1998), social support was operationalized as the received social support from the line manager, the training department, the personnel department, and the security department in dealing with violent incidents. These studies are promising, demonstrating that organizational support may modify the relation between work-related violence and negative health consequences. However, social support specifically targeted at reducing the negative consequences of work-related violence may be more likely to modify the negative effects than social support in general because the modifying effects of social support could be contingent upon matching the source and type of perceived support to the stressor (Leather et al., 1998).
Organizational Justice
Organizational justice refers to the extent to which employees are treated with fairness in the workplace. A study in the United States found that work-related violence against teachers was associated with adverse psychological and physical symptoms, but only when teachers’ satisfaction with the management’s handling of the aftermath of the situation was low (Fox & Stallworth, 2010). A study among teachers found that unfair managerial practices increased the risk for sleep disturbance following work-related violence, whereas working in high-justice conditions seemed to protect teachers from the negative effect of work-related violence on sleep (Gluschkoff et al., 2017). Based on these findings, it appears that organizational justice may influence employees’ reactions to violent acts.
Workplace Safety Perception
Research has found that individuals who perceived their life to be in danger during a traumatic event had higher levels of adverse symptoms (Ozer, Best, Lipsey, & Weiss, 2008). However, a high perception of safety during and following a traumatic event was associated with better psychological and behavioral functioning (Grieger, Fullerton, & Ursano, 2003).
In relation to aggression at work, a review found that workplace bullying had an impact on posttraumatic stress symptoms, but promoting psychological as well as physical safety moderated the impact of bullying on posttraumatic stress symptoms (Bond, Tuckey, & Dollard, 2010). Furthermore, studies have found that fear and concern over the risk of being exposed to future work-related violence may increase employees’ risk for various stress-related disorders, and those who react beforehand with fear are more vulnerable to distress following work-related violence (Santos, Leather, Dunn, & Zarola, 2009; Wieclaw et al., 2006). In relation to the consequences following exposure to work-related violence, one study has examined the importance of employees’ workplace safety perceptions and revealed that such safety perceptions mediate the association between workplace violence and burn-out (Bass et al., 2016). Thus, we examined whether employees’ safety perceptions at work modified the association between work-related violence and threats and depressive symptoms.
The Present Study
The aim of the present study was to examine the associations between exposure to work-related violence and threats and subsequent depressive symptoms in four high-risk occupations in human service work, namely employees working in psychiatric wards, in elder care, in the prison and probation service (PPS), and at special schools, and furthermore, to examine possible modifying effects of organizational social support, organizational justice, and workplace safety perceptions.
The purposes of the article are to examine the following:
The association between frequency of exposure to work-related violence and threats and depressive symptoms in four high-risk sectors;
Whether the association between frequency of exposure to work-related violence and threats and subsequent depression is modified by organizational social support, both general social support and social support that specifically relates to workplace violence;
Whether the association between frequency of exposure to work-related violence and threats and subsequent depression is modified by organizational justice; and
Whether the association between frequency of exposure to work-related violence and threats and subsequent depression is modified by safety perceptions.
Method
Procedure and Participants
The study population consists of a cohort established in 2010 with follow-up in 2011 and 2015. The study population was employed in the following settings: different types of public psychiatric wards (open wards, acute wards, secure wards), the elder care sector, at special schools (schools for pupils with special needs and diagnoses such as attention deficit hyperactivity disorder [ADHD] and autism) and in the PPS. The sectors were chosen because previous research in Denmark has found that these sectors have high frequencies of work-related violence and threats (Borg, 2012). The participants were recruited using convenience sampling. The workplaces were all public workplaces and were contacted by way of a formal meeting with the top managerial level in the municipality (elder sector) or county (psychiatric wards). Details regarding exposure in the cohort are available elsewhere. The data collection is described in detail in a previous study (Rasmussen, Hogh, & Andersen, 2013). In 2010 and 2011, participants working in psychiatric wards, in the elder care sector, and at special schools received and filled out paper-and-pencil questionnaires during a planned meeting at the worksite. Invited participants were employees in jobs with client contact and with no more than 3 weeks of absence prior to survey. Employees who did not participate in the meeting received a questionnaire and a prepaid/stamped envelope to be returned directly to the researchers. A web-based questionnaire was used for participants in the PPS—a decision made by top management. It was stated in the cover letter of the questionnaire, that participation in the study was voluntary and that the data would be treated confidentially.
The data collection in 2015 was based on an invitation to all participants from 2010 who were still living in Denmark. Using their civil registration number, we were able to contact them at home, regardless of whether they were still employed at their original workplace.
The initial sample consisted of 5,333 persons: psychiatry (N = 909/response rate: 85%), special schools (N = 731/response rate: 91%), elder care (N = 940/response rate: 80%), and PPS (N = 2753/response rate: 60%). Eligible for follow-up in 2011 were respondents who answered the questionnaire at baseline in 2010, worked at the same workplace as in 2010, worked with the same clients as in 2010, and had no more than 3 weeks absence at the time of survey in 2011. In the time span between baseline (2010) and follow-up (2011), a few employees had got another job, had retired, were on sick leave, or maternity leave. In 2015, the panel only included employees still at work and having similar work duties as in 2010.
Altogether, 3,584 participated in the follow-up study in 2011. A total of 3,486 participated in the follow-up in 2015. We used a unique personal identification number to match every participant on the individual level.
Measurements
Exposure variables: work-related violence and threats in 2010 and 2011.
