
Abstract
This study used data from the National Survey of Child and Adolescent Well-Being II to examine the effects of intimate partner violence (IPV) on child-welfare-involved toddlers’ psychosocial development. The sample was limited to toddlers aged 12 to 18 months with mothers who did (n = 102) and did not (n = 163) report IPV physical victimization. Multiple linear regression analyses showed, when compared with mothers who did not report IPV physical victimization, mothers who reported IPV physical victimization were more likely to have toddlers with higher levels of socioemotional and behavioral problems (B = 5.06, p < .001). Conversely, delayed social competence was not associated with IPV (B = −1.33, p > .05). Further analyses examining only toddlers with mothers who reported IPV physical victimization revealed, when compared with IPV-exposed toddlers who had a child welfare report of physical abuse as the primary maltreatment type, those with IPV as the primary maltreatment type were at lower risk of having socioemotional and behavioral problems (B = −12.90, p < .05) and delayed social competence (B = 3.27, p < .05). These findings indicate a significant concern regarding toddler psychosocial development when a mother has experienced IPV. This concern is even greater among IPV-exposed toddlers who experience physical abuse. We recommend child welfare workers assess for IPV. Once identified, early prevention and intervention services should be offered and tailored to the specific needs of IPV-affected families.
Intimate partner violence (IPV) is a public health issue that affects families on a daily basis. It is estimated that 15.5 million children live in households where IPV has occurred during the past year (McDonald, Jouriles, Ramisetty-Mikler, Caetano, & Green, 2006). Child stressors related to IPV are associated with poor developmental and behavioral outcomes (Evans, Davies, & DiLillo, 2008; Martinez-Torteya, Bogat, von Eye, & Levendosky, 2009; McDonald, Jouriles, Briggs-Gowan, Rosenfield, & Carter, 2007). In addition, families affected by IPV face environmental stressors that increase the risk of children being abused, neglected, or both (Hazen, Connelly, Kelleher, Landsverk, & Barth, 2004; Hornor, 2005). This is particularly true for younger children.
Age has been shown to be a significant predictor of child maltreatment in IPV households. Children younger than 5 years are disproportionally represented in households experiencing IPV and are at greatest risk of additional child maltreatment (Fantuzzo, Boruch, Beriama, Atkins, & Marcus, 1997; Fusco & Fantuzzo, 2009). IPV during the first 6 months of child rearing is a predictor of multiple types of child maltreatment. Families experiencing IPV during those first 6 months were more than 3 times as likely to experience substantiated physical child abuse, and more than twice as likely to experience substantiated psychological child abuse and/or child neglect than families with no reported IPV (McGuigan & Pratt, 2001).
Due to these risks, many children living in households with IPV are likely to become involved with child welfare services (Hazen et al., 2004). Despite this fact, few researchers have explored the effects of IPV on children involved with child welfare systems. Child welfare researchers have instead focused on its effects on mothers (Dosanjh, Lewis, Mathews, & Bhandari, 2008; Hazen et al., 2004) or combined IPV with other variables, making it difficult to determine its effects on children (Horwitz et al., 2012). The limited amount of child welfare research exploring the effects of IPV on children is concerning, given prior research has demonstrated (a) IPV typically occurs during a critical period of child development (Britto & Pérez-Escamilla, 2013) and (b) child-welfare-involved families affected by IPV may not be receiving appropriate services (Kohl, Barth, Hazen, & Landsverk, 2005).
The current study explored the effects of IPV on the psychosocial outcomes of toddlers aged 12 to 18 months involved in the child welfare system. We define IPV as physical violence against child-welfare-involved mothers perpetrated by a current or former intimate partner. By studying the association between IPV and toddler psychosocial development, we hoped to generate information that would further the understanding of how child welfare services can be tailored to the specific needs of families with toddlers affected by IPV.
Theoretical Framework: Stress and Coping Theory
To understand the ways in which mothers and toddlers are affected by and cope with IPV, it is helpful to view stress and coping through a theoretical framework. Lazarus and Folkman’s (1984) model of stress and coping posits stress is viewed as anything that depletes or exceeds an individual’s resources and jeopardizes his or her well-being. This model perceives emotion and coping as a “dynamic mutually reciprocal relationship” (Folkman & Lazarus, 1988, p. 311), and describes coping as a mediator of an individual’s emotional response. Lazarus and Folkman stated problem-focused coping and emotion-focused coping are used in different situations depending on environmental stressors. Problem-focused coping is used when individuals perceive they can change a distressing situation, whereas emotion-focused coping is implemented when individuals attempt to regulate the distress they are experiencing. Perceptions of environmental stressors have a significant effect on a mother and child’s capacity to cope and help explain the extensive ways that maternal and child well-being are affected by IPV.
Schechter and Willheim (2009) examined the effect of IPV and other developmental disturbances on toddlers between infancy and 3 years old. They found toddlers exposed to developmental disturbances exhibited internal and external behavioral issues, including difficulty being soothed, absence of affect, withdrawn behavior, and difficulty with emotional regulation. Levendosky, Bogat, and Huth-Bocks (2011) referred to IPV as “an assault on the caregiving system” (p. 516). This assault leads to maternal difficulty modeling emotional regulation, which in turn affects the child’s ability to learn how to self-regulate. In addition, the child’s physical and psychological needs may not be met by the mother due to collateral effects of IPV exposure.
