
Abstract
Home care professionals are well positioned to witness or prevent older adult mistreatment in the community. Screening efforts are important because most victims will not easily come forth. Two Canadian local community service centers implemented a systematic screening procedure within preexisting individual clinical supervision sessions to support social workers and improve detection of mistreatment. The aim of this pilot project was to assess fidelity, acceptability, and feasibility of the new procedure. Qualitative data was collected using individual interviews with two clinical supervisors, one focus group with eight social workers and content transcribed from 15 supervision sessions. It was estimated that 400 clients were screened for older adult mistreatment using this new procedure. Results showed the procedure was judged acceptable because it sensitized social workers to risk factors, gave them time to reflect upon and discuss probable cases with their clinical supervisor. Nonetheless, participants did not use the designated statistical code in the new procedure to document mistreatment situations. Feasibility was mainly challenged by the fact that screening for older adult mistreatment competes with other organizational priorities. Future initiatives must develop strategies to counteract those barriers.
Introduction
The World Health Organization (WHO) defines older adult mistreatment as “a single, or repeated acts, or lack of appropriate action, occurring within any relationship where there is an expectation of trust which causes harm or distress to an older person” (Action on Elder Abuse, 1995; WHO, 2002, p. 3). People that mistreat can be family members (e.g., spouse, children, in-laws, grandchildren), friends, health care professionals, or hired help (e.g., paid caregivers). One of the key points in this definition is that older adult mistreatment is contextualized within a trusting relationship. Often, older adults do not report the situation; some downplay it while others deny it or try to hide it.
In the context of older adult mistreatment, primary prevention interventions target risk factors in an attempt to reduce the risk of occurrence, and secondary prevention efforts aim to identify older adult mistreatment situations as early as possible to avoid escalation and further harm to the older adult (De Donder, De Witte, Brosens, Dierckx, & Verté, 2015). Screening procedures are based on the fact that the person that is being mistreated will not easily come forth and that efforts need to be made by social and health care professionals to identify risks and warning signs. Screening for older adult mistreatment is important because in a systematic review, Dong (2015) noted that the prevalence of older adult mistreatment, in North and South America, can range from 10% in adults without cognitive deficits to 47% in those with dementia. In addition, older adult mistreatment has been associated not only with psychosocial distress, but also with greater morbidity and mortality (Dong, 2015).
Screening requires the collection and analysis of data by social and health care professionals, if possible with the help of colleagues, to document probable mistreatment situations (Fulmer, Guadagno, Dyer, & Connolly, 2004). When mistreatment is suspected, tools can be used to assess the common signs and symptoms (Bass, Anetzberger, Ejaz, & Nagpaul, 2001). For some situations, behavioral manifestations are directly observed or are reported by witnesses (i.e., a family member, a friend, a neighbor, a legal guardian, a paid caregiver, or a clinician, etc.; Bass et al., 2001).
Home care professionals are well positioned to witness or prevent older adult mistreatment in the community by identifying potentially hazardous environments, trying to resolve underlying issues, providing additional services, and involving other family members (Dong, 2013). Studies have shown that the majority of mistreated older adults are already clients of health and social services (Sandmoe & Kirkevold, 2011). However, older adult mistreatment screening is not necessarily a well-implemented practice within social and health care establishments. Perel-Levin (2008) stated that “while screening in pediatric settings is widely accepted, equivalent practice focusing on the adult population has not been adopted widely and has never been evaluated properly” (p. 2). Anthony, Lehning, Austin, and Peck (2009) noted that validated screening instruments for older adult mistreatment exist, but they are not being used in any setting.
Recent literature has started shedding some light on the reasons for the poor implementation of screening procedures within social and health care context. In a study by Schmeidel et al. (2012), social workers explained that they relied on nurses and physicians to detect cases. However, in the same study, nurses stated that older adult mistreatment is uncommon, that it was not their job to assess for potential mistreatment, and physicians reported that they had other care priorities and that maintaining a relationship of trust is more important. Both nurses and physicians also noted the importance of time constraints (Schmeidel et al., 2012). These results indicate that health care professionals are not fully assuming responsibility for older adult mistreatment detection.