Based on the definition by Wynne, Clarkin, Cox, and Griffeths (1997), we applied a broad definition of work-related violence including threats of violence as well as physical violence. We used a checklist consisting of the 11 different types of violent incidents and seven different types of threats of violence used in previous research in Sweden (Menckel & Viitasara, 2002). Types of physically violent behaviors included being spat on, hit, hit with an object, scratched/pinched, shoved, held firmly, punched with a fist, kicked, bitten, being hit with a thrown object, and clients using a weapon or a weapon-like object. Threatening behaviors included being threatened with beatings, written threats, threatened in a scolding manner, threatened in an insulting manner, threatened over the phone, threatened involving objects, and threatened indirectly (i.e., threats to family) but with no physical contact. Respondents were asked to indicate how often during the past year they had experienced each of these different types of threats or violence at the workplace. For both work-related violence and threats, the frequency of occurrence was measured on a 5-point Likert-type-like scale ranging from never (0) to almost daily (4). We defined a joint measure of all threatening and all violent incidents measured in 2010 and 2011 for each employee.
This resulted in a score for violence with a possible range from 0 to 44 and a scale for threats with a possible range from 0 to 28. Answers regarding threats and those regarding violence were summed separately. We made dichotomized variables consisting of those exposed to work-related threats and violence regardless of frequency and those not exposed to work-related violence and threats.
Outcome: Depression
Depression was measured by the Major Depression Inventory (MDI). The MDI is a self-rated questionnaire with an algorithm that leads to ICD-10 categories of mild to severe depression. The MDI consists of 10 items, where items 8 and 10 have a sub-item; thus, there were 12 questions in total. Each item measures the presence of symptoms during the past 2 weeks. The response categories were “All the time” (5), “Most of the time” (4), “Slightly more than half the time” (3), “slightly less than half the time” (2), “Some of the time” (1), and “At no time” (0). The scale can also be used as an index in which the 10 items are summed up to give a total score for depression with the following cut-off points: 0-20 = No or doubtful depression, 21-25 = Mild depression, 26-30 = Moderate depression, 31-50 = Severe depression (Bech, Rasmussen, Olsen, Noerholm, & Abildgaard, 2001). The instrument has been previously found to have adequate internal and external validity in psychiatric patients (Bech, Timmerby, Martiny, Lunde, & Soendergaard, 2015).
In the MDI, we applied a cut-off point at 20 to distinguish between those who had symptoms of depression and those who were not depressive (Bech et al., 2001).
Modifying Factors
Organizational general social support
To measure general organizational social support from nearest supervisor and colleagues, we used two scales from the Copenhagen Psychosocial Questionnaire (COPSOQ; Pejtersen, Kristensen, Borg, & Bjorner, 2010).
Social support from the nearest supervisor scale consists of three items (e.g., “How often is your nearest superior willing to listen to your problems at work?”/“How often do you get help and support from your nearest superior?”/“How often does your nearest supervisor talk with you about how well you carry out your work?”).
Social support from the colleagues scale consists of three items (e.g., “How often do you get help and support from your colleagues?”/ “How often are your colleagues willing to listen to your problems at work?”/ “How often do your colleagues talk with you about how well you carry out your work?”).
The items were measured on a 5-point Likert-type scale ranging from “always” (5) to “never/nearly never” (1).
Cronbach’s alpha for the scales was .85 for social support from colleagues and .91 for social support from supervisors. The scales were dichotomized into two groups based on the median split.
Organizational Specific Social Support
To measure organizational social support specifically related to work-related threats and violence, we used two items to measure specific social support following work-related violence that were inspired by Vegchel, Jonge, Söderfeldt, Dormann, and Schaufeli (2004; “Your nearest supervisor provides adequate help and support after a violent or threatening situation” and “your colleagues provide adequate help and support after a violent or threatening situation”).
The items were measured on a 5-point Likert-type scale ranging from “Not at all” (1) to “To a high degree” (5). The scales were dichotomized into two groups based on the medians.
Organizational Justice
To measure organizational justice, we used three items from the second version of the COPSOQ (Pejtersen et al., 2010; “Are all suggestions from employees treated seriously by the management?”/“Is the work distributed fairly?”/ “Are conflicts resolved in a fair way?”).
The items were measured by means of a 5-point Likert-type scale ranging from “to a small extent” (1) to “to a great extent” (5). Cronbach’s alpha for the scale was .86, and the scale was dichotomized into two groups based on the median.
Safety Perception
To measure safety perception at work, we used three items from a scale developed in a Danish study (Hogh, 2001) and labeled safety perception (e.g., “Generally, the safety of my workplace is satisfactory”/“I feel safe by being on my job”/“I can quickly call for help when I need if”).
The items were measured by means of a 5-point Likert-type scale ranging from “completely true” (5) to “completely wrong” (1). Cronbach’s alpha for the scale was .77. The scale was dichotomized into two groups based on the median.
Potential Confounders
Gender and age were retrieved from the initial survey round.
Statistical Analyses
The analyses were conducted in three steps using logistic regression. The reference group was those employees not exposed to work-related threats and violence. First, we estimated the crude odds ratio for the dichotomized measures of all threatening and all violent incidents in 2010 as predictors for depressions in 2010, 2011, and 2015. Next, we adjusted for gender, age, and initial sector in Model 1 and furthermore adjusted for previous depression in Model 2 (continuous scale). We did the analysis across all four sectors and for each sector separately. In the latter analysis, we did not adjust for sectors.