Interestingly, quality of parent–child relationships may protect against behavioral problems in toddlers exposed to IPV (Letourneau, Tramonte, & Willms, 2013; Schultz et al., 2013). For example, Letourneau et al. (2013) utilized the Western Australian Child Health Survey to assess parenting behaviors and found that although mothers exposed to IPV had lower baseline scores on three parenting behaviors (Positive Discipline, Warm and Nurturing Parenting, and Consistent Parenting) than mothers not exposed to IPV, mothers exposed to IPV demonstrated less of a decrease in Warm and Nurturing scores over time. This suggests a positive parenting coping strategy, in that mothers with IPV-exposed toddlers attempt to compensate for other parenting deficits by remaining more sensitive to child needs throughout development.
Effect of IPV on Children
Several studies have found a significant relationship between IPV exposure and impaired biopsychosocial functioning among children. In a meta-analysis of 41 studies, Wolfe, Crooks, Lee, McIntyre-Smith, and Jaffe (2003) found IPV was related to emotional and behavioral problems in children. In addition, they found IPV coupled with child abuse increased the severity of emotional and behavioral problems beyond IPV alone. Kitzmann, Gaylord, Holt, and Kenny (2003) also conducted a meta-analysis of 118 studies that focused on psychosocial adjustment outcomes of children who witnessed IPV. They found children who witnessed IPV had significantly worse psychosocial adjustment outcomes than children who did not witness IPV. Furthermore, when children witnessed IPV and experienced physical abuse, they were more likely to have externalizing symptoms and psychological problems compared with children who only witnessed IPV. In a meta-analysis conducted by Evans et al. (2008), results of a review of 60 studies confirm IPV is significantly related to internalizing and externalizing behaviors and trauma symptoms. Finally, in the most recent meta-analysis conducted by Chan and Yeung (2009), findings supported previous meta-analyses regarding adjustment outcomes (Evans et al., 2008; Kitzmann et al., 2003; Wolfe et al., 2003). Of the 37 studies examined, children’s adjustment outcomes were significantly affected by exposure to IPV.
Although prior meta-analyses have shed light on the effects of IPV on children’s psychosocial development, the majority of included studies defined IPV as a dichotomized event (yes or no) as opposed to a continuous event. This is problematic because the experiences of children who have witnessed several IPV events may differ from those who have only witnessed one IPV event. In addition, these studies failed to examine the effect of IPV severity. Finally, few of the studies included children younger than 3 years, therefore missing opportunities to gain important information about risk and protective factors regarding children’s response to stress during a critical developmental period.
Goals of Current Study
This study examined the effect of IPV physical victimization frequency and severity on the psychosocial development of toddlers between 12 and 18 months old who had been investigated for maltreatment. In addition, we explored other characteristics that may influence IPV-exposed toddlers’ psychosocial outcomes. Specifically, we addressed the following research questions:
Based on the stress and coping theory, we hypothesized that toddlers with mothers who experienced higher frequencies of IPV physical victimization and severe forms of IPV physical victimization would be more likely to have socioemotional and behavioral problems and delays in social competence than toddlers with mothers who experienced less frequent and less severe episodes of IPV physical victimization. This study adds to the literature by focusing on the effects of IPV on the psychosocial outcomes of a unique age group (toddlers). The authors sought to better understand the prevention and intervention needs of child-welfare-involved families affected by IPV to strengthen family systems and enhance toddler developmental outcomes.
Method
Study Design
The current study used data from the second cohort of the National Survey of Child and Adolescent Well-Being II (NSCAW II) to examine the proposed research questions. The NSCAW II is a nationally representative sample of 5,872 children from families that were referred to and investigated by child welfare agencies for potential child abuse or neglect between February 2008 and April 2009. Children had to be at least 17.5 years to be eligible for the NSCAW II study. The children were sampled from child welfare agencies across 81 primary sampling units (PSUs), representing agencies from 81 U.S. counties in 30 states. Children were randomly selected from completed maltreatment investigation cases in each of the PSUs. To ensure the PSUs were nationally representative, a complex weighting strategy that accounted for stratification, clustering, weighting, and oversampling of infants and children in out-of-home placement was used. Additional information regarding sampling design and methods is available elsewhere (Dolan, Smith, Casanueva, & Ringeisen, 2011).
Analytic Sample
Data were collected via face-to-face interviews with multiple sources, including children, parents, nonparent adult caregivers, and investigative caseworkers. At the time of the current study, data had been collected at 3 time points (baseline, 18-month follow-up, and 36-month follow-up). Baseline data from parents were used in the current study’s analyses. Male caregivers, nonbiological caregivers, biological caregivers without toddlers between 12 and 18 months old, and caregivers of toddlers placed in out-of-home care following a maltreatment investigation were excluded from this study, resulting in a sample of 385 mothers with toddlers aged 12 to 18 months (toddlers) in the home at baseline. Consequently, our study findings may be generalized only to mothers with toddlers who remain in the home following a child maltreatment investigation. Furthermore, due to missing data on key variables (n = 120 mothers), our final sample consisted of 265 mothers who voluntarily reported their IPV experiences: 102 mothers who reported they experienced IPV during the past year (recent IPV) and 163 mothers who reported they did not experience recent IPV. However, no significant changes were observed in sample characteristics due to reducing the sample. 1
Measures
Dependent variables
Mothers were interviewed about their child’s socioemotional and behavioral problems and delays in social competence using the Brief Infant Toddler Social Emotional Assessment (BITSEA; Briggs-Gowan & Carter, 2006). The BITSEA is a 42-item instrument designed to be administered to caregivers of toddlers aged 12 to 36 months. This instrument has been proven reliable (Pearson’s correlations were .90 for the Problem subscale and .80 for the Competence subscale for boys and girls) and has construct, convergent, and divergent validity (Baxter, 2007). The current study had Cronbach’s alpha of .9998 for the Problem subscale and .9992 for the Competence subscale, indicating high internal consistency.