In a systematic review about the decision-making process of social and health care professionals with regards to older adult mistreatment, Killick and Taylor (2009) noted that situations where victims are not collaborating or do not want to report put social and health care professionals in an uncomfortable ethical dilemma. In addition, health care professionals’ confidence level with regard to their ability to intervene efficiently plays an important part in the decision to act upon a probable mistreatment situation. Additional factors are the available resources within the organization, guidelines, and having other colleagues to discuss the case (Killick & Taylor, 2009).
Training is required to improve screening for older adult mistreatment within social and health care establishments (Bergeron, 1999; Imbody & Vandsburger, 2011). Nonetheless, increasing knowledge is apparently not sufficient. According to Cooper, Selwood, and Livingston (2009), training increases knowledge and reporting of identified mistreatment in known cases but not necessarily identification of new cases. An approach combining training and clinical supervision might be the way to improve screening and ultimately detection. Social and health care professionals need to interact with other professionals to facilitate their decision-making process (Imbody & Vandsburger, 2011) because screening involves analysis and identification of psychosocial, medical, and legal aspects. Even when using standardized tools, assessment skills and knowledge levels may differ between professionals and influence their interpretation of questions and results (Anthony et al., 2009).
Clinical supervision could help to improve screening by maximizing, for example, the data collection process (Sandmoe & Kirkevold, 2011). Milne (2007) stated that clinical supervision is
the formal provision by senior/qualified health practitioners of an intensive relationship-based education and training that is case-focused and which supports, directs and guides the work of colleagues. (p. 440)
According to this author, three functions are attributed to clinical supervision: (a) quality control, (b) maintaining and facilitating the supervisees’ competence and capability, and (c) helping supervisees’ to work effectively. Cooper et al. (2009) mentioned that the complexity and the subjectivity involved in screening for older adult mistreatment calls for the development and evaluation of new strategies aiming to better support social and health care professionals.
The purpose of this pilot study was to evaluate the implementation process of a new systematic screening procedure for older adult mistreatment within preexisting individual clinical supervision. In this study, providing clinical supervision is regarded as an implementation strategy to improve support for social workers and identification of probable cases in the community. More specifically, the study aimed at (a) evaluating the level of fidelity to the planned procedure, (b) testing the acceptability of the new procedure for participating clinical supervisors and social workers, and (c) to examine the feasibility of implementing a systematic screening procedure for older adult mistreatment within individual clinical supervision in home care.
Method
The evaluation of the implementation was performed using a qualitative research design to not only capture the content of the actual clinical supervision sessions but also the experience of clinical supervisors and social workers.
Setting
In Canada, health and social care are under provincial jurisdiction and the range of services differs from province to province. In Quebec, local community service centers (CLSCs) offer frontline health and social services, including home care. The main purpose of home care is to provide interdisciplinary frontline services to maintain or improve people’s ability to remain at home safely according to their wishes and the feasibility to do so. Services available include professional services (e.g., medical, nursing, social work, etc.), home support (e.g., personal care, domestic help, etc.), and technical support (e.g., equipment, technical aids; Ministère de la santé et des services sociaux, 2003). Although there may be some variation depending on the region, generally, request for home care services for older adults are processed by a centralized intake. Eligible clients are then put on a wait list based on level of priority that determines the order in which they will be seen by an evaluation team responsible for making recommendations for a transfer to the appropriate division for case management. Individuals are admissible for these services regardless of socioeconomic status, race, ethnicity, language, nationality, sex, gender identity, sexual orientation, religion, and age. With consent of the client, family caregivers and clients are involved in the evaluation process and the development of the intervention plan. Social workers can have a more general role such as making global evaluations and providing case management services or have a more specialized role by providing in-depth psychosocial evaluations and support around the loss of autonomy and bereavement.
To better support social workers, two CLSCs from the Montreal area implemented, in their home care division, a systematic screening procedure within individual clinical supervision. The two CLSCs offer services to more than 120,000 inhabitants (Health and Social Service Agency of Montreal, 2014). In Quebec, there is no mandatory reporting or adult protective services addressing older adult mistreatment situations. Health and social services are often responsible for the management of older adult mistreatment situations. In addition to the older adult who is mistreated, the person who mistreats and any other people directly involved and affected by the situation, if they consent, can be referred to specialized resources depending on the mistreatment situation such as medical professionals, legal resources, community resources, and/or specialized help lines. Legal recourse include lawyers specialized in elder law, notaries, the office of the Public Curator who is responsible for the protection of people who are deemed inapt, and the Human Rights Commission whose mandate is to protect people’s rights and freedom from exploitation under Article 48 of the charter of rights of Quebec. Other measures include law enforcement, criminal or civil proceedings, as well as community resources that offer accompaniment and advocacy.