Finally, across sectors, the associations were analyzed between work-related threats and violence in 2010 and depression in 2011, stratified by high and low level of social support, organizational justice, and workplace safety perception. In this analysis we adjusted for gender, sector, and age. We chose to present stratified analysis to present the two groups (high versus low levels) separately. Stratifications provide the reader with the opportunity to interpret the direction and the magnitude of the change in the estimate.
We only examined the modifying effect at an interval of 1 year because we had no information about the level of social support, organizational justice, and safety workplace perception in 2015.
Results were presented with odds ratios (ORs) and 95% confidence intervals (CIs). Statistical analyses were performed using SPSS (Version 20).
Results
Descriptive data are given in Table 1. Most participants were older than 40 years. In general, participants were oldest in elder care and youngest in the special schools. Most participants were women, especially in elder care, where only 3.3% were male employees. In the PPS, most participants were male employees (53.8%).
Descriptive Data of the Population in Four Human Service Sectors.
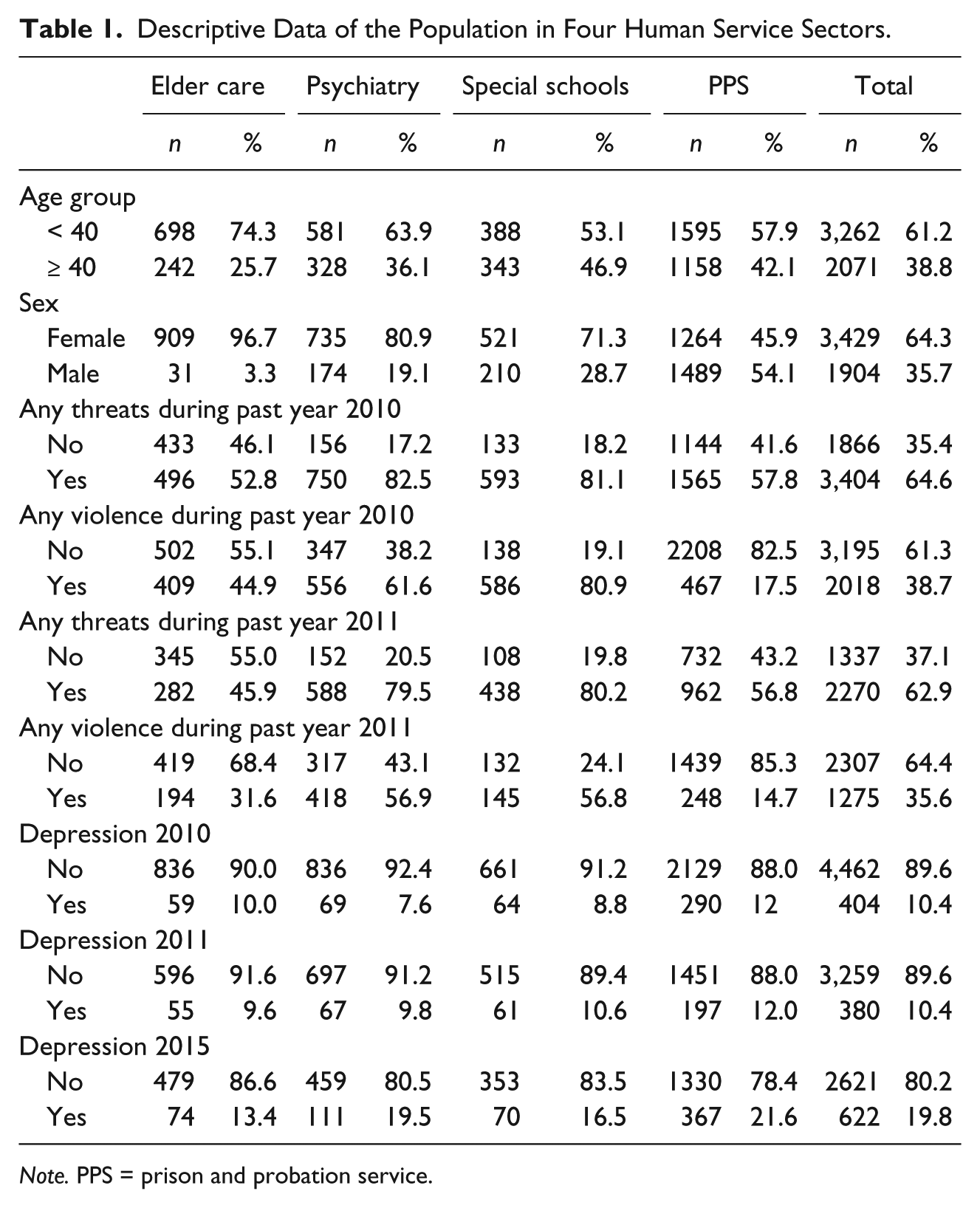
Note. PPS = prison and probation service.
Many participants were exposed to threats at work. In 2010, 64.6% reported having been exposed to work-related threats at least once during the last year. The frequencies were very high in the special schools and in the psychiatric wards, where 81.1% and 82.5%, respectively, had been exposed to work-related threats. The frequency of work-related violence was lower, but still 35.4% had at least once during the past year been exposed to work-related violence, and again the frequencies were higher in the special schools and the psychiatric wards, and much lower in the PPS (17.5%). Details regarding exposures in the cohort are available elsewhere (Rasmussen et al., 2013).
