
Abstract
Intimate partner violence (IPV) results in severe and chronic posttraumatic psychological symptoms, maladaptive trauma-related guilt (TRG) and functional impairment for many women. Cognitive Trauma Therapy (CTT) was developed to specifically address empirically identified contributors of distress and functioning difficulties specific to IPV and has been found to be efficacious in treating posttraumatic stress disorder (PTSD) and reducing TRG. The primary aim of this study was to investigate to what extent reductions in TRG contribute to improvements in PTSD and functioning, given evidence of the important role that TRG plays in posttraumatic distress in IPV survivors and the emphasis placed on TRG in CTT. Twenty women with IPV-related chronic and functionally impairing posttraumatic distress were recruited from the community and completed CTT as part of a larger neurobiological study of PTSD. Women experienced statistically and clinically significant improvements in functioning as well as expected reductions in PTSD and TRG with large effect sizes at post-treatment, and improvements were maintained at 3-month follow-up, with no participant meeting full PTSD criteria. Pre- to mid-treatment reductions in TRG predicted post-treatment PTSD and functioning outcomes. These findings support the efficacy of CTT and provide preliminary evidence for the importance of addressing TRG. Dismantling research is indicated to identify the active ingredient(s) of this multi-module treatment.
Prevalence rates of intimate partner violence (IPV) in America have been reported to be as high as 25% (Thompson et al., 2006). A broad range of negative mental health and functioning consequences has also been associated with IPV, including posttraumatic stress disorder (PTSD) and disorders of anxiety, mood, personality, psychosis, substance use, and sleep; increased rates of somatization, dissociation, and suicidality; and diminished assertiveness, self-advocacy, help-seeking, and effective use of available resources (Foa, Cascardi, Zoellner, & Feeny, 2000; Iverson, McLaughlin, et al., 2013; Kubany, Hill, & Owens, 2003, 2004; Laffaye, Kennedy, & Stein, 2003; R. Norman et al., 2010; S. B. Norman, Stein, & Davidson, 2007; Stein, Walker, Hazen, & Forde, 1997). IPV often includes chronic and repeated abuse by a loved one with whom the victim has placed her trust, and involvement of other family members such as children who may be witnesses or victims of abuse themselves and/or be part of the reason women feel compelled to stay in the relationship (Kubany & Watson, 2002). Furthermore, revictimization is common among women who experience IPV (Iverson, Litwack, et al., 2013). Not surprisingly, pathological trauma-related guilt (TRG) has been identified as a primary component of posttraumatic distress in IPV victims (Kubany, Abueg, et al., 1995; Kubany, Bauer, Muraoka, Richard, & Read, 1995; Kubany et al., 2004; Kubany & Watson, 2002; Street et al., 2006).
TRG has been associated with PTSD and other forms of posttraumatic distress (e.g., depression and substance use disorders; Andrews, Brewin, Rose, & Kirk, 2000; Browne, Trim, Myers, & Norman, 2015; Kim, Thibodeau, & Jorgensen, 2011; Kubany, Abueg, et al., 1995; Leskela, Dieperink, & Thuras, 2002), and has been found to predict suicidality above and beyond mental health symptoms in trauma survivors (e.g., Bryan, Morrow, Etienne, & Ray-Sannerud, 2013). Furthermore, TRG may not spontaneously resolve, and there is some evidence that it is resistant to treatment using current gold standard therapies for PTSD (Farnsworth, Drescher, Nieuwsma, Walser, & Currier, 2014; Monson et al., 2006; Nash, Silva, & Litz, 2009; Nishith, Nixon, & Resick, 2005; Owens, Chard, & Cox, 2008).
Although it is not yet clear why TRG has such a prominent role in posttraumatic distress in IPV survivors, we propose the following conceptual model (see S. B. Norman, Wilkins, Myers, & Allard, 2014). We propose that guilt can be an adaptive emotion in that it compels one to assess one’s actions and, if a value was violated, to repair a wrong or change one’s behavior to recommit to living according to said value. If, however, appraisal of the situation leads to the conclusion that no wrongdoing or violation of values was committed, feelings of guilt naturally dissipate. Some trauma contexts can impede this adaptive appraisal process. When a trauma is perpetrated by someone close or upon whom the victim is dependent in some way, the victim may blame himself or herself for the trauma to maintain the important attachment (e.g., Ullman, 2007). This can result in a great deal of distress, which can prompt avoidance of the trauma memories, inhibiting the potential for effectively evaluating and processing the traumatic experience and associated TRG. Avoidance of such traumatic memories has also been shown to be a risk factor for developing and maintaining psychopathology such as PTSD (e.g., Valentiner, Riggs, Foa, & Gershuny, 1996).