Toddler socioemotional and behavioral problems
The BITSEA Problem subscale was used to assess potential socioemotional and behavioral problems among toddlers. This subscale consists of 31 items, such as “Child seems nervous, tense, or fearful” and “Child has trouble adjusting to change.” Response options for each item ranged from 0 (not true or rarely) to 2 (very true or often). Responses were summed to generate a total BITSEA problem score. Scores could range from 0 to 62, with higher scores indicating more potential socioemotional and behavioral problems. Although continuous scores were used for this measure, it is noteworthy that a cutoff score of 13 or higher for girls aged 12 to 18 months and boys aged 12 to 17 months indicates a possible socioemotional or behavioral problem. Whereas a cutoff score of 15 or higher was used to indicate a potential problem for 18-month-old boys.
Toddler delayed social competence
The BITSEA Competence subscale was used to assess potential delays in social competence. This subscale consists of 11 items. Examples of items include “Child shows pleasure when he or she succeeds (e.g., claps hands for self)” and “Child imitates playful sound when you ask him or her to.” Similar to the BITSEA Problem subscale, response options ranged from 0 (not true or rarely) to 2 (very true or often). Responses were summed to generate a total BITSEA competence score. Scores could range from 0 to 22, with lower scores indicating more potential for delayed social competence. A cutoff score of 12 or lower for boys and girls aged 12 to 17 months indicates a possible delay in social competence. A cutoff score of 14 or lower indicates potential delayed social competence for 18-month-old boys and girls.
Independent variable
Maternal reports of IPV physical victimization were measured using the Physical Assault subscale of the Conflict Tactics Scale–2 (CTS-2; Straus, 1990) administered via computer-assisted audio self-interviews. The CTS-2 Physical Abuse subscale consists of 13 items that measure physically abusive behaviors between intimate partners, such as throwing something at, slapping, or pushing a partner. Acts of severe IPV physical victimization were also identified using the CTS-2. Severe violence behaviors were those identified as posing a greater risk of injury and requiring medical attention (e.g., being choked, beaten up, threatened with a knife or gun). Mothers in the sample were considered to have experienced IPV physical victimization if they reported being a victim of at least one act of physical abuse during the past year (i.e., recent IPV physical victimization); and severe IPV if they reported at least one act of severe IPV during the past year. Response categories include 0 (not at all), 1 (1 time), 2 (2 times), 3 (3-5 times), 4 (6-10 times), 5 (11-20 times), and 6 (more than 20 times). Total scores were calculated by summing the midpoint for the response categories selected by the participant. For example, if a participant indicated that she was slapped by an intimate partner 3 to 5 times during the past year, the incident was recorded as occurring 4 times. This approach has been used in prior studies using the CTS frequency measure (e.g., Hazen et al., 2004). CTS-2 Physical Abuse subscales have been proven valid and reliable (α = .67-.86; Newton, Connelly, & Landsverk, 2001). Our study had a Cronbach’s alpha of .94, indicating high internal consistency.
Covariates
Demographic characteristics
We compared demographic characteristics of mothers who did and did not report recent IPV physical victimization. This included information about their age, child’s age, child’s gender, and child’s race/ethnicity.
Maternal functioning
We also examined risk factors related to maternal functioning. These risk factors included child maltreatment, parenting quality, depressive symptoms, and substance use. The selection of maternal functioning variables was based on empirical evidence, which suggested these variables were important correlates of child behavior and adjustment among children exposed to IPV (e.g., Bauer, Gilbert, Carroll, & Downs, 2013; Whitaker, Orzol, & Kahn, 2006).
Child maltreatment
Caseworkers were interviewed about the most serious type of child maltreatment experienced that led to the child’s inclusion in the NSCAW II study, using the Modified Maltreatment Classification System (MMCS; English & the LONGSCAN Investigators, 1997). The MMCS includes detailed questions about the specific nature of the alleged abuse or neglect. For each child, caseworkers reported all types of child maltreatment included in the case report. After recording all types of child maltreatment, caseworkers were asked to use the MMCS to classify which they perceived as the most serious type of maltreatment.
