
Abstract
The deleterious effects of sexual abuse (SA) are well documented, as many studies have found that SA can increase the risk for psychiatric disorders. While SA has been examined in multiple samples, no studies have examined the characteristics of SA in individuals with severe mental illnesses (SMI). This study examined the prevalence rate and characterized the nature of SA among individuals with SMI who were under psychiatric care in three different inpatient facilities. Utilizing data from the MacArthur Violence Risk Assessment Study, 1,136 individuals with SMI were assessed for SA histories, psychiatric diagnoses, and other demographics. Nearly half of this sample (n = 511) identified SA histories, with almost half indicating that the person was a stranger or someone outside of the family unit. One third reported SA occurred “too many times to count,” and approximately a third indicated the abuse consisted of intercourse, occurring at a mean age of 11.22 years. Results found that individuals with SA histories were often never married, Caucasian, female, had children, described themselves as psychologically unwell, and were commonly voluntary psychiatric admissions. Those with SA histories had significantly higher psychopathology and lower functioning, and were more likely to be diagnosed with depression but less likely to be substance dependent. Identifying SA characteristics in individuals with SMI is a critical component to successful treatment. Thorough screening and assessment of this common problem can help clinicians identify accompanying issues that may exacerbate SMI symptomology, and improve the prognosis for long-term outcomes.
Keywords
Sexual abuse (SA) is a major social problem both in the United States and abroad. The deleterious effects of SA have been well documented, with research across the past 30 years suggesting that being a victim of SA is associated with many different medical, behavioral, and psychosocial problems (Fergusson, McLeod, & Horwood, 2013; Scott, 1992). Recent meta-analyses reported prevalence rates indicating that 8% of men and 18% to 20% of women worldwide will experience some form of SA during childhood (Pereda, Guilera, Forns, & Gomez-Benito, 2009; Stoltenborgh, van Ijzendoorn, Euser, & Bakermans-Kranenburg, 2011).
SA can have a profound effect on mental health (Hillberg, Giachritsis, & Dixon, 2011), as SA has been found to contribute to the development of many psychological problems in SA survivors (Gil-Rivas, Fiorentine, Anglin, & Taylor, 1997). These can take the form of general emotional disturbances such as anger, sadness, poor self-esteem, and self-destructiveness (Bagley & Shewchuk-Dann, 1991; Gil-Rivas et al., 1997). SA issues can also manifest into substance use, as SA has been found to contribute significantly to the development of substance use disorders (SUD; Browne & Finkelhor, 1986; Gil-Rivas et al., 1997; Turner, Finkelhor, & Ormrod, 2006).
Many studies have found that SA can increase the risk for psychiatric disorders later in life (Fergusson, Boden, & Horwood, 2008; Green et al., 2010; Johnson, Cohen, Brown, Smailes, & Bernstein, 1999; Kendler et al., 2000; Read, 1997; Widom, DuMont, & Czaja, 2007; Widom, Marmorstein, & White, 2006), even after adjusting for confounding variables such as inter-parental violence and childhood physical abuse (Fergusson et al., 2013). Specifically, eating disorders (Hernandez, 1995; Root & Fallon, 1988), depression (Briere & Runtz, 1988; Lindert et al., 2014), anxiety (Fromuth, 1986; Lindert et al., 2014), posttraumatic stress disorder (PTSD; Briere & Runtz, 1987; Molnar, Buka, & Kessler, 2001), and schizophrenia (Berenbaum, Valera, & Kerns, 2003; Read, van Os, Morrison, & Ross, 2005) have all been commonly documented and treated in those with SA issues (Briere & Elliott, 1994; Gil-Rivas et al., 1997; Turner et al., 2006). A prior history of SA has also been found among individuals who have psychiatric disorders co-occurring with SUDs, such as bipolar disorder (Goldstein et al., 2008) and treatment-resistant depression (Goldstein et al., 2009).