A report by the Institute of Medicine (IOM & Committee on Treatment of Posttraumatic Stress Disorder, 2008) concluded that cognitive behavioral therapies should be the front line treatment for PTSD, as these approaches are most likely to lead to sustained recovery from the disorder. The report also noted high rates of attrition and non-remittance and recommended further research elucidating group and individual differences in treatment outcomes and treatment development efforts to address disparities. Cognitive Trauma Therapy (CTT; Kubany & Ralston, 2008; Kubany & Watson, 2002) is a cognitive behavioral therapy that has been designed to target TRG and areas of distress and functional impairment specific to IPV and has been found to significantly reduce PTSD compared with waitlists. CTT includes psychoeducation, skills training, exposure to trauma reminders, and cognitive restructuring, each targeting IPV specific issues. For example, the cognitive restructuring component specifically and systematically targets TRG and other cognitive errors commonly associated with IPV. Skills training focuses on stress management, relaxation, using anger constructively, self-advocacy and empowerment, problem solving, assertiveness, managing unwanted contact with the abuser, and learning about characteristics of potentially abusive and controlling men to avoid revictimization.
In an initial test of CTT in 37 women with PTSD related to IPV, Kubany and colleagues (2003) compared immediate treatment versus waitlisted ethnically and culturally diverse participants and found statistically and clinically significant improvements on all measures of distress (PTSD, depression, guilt, self-esteem). Hedge’s g effect sizes indicated mean scores for treated cases were 1.4 to 3.1 standard deviations below that of the waitlisted, untreated group, controlling for pre-treatment scores. Eighty percent or more of the participants achieved “good end-state” as defined by remission of PTSD diagnosis per the Clinician Administered PTSD Scale (CAPS; Blake et al., 1990) and low depression scores on the Beck Depression Inventory (BDI; Beck, Steer, & Garbin, 1988). CTT was equally effective across ethnic/racial groups. A second clinical trial of CTT with an equally diverse sample of 125 women with PTSD related to IPV obtained similar findings with high mean Hedge’s g effect sizes (CTT vs. waitlist) for the intent-to-treat sample (ranging from 1.2 to 2.0) and a 70% remission rate at 6-month follow-up (Kubany et al., 2004). Improvements were also found in TRG and self-esteem and were maintained at 3-month follow-up, and did not differ between ethnic/racial groups. Women reported high satisfaction with this treatment (Kubany et al., 2004).
These promising outcomes, particularly with regard to PTSD and TRG reduction, warrant more empirical study. More specifically, it has not yet been empirically established that reduction in TRG is integral to improvements in PTSD and functional outcomes, as proposed by the developers of CTT (Kubany et al., 2003, 2004; Kubany & Ralston, 2008; Kubany & Watson, 2002). The current study assessed the role of TRG in the pre- to post-CTT treatment reductions in posttraumatic distress and functioning in a sample of women with PTSD related to IPV taking part in a larger neurobiological study (see Aupperle et al., 2012; Twamley et al., 2009). The primary aim of the current study was to investigate to what extent reductions in TRG contribute to improvements in PTSD and functioning. We hypothesized that reductions in TRG at mid-treatment would significantly predict subsequent reductions in PTSD symptoms and functioning at post-treatment.
Method
Participants
Participants were women who took part in a larger neurobiological study of IPV survivors that was approved by the local university and Veterans Affairs institutional review boards. Women were recruited through ads posted in local print and Internet circulars, and flyers distributed to community IPV agencies. Self-referred women meeting full or partial 1 criteria for PTSD at the intake interview were invited to receive psychotherapy at no cost. Of the 41 participants who were offered psychotherapy, 29 (70.7%) initiated treatment, and 20 of these (69.0%) completed treatment. There were no differences between treatment completers and dropouts on any demographic or pre-treatment symptom or functioning measures, except that treatment completers experienced more distress reliving/re-experiencing symptoms at baseline, and treatment dropouts experienced more impairing avoidance and numbing symptoms at baseline, F(3, 33) = 3.77, Pillais = .26, p < .05.
The sample for the current study consists of the 20 treatment completers. At baseline, participants had full (n = 14) or partial (n = 6) PTSD related to IPV they had experienced within the preceding 5 years but not in the last 30 days. The mean age of participants was 38.70 years (SD = 6.78, range = 28-56), and they had an average of 14.20 years of education (SD = 2.09, range = 11-18). The majority were employed (n = 15, 75.0%), were separated or divorced (n = 14, 70.0%; five were single, and one was married), and did not have children (n = 14, 75.0%; M number of children = 1.89, SD = 1.89, range = 0-8). Sixty percent (n = 12) self-identified as Caucasian, two (10.0%) African American, one (5.0%) Hispanic, one (5.0%) Mexican, and the rest (n = 3, 15.0%) “other.” The average number of abusive relationships per participant was 2 (SD = 0.92, range = 1-4), with the abuse in the last relationship lasting an average of 5.30 years (SD = 1.89, range = 1-7). Many (n = 8, 40.0%) were still in contact with their most recent abusive partner (typically for child custody/care purposes), but none were currently in an abusive relationship (per exclusion criteria). All but two women in this study experienced child abuse in addition to the IPV. All treatment completers were retained until the 3-month follow-up assessment except one woman who moved out of the country after completing the post-treatment assessment.
