
Abstract
Previous research has indicated that childhood maltreatment is predictive of psychiatric symptoms in adulthood. Among the potential intervening factors in this relationship are affective reactions in the victims, neurodevelopmental problems, and resilience. The purpose of this study was to test, in a nonclinical low-risk sample, an integrative developmentally based psychoneurological model of the roles of limbic system dysfunction, shame and guilt, and resiliency as potential intervening variables between childhood maltreatment and adult psychiatric symptoms. Also of interest was whether there were gender-specific pathways from maltreatment to symptoms. Based on the results of preliminary analyses, several regressions were conducted separately by gender, entering the different forms of parental aggression at Step 1, resilience at Step 2, the resilience by parental aggression interaction term at Step 3, shame and guilt at Step 4, and limbic dysfunction at Step 5, as predictors of psychiatric symptoms. Analyses indicated that both maternal psychological maltreatment and paternal physical maltreatment were predictive of total psychiatric symptomatology in adulthood, with shame mediating the relationship in women and guilt mediating it in men, limbic system symptoms mediating the relationship in both genders, and trait resilience moderating the relationship in both genders.
Keywords
There is a substantial literature on the negative effects of childhood maltreatment, with a considerable emphasis on intergenerational transmission of violence and the contribution of childhood experience of violence to later psychopathology. Although this research supports the propositions that violence breeds violence and violence breeds illness, it also indicates that not every maltreated child becomes an abusive or mentally ill adult. Moreover, much of this research (a) lacks a strong theoretical basis, (b) provides limited information on the developmental mechanisms contributing to later pathology in maltreated children, (c) relies on clinical samples, and (d) fails to consider the extent to which developmental pathways may differ by gender. The purpose of the current study was to examine an integrative developmentally based, psychoneurological model of mechanisms that mediate or moderate the relationship between childhood maltreatment and psychiatric symptoms in nonclinical samples of women and men. This developmental model assumes that shame, guilt, and resilience share with limbic system dysfunction significant psychoneurological foundations that help elucidate the understudied pathways from childhood maltreatment to adult symptomatology.
Childhood maltreatment encompasses physical abuse (defined as nonaccidental bodily injury), emotional or psychological abuse (defined as persistent opposition to basic emotional needs), sexual abuse, and neglect (Cicchetti & Toth, 2005). According to the U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau (2016), an estimated 702,000 children reported maltreatment in 2014, a rate of 9.4 per 1,000 children. Seventy-five percent of these children experienced parental or caretaker neglect, 17.0% experienced physical abuse, 8.3% experienced sexual abuse, and 6.8% experienced other types of maltreatment, such as psychological (U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau, 2016).
Moreover, reports such as these from government agencies often underestimate the true prevalence of abuse (Cicchetti & Toth, 2005; Gilbert et al., 2009). A study of self-reported childhood maltreatment in the Eastern and Southeastern United States found 4 to 6 times greater prevalence of abuse than reported in Child Protection Services’ records (Everson et al., 2008). In a sample of 15,197 adults, the National Research Council Panel of Research on Child Abuse and Neglect found a prevalence rate of 41.5% who had experienced supervision neglect, such as being left unsupervised when an adult should have been at home; 11.8% reporting physical neglect, such as not being cleaned or attended to medically; 28.4% physical assault; and 4.5% sexual abuse (Hussey, Chang, & Kotch, 2006).
The relationship between childhood maltreatment and later psychiatric symptomatology has been investigated in many patient samples. Compared with the general population, patients with the following conditions have reported greater prevalence of childhood abuse: major depression (e.g., Mueller-Pfeiffer et al., 2013; Pietrek, Elbert, Weierstall, Müller, & Rockstroh, 2013); posttraumatic stress disorder (PTSD; e.g., Alim et al., 2006; Breslau et al., 2014; Khoury, Tang, Bradley, Cubells, & Ressler, 2010; McQuaid, Pedrelli, McCahill, & Stein, 2001; Van Voorhees, Dennis, Calhoun, & Beckham, 2014); somatization disorder and physical symptoms in adulthood (e.g., Felitti et al., 1998; Schulte & Petermann, 2011); and bipolar disorder (Etain et al., 2010; Hyun, Friedman, & Dunner, 2000; Larsson et al., 2013). Other research indicates that individuals with a history of childhood physical or sexual abuse exhibit more symptoms of anxiety (MacMillan et al., 2001; Teicher, Samson, Polcari, & McGreenery, 2006), depression (MacMillan et al., 2001; Teicher et al., 2006), and anger-hostility (Teicher et al., 2006) than individuals not reporting such abuse.
In our review of the literature underlying our proposed psychoneurological model of the developmental pathways from childhood maltreatment to psychiatric symptoms, the strands of evidence that contribute to each of the proposed pathways are considered. To our knowledge, there is no previous research testing a model of the maltreatment–symptoms relationship that includes limbic system dysfunction, shame, guilt, and resilience and the relationships among them.
Neurological Outcomes of Childhood Maltreatment
Studies of the neurodevelopmental outcomes of childhood maltreatment have tended to focus on its impact on the limbic system (Teicher et al., 2003). The major structures of the limbic system consist of the hippocampus (involved in memory formation and retrieval), the hypothalamus (which regulates the autonomic nervous system and thereby the stress response), and the amygdala (involved in emotion processing and regulation). There is evidence that childhood maltreatment is associated with later limbic system dysfunction, particularly limbic system irritability (heightened electrical activity in limbic structures, overreactivity in limbic structures in response to stress, increased prevalence of symptoms suggestive of temporal lobe epilepsy; Teicher, 2000). 1
In studies using a self-report measure of symptoms of limbic system irritability (e.g., somatic and perceptual distortions, brief hallucinatory events, motor automatisms, and dissociative symptoms), Teicher, Glod, Surrey, and Swett (1993) found positive associations between childhood maltreatment and symptoms of limbic abnormality, and Teicher et al. (2006) found that adults with a history of childhood emotional or physical abuse reported greater limbic system irritability than those with no abuse; moreover, adults with combined childhood emotional and physical abuses reported higher rates of limbic system symptoms than individuals reporting a single type of abuse. In an exploratory diffusion tensor imaging study of young adults, Choi, Jeong, Rohan, Polcari, and Teicher (2009) found that reports of parental verbal abuse during childhood were associated with reduced neural integrity in pathways also characterized by increased limbic system irritability.
There has also been research regarding the possibility that neurobiological outcomes mediate the relationship between childhood maltreatment and later vulnerability to traumatic stress and other psychiatric disorders, particularly as related to aggression (e.g., Lee & Hoaken, 2007). There is some evidence that repeated exposure to childhood trauma is associated with kindling, a process of oversensitizing the limbic system (van der Kolk & Saporta, 1991), and is implicated in lowering the threshold for psychological vulnerability to subsequent traumas (van der Kolk, McFarlane, & Weisaeth, 2006). There is also evidence that limbic system dysfunction is linked to various consequences of childhood maltreatment pertaining to emotional expression and cognition (Grassi-Oliveira, Ashy, & Stein, 2008). For example, limbic system irritability has been found to be positively correlated with psychiatric symptoms of anxiety, depression, and anger-hostility (Anderson, Teicher, Polcari, & Renshaw, 2002).