Systematic Screening Procedure for Older Adult Mistreatment Within Individual Clinical Supervision
Providing clinical supervision means providing clinicians with ongoing supervision focusing on the new procedure as well as training clinical supervisors in regard to this procedure (Powell et al., 2015). The clinical supervisors received 1-hr training by the second and third authors on the development and use of a screening tool within the context of individual clinical supervision 1 month prior to the training of the social workers. Social workers received training by the supervisors in a preexisting staff meeting. Table 1 presents the logical model of the systematic screening procedure that comprises two main components: (a) caseload evaluation by each social worker and (b) weekly 30-min individual supervision meetings with their clinical supervisor. Supervision meetings were already part of practice prior to the implementation of the systematic screening procedure. The supervision was, however, not purely clinical, and within a 30-min period per week, the supervisor was expected to first ensure that administrative requirements were being met. The remaining time was allocated to clinical issues within a whole caseload. With the new systematic screening procedure, the clinical supervisors discussed the following issues with each participating social worker:
Components of the Systematic Screening Procedure for Older Adult Mistreatment Within Individual Clinical Supervision.
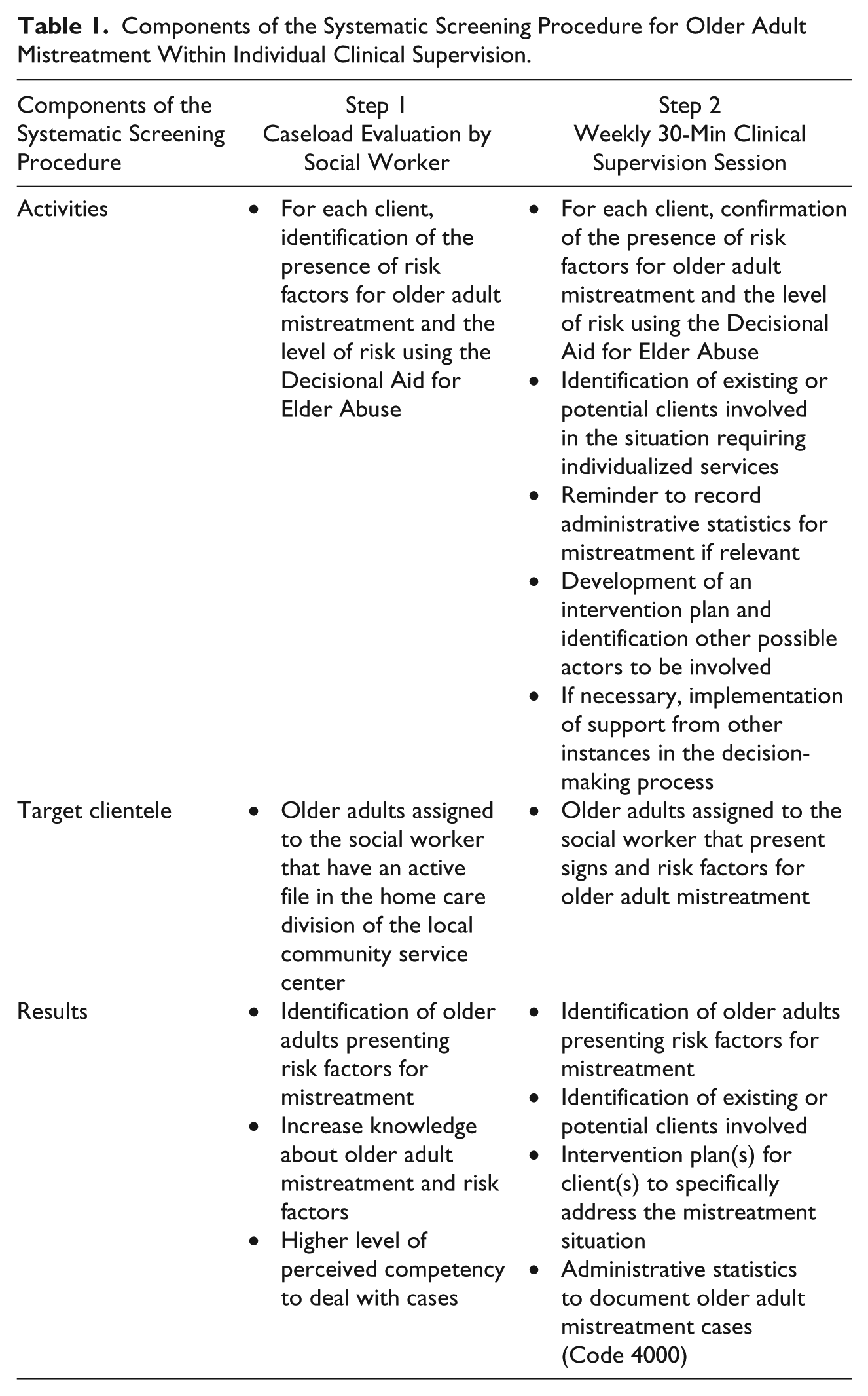
Are there any clients that present risk factors for older adult mistreatment within your caseload?