Measures
Participants completed a demographic questionnaire and the following diagnostic interview and self-report symptom and functioning measures. The CAPS (Blake et al., 1990, 1995) is a standard semi-structured interview used to assess PTSD status and severity. The CAPS assesses each of the 17 items from the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria B, C, and D, and it has demonstrated high levels of internal consistency, good inter-rater reliability, and excellent convergent validity. Participants were asked to discuss their symptoms during the past month as they related to the most traumatic IPV event(s) from their most recent abusive relationship, and interviewers rated the frequency and intensity each on 0 to 4 scales. Severity scores were computed by summing all frequency and intensity ratings, and used interpretively as follows: 0-19 = asymptomatic or having few symptoms, 20-39 = mild or subthreshold, 40-59 moderate or above threshold, 60-79 = severe, and >80 = extreme (Schnurr et al., 2007; Weathers, Keane, & Davidson, 2001). Clinically significant treatment response cutoffs range from a 10-point to a 15-point decrease in the CAPS severity score (Schnurr et al., 2007; Weathers et al., 2001).
Participants were identified as having partial PTSD if they failed to meet either Criterion C or D using the 1/2 scoring method (Weathers et al., 2001), and their severity score was 30 or higher. CAPS interviews were audiotaped and 10% were randomly selected and reliability checked by one of the study assessors other than the one who conducted the assessment throughout the study to monitor the reliability of the interview process using inter-rater reliability assessments (intraclass correlation for CAPS severity = .92). The alpha coefficient for the total measure (severity score) was .73, and .63, .59, and .49 for Criterion B, C, and D subscales, respectively.
The TRG Inventory (TRGI; Kubany et al., 1996) is a 32-item self-report questionnaire designed to measure experiences of guilt associated with the experience of a traumatic event. It includes three scales: (a) Global Guilt (four items) which reflects frequency and intensity of guilt experienced, (b) Distress (six items) which indicates amount of distress experienced when thinking about the guilt inducing event, and (c) Guilt Cognitions (22 items) which captures the extent to which respondents endorse various conclusions about their guilt with relation to the trauma (e.g., “I should have known better,” “I could have prevented what happened”). A series of psychometric studies using diverse samples revealed good internal consistency, test–retest reliability, and construct, criterion, convergent, and discriminant validity (Myers, Wilkins, Allard, & Norman, 2012). In the current study, the alpha coefficient for the total inventory 2 was .97.
The Sheehan Disability Scale (SDS; Sheehan, 1983; Sheehan, Harnett-Sheehan, & Raj, 1996) assesses quality of life across three domains (work, social, and family), using verbal descriptive anchors and visual-spatial scales to rate to what extent symptoms disrupt functioning ranging from 0 (not at all) to 10 (extremely). The three items are summed into a global functional impairment measure that ranges from 0 to 30, with higher scores reflecting greater impairment. It has good reliability and construct validity, and is sensitive to change (Leon, Olfson, Portera, Farber, & Sheehan, 1997). In the current study, the alpha coefficient was .89 (and .95, .77, and .96 for Global Guilt, Distress, and Cognitions subscales, respectively).
Intervention
CTT (Kubany & Ralston, 2008) is a manualized, modular intervention designed to treat PTSD and functional impairment in IPV victims by addressing the specific needs of this population. Each of the 11 modules includes substantial psychoeducation, in-session practices, and homework assignments, and focus on the following topic areas: (a) overview and introduction to self-empowerment, (b) stress and relaxation, (c) PTSD and re-learning (exposure to reminders), (d) learned helplessness and coping strategies, (e) catching and challenging negative self-talk, (f) TRG appraisal (typically administered over two or more sessions), (g) managing anger, (h) assertiveness training, (i) identifying and challenging “shoulds,” (j) identifying potentially abusive men, (k) self-advocacy and final review. The TRG appraisal module consists of cognitive restructuring of incorrect conclusions about how foreseeable and, therefore, preventable IPV events were; the identification of all contributing factors and a re-evaluation of the extent to which the woman was responsible for the IPV; recalling the options available in the context of the IPV and why the option chosen was the best one at the time; defining blame versus responsibility; and distinguishing between wrongdoing and an unwanted outcome.
Participants received an average of 12, 90-min weekly individual sessions (SD = 1.61, range = 10-15). In accordance with the manualized protocol, number of sessions varied depending on the speed with which participants completed each module. Typically, when additional sessions were deemed necessary, it was to address additional sources of TRG. CTT was administered or supervised (live or via recordings) by study authors (C.A., S.N.). Other study therapists were two postdoctoral and one master’s level therapists, each fully trained to adherence as judged through direct observation of at least one complete set of therapy sessions with successful outcome (PTSD remission). Training involved reading the therapy manual, observing recordings of two complete sets of therapy session administered by Dr. Kubany (developer of CTT), and observing one live complete set of therapy sessions administered by study authors (C.A., S.N.), who were previously similarly fully trained. All study therapists received supervision by their trainer throughout the course of treatment with each study participant.