Affective Responses to Childhood Maltreatment
The immediate outcomes of childhood maltreatment include heightened feelings of shame, feelings that are associated with psychiatric symptoms. In one longitudinal study of children from abusive and nonabusive homes, Stuewig and McCloskey (2005) found that harsh parenting during childhood was associated with shame-proneness during adolescence and that, over time, shame-proneness was associated with depression. In a study looking at childhood maltreatment and internalized shame in adults diagnosed with bipolar disorder, Fowke, Ross, and Ashcroft (2012) found that significantly more participants in their bipolar disorder sample than in their nonpsychiatric sample reported childhood physical abuse, emotional abuse, and neglect; levels of internalized shame were also significantly higher in the bipolar group. Moreover, in the bipolar group, there were significant positive correlations between all of the childhood maltreatment scores and internalized shame. There appears to have been little or no research on the relationship between childhood maltreatment and guilt, and little or no attention to the possibility of gender differences in any such relationship.
Kim, Thibodeau, and Jorgensen (2001) have emphasized the importance of differentiating between shame and guilt, both of which are considered to involve self-evaluative processes related to important behavioral standards and having important implications for “social survival” within particular cultural contexts. They describe shame as involving an inner-directed negative view of the entire self and guilt as involving an outward-directed negative view of specific behaviors in regard to others. In their comprehensive review of relevant studies, they found that shame was much more strongly related to depression than guilt. In their discussion of their findings, they suggest that more research is needed to determine the extent to which sex moderates associations of shame and guilt with depressive symptoms. In the current study, a somewhat different approach was taken, examining the extent to which shame and guilt mediated the relationship between childhood maltreatment and symptomatology.
Evidence has started to emerge in support of a developmental, neurological basis for those two “moral” emotions, guilt and shame. Neuroimaging studies have identified unique activation patterns for shame and guilt that differ from neutral emotion conditions (Michl et al., 2014). Both emotions have been found to be associated with activation in the temporal lobe; however, shame is associated with greater activation in the medial and anterior frontal lobe, whereas guilt is associated with activation in the amygdala and insula.
Studies involving lesions and other forms of damage to the prefrontal cortex have provided further evidence for a neurological basis for these emotions. For example, patients with lesions in the medial prefrontal cortex show diminished emotional experience, including lowered self-conscious emotions that serve a social function, such as guilt, shame, and embarrassment (e.g., Philippi & Koenigs, 2014). In a study conducted by Koenigs and colleagues (2007), patients with focal bilateral damage to the ventromedial prefrontal cortex showed severely diminished embarrassment and guilt, while comparison subjects had intact emotional processing. Moreover, fronto-temporal dementia, which causes degeneration of the medial prefrontal cortex, is tied to a decline in self-conscious emotions that are closely linked to shame and guilt (Lewis, 2010; Michl et al., 2014) such as embarrassment (Philippi & Koenigs, 2014).
Resilience
Not all individuals who experience childhood maltreatment develop psychiatric symptoms; some of these victims appear to be resilient. Resilience refers to individual characteristics (e.g., positive self-esteem and self-control) and external/environmental factors (e.g., family and educational support) that allow individuals to adapt successfully to stressful situations (Luthar, Cicchetti, & Becker, 2000). In a study of 132 college students, Campbell-Sills, Cohan, and Stein (2006) identified trait resilience as a protective factor in the relationship between childhood emotional neglect and present psychiatric symptoms. In a study of 70 PTSD patients, Daniels et al. (2012) found trait resilience to be a significant negative predictor of PTSD symptoms in patients who had reported severe childhood trauma. In a sample of adults who had experienced childhood sexual abuse, Ginzburg et al. (2006) found psychiatric symptoms to be positively correlated with guilt and shame, and negatively correlated with traits of resilience.
Research exploring neurobiological contributors to resilience has indicated the importance of genetic and potential epigenetic mechanisms in response to stress (Feder, Nestler, & Charney, 2009; Southwick & Charney, 2012). Genetic polymorphisms affect limbic reactivity and prefrontal-limbic connectivity, influencing responses to traumatic events (Feder et al., 2009). Brain-imaging studies have confirmed that the prefrontal region is potentially influential in reducing activity in the amygdalae (Hariri, Bookheimer, & Mazziotta, 2000). Animal studies have also shown the importance of this region (Southwick & Charney, 2012). Early experiences coping with stress increase neuroplasticity in the prefrontal cortex, which buffers against the negative effects of future uncontrollable stress (Southwick & Charney, 2012). In addition to prefrontal cortical functioning and capacity to regulate limbic reactivity to stress, moderators of resilience include effective regulation of the hypothalamic-pituitary-adrenal (HPA) axis (which influences hormone secretion in reaction to stress) and the sympathetic nervous system (SNS; which influences the body’s “fight or flight” reaction in response to stress) (Southwick & Charney, 2012).
Russo, Murrough, Han, Charney, and Nestler (2012) have noted that the “study of human resilience is still a mostly phenomenological literature that has only begun to characterize biological factors in resilient individuals that are associated with more successful coping responses” (p. 1475). Based on their review of the scanty relevant literature, they report that developmentally, childhood abuse affects the same regions of the brain shown to contribute to resilience, such as the limbic system. They also found that neurological and genetic resilience has a buffering effect against depression. Thus, resilience may involve psychoneurological processes. The research they summarize on the impact of stress on the limbic system and related processes, taken together with Teicher and colleagues’ (2006) conclusions about the neurological impact of childhood abuse, suggests that childhood abuse may affect the same regions of the brain shown to contribute to resilience, and that any relationship between childhood maltreatment and resilience may have a neurological basis. Previous literature has incorporated resilience, as well as shame and guilt, into studies investigating neurological underpinnings of stress outcomes and psychiatric symptoms; however, the relationship between shame and guilt and resilience has been neglected, particularly from a developmental psychoneurological framework that attends to the issue of potential gender differences in pathways.
Figure 1 provides our proposed model of the relationships among the variables of interest in the current study: childhood maltreatment as a predictor, adult psychiatric symptoms as an outcome, shame and guilt as affective mediators of the maltreatment–psychiatric outcomes relationship, limbic system dysfunction as a neurological mediator of the maltreatment–psychiatric outcomes relationship, and resilience as a moderator of the maltreatment–psychiatric outcomes relationship. This conceptual model of psychiatric outcomes was tested in the current study. Specifically, the present study investigated a conceptual model of psychiatric outcomes in nonclinical samples of men and women reporting childhood psychological or physical maltreatment.