Parenting quality
The Home Observation for Measurement of the Environment–Short Form (HOME-SF) inventory for toddlers aged 2 years or younger was used to measure mother’s behaviors toward the child and various aspects of the physical environment (e.g., safe play environment, size of living space). The HOME-SF was developed by the National Longitudinal Study of Youth (Baker, Keck, Mott, & Quinlan, 1993). This instrument includes both observational and scripted measures; however, only scripted items were used in the current study because this measure had less missing data. HOME-SF for toddlers aged 0 to 2 consists of 13 scripted measures about the child’s home environment; and two subscales assessing (a) child’s cognitive stimulation and (b) emotional support. A sum of scores from the two subscales was used to generate a total score. Higher HOME-SF total scores indicate better parenting qualities. Studies examining the HOME’s psychometric properties reveal internal consistency ranging from .30 to .80, and interrater reliability greater than or equal to 85% (Bradley, 1994).
Depressive symptoms
Maternal depressive symptoms were measured using the Composite International Diagnostic Interview Short–Form (CIDI-SF; Kessler, Andrews, Mroczek, Ustun, & Wittchen, 1998). The CIDI-SF is a 21-item instrument that evaluates symptoms of major depression using criteria from the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994). Respondents are classified as having major depressive symptoms if they respond yes to one of the following diagnostic screening categories: (a) have dysphoric mood (feeling sad, blue, or depressed) in a 2-week period during the past 12 months, (b) have anhedonia (lack of enjoyment of any activity) for most of the day in a 2-week period during the past 12 months, or (c) take medication for depression. In addition to endorsing a screening question, respondents must confirm experiencing three or more symptoms of depression from the following list: gain or loss of weight, increased or decreased sleep, feelings of guilt or worthlessness, diminished ability to concentrate, and recurring thoughts of death or suicide.
The CIDI-SF has been deemed a reliable and valid scale. Studies assessing its interrater reliability report a range from .67 to 1 (Andrews, Peters, Guzman, & Bird, 1995; Wittchen et al., 1991); concordance with clinical diagnoses ranged from .76 to .84 (Janca, Robins, Bucholz, Early, & Shayka, 1992).
Substance use
Alcohol and/or substance use was examined using caseworker risk assessment reports of whether there was active alcohol abuse (yes or no) or substance use (yes or no) by the caregiver at the time of investigation. In addition, caregivers reported on their alcohol and substance use using the Alcohol Use Disorders Identification Test (AUDIT) and Drug Abuse Screening Test (DAST-20), respectively. Caregivers were determined to have an alcohol or substance use problem if either their caseworker reported so or they met the criteria using the AUDIT or DAST-20.
AUDIT
The AUDIT is a 10-item instrument developed by the World Health Organization (WHO) as a brief method of screening for excessive drinking during the past year. The instrument includes questions such as “How often during the last year have you found that you were not able to stop drinking once you had started?” Responses were scored on a 4-point scale with options varying by question. Items were summed to generate a total score with a possible range from 0 to 40. While the AUDIT manual recommends considering a total score of 8 or higher as evidence of harmful use or alcohol dependence, a review of studies using the AUDIT found that this cutpoint should be lowered to adequately detect harmful use or dependence in women (Reinert & Allen, 2002): likely a cutpoint greater than or equal to 5. Therefore, the current study used a cutoff score greater than or equal to 5. The AUDIT has demonstrated to be a valid (Reinert & Allen, 2002) and reliable (alpha = .79 with cutpoint of 5; Neumann et al., 2004) measure for detecting dependence or risky alcohol consumption in women.
DAST-20
The DAST-20 is a 20-item instrument used to identify individuals who have been abusing psychoactive drugs during the past year. DAST-20 scores are highly diagnostic with respect to a DSM diagnosis of psychoactive drug dependence. A yes or no (scored as 1 or 0, respectively) response is requested for questions such as “During the past 12 months, have you been in trouble at work because of drug abuse?” Scores are summed and can range from 0 to 20. Although the cutoff score for substance use and/or dependence is generally 6 or above, the current study used 5 as a cutoff score. This decision was made based on research that suggests a cutoff of 5/6 had the maximum sensitivity or ability to detect substance use cases (Cocco & Carey, 1998; Staley & El-Guebaly, 1990). The DAST-20 has demonstrated high internal consistency (α = .92; Cocco & Carey, 1998). Discriminant validity has been demonstrated by the scale’s ability to differentiate individuals with primary alcohol problems, drug problems, or some combination of alcohol and drug problem (Staley & El-Guebaly, 1990).
Analytic Plan
All analyses were conducted using Stata 12 software. Descriptive statistics were used to summarize demographic and maternal functioning characteristics. In addition, bivariate analyses (i.e., f test and t test) were employed to explore the relationship between mothers who reported recent IPV physical victimization and mothers who did not report recent IPV physical victimization. Finally, linear regression models were examined to assess the influence of (a) IPV on toddlers’ socioemotional and behavioral problems and delayed competence; and (b) IPV frequency and severity on IPV-exposed toddlers’ socioemotional or behavioral problems and delayed social competence. In this analysis, we controlled for all covariates measured in the study. Furthermore, because the IPV data were positively skewed (see Figure 1), we conducted a log transformation to make the positive skew more normal (see Figure 2). We used the transformed version of the variable in regression models involving IPV frequency (i.e., Model 2 and Model 4).