Procedures
Women responding to recruitment flyers were screened for eligibility via telephone after giving verbal informed consent. Eligible callers were scheduled for a series of in person meetings in which full informed consent was obtained, and a diagnostic interview and self-report measures were completed. Participants were excluded if they were currently in an abusive relationship or imminently considering reestablishing the relationship, and for factors known to affect neurocognitive functioning or interfere with functional magnetic resonance imaging (fMRI) scanning as these were components of the larger parent study 3 (i.e., current or substantial history, >5 years, of substance abuse; recent psychotropic medication or steroid use; history of bipolar disorder, schizophrenia, attention deficit disorder, learning disability, >10 min or hospitalized loss of consciousness, or any neurological illness; and <eighth grade English reading ability).
Women who were eligible and met full or partial criteria for PTSD at the initial diagnostic evaluation were invited to continue on to the treatment phase of the study and to complete pre, mid, post, and 3-month follow-up symptom assessments, and a post-treatment fMRI scanning session. Partial PTSD participants were included in the treatment arm of the study and grouped together with full PTSD participants for analyses to form the PTSD-positive group because prior studies have shown that individuals with partial PTSD suffer comparable distress and impairment to those with full PTSD (S. B. Norman et al., 2007; Stein, Walker, Hazen, & Forde, 1997; Zlotnick, Frankling, & Zimmerman, 2002). Subjects were compensated for participating in each assessment component in which they participated, up to US$400 total.
Analyses
A pair of repeated measures ANOVAs tested changes in PTSD (CAPS total score) and functioning (SDS total score) symptoms from pre-treatment to post-treatment. Effect sizes for these were calculated using Cohen’s d adjusted for repeated measures, which removes the correlation between the measures completed at the two time points (Wolf, 1986). A pair of regression analyses was used to predict PTSD and functioning outcomes, respectively, at post-treatment from TRG at mid-treatment, controlling for all prior scores. More specifically, for PTSD, we first predicted CAPS post-treatment total scores from mid-treatment TRGI total scores, after entering pre-treatment CAPS and TRGI scores (to control for baseline variance) and mid-treatment CAPS (to rule out the potential that mid-treatment TRGI is associated with post-treatment CAPS because it is associated with mid-treatment CAPS). We then ran the converse regression analysis predicting post-treatment TRGI scores from mid-treatment CAPS scores, after entering prior CAPS and TRGI scores. We expressly used scores obtained at different time points (e.g., TRG reported at mid-treatment predicting PTSD reported at post-treatment) and tested the converse model to rule out the opposite direction of effect (i.e., change in PTSD at mid-treatment explaining pre- to post-treatment change in TRG). We ran a similar pair of regression analyses to assess the role of change in TRG in functioning (SDS) outcomes. A minimum of two participants per variable has been found to be adequate and that adjusted R2 estimates especially behave well in their estimation of regression coefficients, standard errors, and confidence intervals (Austin & Steyerberg, 2015).
Results
Descriptives and Direct Outcomes
The only difference in baseline measure scores between treatment completers and non-completers, as mentioned above, was in PTSD symptoms. These were controlled for in subsequent analyses. Baseline measure scores did not differ by PTSD diagnostic criteria. Table 1 displays the mean scores for each of the outcome measures at pre, mid, post-treatment, and follow-up assessment times. Pre- to post-treatment reduction in PTSD severity was significant, with a large effect size, and reflected a clinically significant change. Mean decrease in CAPS severity score from pre- to post-treatment was 49.95 (SD = 19.65, range = 4-77), with all but one of the participants decreasing in severity by 15 points or more. From pre-treatment, CAPS severity scores decreased on average by 51% by mid-treatment, 70% by post-treatment, and 74% by follow-up. By mid-treatment, the average CAPS severity score was 33.55, with 25% of participants having achieved total remission (scores less than 20) and 50% falling in the mild or subthreshold range (20-39). These results were maintained or improved at follow-up. At post-treatment, the average CAPS severity score was 19, with 65% of the sample having achieved total remission, 15% falling in the mild or subthreshold range, and the remaining (20%) in the moderate range (40-59). At follow-up, participants had an average CAPS severity score of 17.84, with 63% still in remission, 32% falling in the mild range, and one (5%) having a severe score. Pre- to post-treatment improvements in TRG and functioning with large effect sizes were also observed.
PTSD, Trauma-Related Guilt, and Functioning Scores, and Pre- to Post-treatment ANOVA Results (n = 20).