Prior studies have examined the prevalence rates of SA in individuals with severe mental illnesses (SMI), with varying results. For example, a study by Mueser et al. (1998) of 275 individuals with SMI found a history of SA in 44.7% of study participants. Similarly, in a study by O’Hare and Sherrer (2009) involving 354 community mental health clients, 41.7% reported one or more episodes of SA. However, a study by Shack, Averill, Kopecky, Krajewski, and Gummattira (2004) of 271 individuals with SMI in an inpatient facility found that only 6.6% of respondents reported a history of SA, while 29.2% reported histories of both SA and physical abuse. All three of these studies examined individuals in one setting while utilizing modest sample sizes, which can limit generalizability. In addition, while O’Hare and Sherrer (2009) and Mueser et al. (1998) both used measures to assess SA, Shack et al. (2004) used a diagnostic interview.
Thus, while the prevalence of SA in individuals with SMI has been investigated (Mueser et al., 1998; O’Hare & Sherrer, 2009; Shack et al., 2004), less is known about the characteristics of SA in this population, who is most likely to be affected, and the impact of SA on mental health outcomes among such individuals. In addition to examining the prevalence rate of SA in individuals with SMI, this study sought to characterize and describe the nature of SA among individuals with SMI who are under direct psychiatric care in inpatient clinical facilities in three different U.S. cities.
Identifying characteristics of SA in individuals with SMI is critical, as individuals with a history of SA have a higher risk of suicide and other self-injurious behaviors, as well as a decreased quality of life (Perez-Fuentes et al., 2013) and higher overall levels of psychological distress (Delany-Brumsey, Joseph, Myers, Ullman, & Wyatt, 2013; Jarvis & Copeland, 1997). In addition, factors such as the severity, frequency, and duration of abuse can impact an individual’s risk for more severe forms of psychopathology (Hillberg et al., 2011) and psychological distress (Molnar et al., 2001). For example, SA involving penetration or SA perpetrated by an individual’s father or stepfather has been associated with greater negative outcomes (Beitchman et al., 1992). Thus, when SA is combined with the difficulties and challenges of SMI, negative symptomology can be amplified.
Considering the fluctuations in findings of prior studies, the problems associated with SA in individuals with SMI needs to be examined further. While studies have found high levels of SA in this population, we do not know what these individuals’ clinical picture looks like. Considering that individuals with SMI are already susceptible to comorbid PTSD (Mueser, Rosenberg, Goodman, & Trumbetta, 2002) and SUDs (Johns, 1997), identifying and treating SA in individuals with SMI are of paramount importance for the successful maintenance of psychiatric symptoms and subsequently improving overall functioning and quality of life.
Method
Participants
This study was conducted by utilizing data from the MacArthur Violence Risk Assessment Study, which has been described in detail elsewhere (Monahan et al., 2001). Participants were recruited from three psychiatric inpatient units in different cities (Worcester, Massachusetts; Pittsburgh, Pennsylvania; and Kansas City, Missouri), with data collection occurring from mid-1992 to late 1995. Participants were eligible for this study if they were (a) between 18 and 40 years old, (b) of Caucasian or African American ethnicity, (c) spoke English as a primary language, (d) carried a civil commitment for no more than 21 days, and (e) had a major diagnosis of a mood disorder (e.g., major depressive disorder, bipolar disorder); psychotic disorder (e.g., schizophrenia, schizoaffective disorder); or drug or alcohol dependence. The mean time between admission to the hospital and being approached by a research interviewer for obtaining informed consent was 4.5 days, while the median length of hospitalization for participants in the study was 9 days.
Across the timetable of the study, a total of 12,873 patients were admitted between the three sites, of which 7,740 patients met the inclusion criteria. The researchers then took a quota sample of 1,695 patients and asked them if they would participate in the study, with 1,136 (67%) agreeing to participate. These participants had a mean age of 30 years (SD = 6) with 25% between 18 and 24 years, and 75% between 25 and 40 years. The participants were mostly male (59%), Caucasian (69%), and single (57%), with almost half (41%) never graduated from high school. A majority of the participants had been previously hospitalized (72%), almost half were involuntarily committed (42%), and more than half (56%) had a chart admission diagnosis of alcohol or drug abuse/dependence.
Measures
Sexual trauma
Respondent experiences of SA were measured during initial assessment via the question, “Did anyone ever bother you sexually or try to have sex with you against your will?” If an incident of SA was confirmed, the participant was asked additional follow-up questions, including (a) the relationship to the perpetrator (including specific family members and friends), (b) the nature of the SA (including intercourse, attempted intercourse, sodomy, inappropriate touching, oral sex, hugging or kissing, and other), (c) the frequency of SA (including once, twice, sometimes, frequently, too many to count), and (d) the age when the abuse occurred. If there was more than one incident of SA, a maximum of two additional incidents were documented using the same follow-up questions. For this study, only participants who answered yes or no (n = 1,100) were included in the analysis, as participants who refused to answer or did not know or remember if abuse had occurred were excluded (n = 36).