If the answer is yes, what was their level of risk? Which actions must be undertaken and by which actors?
Is there more than one client in the possible mistreatment situation? (e.g., Is there a spouse or another older adult that would also be at risk of mistreatment situation).
If a mistreatment situation is identified, the clinical supervisor reminded the social worker to administratively document older adult mistreatment cases using a designated statistical code (Code 4000).
The systematic procedure included a screening tool (available at the following address: http://www.prendreencharge.com/en/tools-for-professionals/, developed within the “Taking Charge Initiative: Elder Abuse Is a Global Issue” project funded by the Government of Canada’s New Horizons for Seniors Program). This tool was developed by a team specialized in older adult mistreatment including a researcher, a clinical specialist (second author), and a social worker/research assistant (third author). The content of this tool was first validated and field tested in 2011 by social and health care professionals from three different contexts: elder abuse helpline, intake, and home care. The present pilot study aimed at supporting the integration of this screening tool within individual clinical supervision. This tool includes a Decisional Aid for Elder Abuse covering screening and risk assessment to help health care professionals process relevant information according to risks and legal responsibilities. It provides a visual template for processing different scenarios in terms of urgency and the capacity of the older adult to consent. Optional annexes are also provided to further support their analysis and interventions including definitions of older adult mistreatment, a decision-aid for intervening with vulnerable older adults, an assessment tool for suicide risks, and a list of specialized resources for older adult mistreatment. Social workers had to evaluate their whole caseload using this tool prior to the individual clinical supervision meetings.
For complex cases, clinical supervisors and social workers have access to older adult mistreatment specialized support structures: clinical team meetings, access to a professional multi-sectorial consultation team, and consultation with an in-house expert practitioner (coordinator of leading practices for the prevention of older adult mistreatment). Complex cases refer to situations that require, at the level of evaluation and/intervention, involvement of various disciplines and/or sectors. For example, financial exploitation of a person with questionable cognitive capacity that has psychological and physical consequences require involvement by health, financial, and legal professionals, as well as law enforcement, public curator, or Human Rights Commission.
Participants
The pilot project was approved by the director of home care of the two CLSC as well as the only two clinical supervisors (one from each CLSC) in charge of home care social workers. Home care social workers were recruited through a 30-min presentation of the project by the first three authors. During that meeting, 30 social workers were given a written invitation as well as the consent form that could be signed right away or sent to the first author by email or internal mail at a later time. Overall, eight social workers agreed to participate in the data collection. All participants had previously received training on screening and intervention for older adult mistreatment as it was part of the continued professional development program provided by the employer within the context of a provincial government initiative to counter older adult mistreatment. This training includes information on prevalence, causes, definition, risk factors, as well as advantages of screening and early intervention to minimize the impact or consequences of older adult mistreatment. This training also highlighted systematic use of tools as well as recourse to specialized resources. To facilitate recruitment of participants, demographic information was not collected due to the perceived sensitivity of the topic and risk for confidentiality. This project was reviewed by the research ethics committee associated with the health establishments involved and was categorized as a program evaluation.
Data Collection
The choice of implementation outcomes is based on the taxonomy developed by Proctor et al. (2011). First, fidelity was evaluated to describe the degree to which the new systematic screening procedure was implemented as it was intended originally. Second, acceptability reflects the perception of clinical supervisors and social workers with regard to their satisfaction with the new procedure. Third, feasibility refers to the extent to which this new procedure can be successfully perpetuated within home care.