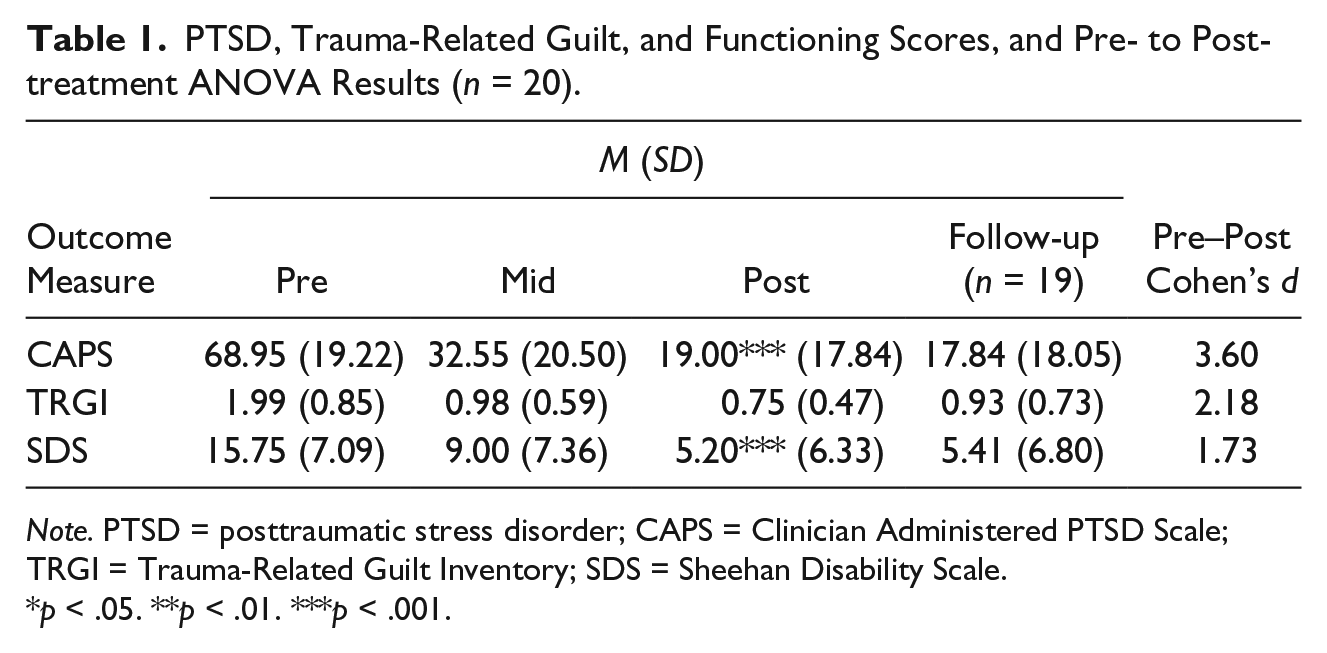
Note. PTSD = posttraumatic stress disorder; CAPS = Clinician Administered PTSD Scale; TRGI = Trauma-Related Guilt Inventory; SDS = Sheehan Disability Scale.
p < .05. **p < .01. ***p < .001.
Role of TRG in Outcomes
Post-treatment CAPS total scores were positively correlated with TRGI totals at each of the time points, and mid-treatment TRGI was positively correlated with mid-treatment CAPS (see Table 2). The only correlation that was .70 or higher was between the hypothesized predictor (mid-treatment TRGI) and predicted (post-treatment PTSD [CAPS] severity) variables. Therefore, it was appropriate to include (control for) each of these variables in the hypothesis testing regression analyses related to PTSD. Table 3 summarizes the results from the pair of regression analyses used to assess the role of pre- to mid-treatment reductions in TRG in PTSD outcomes at posttest. A significant multiple regression analysis revealed that of all variables entered simultaneously (pre-treatment TRGI and CAPS, and mid-treatment TRGI), only mid-treatment TRGI total scores predicted post-treatment CAPS total scores. The converse regression analysis, predicting post-treatment TRG from PTSD, measured at mid-treatment (controlling for TRGI and CAPS at all other prior and concurrent time points) was not significant.
Bivariate Correlations of TRGI and CAPS Total Scores at All Time Points (n = 20).
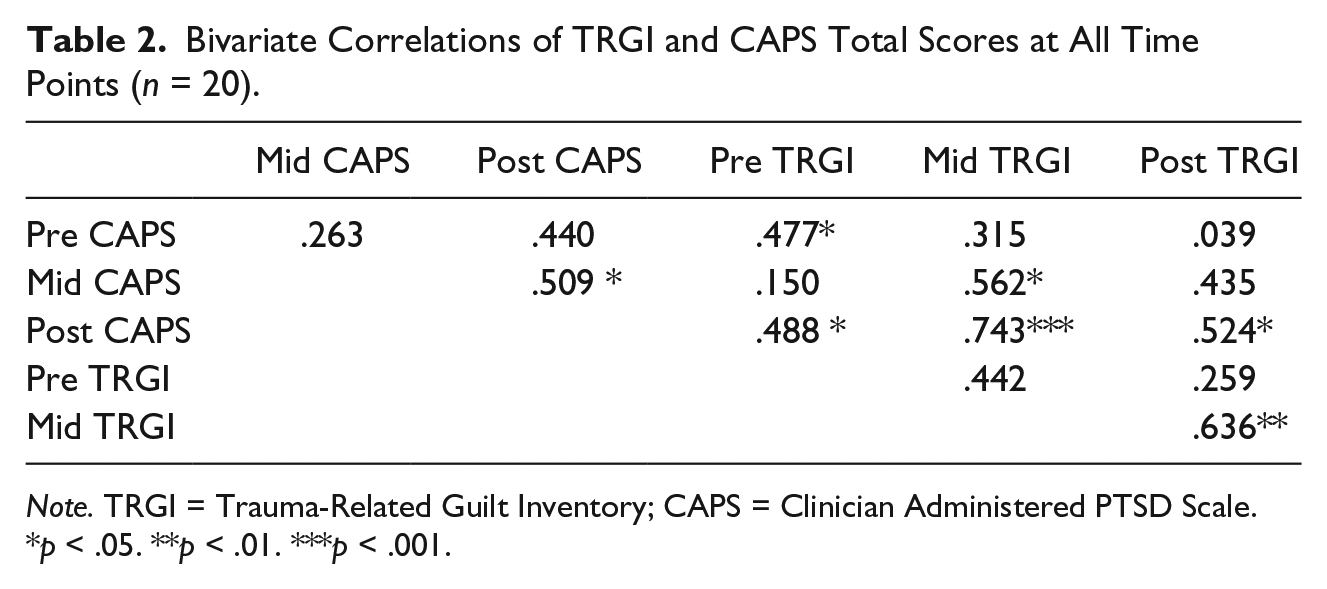
Note. TRGI = Trauma-Related Guilt Inventory; CAPS = Clinician Administered PTSD Scale.