In all, 10.4% of the participants reported symptoms corresponding to clinical depression in 2010, increasing to 19.8% in 2015. In 2010, the highest frequencies of depressive symptoms were found in the elder care sector and in the PPS. In 2015, highest frequencies of depressive symptoms were found in the special schools and in the PPS.
The associations between work-related threats and depression are shown in Table 2. Across all sectors, work-related threats were associated with increased risk of depression in 2010 and in 2015. In 2011, work-related threats were not associated with an increased risk of depression after adjusting for baseline depression (see Model 2). For employees in elder care and in the PPS, work-related threats were associated with increased risk of depression in 2015 even after adjusting for previous depression. Furthermore, for employees working in psychiatric wards, the risk for depression following work-related threats was high in the short term (2011), and for employees working in special schools, the risk for depression following work-related threats was high in the long term (2015). However, the last-mentioned associations were not statistically significant. Finally, we note that after adjusting for baseline depression, all the estimates showed decreases.
Associations Between Exposure to Work-Related Threats and Risk for Depression in 2010, 2011, and 2015.
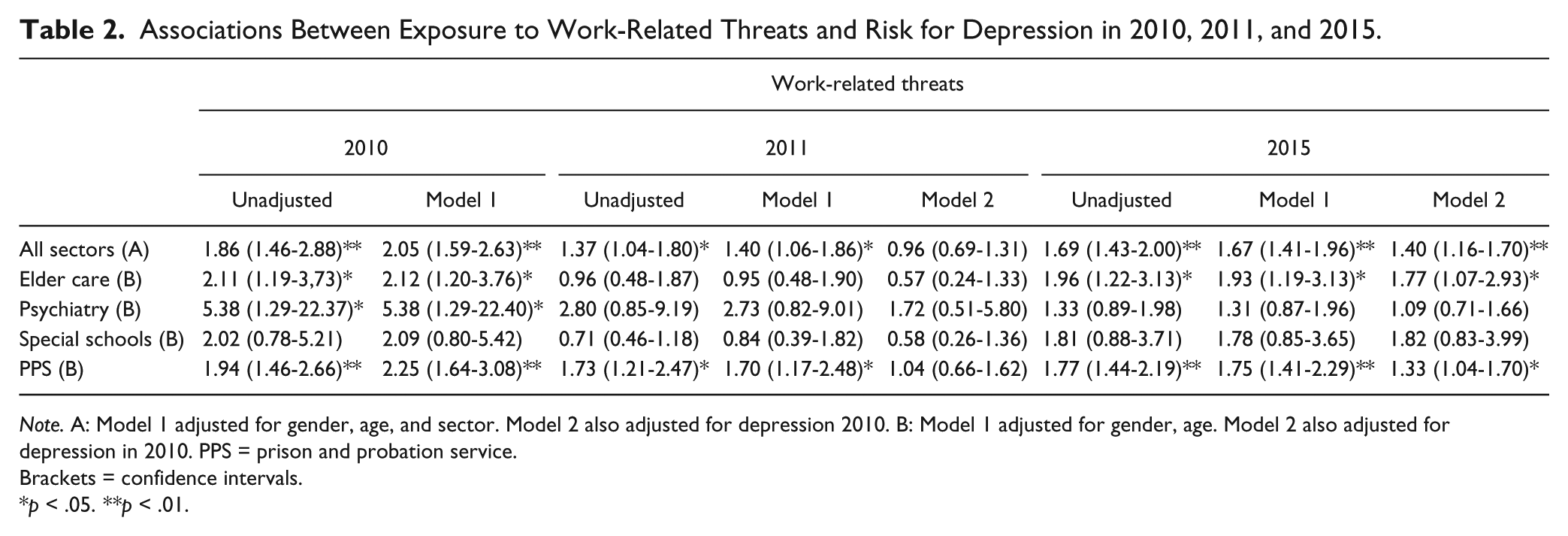
Note. A: Model 1 adjusted for gender, age, and sector. Model 2 also adjusted for depression 2010. B: Model 1 adjusted for gender, age. Model 2 also adjusted for depression in 2010. PPS = prison and probation service.
Brackets = confidence intervals.
p < .05. **p < .01.
The associations between work-related violence and depression are shown in Table 3. Across all sectors, work-related violence was associated with increased risk of depression in 2010, 2011, and 2015. However, in 2011 the association was not statistically significant after adjusting for previous depression (see Model 2). For employees in the PPS, work-related violence was associated with increased risk for depression in 2010, 2011, and 2015. For employees working in the elder sector, the effect of work-related violence showed the same tendency, although it was not statistically significant. For employees working in psychiatric wards, the risk for depression following work-related violence was increased in both 2011 and 2015, and for employees working in special schools, the risk for depression following work-related threats was higher in 2015. However, the last-mentioned associations were not statistically significant.
Associations Between Exposure to Work-Related Violence and Risk for Depression in 2010, 2011, and 2015.