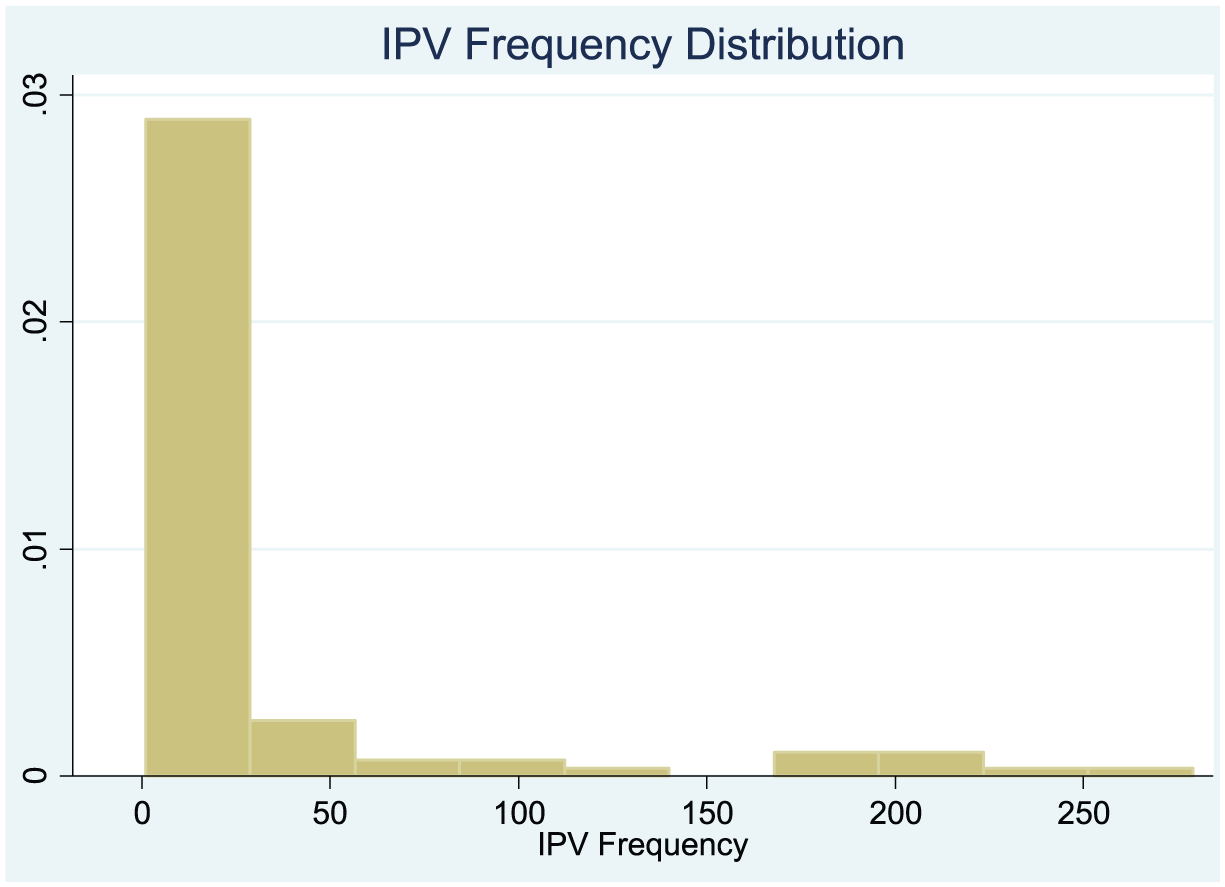
IPV frequency distribution prior to log transformation of data.
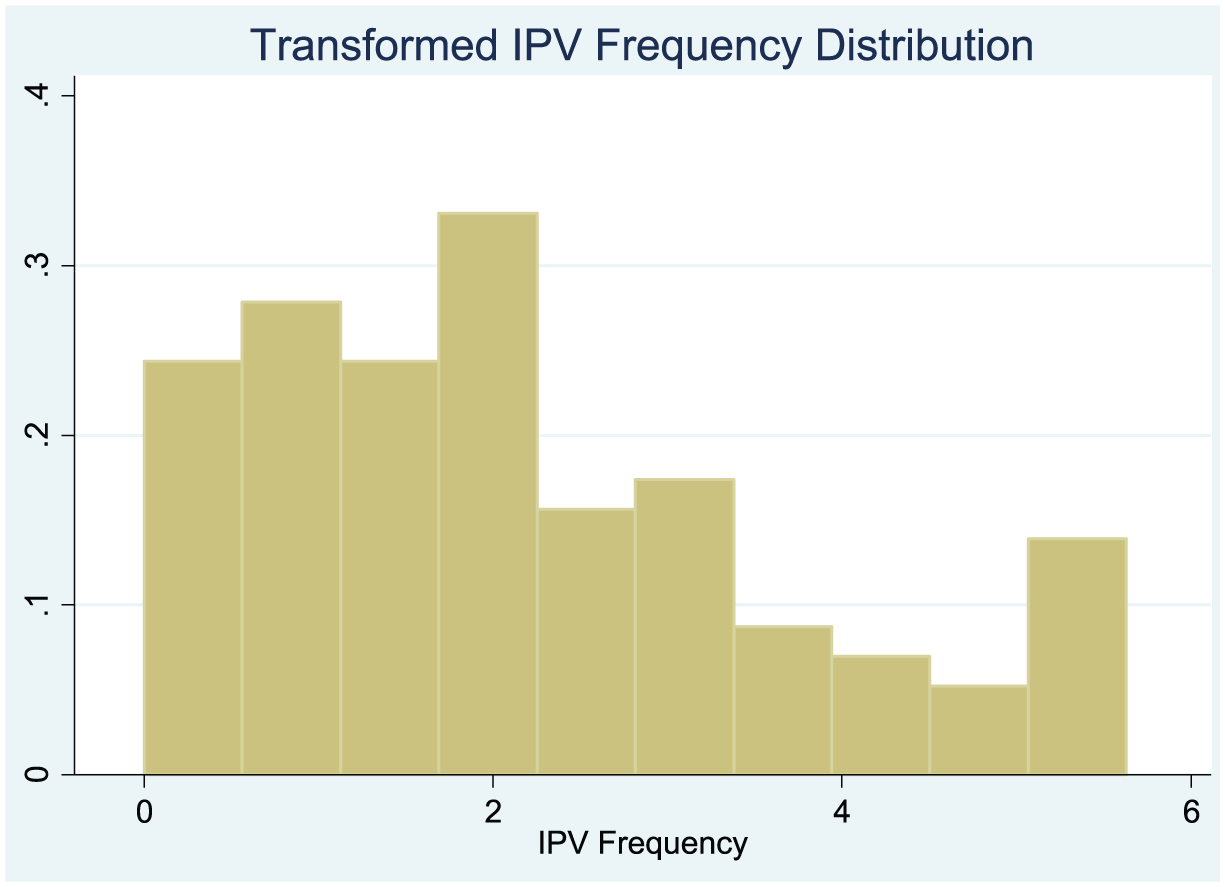
IPV frequency distribution post log transformation of data.
All analyses presented in this study used NSCAW II sampling weights that were created for national generalization and may be applied to mothers in the U.S. child welfare population with toddlers aged 12 to 18 months remaining in the home. In some cases, nonweighted sample sizes are presented to provide information about the amount of data on which analyses were based.
Results
Sample Characteristics
Of the 265 mothers included in this study, 29.07% (unweighted n = 102) reported recent IPV physical victimization with an average frequency of 14.08, and 25.07% (unweighted n = 102) reporting severe IPV physical victimization. Comparisons between the characteristics of mothers who reported recent IPV and those who did not (see Table 1) revealed similarities in their age, parenting quality, substance use, and child’s gender (p > .05). Although the two groups were similar in many ways, they significantly differed in terms of child’s age, depressive symptoms, child race and ethnicity, and primary maltreatment type. Compared with mothers who did not report recent IPV physical victimization, mothers who reported recent IPV physical victimization were more likely to have younger toddlers, F(1, 72) = 6.34, p = .014, and depressive symptoms, F(1, 72) = 5.99, p = .017. Their toddlers were less likely to be African American, F(1, 72) = 26.76, p < .001. Instead, they were more likely to have their race and ethnicity categorized as other, F(1, 72) = 148.60, p < .001. In addition, they were more likely to be classified as having emotional abuse, F(1, 72) = 6.38, p = .014, substance using parent, F(1, 72) = 6.33, p = .014, or IPV as their primary maltreatment type, F(1, 72) = 11.65, p = .001; and less likely to have neglect-failure to provide, F(1, 72) = 8.75, p = 004, or “other,” F(1, 72) = 21.88, p < .001.
Maternal and Child Demographics.

Note. Unweighted sample size reported; proportions and means are based on weighted data. The F tests conducted on categorical variables, and t tests conducted on maternal age and cumulative risk score variables. IPV = intimate partner violence.
Socioemotional and Behavioral Problems