p < .05. **p < .01. ***p < .001.
Summary of Multiple Regression Analyses Examining Trauma-Related Guilt and PTSD (n = 19).
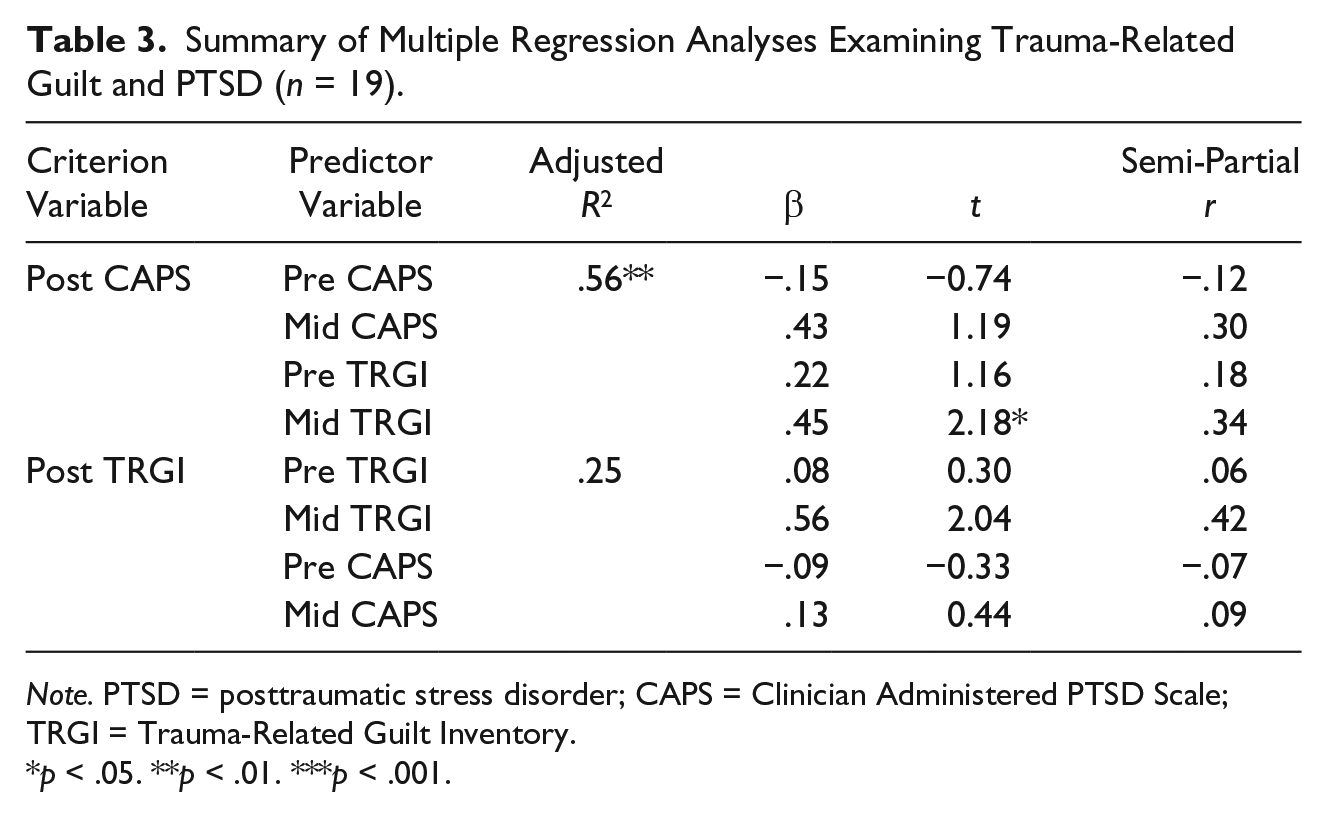
Note. PTSD = posttraumatic stress disorder; CAPS = Clinician Administered PTSD Scale; TRGI = Trauma-Related Guilt Inventory.
p < .05. **p < .01. ***p < .001.