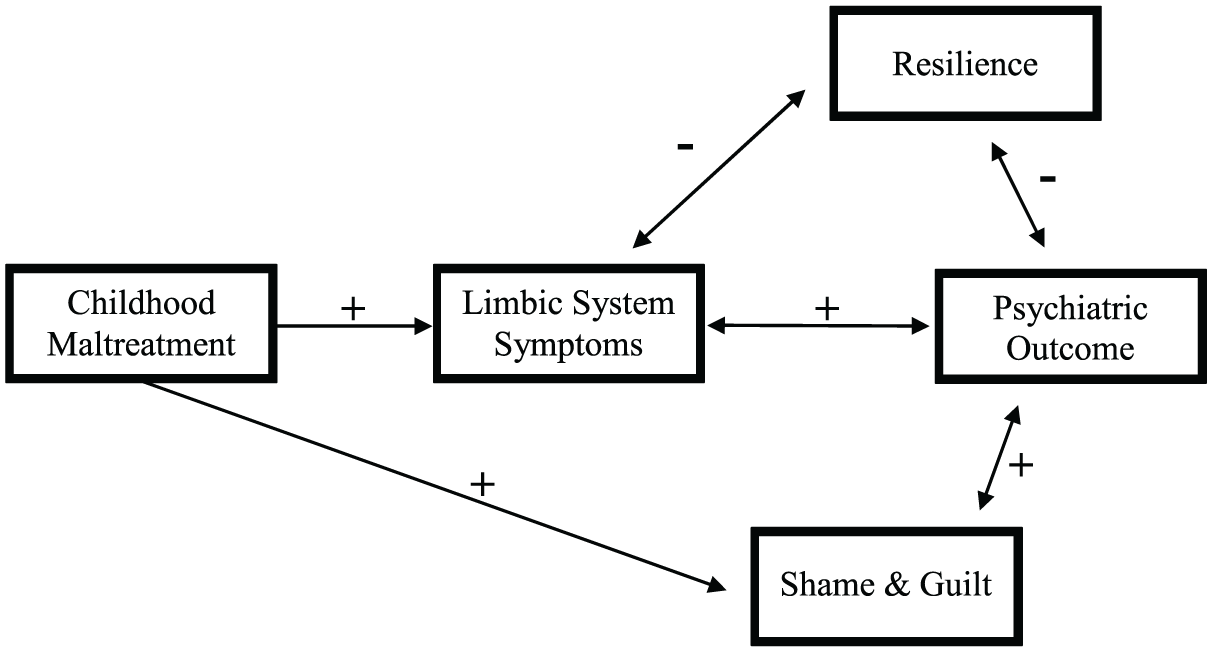
Childhood maltreatment model of psychiatric outcomes.
The investigation was guided by the following hypotheses:
Method
The current project was a secondary analysis of an available dataset. Protocols of the project were reviewed and approved by the university’s Institutional Review Board. The research was conducted in compliance with all American Psychological Association guidelines and state and federal laws. All surveys were collected anonymously, and all participants included in the dataset had given permission for their anonymous responses to be analyzed in future studies.
Participants
The sample consisted of 439 participants (239 females, 200 males) recruited by students in a research methods class from a large, urban university in the Northeastern United States. Participants ranged in age from 18 to 69 years, with a mean age of 27 years and a median age of 21 years. The average participant was a non-Hispanic, White, unmarried college student whose self-reported socioeconomic status was middle or upper-middle class.
Measures
Demographic Questionnaire
Information regarding sex, age, ethnicity, marital status, socioeconomic status, and education level was obtained from the participants.
Conflict Tactics Scales: Parent–Child (CTSPC)
The CTSPC is a 44-item questionnaire that measures the self-reported frequency of conflict tactics (negotiation tactics, psychological aggression, and physical aggression) employed by the participant’s parents during the “worst year” of the participant’s childhood (Straus & Hamby, 1997). For each tactic witnessed or reported by the participant, participants reported frequencies ranging from 0 (“never happened”) to 6 (“happened more than 20 times”). These numbers were summed to obtain the overall scores for each conflict subscale. The CTSPC has shown good construct and discriminant validity and good reliability, with internal consistencies ranging from .79 to .95 (Ashy, 2003; Straus & Hamby, 1997).
Resilience Scale (RS)
The RS (Wagnild & Young, 1993) is a self-report questionnaire dealing with self-acceptance and personal competence (e.g., “I usually take things in stride”; “I am friends with myself”). Originally consisting of 25 items, the version employed in this study was a shortened, 10-item questionnaire derived from a factor analysis performed by Neill and Dias (2001). Participants respond to each question on a scale of 1 to 7, with 1 being “strongly disagree,” 4 being “neutral,” and 7 being “strongly agree.” The RS has demonstrated good construct validity along with high reliability (Wagnild & Young, 1993). A review of resilience instruments by Ahern, Kiehl, Lou Sole, and Byers (2006) found the RS to be the most suitable instrument to study resilience in young adults due to its confirmation in multiple studies.
Limbic System Function Questionnaire (LSCL-33)
The LSCL (Teicher et al., 1993) is a 33-item, self-report scale that asks participants to rate how frequently they experience various forms of limbic irritability, consisting of visual disturbances, somatic disturbances (e.g., numbness), dissociative disturbances, hallucinatory events (e.g., hearing voices), and automatisms (e.g., twitching). The LSCL is a noninvasive method of measuring temporolimbic functioning and has been correlated with the Dissociative Experiences Scale and the Hopkins Symptoms Checklist (Teicher et al., 1993). Participants are asked to describe the lifetime frequency of limbic system events as occurring “never,” “rarely,” “sometimes,” or “often.” A score of 0, 1, 2, 3, or 4 is assigned for each item (0 = never, 4 = often). A total score for all 33 items was calculated, along with scores for sensory, somatic, behavioral, and mnemonic disturbances. In prior studies, normal adults have exhibited total LSCL-33 scores lower than 10, while patients diagnosed with temporal lobe epilepsy have exhibited total LSCL-33 scores in the range of 23 to 60 (Anderson et al., 2002). The LSCL-33 has shown high test–retest reliability, with r = .92 for the whole scale and .78 to .86 for subscales (Ashy, 2003; Teicher et al., 1993).
Symptom Questionnaire (SQ)
The SQ (Kellner, 1987) is a 92-item, true/false scale with four symptom subscales (Depression, Anxiety, Anger, Somatization) and four well-being subscales (Content, Relaxed, Friendly, Somatic Well-Being). The SQ has been validated in a normal population (Teicher, Samson, Sheu, Polcari, & McGreenery, 2010). The test–retest reliability of the subscales in various studies was r = .71 for anxiety, r = .95 for depression, r = .77 for somatic, and r = .82 for hostility (Ashy, 2003; Kellner, 1987).
Personal Feelings Questionnaire (PFQ-2)
The PFQ (Harder & Zalma, 1990) is a 22-item measure that assesses expressions of shame and guilt. Response choices range from 1 (“You never experience the feeling”) to 4 (“You almost continuously feel the feeling”). The PFQ has shown good internal consistency and construct validity with evidence of convergent and discriminant validity (Harder & Zalma, 1990).