Sociodemographics
Information regarding the participant’s age, gender, race, marital status, and number of children were all assessed at study entry and coded. Socioeconomic status (SES) was measured by Hollingshead and Redlich’s (1958) SES Index. This index has been frequently used in both sociological and psychological research, partially because it considers educational attainment and occupational history when it assigns a composite SES score. Higher ratings on the SES Index indicate higher socioeconomic levels. Social network characteristics were measured via the Social Network Inventory (SNI; Estroff & Zimmer, 1994), including the total aggregate number of people in the respondent’s social network and the proportion of both mental health professionals and family members within the network for which the respondent had regular contact. Verbal IQ was measured by the 35-question vocabulary subtest (α = .93) of the Wechsler Adult Intelligence Scale–Revised (WAIS-R; Wechsler, 1999), which has shown good psychometric properties (Reynolds, Willson, & Clark, 1983; Wechsler, 1999).
Psychiatric status
Psychiatric indicators were measured by several methods. Initially, a clinician (PhD or MA/MSW) confirmed the participant’s principal Axis I chart diagnosis by utilizing the Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; American Psychiatric Association, 1987) checklist (Janca & Helzer, 1990). DSM-III-R checklist diagnoses matched the participant’s hospital chart diagnosis 85.7% of the time. During this diagnostic interview, participants were also asked if they felt “psychiatrically unwell,” with yes/no responses dichotomously coded.
To measure the severity of the respondent’s anxiety and depression levels, the Brief Psychiatric Rating Scale (BPRS; Overall & Gorham, 1962) was administered. The BPRS is an 18-item clinical assessment that rates the severity of psychiatric symptoms from the previous week, using a scale from 1 (no symptoms present) to 7 (very severe symptoms). The BPRS has been widely used in social science research, and has been shown to be a reliable and valid assessment with good psychometric properties (Long & Brekke, 1999). Similarly, Global Assessment of Functioning (GAF; Endicott, Spitzer, Fleiss, & Cohen, 1976) scores were also obtained. GAF scores assess an individual’s functioning within society, with higher scores indicating higher levels of functioning.
Regarding variables surrounding the current hospitalization, chart reviews were done to confirm the legal status of the participant’s psychiatric admission (e.g., voluntary or involuntary). Similarly, any record of prior psychiatric hospitalization was indicated by the participant’s self-report and confirmed by chart review.
Substance use
Participants were asked about any existing history of alcohol and drug abuse, which were corroborated by chart reviews and/or collateral interviews with a family member or friend. Alcohol- and drug-related diagnoses (e.g., alcohol abuse, alcohol dependence) were based on the clinician-administered DSM-III-R checklist (Janca & Helzer, 1990), and the presence or absence of a diagnosis was dichotomously coded.
Procedures
Study procedures were fully explained to all recruited patients, and written informed consent was obtained prior to participation in the study. The research was reviewed annually by each participating university’s institutional review board (see Monahan, Appelbaum, Mulvey, Robbins, & Lidz, 1993). Data from participants were collected in two parts. First, participants were interviewed by a research interviewer, who obtained information such as demographics, historical factors, and risk factors in four different domains: personal or dispositional factors, historical or developmental factors, contextual or situational factors, and clinical or symptom factors. Second, participants were also assessed by a research clinician (PhD or MA/MSW) who used the DSM-III-R checklist (Janca & Helzer, 1990) to confirm the chart diagnosis. When disagreements occurred over a patient’s diagnosis, a consultant psychiatrist at each study site resolved the issue. The research clinician also administered several clinical scales that require previous training, such as the WAIS-R (Wechsler, 1999). When possible, participant self-reports were corroborated by chart review of hospital records, collateral informants (nominated by the participant), and police and county records (when written informed consent was obtained).