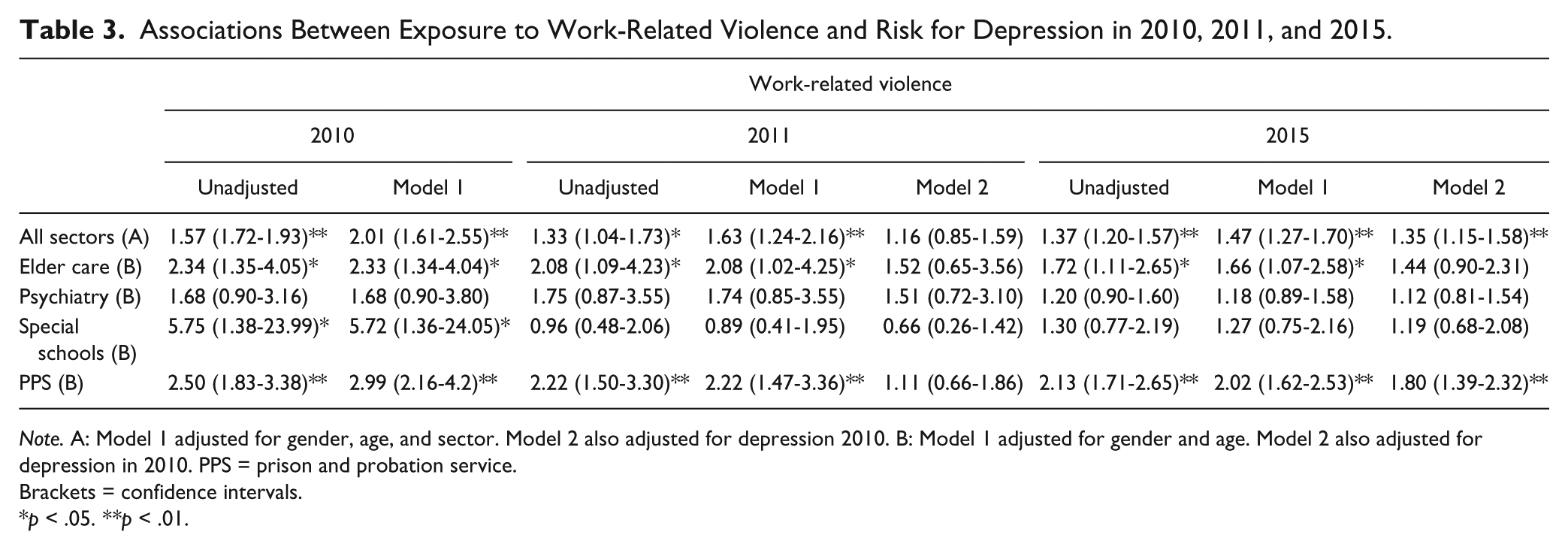
Note. A: Model 1 adjusted for gender, age, and sector. Model 2 also adjusted for depression 2010. B: Model 1 adjusted for gender and age. Model 2 also adjusted for depression in 2010. PPS = prison and probation service.
Brackets = confidence intervals.
p < .05. **p < .01.
Across all sectors, the risk for depression in 2010 and 2015 following work-related threats was slightly higher than the risk for depression following work-related violence, but the differences were very small. In 2011, the risk for depression was higher following work-related violence. However, for employees working in the PPS, the risk for depression subsequent to work-related violence was greater both short and long term. For employees working in psychiatric wards, the risk for depression subsequent to work-related threats was greater in the short term and for employees working in elder care and special schools the risk for depression following work-related threats was worse in the long term in 2015. However, in psychiatric wards and special schools the association was not statistically significant.
The associations between work-related threats in 2010 and depression in 2011, stratified by level and source of social support, organizational justice, and safety workplace perceptions, are shown in Table 4.
Associations Between Work-Related Threats in 2010 and Depression in 2011, Stratified by Level and Source of Social Support, Organizational Justice, and Safety Workplace Perception.
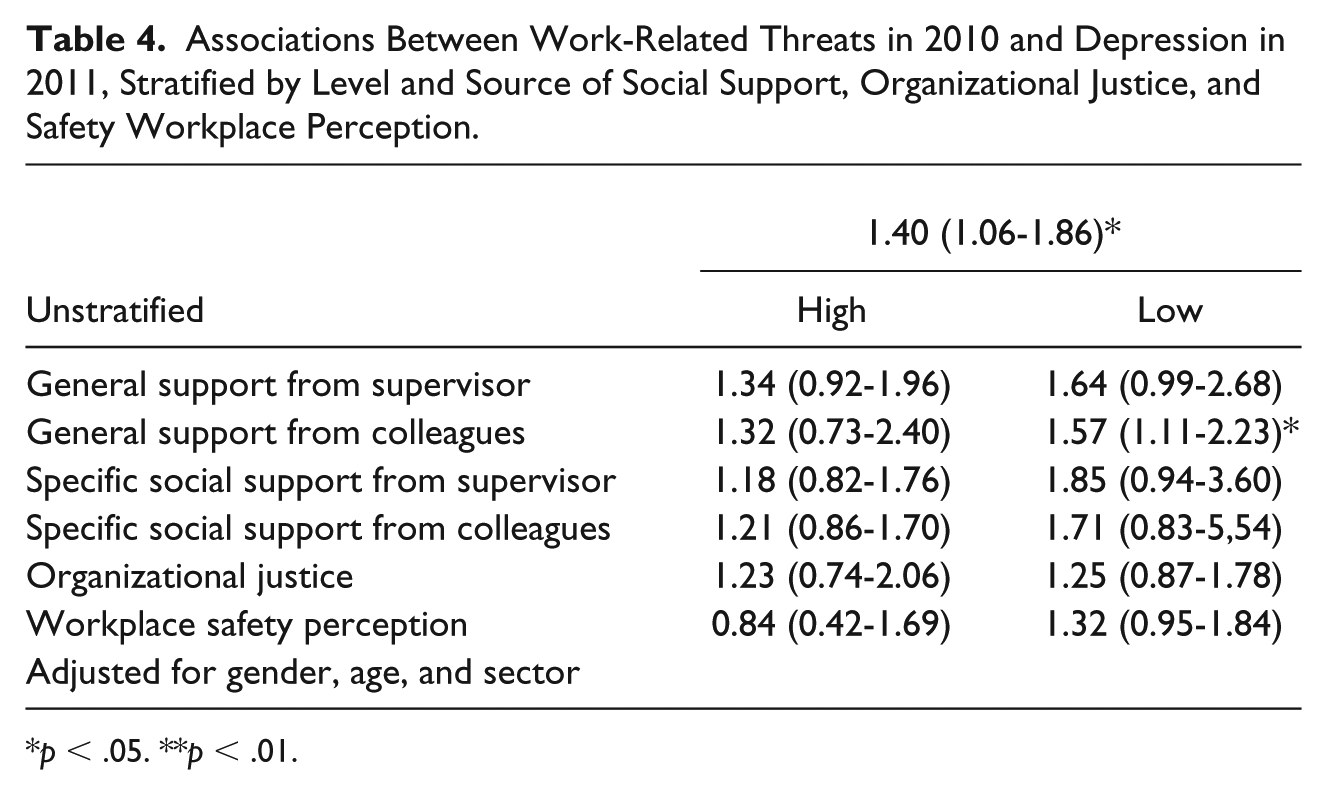
p < .05. **p < .01.