Data Analysis
The t tests were performed to determine whether differences by gender were present in any of the main variables under investigation (childhood maltreatment history, psychiatric symptoms, guilt and shame assessments, limbic system symptom rating, and resilience score).
To test Hypotheses 1 and 2, Pearson’s correlations were conducted separately by gender. Based on the outcomes of the bivariate Pearson correlations, multiple regressions were conducted to determine the relative contributions of the predictor factor (childhood maltreatment), the proposed mediators (guilt, shame, and limbic system symptoms), and the proposed moderator (resilience) to psychiatric outcomes. Relationships were analyzed separately for males and females as a function of type of maltreatment (mother physical, mother psychological, father physical, and father psychological). 2
Results
Descriptive Statistics
Table 1 provides means and standard deviations for all study variables, separately by gender. Participants reported incidences of parental psychological and physical aggression comparable with samples in previous studies (Teicher & Parigger, 2015). Furthermore, their limbic ratings were comparable with those in previous nonclinical samples (Teicher et al., 1993), as were their reported levels of anxiety, depression, somatization, and hostility (Kellner, 1987).
Descriptive Statistics for Major Study Variables Separately by Gender, with t Test Results.
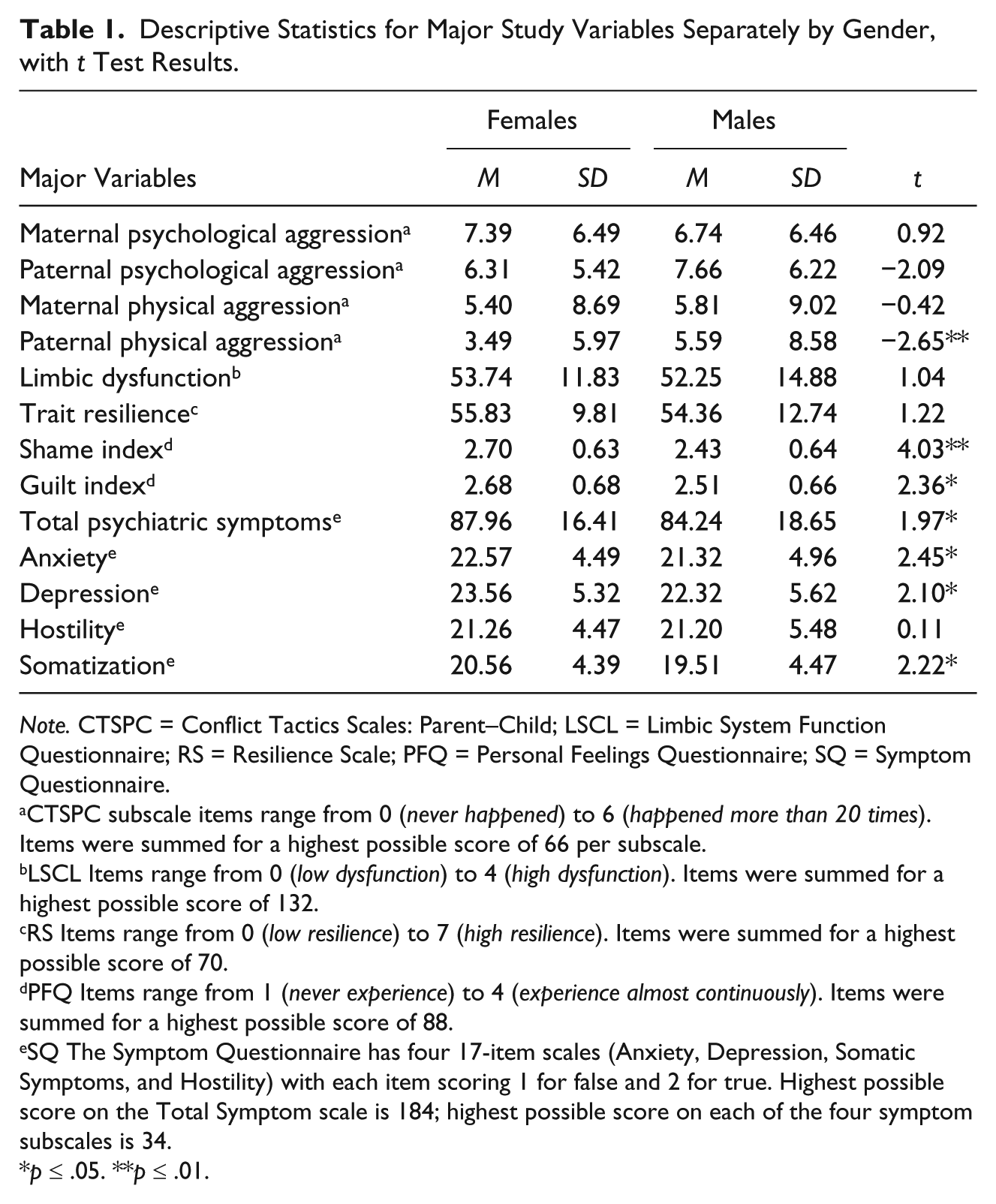
Note. CTSPC = Conflict Tactics Scales: Parent–Child; LSCL = Limbic System Function Questionnaire; RS = Resilience Scale; PFQ = Personal Feelings Questionnaire; SQ = Symptom Questionnaire.
CTSPC subscale items range from 0 (never happened) to 6 (happened more than 20 times). Items were summed for a highest possible score of 66 per subscale.
LSCL Items range from 0 (low dysfunction) to 4 (high dysfunction). Items were summed for a highest possible score of 132.
RS Items range from 0 (low resilience) to 7 (high resilience). Items were summed for a highest possible score of 70.
PFQ Items range from 1 (never experience) to 4 (experience almost continuously). Items were summed for a highest possible score of 88.
SQ The Symptom Questionnaire has four 17-item scales (Anxiety, Depression, Somatic Symptoms, and Hostility) with each item scoring 1 for false and 2 for true. Highest possible score on the Total Symptom scale is 184; highest possible score on each of the four symptom subscales is 34.
p ≤ .05. **p ≤ .01.
As shown in Table 1, t tests revealed significant gender differences on several study variables. Specifically, male participants reported a higher incidence of paternal psychological and physical aggression than females. By contrast, female participants reported higher levels of guilt and shame, as well as higher levels of anxiety, depression, somatization, and total psychiatric symptoms than males.
Correlations Between Different Forms of Parental Aggression and Predicted Outcomes, Mediators, and Moderator
To test Hypothesis 1 (that exposure to childhood maltreatment would be negatively correlated with resilience and positively correlated with limbic system dysfunction, guilt, shame, and psychiatric symptoms), several correlations were performed, separately by gender. As can be seen in Table 2, patterns of correlation varied somewhat by subject gender, type of aggression, and source of aggression.
Correlations Between Childhood Experiences of Aggression and Major Study Variables for Males and Females.