Post-treatment SDS total scores were positively correlated with TRGI totals at each of the time points, and mid-treatment TRGI was positively correlated with mid-treatment CAPS (see Table 4). The only correlation that approached .70 was between the hypothesized predictor (mid-treatment TRGI) and predicted (post-treatment functioning [SDS]) variables. Therefore, it was appropriate to include (control for) each of these variables in the hypothesis testing regression analyses related to SDS. Table 5 summarizes the pair of regression analyses testing the role of pre- to mid-treatment change in TRG on functioning outcome. A significant model emerged whereby mid-treatment TRGI total scores uniquely predicted post-treatment SDS total scores when entered simultaneously with all other variables. Pre- and mid-treatment SDS scores also were found to uniquely predict post-treatment SDS score in this model. The converse model, predicting post-treatment TRGI from mid-treatment SDS, was not significant.
Bivariate Correlations of TRGI and SDS Total Scores at All Time Points (n = 20).
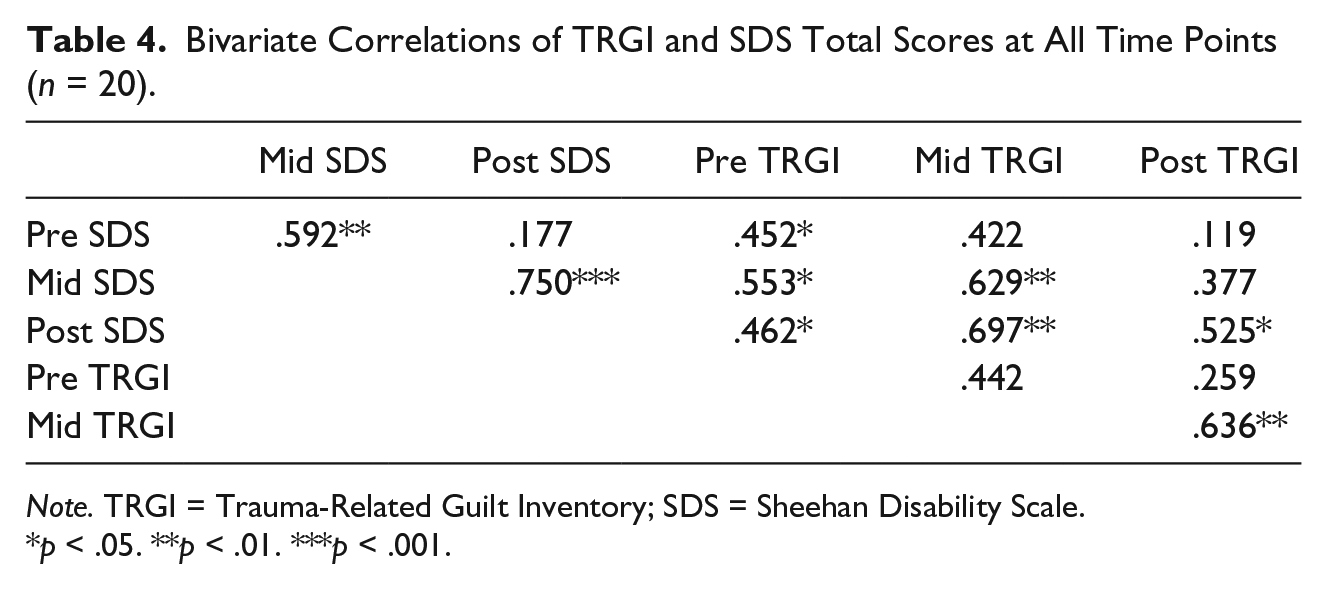
Note. TRGI = Trauma-Related Guilt Inventory; SDS = Sheehan Disability Scale.
p < .05. **p < .01. ***p < .001.
Summary of Multiple Regression Analyses Examining Trauma-Related Guilt and Functioning (n = 19).

Note. SDS = Sheehan Disability Scale; TRGI = Trauma-Related Guilt Inventory.
p < .05. **p < .01. ***p < .001.
Discussion
As expected from prior randomized trials of CTT, improvements in PTSD and functioning from pre- to post-treatment were robust in this sample and were maintained at the 3-month follow-up, and outcomes were comparable with those reported in studies of the most effective treatments of PTSD. A meta-analysis of PTSD clinical trials (Bradley, Greene, Russ, Dutra, & Westen, 2005) revealed an average PTSD remission rate of 67% for treatment completers at post-treatment, which was very nearly obtained in the current study (65%). The Bradley meta-analysis also revealed a mean pre- to post-treatment PTSD symptom reduction effect size of 1.43 (SD = 0.67) across all studies, while participants in the current study obtained a pre- to post-treatment effect size of 3.60. The effect size for the pre- to post-treatment change in TRGI obtained in the current study (2.18) approached the mean effect size of pre- to post-treatment reductions in TRGI scores obtained in the two previous clinical trials of CTT (Hedge’s g converted to Cohen’s d = 2.54, SD = 0.46; Kubany et al., 2003, 2004). Comparatively, CPT obtained an effect size of .87 for the significant reduction associated with the Distress scale of the TRGI compared with a waitlist condition (Monson et al., 2006). Only a handful of studies have included functioning as an outcome of PTSD treatment. One study reported an effect size of 0.18 for pre- to post-treatment improvement in quality of life (using the Quality of Life Index; Frisch, Cornell, Villanueva, & Retzlaff, 1992) and .47 in mental health functioning (using the Short Form-36; Ware & Sherbourne, 1992) among women undergoing Prolonged Exposure (PE; Schnurr et al., 2007). In comparison, pre- to post-treatment improvement in functioning using the SDS in our study obtained an effect size of 1.74. Together, these findings provide further support for the efficacy of CTT in reducing IPV-related PTSD and TRG, and preliminary evidence for improving functioning. The large pre- to post-treatment outcome effects in the current sample are notable given that almost all participants reported histories of other interpersonal trauma in addition to the IPV that was the target of the treatment.