Data collection was performed over a 3-month period, from April to June 2013. The participants had received formal training in older adult mistreatment months prior to the introduction of the systematic procedure and were already involved in non-structured screening in their practice. The participants used the new systematic screening procedure for older adult mistreatment for 6 weeks before data collection, to have time to integrate it into their practice. A 6-weeks’ time lapse was deemed sufficient to evaluate their caseload and have at least four clinical supervision sessions using the new procedure. Three data collection methods were used: (a) individual interviews with clinical supervisors (n = 2), (b) a focus group with social workers (n = 8), and (c) digital audio recordings of two clinical supervision sessions for each participating social worker (n = 15). Triangulation of data collected from different sources aims to determine the consistency of a finding (Yin, 2014).
Fidelity was mainly assessed using the audio recordings of clinical supervision sessions. To avoid the intrusion of researchers, clinical supervisors were responsible to record the clinical supervision sessions with digital recording devices provided by the research team. In the 30-min supervision meetings, on average, 8 min were devoted to the new systematic screening procedure.
Individual interviews with two clinical supervisors and a focus group with the social workers were used to evaluate acceptability and feasibility of the new procedure as well as provide additional information about fidelity. One interviewer specialized in older adult mistreatment support for the population and professionals conducted individual interviews with the clinical supervisors that lasted an average of 20 min. This interviewer became an observer during the focus group to take notes and validate the information collected with the participants. The focus group lasted 56 min and was conducted by the last author; a research professional specialized in qualitative research. The following questions were used: (a) Overall, how was the experience of using the new systematic screening procedure? (b) Are there elements that have hindered its use as part of your practice? (c) Are there elements that have facilitated its use as part of your practice? (d) Are there any changes that you recommend to the screening procedure? and (e) Do you have any other comments regarding the screening procedure?
Data Analysis
All data were transcribed by a person specialized in this type of work and checked by the first author who also analyzed all the interview transcripts using the Miles, Huberman, and Saldaña (2013) analytical method. Data analysis focused on describing the fidelity, acceptability, and feasibility of the new systematic screening procedure. Two processes were used to analyze the data: codification and matrix building. First, codes were used to label units of text (words, sentences, paragraphs) that encompass a distinct meaning. The coding list emerged from the data. Second, matrices were used to further analyze patterns and relationships between codes and compare sources of data. Data analysis was validated by the second and fourth authors.
Results
Data presented in this section integrated information from the individual interviews with two clinical supervisors, the focus group with eight social workers, as well as the transcribed content of 15 supervision sessions. Results are presented according to the three main outcomes related to the implementation process: fidelity, acceptability, and feasibility.
Fidelity
This part of the results examines the degree to which this new procedure was implemented as it was intended. The planned systematic screening procedure comprises two main components: (a) evaluation of the caseload by the social workers using the screening tool and (b) 30-min weekly individual supervision meetings with the clinical supervisor.
As planned in the screening procedure, the social workers reviewed their caseload using the screening tool prior to the supervision session with the clinical supervisor.
Basically, before we met, they were to look at, you know, review their cases in their head, or take a look at the list and apply their screening tool. I mean, you can’t expect them to do it with 65 clients, which most of the workers have. But as I said, most of the clients, there’s no element of mistreatment. (Clinical Supervisor 1)
It was estimated that this new procedure was tested on more than 400 clients since the average social workers caseload comprises 60 clients. Because known mistreatment cases are often assigned to more experienced social workers, one of them actually identified 23 probable mistreatment cases within her caseload.
. . . every worker now receives new assignments with probable mistreatment cases. But I’ll have to say that when it looks a lot more complex I will assign them to the particular workers. It’s just easier that way to be honest. It’s more client-centered. (Clinical Supervisor 2)
Regarding the clinical supervision meetings, only half of the procedure was implemented as planned. The recordings demonstrated that clinical supervisors did enquire about clients presenting risk factors for older adult mistreatment at the beginning of the session. Generally, social workers were able to give an approximate number of probable mistreatment cases in their caseload. In addition, the level of risk related to older adult mistreatment was addressed by clinical supervisor for almost all the cases presented by the social workers. Not only social workers brought forth cases that had evident signs of mistreatment, but also those they had a gut feeling that something was wrong. Additional data collection by the social workers was sometimes necessary to confirm level of risk at the subsequent supervision session. For more complex cases, the possibility of accessing additional older adult mistreatment expertise was discussed.