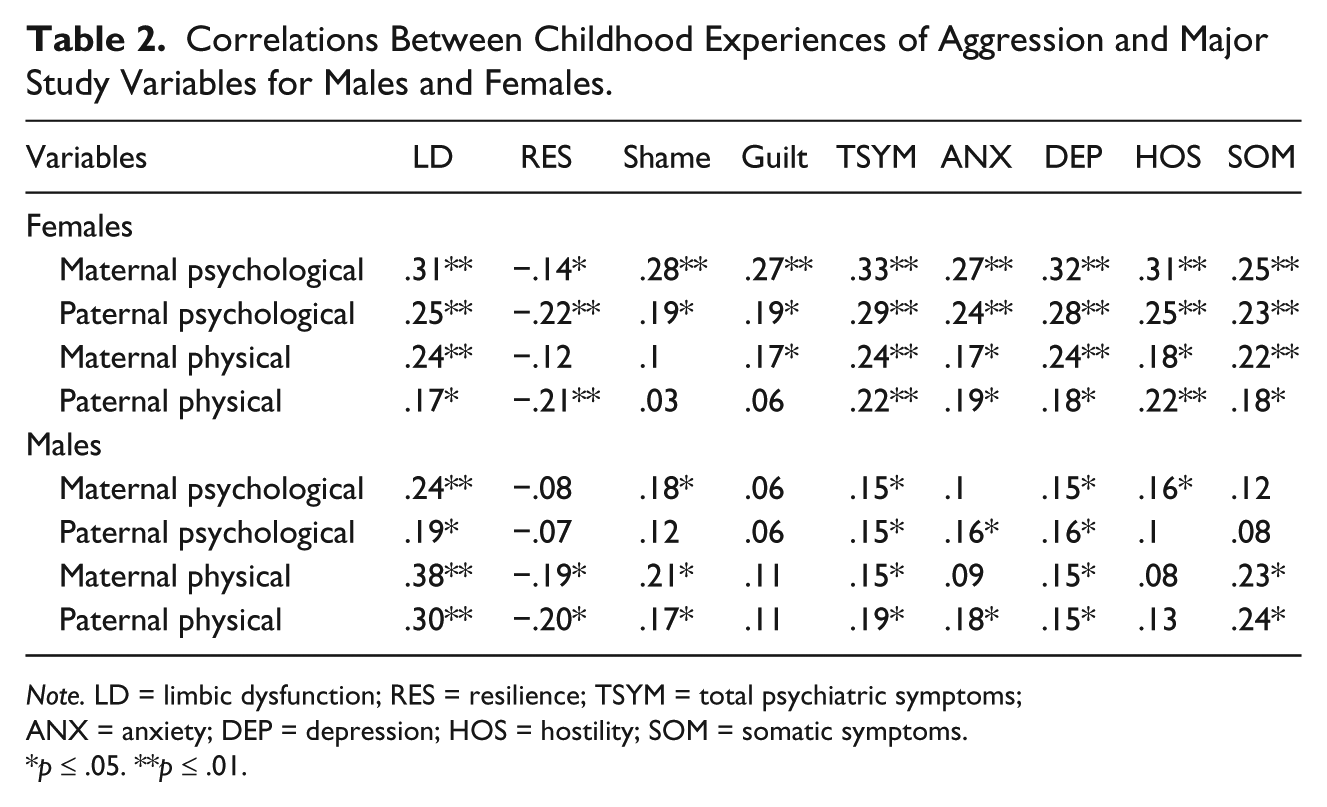
Note. LD = limbic dysfunction; RES = resilience; TSYM = total psychiatric symptoms; ANX = anxiety; DEP = depression; HOS = hostility; SOM = somatic symptoms.
p ≤ .05. **p ≤ .01.
Parental aggression and later symptoms
In females, both maternal and paternal psychological and physical aggression were significantly positively correlated with all psychological symptoms and limbic system dysfunction. In males, paternal and maternal physical aggression were significantly positively correlated with somatization but uncorrelated with other psychiatric symptoms, and there were no significant correlations between psychological aggression from either parent and any psychiatric symptom or limbic system dysfunction.
Parental aggression and resilience
In females, paternal and maternal psychological aggression, as well as paternal physical aggression, were significantly negatively correlated with resilience, whereas in males, only paternal and maternal physical aggression showed significant negative correlations with resilience. In females, paternal and maternal psychological aggression were significantly positively correlated with shame, and paternal and maternal psychological aggression, as well as maternal physical aggression, were significantly positively correlated with guilt. By contrast, in males, paternal and maternal physical aggression, as well as maternal psychological aggression, were significantly positively correlated with shame, but no forms of parental aggression were significantly correlated with guilt.
Correlates of Limbic System Dysfunction, Separately by Gender
Findings regarding Hypothesis 2 (that limbic dysfunction would be negatively correlated with resilience and positively correlated with guilt, shame, and psychiatric symptoms) can be found in Table 3. As can be seen, for women, limbic system dysfunction was significantly negatively correlated with resilience and positively correlated with shame, guilt, and all psychiatric symptoms. In males, limbic dysfunction was significantly positively correlated with shame, guilt, and all psychiatric symptoms but was not associated with resilience.
Correlations Between Limbic Dysfunction and Other Major Study Variables.