Toddlers’ socioemotional and behavioral problem scores ranged from 1 to 36 in the current study. On average, toddlers with mothers who reported IPV physical victimization had significantly (p < .05) higher levels of socioemotional and behavioral problems (M = 13.68) than toddlers with mothers who did not report IPV physical victimization (M = 8.29). This was true even after controlling for differences in demographic and caregiver functioning characteristic. A multiple linear regression model predicting IPV’s impact on socioemotional and behavioral problems (see Table 2; Model 1) revealed that, taking into account control variables, mothers who experienced IPV physical victimization had toddlers with higher levels of socioemotional and behavioral problems, by approximately 5.15 units (95% confidence interval [CI] = [2.33, 7.97]). This model also suggests maternal substance use and depressive symptoms predict higher socioemotional and behavioral problem scores (p < .05). Conversely, alleged IPV as the primary maltreatment report predict lower socioemotional and behavioral problem scores compared with physical abuse (95% CI = [−13.07, −1.50]).
Linear Regression Predicting Potential Socioemotional or Behavioral Problems.

Note. B = beta; CI = confidence interval; IPV = intimate partner violence; ref. = reference category.
p < .05. **p < .01. ***p < .001.
In the second regression model examining predictors of socioemotional and behavior problems (Table 2; Model 2), only toddlers with mothers who reported IPV physical victimization were examined. In addition to the control variables included in Model 1, this model included measures of IPV frequency and severity. Results indicate that IPV frequency and severity are not significant predictors of socioemotional and behavioral problems among toddlers exposed to IPV physical victimization (p > .05). However, among toddlers with mothers who reported IPV physical victimization, mothers’ age, child’s race/ethnicity, and primary maltreatment type are significant predictors of socioemotional and behavioral problems. The model predicts socioemotional and behavior problems scores decrease by 0.52 for every year mothers’ age increases (95% CI = [−0.71, −0.34]). Furthermore, the model predicts higher socioemotional and behavioral problem scores for African American toddlers compared with White toddlers (95% CI = [0.97, 8.29]). All primary maltreatment types, including IPV, predicted significantly lower behavior problem scores than physical abuse maltreatment type.