Overall, no significant differences were found between the effect of high or low levels of social support on the association between work-related threats and subsequent depression, but there was a tendency for high levels of specific social support to modify the association between exposure to work-related threats and subsequent depression. Furthermore, compared to low levels, high levels of safety workplace perceptions decreased the association between work-related threats and subsequent depression. However, the differences were not statistically significant.
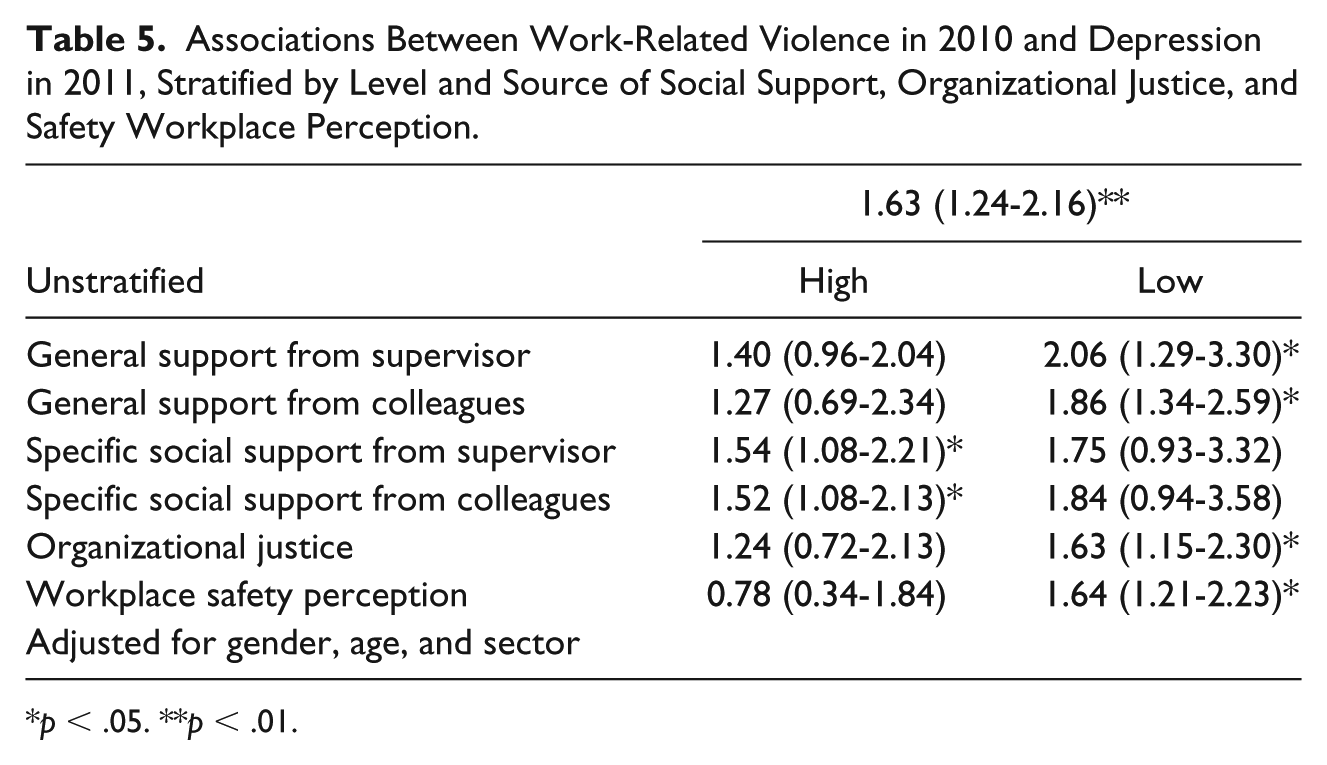
The associations between work-related violence in 2010 and depression in 2011, stratified by level and source of social support, organizational justice, and safety workplace perception, are shown in Table 5.
Associations Between Work-Related Violence in 2010 and Depression in 2011, Stratified by Level and Source of Social Support, Organizational Justice, and Safety Workplace Perception.
p < .05. **p < .01.