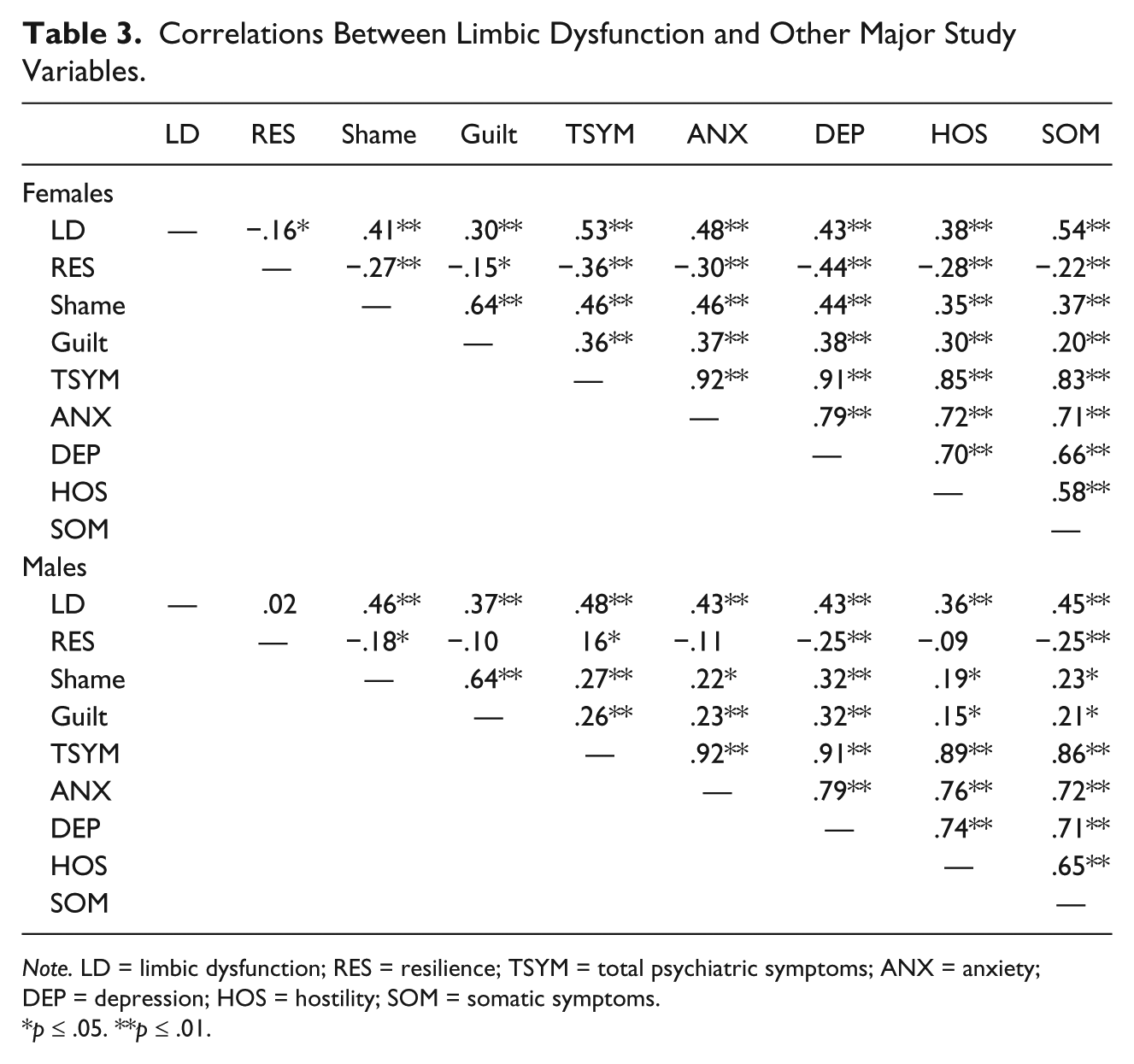
Note. LD = limbic dysfunction; RES = resilience; TSYM = total psychiatric symptoms; ANX = anxiety; DEP = depression; HOS = hostility; SOM = somatic symptoms.
p ≤ .05. **p ≤ .01.
Regression Analyses
The results of regression analyses run to test Hypothesis 3 (that the relationship between childhood maltreatment and adult psychiatric symptoms would be mediated by limbic system dysfunction, guilt, and shame, and moderated by trait resilience) can be seen in Tables 4 to 6. The analyses are separated by type of parental aggression (mother psychological, mother physical, father psychological, and father physical) and also by gender. In each analysis, total scores for psychiatric symptoms were regressed first on one specific form of parental aggression; resilience scores were added at Step 2; the resilience by parental aggression interaction term was added at Step 3; guilt and shame were added at Step 4; and limbic system dysfunction was added at Step 5.
Linear Multiple Regression Model for the Prediction of Total Psychiatric Symptoms by Maternal Psychological Aggression Mediators and Moderators.
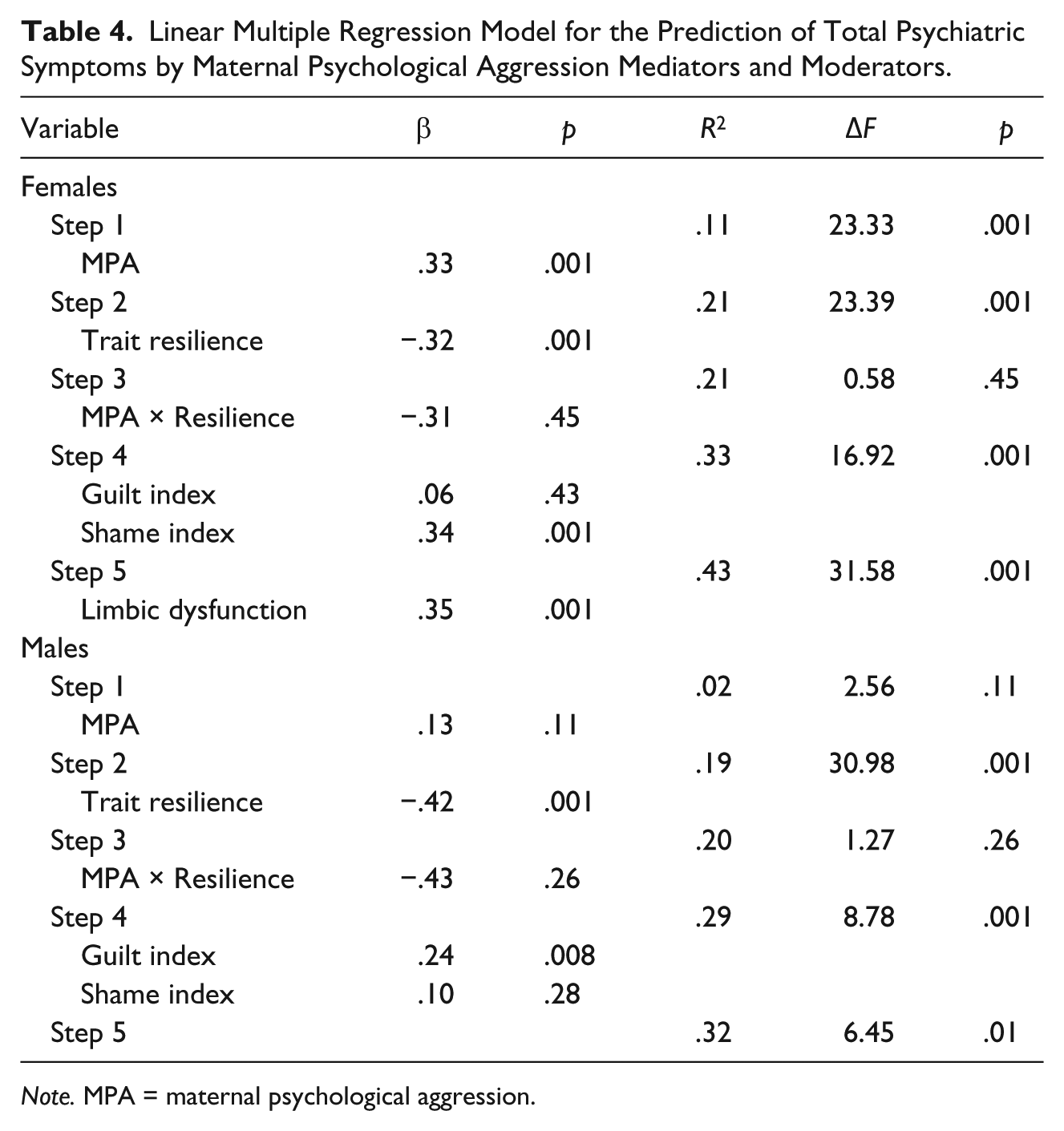
Note. MPA = maternal psychological aggression.
Linear Multiple Regression Model for the Prediction of Total Psychiatric Symptoms by Maternal Physical Aggression Mediators and Moderators.