Delayed Social Competence
Delayed social competence scores ranged from 4 to 22. Results from bivariate analyses revealed no significant difference in delayed social competence scores when comparing toddlers with mothers who reported IPV physical victimization (M = 14.02) with those without IPV physical victimization reports (M = 15.15). Similarly, the multiple linear regression model predicting the impact of IPV physical victimization on delayed social competence suggests that mothers’ IPV experience is not a significant predictor of delayed social competence, after controlling for covariates (Table 3; Model 3; 95% CI = [−2.76, 0.09]). However, this model predicts toddlers with a race/ethnicity categorized as “Other” were more likely to have scores indicating delays in social competence (i.e., lower scores) than White toddlers; and toddlers with substance using parent as the primary maltreatment type compared with those with physical abuse were less likely to have scores indicating delays in social competence (i.e., higher scores).
Linear Regression Predicting Delayed Social Competence.

Note. B = beta; CI = confidence interval; IPV = intimate partner violence; ref. = reference category.
The n value for model 3 is 265.
p < .05. **p < .01.
When examining predictors of delayed social competence among toddlers with mothers who reported IPV physical victimization (Table 3; see Model 4), we found that neither IPV frequency nor IPV severity are predictors (p > .05). Instead, child’s age and primary maltreatment type were found to be significant predictors. The model predicts delayed social competence scores increase by 0.59 for every month child’s age increases (95% CI = [0.06, 1.12]), suggesting the older the IPV-exposed toddler, the less likely he or she is to have delayed social competence. Furthermore, it was predicted that the following primary maltreatment types decrease risk for delayed social competence when compared with physical abuse maltreatment type: emotional abuse, substance abusing parent, and IPV primary maltreatment types (p < .05).
Discussion
In this study, we investigated the effect of IPV frequency and severity on the psychosocial development (i.e., socioemotional development, behavioral development, and social competence) of toddlers between 12 and 18 months old who had been investigated for maltreatment. In addition, other variables were examined that might influence psychosocial outcomes of toddlers exposed to IPV physical victimization, including demographic characteristics, maternal functioning (i.e., major depressive symptoms and substance use), child maltreatment, and parenting quality.
We found that toddlers with mothers who reported IPV physical victimization had significantly (p < .05) higher levels of socioemotional or behavioral problems (M = 13.68) than toddlers with mothers who did not report IPV physical victimization (M = 8.29). This finding highlights the negative effect of IPV on toddler psychosocial development and supports findings from prior studies that suggest IPV negatively influences child behavior (Chan & Yeung, 2009; Evans et al., 2008; Kitzmann et al., 2003; Wolfe et al., 2003). Also similar to findings from prior research (e.g., Bauer et al., 2013; Whitaker et al., 2006), we found that maternal substance use and major depressive symptoms predict higher socioemotional or behavioral problem scores (p < .05).
When examining the effects of IPV frequency on socioemotional and behavioral problems, analysis revealed IPV frequency was not a predictor of socioemotional and behavioral problems among toddlers exposed to IPV physical victimization; therefore, results did not support our hypothesis. In addition, we found IPV severity is not a significant predictor of socioemotional and behavioral problems among toddlers exposed to IPV physical victimization. This is not surprising, given that post hoc analyses revealed a significant relationship existing between IPV severity and IPV frequency, mothers who reported severe IPV were more likely to report higher IPV frequencies than mothers who did not report severe IPV, F(1, 72) = 20.73, p = .000. Furthermore, of the mothers reporting IPV physical victimization, maternal age, child’s race/ethnicity, and primary maltreatment types are significant predictors of socioemotional and behavior problems. Specifically, a higher risk for socioemotional and behavioral problems existed for toddlers of older mothers and African American toddlers. We are unable to explain this finding. Additional research is needed to understand why maternal age and child race/ethnicity may contribute to toddler psychosocial difficulties. We also found that all primary maltreatment types predicted significantly lower behavior problem scores than physical abuse maltreatment type. This finding may partly be explained by the “double whammy” effect found in prior studies (Kitzmann et al., 2003; Wolfe et al., 2003), which suggests children who experience more than one type of maltreatment, such as physical abuse and IPV, are more likely to exhibit externalizing symptoms and more psychological problems than children who only experience one type of maltreatment such as IPV exposure.
Another aspect of psychosocial development that was examined is social competence. Different than socioemotional and behavioral risk findings, we found no significant relationship between IPV physical victimization and delayed competence. Furthermore, IPV frequency and severity were not predictors of delayed social competence among toddlers with mothers who experienced IPV physical victimization. However, when IPV was the primary child maltreatment type (i.e., the primary reason for child welfare involvement), these toddlers were significantly less likely to have delayed social competence problems than when physical abuse was the primary maltreatment type. Similar to the socioemotional and behavioral problems findings, these findings may also be explained by the “double whammy” effect.