Results
Characteristics of SA Victims
When examining the overall characteristics of participants who were sexually abused in the study sample (N = 1,136), results indicate that 45% of this sample (n = 511) identified, at minimum, one incident of SA in their lifetime, as perpetrated by at least one abuser, while 3.2% (n = 36) refused to confirm or deny the existence of an SA history (see Table 1). When asked about the identity of the first abuser, almost half (43.4%) indicated that the person was a “stranger” or “various others,” and nearly a third (36.2%) indicated that a family member perpetrated the abuse. When abuse occurred within the family, the father (11.5%) and brother (6.8%) were the most common perpetrators. In reference to the frequency of abuse, one third (33%) of the sample reported that the abuse by the first perpetrator occurred “too many times to count,” and slightly less than a third (30.7%) indicated the incident only occurred “once.” When asked to describe the nature of the SA, almost a third (29.4%) claimed sexual intercourse and almost one fifth (18.2%) reported that they experienced sodomy. The age of the first abusive incident ranged from 1 to 40 years with a mean of 11.22 (SD = 7.3) years. Of the subjects who were sexually abused by at least one perpetrator, 45.8% (n = 234) claimed they were subsequently abused by both a second and a third person during their lifetime, with the mean age of those incidents being 12.68 (SD = 7.8) and 14.08 (SD = 9.97) years of age, respectively.
Characteristics of Sexually Abused Persons (n = 511).

N = 1,136.
Next, we examined characteristics of individuals with SMI who were sexually abused (see Table 2). Results indicated that individuals with a history of SA were more likely to be Caucasian (72%), female (64%), and with a mean age of 29.63 (SD = 6.23) years old at the time of the study, while they were more likely to have been never married (53.1%) and have children (53%). Of these females, a majority were voluntary psychiatric admissions (72.6%) who describe themselves as psychologically unwell (79.3%). In this sample, depression and psychotic disorders were the most common principle diagnoses (45.8% and 18.4%), with comorbid Axis I disorders and SUDs occurring in 38.9% of the sample. Primarily, they were abused by a stranger or someone outside of the family (43.4%), but when abuse occurred within the family, the father (11.5%) and brother (6.8%) were the most common perpetrators.
Comparisons of Sexually Abused and Non-Sexually Abused Persons (n = 1,100).
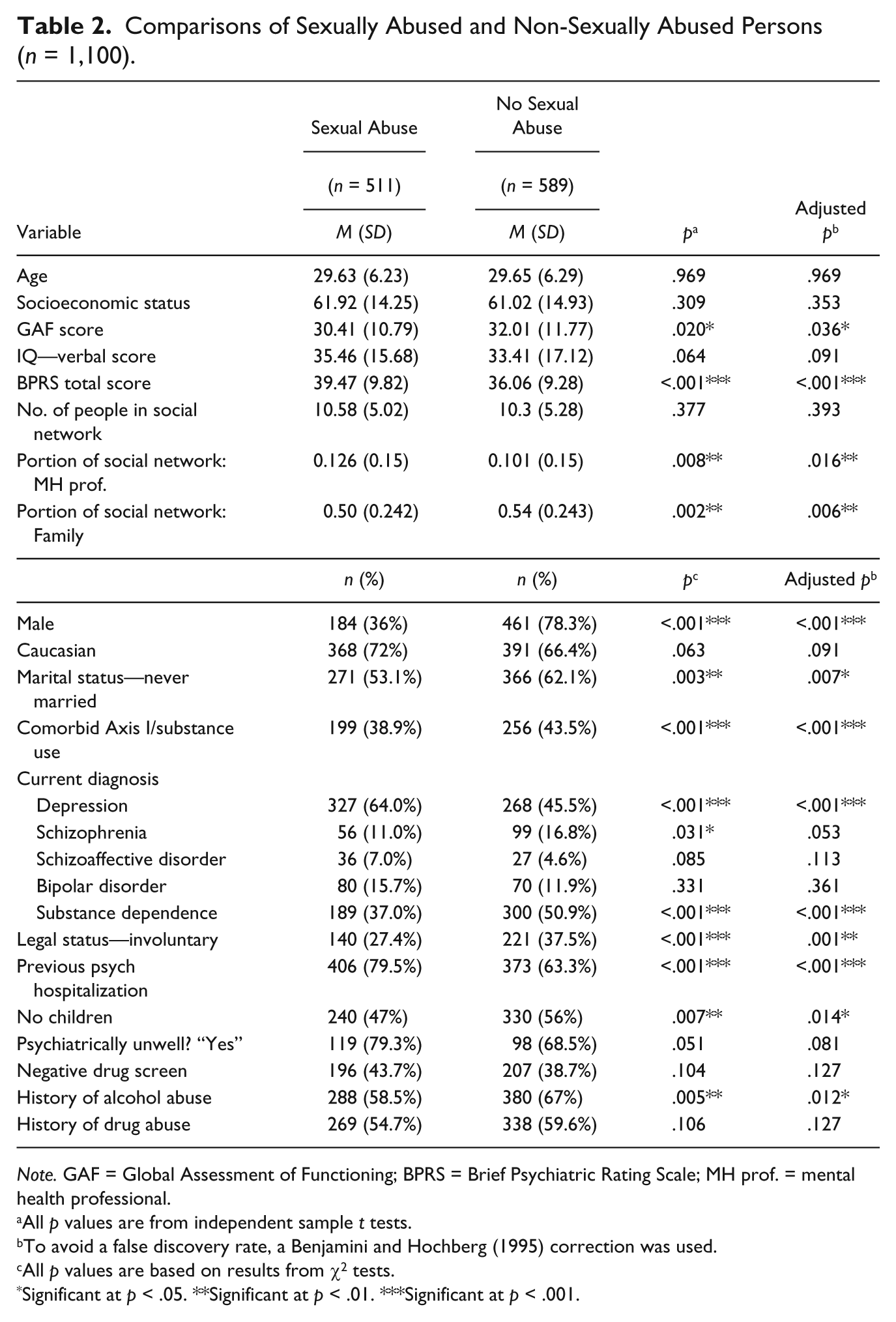
Note. GAF = Global Assessment of Functioning; BPRS = Brief Psychiatric Rating Scale; MH prof. = mental health professional.
All p values are from independent sample t tests.
To avoid a false discovery rate, a Benjamini and Hochberg (1995) correction was used.
All p values are based on results from χ2 tests.
Significant at p < .05. **Significant at p < .01. ***Significant at p < .001.