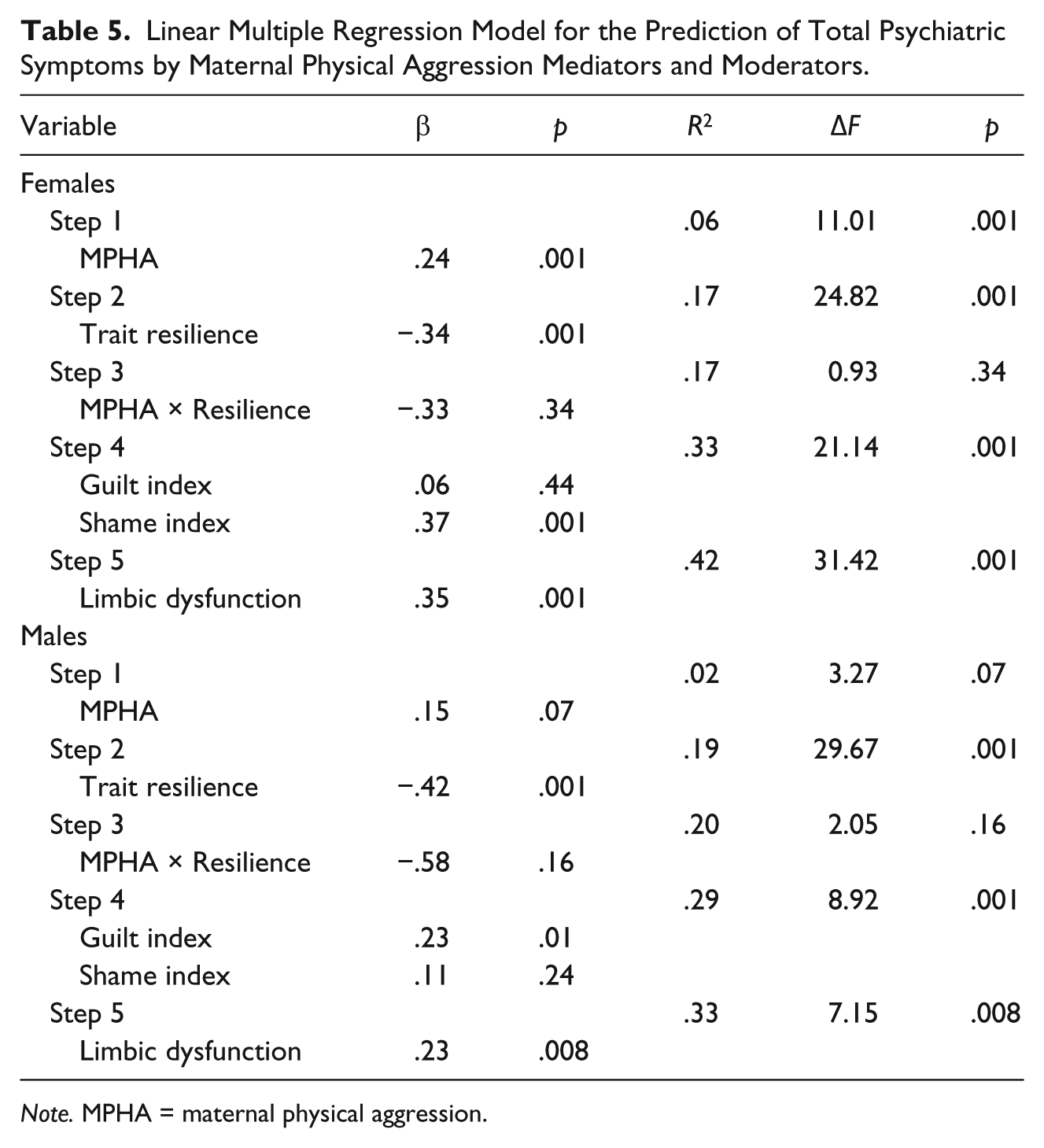
Note. MPHA = maternal physical aggression.
Linear Multiple Regression Model for the Prediction of Total Psychiatric Symptoms by Paternal Psychological Aggression Mediators and Moderators.

Note. PPA = paternal psychological aggression.
As shown in Step 1 of Tables 4 to 6, each type of parental maltreatment contributed significantly to psychiatric symptoms in females; however, in males, only paternal physical aggression contributed significantly to psychiatric symptoms, with maternal physical aggression and paternal psychological aggression making only marginally significant contributions. In both males and females, trait resilience added significantly to variance in psychiatric symptoms at Step 2 of each equation. The resilience by parental aggression interaction term, added at Step 3, did not add significantly to variance explained in any of the equations. At Step 4, in females, shame and guilt added significantly to variance in symptomatology, but the Betas revealed that it was only shame that added significantly to psychiatric outcomes in all four parental aggression analyses. In males, it was guilt that added significantly to variance in psychiatric symptoms in each equation. At the final step, limbic system symptoms added significantly to prediction of psychiatric symptoms in both males and females in all four equations.
Discussion
The goal of this developmentally based psychoneurological study was to examine the relationships among childhood maltreatment, limbic dysfunction, trait resilience, shame and guilt, and psychiatric symptoms, and to determine whether those relationships varied by gender. It was predicted that shame and guilt and limbic dysfunction would mediate, and resilience would moderate the relationships between childhood maltreatment and later psychiatric symptoms. The findings of this investigation indicated that maternal psychological maltreatment and paternal physical maltreatment were predictive of total psychiatric symptomatology in adulthood, with shame contributing to symptomatology in women and guilt in men. Limbic dysfunction was found to play a significant role in mediating the relationship between childhood maltreatment and psychiatric symptoms, whereas trait resilience was found to play a moderating, protective role in predicting psychiatric symptomatology.
In our preliminary analyses, female participants scored higher than males in anxiety, depression, somatization, guilt, shame, and total psychiatric symptoms. These findings are consistent with other studies showing higher scores in females than in males in somatization (e.g., Ashy, 2003; Teicher et al., 1993), anxiety and depression (e.g., Altemus, 2006; Piccinelli & Wilkinson, 2000), shame and guilt (e.g., Else-Quest, Higgins, Allison, & Morton, 2012; Hoglund & Nicholas, 1995), and a range of internalizing symptoms (e.g., Kramer, Krueger, & Hicks, 2008). Males reported more paternal psychological and physical aggression than females, which is consistent with previous research findings (Ashy, 2003; Ashy & Malley-Morrison, 2000).
The first hypothesis in our developmentally based psychoneurological model, that exposure to childhood maltreatment would be negatively correlated with resilience and positively correlated with limbic dysfunction, guilt, shame, and psychiatric symptoms, was partially supported in both males and females. These correlations are consistent with the results of previous research on childhood maltreatment and resilience in adulthood (e.g., Luthar et al., 2000), as well as research on childhood maltreatment and limbic dysfunction in adulthood (e.g., Anderson et al., 2002; Ashy, 2003; Teicher et al., 2006). The positive association between childhood maltreatment and guilt and shame is also consistent with research showing high levels of negative self-perception and neuroticism in individuals with traumatic experiences (Campbell-Sills et al., 2006; Kling, Ryff, Love, & Essex, 2003).