The current study also provides preliminary evidence that reductions in TRG predict improvements in PTSD and functioning. A pair of multiple regression analyses supported our hypotheses that reductions in TRG at mid-treatment would predict reductions in PTSD at post-treatment. That the independent variable (TRGI at mid-treatment) preceded in time the dependent variable (post-treatment CAPS) provides support for the hypothesized directional link from the independent variable to the dependent variable. Furthermore, post-treatment TRG did not predict mid-treatment PTSD severity, so that no support was found of a potential reverse effect. Similar regression analyses supported our hypotheses that reductions in TRG at mid-treatment would predict improvements in functioning at post-treatment. This set of results suggests the link between TRG and PTSD and functioning is in the hypothesized direction (i.e., that successfully reducing TRG contributes to the reduction in PTSD severity and improvement in functioning, and not the other way around). Causality, of course, cannot be ascertained by these findings. Together with previous findings, this study suggest that PTSD interventions that target unique characteristics of particular trauma groups, like CTT, and the potential mechanistic role of TRG in recovery from some trauma, merit further study.
These findings support the importance of targeting TRG in the treatment of PTSD related to IPV and provide further evidence that CTT is a treatment model that can do so efficaciously. A comparison of CTT with other PTSD treatments is needed to determine relative efficacy in women who have experienced IPV, given the higher than average effect sizes obtained for CTT in this and prior studies. In addition, a dismantling study of CTT is warranted to evaluate the necessity of the TRG module, which is purported to be the key mechanism of the treatment (Kubany et al., 2003, 2004; Kubany & Ralston, 2008; Kubany & Watson, 2002). Because TRG is associated with PTSD caused by other types of trauma as well (e.g., Browne et al., 2015), targeting TRG more explicitly and systematically may enhance the effectiveness of treatments in other populations. Although current gold standard treatments for PTSD are very effective, there remains room for improvement as up to 50% of people who start one of the evidence-based treatments do not experience remission (Bradley et al., 2005; IOM & Committee on Treatment of Posttraumatic Stress Disorder, 2008). Therefore, identifying promising leverage points for change, such as TRG, and developing and testing interventions targeting these, are critical to improving outcomes. Indeed, guilt and shame are features of other psychopathology (e.g., Browne et al., 2015) so that targeting these may be a viable transdiagnostic intervention.
The current study is the first to assess the role of changes in TRG in treatment outcomes and contributes important information that can inform efforts to improve treatments for posttraumatic distress. More research is needed in this area, however, to replicate and expand upon these findings. Limitations of the current study include the lack of a control condition, which means that potential confounding variables could not be controlled, a traditional mediation analysis could not be conducted, and symptom and functioning improvements cannot be causally attributed to the treatment. The relatively small sample size limited our ability to control for other potentially important predictors of outcome and the power to detect significance. Finally, the results may only be generalizable to women who have PTSD related to IPV and who do not have serious comorbid disorders (i.e., bipolar, psychotic, or active substance use disorders). And of course, findings may not be generalizable to all survivors of IPV given the potential sources of heterogeneity that could not be controlled for due to the small sample size.
A strength of this study, nonetheless, is the sample’s diversity in age, ethnicity, and other demographic factors, allowing for some generalizability within this trauma group. In addition, results were not confounded by the use of psychotropic medications or other concurrent treatment, as this was an exclusion criterion for entry into the study. Other strengths include assessment of functioning in addition to PTSD.
In summary, the findings from the current investigation provide support for targeting TRG in the treatment of PTSD in survivors of IPV, and suggest the need for further research on the role of TRG in the development of PTSD and other psychopathology and their treatments in other populations. These results need to be replicated in larger samples, and treatment outcomes need to be compared between different therapies and between different trauma samples. There may be different reasons that TRG develops following different types of trauma, and therefore, interventions targeting TRG may need to differ. To this end, further research is needed to develop and test models of the role of TRG in the development of posttraumatic distress in different trauma populations.
Footnotes
Acknowledgements
The authors acknowledge the invaluable contributions of the women who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based on work funded by a Department of Veterans Affairs Merit Review Award (Principal Investigator: Stein), a NIAAA K23 award (Principal Investigator: Norman), and a Career Development Award (Principal Investigator: Thorp), and is supported with resources and the use of facilities at the VA San Diego Healthcare System and University of California San Diego School of Medicine.