Comparison of SA Victims Versus Non-SA Victims
When comparing individuals with SA histories versus those who do not have a history of SA (see Table 2), chi-square (χ2) test results reveal no significant differences in terms of race, negative drug screen at admission, a history of drug abuse, or feelings of being psychiatrically unwell (all p > .081). However, there were some significant differences, as those with SA histories were more likely to be female (p < .001), to have been married (p = .007), to have children (p = .014), to have been voluntarily admitted (p = .001), and have a history of psychiatric hospitalization (p < .001). In addition, those with SA histories were also less likely to present with comorbid Axis I and SUD (p < .001), and have a history of alcohol abuse (p = .012). In reference to the current diagnoses of individuals with SA histories versus individuals with no history of SA, individuals with no SA histories diagnosed with schizophrenia were trending toward significance (p = .053), with no significant differences in terms of schizoaffective disorder or bipolar disorder diagnoses (all p > .091). Significant diagnostic differences indicated that those with SA histories were significantly more likely to be currently diagnosed with depression (p < .001), but less likely to have a current diagnosis of substance dependence (p < .001).
When examining group mean scores between individuals with a history of SA versus those with no SA history, independent t test results revealed no significant differences in terms of age, SES, IQ verbal scores, and number of people in their social network (all p > .091). However, individuals with a history of SA had significantly lower GAF (p = .036) scores, higher BPRS (p < .001) scores, and had a higher proportion of mental health professionals (p = .016) yet less family members within their social network (p = .006). All between-group differences reported survived correction for multiple inference testing (Benjamini & Hochberg, 1995), indicating robust discrepancies between those with and without a history of SA.
Discussion
SA is a common issue that results in multiple negative repercussions, yet knowing the impact that SA has on mental health (Hillberg et al., 2011), the characteristics of SA in individuals with SMI have largely been overlooked. Therefore, the purpose of this study was to examine the characteristics of SA in individuals with SMI who were psychiatrically hospitalized and to estimate which individuals may have a history of SA. Several studies have found a relationship between SA histories and later psychiatric diagnoses (Fergusson et al., 2008; Green et al., 2010; Johnson et al., 1999; Kendler et al., 2000; Read, 1997; Widom et al., 2007; Widom et al., 2006). Thus, identifying and treating SA in individuals with SMI are critical for the successful maintenance of psychiatric symptoms and improvement of both functioning and quality of life.