In addition, we found other factors including child’s age predicted delayed social competence among toddlers in IPV-affected families. This finding contradicts past research findings that suggest age is not a significant moderator between IPV exposure and child psychosocial problems (Evans et al., 2008; Kitzmann et al., 2003; Wolfe et al., 2003). However, prior studies have not examined delayed social competence as an outcome or children of younger ages. Additional research is needed to understand the impact IPV has on toddlers’ social competence.
Limitations
Although the current study adds to the extant child welfare literature on IPV and child psychosocial development, it is not without limitations. This study was limited to information available in the NSCAW II; therefore, we were unable to examine the effects of other types of IPV (e.g., emotional and psychological abuse; reciprocal/bidirectional IPV) on toddlers’ psychosocial development. In a related vein, we were confined to using a measure of IPV frequency that is extremely positively skewed. As a result, we were unable to determine the exact frequency of IPV, and estimates may be less accurate. Another limitation of the study is that our analyses only included cross-sectional data, making it difficult to make causal inferences. Although NSCAW II includes multiple waves of data, we were unable to longitudinally examine toddlers’ psychosocial outcomes given the scarce data available for socioemotional and behavioral problems and delayed social competence during 18- and 36-month follow-up. Finally, given toddlers’ psychosocial development was measured based on mothers’ report, bias may exist in this measure; however, there is strong support for reliability and validity of the scale used to measure this outcome. Notwithstanding these limitations, this study highlights the need for child welfare practice, policy, and research that improve the developmental outcomes of toddlers living in homes with IPV.
Practice Implications
Given our findings that IPV physical victimization negatively affects the psychosocial adjustment of toddlers, early intervention and preventions efforts are needed for families affected by IPV. We recommend that prior to making decisions regarding cases with IPV, child welfare workers fully assess IPV-affected families for other factors that may be negatively affecting their child’s development. For example, our findings suggest, in addition to IPV, types of maltreatment and maternal functioning may play a role in toddlers’ developmental outcomes.
Although depressive symptoms were not a significant predictor of socioemotional and behavioral problems among toddlers with mothers who reported IPV physical victimization, when examining the entire sample of mothers (i.e., those with and without IPV physical victimization) we found that maternal depressive symptoms did negatively affect toddlers’ behavioral outcomes. Furthermore, bivariate results revealed that mothers who reported IPV physical victimization were significantly more likely to suffer from depressive symptoms than mothers who did not report IPV physical victimization. Based on these findings, we recommend early intervention services focus on improving maternal mental health. Because IPV exposure and maternal depressive symptoms have been found to collectively predict poor child behavioral outcomes (e.g., Bauer et al., 2013), such services may help mothers process and cope with the stressors associated with IPV, thereby, decreasing their children’s risk for poor psychosocial outcomes. For example, Child–Parent Psychotherapy has been found to enhance mother–toddler interactions, improve maternal depressive symptoms, improve child behavioral challenges, and enhance maternal child rearing attitudes (Gosh Ippen, Noroña, Lieberman, 2014; Lavi, Gard, Hagan, Van Horn, & Lieberman, 2015; Willheim, 2013).
Policy Implications
Results showing IPV negatively affects toddlers’ behavioral outcomes but only when it is not the primary maltreatment type reported to child welfare suggest a compound effect may exist among toddlers exposed to IPV. Toddlers who have been exposed to IPV and experience another primary maltreatment type outside of IPV (e.g., physical aggression) may have worse outcomes than toddlers only exposed to IPV (Kitzmann et al., 2003; Wolfe et al., 2003). In light of this finding, it is imperative that child welfare caseworkers assess for IPV even when it is not the primary maltreatment type. This assessment can provide a more comprehensive picture of developmental risk and protective factors that can assist in appropriately identifying the needs of families involved in child welfare.
Research Implications
There is a critical need for ongoing research focused on toddler development and longitudinal outcomes. Longitudinally examining the effects of IPV will allow researchers to investigate both within- and between-group differences and pinpoint periods during which young toddlers are at greatest risk of psychosocial problems and intervention should occur. In addition, given the limited IPV research examining social competence among young children, additional research is necessary to study this relationship. Future research should also assess the effects of other forms of IPV (i.e., emotional abuse and sexual abuse; and reciprocal/bidirectional IPV). Finally, we recommend researchers measure IPV frequency using more accurate means than permitted with the CTS-2. This may involve examining IPV frequency using qualitative methods or tools such as a calendar to help the women recall separate instances of IPV.
Conclusion
Child welfare agencies can play a vital role in assisting the families of the many children exposed to IPV and at risk of psychosocial problems. This study fills a gap in the literature by focusing on the psychosocial development of a group of children that is sorely understudied by IPV researchers, toddlers. In addition, we used a nationally representative sample and measured IPV based on its frequency and severity. Our overall findings shed light on the negative effect IPV has on the behavioral development of toddlers aged 12 to 18 months. In addition, other factors were found to affect psychosocial functioning of toddlers illustrating the interwoven challenges IPV-affected families may experience. The findings indicate the need for additional examination of the multiple and complex factors that affect toddler psychosocial development. We recommend early intervention services for IPV-affected families with toddlers that focus on not only decreasing risk of IPV but also addressing the multifaceted needs of these families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.