No statistically significant differences were found between the effect of high or low levels of social support on the association between work-related threats and subsequent depression, but there was a tendency for high levels of general support, especially general social support from colleagues, to modify the association between exposure to work-related violence and subsequent depression. Furthermore, high levels of organizational justice and especially high levels of workplace safety perceptions decreased the association between work-related threats and subsequent depression. However, none of the differences were statistically significant.
Discussion
We found that human service employees are exposed to high levels of both work-related violence and threats, especially employees working in psychiatric wards and in special schools. The frequency of work-related violence and threats in our study is high compared with other studies in Denmark among employees in comparable occupations (Borg, 2012). One explanation may be that we asked respondents whether they had been exposed to concrete threats and acts of violence instead of a general question, which only to a minor degree allowed respondents to self-determine whether a specific episode should be characterized as a work-related threat or an act of violence. The experience of threats and physical violence may be shaped by individual appraisals and attributions, social roles, and workplace norms, and this may result in differential misclassification bias. Thus, to overcome the individual or collective definition of work-related threats and violence, we asked respondents whether they had been exposed to concrete threats and acts of violence (Mackay, 1994).
We found that exposure to both work-related violence and threats increased the risk for depression both at short term and long term. The risk for depression in 2010 and 2015 following work-related threats was slightly higher than the risk for depression following work-related violence. The results suggest that depression can be a consequence for those employees exposed to work-related threats and violence. The result is in line with previous cross-sectional studies that have found associations between work-related violence and depression (Byun et al., 2009; Lam, 2002; da Silva et al., 2015). We found that work-related threats and violence increased the risk for depression cross-sectionally, but both 1 and 4 years later. The results are in line with previous longitudinal research that has found long-term associations between work-related violence and health consequences. For instance, a large cross-occupational study over 3.6 years found that the exposure to work-related violence increases the use of psychotropics (Madsen et al., 2011), and other studies have found an increased risk for long-term sick leave 1 and 3 years after exposure to work-related threats and violence (Clausen, Hogh, & Borg, 2012; Rugulies, Bultmann, Aust, & Burr, 2006). Finally, a study found increased risk for absence from work for those employees having been exposed to physical violence at work 10 years earlier (Friis, Larsen, & Lasgaard, 2017). However, considering sick leave as a consequence of work-related violence makes it difficult to determine which specific health problem is being measured.
Thus, our study contributes to the existing literature by providing longitudinal evidence for the long-term health consequence of work-related threats and violence in the form of an increased risk for depression.
Some sector differences were found. Both at short term as well as at long term (in 2015), employees working in the PPS were the most negatively affected by work-related violence compared to the other sectors, although the exposure to work-related violence and threats was higher in employees working in the special schools and psychiatric wards. One explanation may be that threats and violence experiences by employees in the PPS may be of a more life-treating nature. In line with this, a study found that employees in prisons were more often victims of “VID” (violence, injury, death) in their careers than others (Spinaris, Denhof, & Kellaway, 2012). Thus, the explanation for the increased risk for depression may be because employees in the PPS experience more danger during threatened and violent incidents than do individuals in the three others sectors. This is in line with previous research that has found that the danger experienced during the trauma is linked to an increased risk of posttraumatic symptoms (Ozer et al., 2008).
In this present study, employees working in elder care and at special schools had a higher long-term risk (in 2015) for depression following work-related threats although work-related threats in the elder sector and at special schools may be of a less life-threatening nature than threats in the PPS (e.g., the perpetrator was a pupil or an older client). However, especially for employees at special schools, depression following work-related threats may be the result of frequent, but less intense, minor threats and not just a result of one significant exceptional threat. The cumulative impact of less intense, minor stressors on mental health can have a stronger relationship with physical and psychological symptoms than single major stressful episodes (Heron, Bryan, Dougherty, & Chapman, 2013; Stefanek, Strohmeier, Fandrem, & Spiel, 2012).
We examined the modifying effect of social support, organizational justice, and safety perception. In our study, organizational social support was slightly associated with a decreased reporting of depressive symptoms. The result is in line with previous studies that have found that organizational social support can modify the association between work-related violence and negative health outcomes (Leather et al., 1998; Schat & Kelloway, 2003; van Emmerik et al., 2007). It was surprising that the modifying effect of social support on depression following work-related threats and violence was not stronger, as previous studies found statistically significant modifying effects of social support (Leather et al., 1998; Schat & Kelloway, 2003). However, social support may most likely occur when congruence exists among sources of social support, timing of social support, and type of social support (Leather et al., 1998). In the study by Schat and Kelloway (2003), social support was operationalized as emotional and instrumental support, which may better capture the type of social support that is needed following work-related threats and violence. Furthermore, we found that high levels of general social support from colleagues decreased the risk for depression following work-related violence. Previous studies have found that employees receiving more social support from colleagues reported less posttraumatic symptoms following a traumatic event (Hsieh et al., 2016; Stephens, Long, & Miller, 1997), which reveals the importance of the source of social support. In summary, although the results are subject to some uncertainty, social support seems to have some modifying effect on the association between work-related violence and threats and depression.
We found that organizational justice decreased the risk for depression following work-related violence, which is line with a previous study (Gluschkoff et al., 2017). One explanation may that fair organizations and supervisors are more proactive in preventing work-related violence, and employees feel supervisors’ support and help may decrease their reactions to work-related violence.