We found that 45% of our sample experienced SA, with almost half of those individuals abused for a second and third time. Initial incidents of SA consisted of intercourse at a mean age of almost 11 years, perpetrated by a stranger or someone outside the family, and occurred “too many times to count.” Individuals with SMI who experienced SA were most frequently never married, female, Caucasians, who have children, and were approximately 30 years old at the time of study. In addition, they were most commonly diagnosed with depression, voluntary admitted, had a history of psychiatric hospitalization, and described themselves as psychologically unwell. Finally, individuals who experienced SA were more likely to have higher levels of psychopathology and decreased functioning, yet less likely to have a history of alcohol abuse, a current diagnosis of substance dependence, and to present with comorbid Axis I and substance use problems.
Thorough and detailed screening for SA among individuals with SMI can help clinicians highlight some of the potential issues that may be seen in practice settings. Studies have already found that when in treatment, individuals with a history of SA entered treatment with more psychiatric and family problems (Branstetter, Bower, Kamien, & Amass, 2008), and scored lower on social and family relations, physical and mental health, and quality of life measures (Oviedo-Joekes et al., 2011). Thus, issues related to SA could exacerbate already existing symptoms in individuals with SMI, making effective screening at treatment entry of paramount importance. In the past, treatment providers have been somewhat reluctant to screen for abuse backgrounds (Briere & Runtz, 1988; Rose, 1991). However, proper screening could help SA survivors deal with the traumatic impact of SA while also concurrently addressing psychiatric symptoms, subsequently improving their overall functioning. This could be achieved through trauma-focused cognitive-behavioral therapy, as it has been shown to be effective with individuals with SA histories (Linden & Zehner, 2007).
The prevalence rate of 45% found in this study is near identical to the rate found in other studies of individuals with SMI. Mueser et al. (1998) discovered that 44.7% of study participants had a history of SA, while O’Hare and Sherrer (2009) found a history of SA in 41.7% of their sample. However, when compared with a similar study of an inpatient population of individuals with SMI, the rate is much higher than the 6.6% for SA and 29.2% for concurrent SA and physical abuse reported in Shack et al. (2004). Of the three studies, O’Hare and Sherrer (2009) had the highest number of participants (N = 354), and considering that those results (41.9%) and the rate found by Mueser et al. (1998) mirror the results we found with 1,100 participants suggests that the prevalence rate found is most likely representative of the SMI population. It should also be noted that a prevalence rate of 45.9% was found among females in the study by Shack et al. (2004), further supporting these findings. Future studies should monitor this prevalence rate to determine if any fluctuations are due to other heterogeneous factors or if it remains constant, especially considering that the prevalence rate among SMI is much higher than the 8% of men and 18% to 20% of women with SA histories in the general population (Pereda et al., 2009; Stoltenborgh et al., 2011).
The results found for characteristics of SA share similarities with other studies of individuals in the general population. In our study, the perpetrator was most commonly identified as non-family members or strangers (43.4%), similar to what Fergusson, Lynskey, and Horwood (1996) found in their study, as 47.7% of perpetrators were non-family members. The frequency of abuse was also similar to other studies, as one incident of abuse was reported by 30.7% in our sample, and 22% in Merrill, Thomsen, Sinclair, Gold, and Milner (2001). When examining the nature of abuse, intercourse was the most common form of perpetrated SA in our study (29.4%), as was the case in Merrill et al. (2001) who reported sexual intercourse among 64% of their sample. In addition, only one perpetrator was found in 54.2% of our respondents, while slightly more (71%) respondents identified one perpetrator in Merrill et al. (2001). These results suggest that the characteristics of SA among individuals with SMI slightly vary in regard to nature of abuse and number of perpetrators, yet are very similar to other characteristics experienced by individuals in the general population.
Studies in the general population as well as other subgroups have commonly found that a larger percentage of individuals who have been sexually abused are female (Boney-McCoy & Finkelhor, 1995; Fergusson et al., 1996; Sedlak, 1997), Caucasian (Merrill et al., 2001), and single (Merrill et al., 2001). Variables such as SES and race were not significantly related to SA, which was also the case in other studies (Fergusson et al., 1996; Ullman, 2007). Thus, it appears that characteristics of SA among individuals with SMI are again somewhat similar to those in the general population.