The screening tool was not systematically used within the supervision meetings, but it was used for situations where the clinical supervisor wanted to discuss more thoroughly the level of risk for a specific case with the social worker and reach a consensus. Social workers hypothesized that the tool is not automatically used in clinical supervision because clinical supervisor trust their ability to detect older adult mistreatment situations.
You know, it’s assumed that we have a good idea because we’ve been doing mistreatment cases for so long that we know where we’re going with it. (Social Worker 4; Focus group)
The session recordings showed two aspects of the systematic screening procedure that were overlooked by the participants: (a) the clinical supervisor did not systematically enquire about additional clients involved in the probable mistreatment situation, and (b) they did not remind the social workers to document the mistreatment situations using a designated statistical code. None of these aspects of the procedure were mentioned in the interviews. This discrepancy with what was planned raises serious questions regarding the accuracy of administrative data associated with older adult mistreatment situations within the two CLSC. In the initial evaluation protocol, efficacy of the new systematic screening procedure was to be assessed using administrative data to identify older adult mistreatment cases, and these results indicated that this outcome was not reliable.
Acceptability
Acceptability refers to the perception among individual providers that the implemented procedure is satisfactory. The social workers described that the tool provided a lens through which information was collected and analyzed regarding probable older adult mistreatment situations.
For example, in one of the situations, I went back to see the client to ask more specific questions, you know, where there were doubts; and I was able to bring that back to the meeting afterwards and confirm that the level was low in terms of financial exploitation in this case. (Social Worker 2; Focus group)
It was perceived that use of the screening tool to evaluate their caseload prior to a clinical supervision meeting was more crucial for new social workers. Because time is restricted, social workers do a preselection of cases to discuss during clinical supervision, but this process rests on their ability to efficiently identify probable mistreatment situations.
Well, I think that the more senior workers are able to pick up more the cues when there is a suspicion of mistreatment that they bring it more readily than the newer workers.
Do you mean those that have more experience in general—
Yeah. In home care.
or those in older adult mistreatment?
No, I would say in general. I think it was a more valuable tool perhaps for the newer workers. That it was interesting for them to look at that particular screening tool, and to apply it to their clients. (Focus group)
For clinical supervisor, the screening tool could be used to structure the meeting:
It gives us a basis of communication you know, and looking at very concrete kinds of risk factors so that if it exists, it exists, and if it doesn’t, it doesn’t, but they’re clearly identified. So I think that it helps me in supporting the workers in knowing what the next step should be. So it gives us like I said before, a common language. (Clinical Supervisor 1)
Social workers appreciated that the new procedure provided more time to reflect on older adult mistreatment and talk with their clinical supervisor about this issue. Because the procedure is systematic and that there is time dedicated each week especially for probable mistreatment situations, suspected cases are discussed more rapidly with the clinical supervisor. Participants wanted to perpetuate the systematic screening procedure within individual clinical supervision because they acknowledge the need to efficiently screen for older adult mistreatment. They admit that the screening procedure increased their sensitivity to risk factors and that usually, they are not on the lookout for clients presenting more subtle signs. They know that type of case is often overlooked and that the situation will probably get worse with time.
I think it was a learning experience for me too, because I do regular case reviews. I don’t think, for example, some of the issues would have been brought up if it weren’t for the screening tool. (Clinical Supervisor 2)
Social workers agreed that it is the responsibility of their clinical supervisor to prioritize the use of the screening tool for the identification of probable mistreatment situations.
I think it’s important that the clinical supervisors remind us to use the tool when . . . especially when we have our big case reviews.
It’s true.
Because we might not remember I think it should be up to them to bring this up. (Focus group)
Feasibility
Participants identified three main issues influencing to what extent the new systematic screening procedure could be successfully used within the CLSCs: older adult mistreatment is competing with other priorities; the procedure must go beyond screening, and there is a need to clarify where to record information regarding older adult mistreatment.