From a psychoneurological perspective, a possible basis for the link between childhood maltreatment and limbic dysfunction can be found at the biological level, as enhanced activity of stress response systems may cause the brain to follow alternative developmental pathways to manage an environment of heightened stressors (Teicher et al., 2006). Moreover, the negative associations found between maltreatment and resilience can be considered in light of the altered environment experienced by maltreated children; what may constitute resilience in an abnormally stressful environment may not characterize resilience in the normal environment as measured by the Reslience Scale (Wagnild & Young, 1993). Furthermore, the contribution of childhood maltreatment to feelings of guilt and shame may be explained through limbic dysfunction or through behavioral and cognitive mechanisms, such as a negative self-concept and behavioral inhibition, or through internalization of blame for the experienced abuse.
There were several gender-specific findings related to the first hypothesis. Exposure to maltreatment was associated with all psychiatric symptoms in females; however, in males, exposure to maltreatment was associated only with somatization. One possible explanation for this finding is that the connection between abuse and psychiatric symptoms is direct in females but may be indirect in males through other variables such as alcohol and substance abuse (Kessler et al., 1994).
The second hypothesis, that limbic dysfunction would be negatively correlated with resilience and positively correlated with guilt, shame, and psychiatric symptoms, was partially supported, with some variations observed for males and females. The negative association between limbic dysfunction and resilience was supported in females but not in males; this association was not robust, so further study would be appropriate. Resilience has been shown to be a moderator of psychiatric symptoms and PTSD in both males and females with histories of childhood trauma (Campbell-Sills et al., 2006; Daniels et al., 2012), and the amygdala has been implicated in the ability to regulate emotions in response to fearful stimuli (Amorapanth, LeDoux, & Nader, 2000). As the limbic system is involved in emotional regulation, and resilience is conceptualized as the ability to regulate emotions, the limbic dysfunctions might be affecting the core of resilience.
In support of our developmentally based psychoneurological model, the positive relationships among self-reported limbic dysfunction, guilt, and shame are consistent with functional magnetic resonance imaging (fMRI) studies showing activation of the amygdala in response to hostile stimuli (Aleman & Swart, 2008; Sambataro et al., 2006). The association between limbic dysfunction and psychiatric symptoms is consistent with findings from Teicher et al. (2006) indicating comparatively large effect sizes for anxiety, depression, and hostility in individuals exposed to childhood traumas compared with individuals not reporting such exposure.
The third hypothesis, which was the most direct test of our integrated developmentally based psychoneurological model, predicted that resilience, guilt, shame, and limbic dysfunction are intervening variables between childhood maltreatment and adult psychiatric symptoms; this hypothesis was supported by the results of the linear regression analyses. In females, maternal and paternal psychological aggression, shame, limbic system dysfunction, and resilience contributed significantly to the variance in psychiatric symptoms, with shame as a major predictor of symptoms and a mediator of the childhood aggression–symptoms relationship. In males, paternal physical aggression, guilt, limbic system dysfunction, and resilience contributed significantly to the variance in psychiatric symptoms, with guilt as a major predictor of symptoms and a mediator of the maltreatment–symptoms relationship. Based on the regression analysis, limbic system dysfunction, guilt, and shame can be seen as risk factors for psychiatric symptoms (with some variation by gender), while, consistent with previous research (Campbell-Sills et al., 2006), resilience can be seen as a protective factor.
Of particular interest are the findings concerning shame and guilt, which provide some support for a partially gender-specific pathway from childhood maltreatment to psychiatric symptomatology. These findings make sense in regard to the literature, indicating that abused females tend to express their distress through internalizing symptoms and abused males tend to express their distress more through externalizing symptoms. The findings also have clinical implications, suggesting that child and adolescent clinicians might do well to address symptoms of extreme shame or guilt in an effort to subvert the development of psychiatric symptoms, particularly in traumatized youth. Moreover, Sable, Danis, Mauzy, and Gallagher (2006) found that shame and guilt were barriers to the reporting of sexual assault in college students; shame and guilt may play similar roles in maltreated children.
The nature of the sample recruited for this study has both negative and positive implications. On one hand, finding support for hypotheses derived from our developmentally based psychoneurological model in a relatively advantaged nonclinical sample testifies to the power of these relationships in a sample with access to environmental protective factors that are not typically available to severely maltreated children (Garmezy, 1991). On the other hand, inclusion of a higher risk sample would have provided additional confirmation of the generalizability of the proposed pathways between various levels of maltreatment and developmentally based psychoneurological outcomes.
Like most studies, the present study has limitations that point to the need for future research. For example, our version of the widely used childhood maltreatment measure included only physical and psychological maltreatment from parents to child. Other forms of childhood maltreatment, including neglect, sexual trauma, witnessed violence between parents, sibling and peer aggressions, and abuses by authority figures outside the home, are potential areas for future research. Future tests of the model might consider the extent to which social class and other demographic variables moderate the relationships described in our current model and the extent to which gender differences vary by culture.
The risk of recall bias in the use of CTS might be considered another limitation, and indeed has been identified as a limitation in at least one critical review of literature analyzing studies of childhood maltreatment as a predictor of intimate partner violence (Gil-Gonzalez, Vives-Cases, Ruiz, Carrasco-Portino, & Alvarez-Dardet, 2008). However, the CTS has been administered numerous times in studies all around the world and has gained consistent support for its validity. Given that the findings of this study are largely consistent with the predictions of the conceptual model, this suggests that recall bias is not a unique problem for this study and does not call the findings of this study into question.
Another limitation of the project was its technical inability to specify and assess dysfunctions in particular limbic areas or other areas such as the prefrontal cortex. Childhood emotional maltreatment has been found to be linked to changes in the medial prefrontal cortex (mPFC) morphology. In addition, child emotional maltreatment has been linked to amygdala hyperactivity and increased risk for the development of psychopathology (van Harmelen et al., 2014). Future research should use imaging techniques and physiological instruments to confirm limbic dysfunction through direct assessments of the brain. Moreover, resilience is a relatively new area of research, and multilevel analysis may be needed to understand the complex phenomena that determine individual levels of resilience and their relevance to various psychiatric disorders.
Despite these limitations, these findings provide a basis for some optimism regarding the development of individuals who have been maltreated in childhood. Even if maltreatment has the power to affect neurological functioning, the development of resilience can help counter the long-term negative effects of maltreatment. Indeed, the findings of this study may have implications for health care professionals. The mediating role of resilience suggests that treatment of individuals who have experienced childhood traumas should focus on the psychological resources available to the individual in addition to his or her vulnerabilities.
Footnotes
Authors’ Note
The authors of this article would like to acknowledge Victoria Guskiewicz, Kimberly Roemer, and Kyle Shields of Merrimack College for their contribution in editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Author Biographies
![]() , and monthly e-newsletter, Choosing peace for good.
, and monthly e-newsletter, Choosing peace for good.