Finally, we found that workplace safety perceptions decreased the risk for depression following work-related threats and violence. Perceived lack of safety at the workplace may undermine the ability of employees to establish and maintain meaningful relationships at work, leading to decreased job investment and less commitment to the job (van Emmerik et al., 2007). One study found that 22% of those who reported that they had experienced work-related violence believed that the workplace environment did not provide sufficient safety for them to perform their duties satisfactorily (Fasanya & Dada, 2016). Therefore, it is essential for employers to foster a strong climate of safety (Hoffer Gittell, 2002). Enhancing employees’ perception of safety in the work environment and management commitment to safety may improve the feeling of safety and can instill a “feeling of security” among the employees (Isaak et al., 2017).
Limitations and Strengths
There are several limitations in this study that may have affected the results. First, depression may be related to factors other than work-related threats and violence. However, as we adjusted for gender, age, sectors, and previous depression, we believe that individuals exposed to work-related threats and violence did not differ from nonexposed individuals with regard to their risk for developing depression. Second, the occurrence of violence and threats at work and symptoms of depression was measured by self-report at the same time in the first round in 2010, and thus we cannot rule out the risk of common methods variance. Furthermore, the exposure to work-related threats and violence and the modifying variables (social support, organizational support, and workplace safety perceptions) were measured at the same time, and thus the perception of social support, organizational justice, and safety perception was measured after the exposure to work-related threats and violence. Therefore, we cannot rule out the possibility that perception of the modifying variables was influenced by the experience of work-related threats and violence, which may have led to misclassification.
Another limitation may be the initial inclusion procedure for participants in this study. Employees who had been absent from work for more than 3 weeks prior to receiving the questionnaire were excluded. This procedure was chosen because in a previous study in the same groups, our aim had been to estimate the associations between the psychosocial work environment and work-related threats and violence, and thus being present at work was crucial (Andersen, Hogh, Biering, & Gadegaard, 2018), but this procedure may have overlooked persons who were on long-term sick leave due to exposure to threats and violence or symptoms of depression. This could entail an underestimation of the associations in this study and thus introduce selection bias if the participants represent only those who are able to work.
Due to the feeling of helplessness often experienced by depressed individuals, employees with depressive symptoms may experience patients, clients, inmates, and pupils as more threatening, possibly causing response bias. However, we consider work-related violence to be less sensitive to such bias, and the association between work-related violence and depression showed nearly similar results as did the association between work-related threats and depression, suggesting that response bias does not substantially influence the results.
It may be a limitation that some associations between variables were not statistically significant. However, the purpose of the study was to examine associations between variables, and reducing data analysis to rules such as considering statistical significance a prerequisite for definite conclusions can overlook relevant information. In cohort studies like this in which exposure and the size of groups is not randomly assigned, the power will be affected in some analysis and important associations may be overlooked. Therefore, the sizes of the risk estimates may provide important information and be of practical relevance regardless of statistical significance (Wasserstein & Lazar, 2016).
Although the threatening and violent acts vary in quality, we decided not to differentiate between the different threatening and violent acts, as previous research has found that the danger experienced during a trauma is linked to an increased risk of posttraumatic symptoms, not the event itself (Ozer et al., 2008).
The dichotomization of the dependent variables may cause some loss of information; however, dividing groups with regards to high or low levels of exposure to work-related violence and work-related threats may enhance the understanding of the mechanisms and the direction of the estimates. Both outcomes were sum-scales of a range of threatening and violent events, in combination with their frequency. However, these events are not necessarily comparable; something that has happened frequently may not have the same impact as something that happened only once but was of a more serious nature. Also, across the four sectors, the same event may have been experienced differently. By dichotomizing these scales, we intended to identify those most affected.
It can be discussed whether the reported baseline is a true baseline or just an arbitrary point in time (Cologne, 2006). The exposure to work-related threats and violence seems to be rather stable over time in these sectors as the frequencies of work-related threats and violence were high in 2010, 2011, and in 2015. Thus, the frequencies of work-related violence may have been high during the years before data collection. Therefore, the effects of the expose to work-related threats and violence measured in 2010 on symptoms of depression measured in 2011 may be an accumulated effect of work-related threats and violence that had taken place before the data collection.
Finally, the study has several strengths. We used a more objective way to measure the exposure to work-related threats and violence, which to a minor degree allows the participants to self-determine whether a specific episode should be defined as a work-related threat or violence or not. Furthermore, the sample size is large compared to previous studies of the health consequences of work-related threats and violence, the response rates are high, and we used a follow-up design. Finally, we used a validated measure of depression.
Conclusion
Employees working in the human service sector are very frequently exposed to work-related violence and threats. The results show that work-related threats and violence increase the risk for depression in subsequent years. It is important to note that risk for depression was affected not only by work-related violence but also by work-related threats.
The major practical implication of this research is that the negative health-related consequences of workplace violence may be modified by interventions that enhance the availability of social support. Furthermore, to decrease the risk for depression following work-related threats and violence, it is important for managers to create safe workplaces and to manage their employees fairly and justly.
Finally, our results should provide impetus for future research to examine other factors that could help to prevent or reduce the negative consequences of workplace violence. Preventing or reducing the negative consequences of workplace violence and threats is not only an issue for high-risk occupations but also for social workers, bus and taxi drivers, service workers, general practitioners, and home care workers as they can also be exposed to violence and threats. In these sectors, prevention may be even more important as the employees often work alone and it may be difficult to get help.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Danish Environmental Research Fund (Grant No. 14-2014-03/2014416500).