Despite the many similarities, one unexpected result we observed is that in this sample, individuals who were not sexually abused had higher rates of substance dependence and a higher percentage of histories of both alcohol and drug abuse. Several studies have strongly linked SA to substance use (Amos et al., 2008; Bergen, Martin, Richardson, Allison, & Roeger, 2004; Dube et al., 2005; El-Bassel, Ivanoff, Schilling, Gilbert, & Chen, 1995; Fergusson et al., 2013; Kendler et al., 2000; King et al., 2011; McLaughlin et al., 2010; Meade et al., 2012; Mullen, Martin, Anderson, Romans, & Herbison, 1993; Nelson et al., 2006; Robin, Chester, Rasmussen, Jaranson, & Goldman, 1997; Sartor et al., 2007; Singer, Petchers, & Hussey, 1989). Currently, studies have suggested that childhood SA (CSA) survivors face an increased potential to develop an SUD at any point during life (Afifi, Henriksen, Asmundson, & Sareen, 2012). Thus, future studies need to further test the relationship between SA and substance use among individuals with SMI to deduce if the lower percentage of substance dependence and histories of drug and alcohol abuse found in this study are representative of the true relationship in individuals with SMI.
There are also several limitations to this study. First, as in many other conducted studies, assessment of SA was primarily gauged by participant self-report. Thus, the estimates resulting from this study are most likely floor estimates, as the nature of self-reporting SA tends to be a methodological issue, as distortion of past memories, uncertainty of events, and a reluctance to disclose all have an impact on SA disclosure (Briere & Elliott, 2003). Individuals may be more likely to not remember incidents of abuse in childhood, or they may simply have chosen not to address the memories or classify them as abuse (Cascardi, Mueser, DeGirolomo, & Murrin, 1996; Rosenfeld, Nadelson, & Krieger, 1979). This may be reflected in the question in the MacArthur study that asked if a participant had ever been forced into sex, as 89% of 1,136 participants claimed to have been forced into sex, while only 45% claimed to have been sexually abused. This discrepancy may mean that the actual rates of SA in this sample have been underestimated or that many individuals were further victims of sexual assault later in adulthood, as sexual revictimization is commonly reported in individuals with a history of SA (Classen, Palesh, & Aggarwal, 2005; Messman-Moore & Long, 2000, 2003). These issues surrounding SA disclosure can compound the difficulties of generalizing results to larger populations (Briere & Elliott, 2003).
Second, data used for this analysis were cross-sectional, making it difficult to deduce if any mental health issues were attributable to incidents of SA or to some factor, as SA frequently occurs concurrently with other forms of child maltreatment (Boney-McCoy & Finkelhor, 1995; Finkelhor, Moore, Hamby, & Straus, 1997). It is also important to note that this study does not attempt to suggest causality, as it is not known if SA occurred prior to the onset of SMI, or vice versa. In addition, these cross-sectional data in the MacArthur Violence Risk Assessment Study (Monahan et al., 2001) were collected between 1992 and 1995, and while the MacArthur study has not been replicated, more recent studies of individuals with SMI have been done. However, the MacArthur study was an extremely thorough, rigorous, and comprehensive examination of people with SMI. The data included detailed information on the SA histories of individuals with SMI, something not available in more recent studies.
Overall, we found that 45% of individuals with SMI identified at least one incident of SA in their lifetime, perpetuated by a stranger, consisting of intercourse, and occurring “too many times to count.” Those with SA histories were most commonly Caucasian, female, never married, with children, and almost 30 years old. Individuals who were sexually abused were most commonly diagnosed with depression, voluntary admitted, had previous psychiatric hospitalizations, described themselves as psychologically unwell, and had more problematic functioning and psychopathology when compared with individuals with no history of SA. Thus, it is important to screen for both SA histories in individuals with SMI, in addition to screening for possible comorbid PTSD. Identifying these issues can aid long-term treatment and improve the prognosis for individuals with SMI.
Footnotes
Authors’ Note
National Institutes of Health had no role in the study design, collection, analysis, or interpretation of the data, writing the manuscript, or the decision to submit the article for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by National Institutes of Health (NIH) Grant MH-95783 (SME).