Older adult mistreatment is competing with other priorities
Participants reported that they did not have enough time during the supervision meeting to go through all the cases and that too much time was still spent on administrative issues. Of the 30-min meeting, the systematic screening procedure for older adult mistreatment never lasted more than 15 min and the remaining of the meeting was used for administrative supervision. Often, cases had to be pushed to the next clinical supervision meeting because of a lack of time. In the following example, a social worker explains the inner workings of administrative supervision.
Our supervision used to be clinical, right? But now with the context of optimization where there is an added focus on worker performance, we have to fill out a grid where we write down the number of visits and the amount of time for different types of activities. This is a tool that the CLSC uses to evaluate our performance, basically. So the supervision meetings that used to be clinical became a component of performance. (Social Worker 2; Focus group)
Some of the social workers believe they will continue to use the procedure but not systematically because of competing priorities.
We have so many other things that we “have” to do that this is adding to that pile. If we don’t “have” to do something, sometimes we just don’t because we don’t “have” to. Because the pile of “have to” and we “want to” is very distinct. So I think it’s a great tool and I think that it helps you kind of zone in and maybe focus on things you wouldn’t have picked up on otherwise. I don’t think that we always have the time to use it, and I think that it’s only going to be the cases where we have those suspicions we’ll probably use the tool versus every case. (Social Worker 4; Focus group)
According to social workers, older adult mistreatment has to be an institutional priority so that the time they invest in the procedure is valued and acknowledged.
At the same time, we have a whole system that’s impeding everything that’s coming from your end. So it doesn’t work because unless there’s an understanding, willingness, recognition, and change from that system to allow us the time to use these wonderful new tools that are coming our way, it’s doomed to disaster. You’re wasting your time, and we’re wasting our time. (Social Worker 1; Focus group)
Procedures must go beyond screening
According to participants, the procedure must go beyond screening and help them develop person-centered interventions within the context of clinical supervision. The participants felt that the procedure did not address questions in terms of how to monitor, which questions to ask the client or family, and how to intervene.
Because there’s one thing about screening—it’s great, but if you don’t know what to do with your screening or you’re not sure what to do, or where to go, then it becomes difficult for the social worker. (Clinical Supervisor 1)
Social workers stressed the importance of combining the level of risk and a protocol to indicate which action should take place according to the level of potential threat.
But also it’s easier for us to go to someone and say, listen, this is what they scored, this is what’s happened, and it’s an easy way to present it as well, because if it means something, it’s something that someone can say, “Oh,” and. . . . You know what I mean? This is what it is, we need help.
And maybe, like, a protocol we could have in place, is let’s say you make your first visit and you’ve scored it, and the person gets a certain level, then you bring those to your SAC at the next meeting. And there has to be room in the clinical to address those cases. (Focus group)
In addition, to help social workers go further in their decision-making process, clinical supervisors need experience in older adult mistreatment and know what questions to ask the client or family.
You need somebody with the experience to help you delve into it further. Right? Because identifying older adult mistreatment is one thing, but knowing which questions to go back and go into it in more depth is something else that requires a bit more finesse and experience. (Social Worker 3; Focus group)
Clarification of the procedure to manage information about the client
One of the clinical supervisors brought up ethical issues that made her uncomfortable regarding where to write information about mistreatment cases: Clients have access to their file, and they are not being told that information from their file is being used to identify signs and risk factors of mistreatment.
I mean, clients don’t necessarily know we’re screening them for older adult mistreatment, right? So, it’s their file, so it’s a little tricky I find. You do a whole visit for an evaluation for suspected mistreatment, or you’re screening, do you write that in a note? Yes, of course, because it’s an evaluation that we’re doing, but clinically, it’s a little tricky. (Clinical Supervisor 1)
Logistically, there was also an issue about not being able to efficiently follow-up mistreatment cases from one supervision meeting to the next. At the following meeting, participants had difficulty in remembering which cases were already discussed and which one had to be discussed with the clinical supervisor.
So I think the infringement would be the time, and then making sure that there is a follow up. Maybe we should try this kind of recommended intervention system, make sure that we come back to that later or at some point, a week later, two weeks later, or a month later, depending on when they were going to proceed, to make sure that we follow up and see how did that work, did it work? You know what else are we looking at, what other information do you have? So, keeping the dialogue going. (Clinical Supervisor 1)
Discussion
Implementation evaluations can be useful prior to evaluating the efficacy of a new program for ensuring that care providers are applying the program according to plan (fidelity), that it is acceptable for them (acceptability), and that it can be perpetuated (feasibility). The present study aimed at assessing those aspects with regard to the implementation of a new systematic screening procedure for older adult mistreatment within the home care division of two Canadian CLSCs.
As planned, results demonstrated that the social workers reviewed their caseload using the screening tool, and potential cases of mistreatment were discussed during supervision meetings. Nonetheless, some aspects of the procedure were overlooked: Participants did not identify additional clients affected by the mistreatment situation or administratively documented mistreatment cases. Some authors (Anthony et al., 2009; Stolee, Hiller, Etkin, & McLeod, 2012) have recommended implementing data management systems to track older adult mistreatment cases and information. The results from this study show that even with clinical supervision, home care professionals omitted to include crucial information regarding suspected older adult mistreatment cases. Consequently, administrative data are not necessarily reliable. Some of the reasons mentioned for not documenting the information were confidentiality issues and unclear procedures. Some are uncomfortable with the fact that information from the client’s file is being used to identify signs and risk factors of mistreatment without the client’s awareness especially since the client can access his file. As Schmeidel et al. (2012) noted, maintaining a relationship of trust is more important for some social and health care professionals than discussing older adult mistreatment with potential victims.
In regard to acceptability, clinical supervisors reported that the screening tool helped to structure the clinical supervision meetings but was not used systematically. Social workers felt it was more useful for less experienced workers. This might explain in part why 22 of the 30 social workers approached for this pilot project were not interested in participating as they might have felt they did not need help with screening. A qualitative study by Goldblatt, Band-Winterstein, and Alon (2018) exploring the social workers’ reflections on their experience of the therapeutic encounter with victims and perpetrators of older adult mistreatment described that a maturation process actually occurred in the professional as well as personal life of the social workers as they dealt with these types of cases. This also supports the hypothesis that less experienced social workers might benefit more from a screening tool than experienced workers as they might need more structure and support for screening.
Social workers acknowledged that there is a need for efficient screening of older adult mistreatment. They also reported that the new procedure increased their sensitivity to subtle signs of mistreatment as well as provided more time for screening and discussing potential cases with their clinical supervisor. These results from the pilot project indicate that social workers might prefer more time to screen their caseload and pre-planned clinical supervision sessions rather than having a specific screening tool. Time constraints (Schmeidel et al., 2012) and not having other colleagues to discuss cases (Killick & Taylor, 2009) have been identified as factors inhibiting screening.
However, other contextual elements must be present to implement a systematic screening procedure within individual clinical supervision and ensure feasibility. First, older adult mistreatment must be a priority set by upper management of health care establishments so that enough time can be allocated for screening. If it is not mandatory, it might not get done even if participants acknowledge the importance of the procedure. Stolee et al. (2012) identified the lack of organizational priority for older adult mistreatment and competing priorities as one of the current challenges associated with developing and implementing mistreatment practices. Government initiatives such as increased funding for prevention and intervention are essential.
Second, clinical supervisors and social workers in home care must have a significant level of training regarding not only screening for older adult mistreatment but also managing this type of situation. In the same sense, tools and procedures developed for home care must not only cover screening but also interventions related to older adult mistreatment. As reported by Killick and Taylor (2009), the social and health care professional’s confidence in his or her ability to intervene efficiently plays a role in the decision to manage the mistreatment situation.
Conclusion and Limitations
This pilot study gives indication on which elements to consider when implementing a systematic procedure within individual clinical supervision. It must be taken into consideration that this pilot project was implemented within a Canadian (province of Quebec) home care context and the sample size was small, meaning that there are limitations to its transferability to other contexts. In addition, participants were included in this study on a voluntary basis, meaning that they were probably more interested in improving screening for older adult mistreatment to begin with. Further studies are necessary to identify appropriate implementation strategies to address the contextual issues found in this pilot project as well as to evaluate the efficacy and efficiency of this new systematic screening procedure for older adult mistreatment within individual clinical supervision.
Footnotes
Acknowledgements
A special thanks to the clinical supervisors and social workers that accepted to participate in the evaluation of the implementation of the systematic screening procedure for older adult mistreatment. For her help with the literature search and insightful comments on the manuscript, we also thank Muriel Guériton, specialized librarian of the Health Intervention and Technology Assessment Unit.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Integrated Health and Social Services University Network for West-Central Montreal (Quebec, Canada).