
Abstract
The present study examined the working alliance, as measured by the full-length Working Alliance Inventory (WAI), and its association with psychopathy, treatment completion, and recidivism in a sample of 111 incarcerated adult male sexual offenders. The men completed the WAI 3 months into their treatment program, while psychopathy was measured via file-based ratings of the Hare’s Psychopathy Checklist–Revised (PCL-R), and outcome data were collected via the Canadian Police Information Centre. The majority (85%) of high PCL-R scoring men (PCL-R 25+) successfully completed their treatment program, and by and large, the men demonstrated strong working alliances with their primary therapists. The WAI scale components showed differential associations with the structural features of psychopathy. Specifically, the Affective facet was significantly associated with weaker Bond scores, while the Lifestyle facet was associated with lower Task scores; these results were upheld after controlling for scores on the other PCL-R facets. Strength of alliance, however, was not significantly associated with any recidivism outcomes, irrespective of controls for psychopathy. Implications for the treatment of offenders with high levels of psychopathic traits are discussed in light of extant findings and unique features of the therapeutic alliance.
Psychopathy is a serious personality disorder that is defined by a constellation of behaviors and personality characteristics including egocentricity; impulsivity; irresponsibility; shallow emotions; lack of empathy, remorse, and guilt; pathological lying; manipulation; and the persistent violation of social norms and expectations (Cleckley, 1976; Hare, 1993, 2003). With such defining attributes, it is perhaps unsurprising that the treatment of psychopathy has historically been greeted with therapeutic pessimism (Salekin, 2002; Wong & Hare, 2005). Indeed, research has demonstrated offenders with psychopathic traits to have high rates of treatment noncompletion (Ogloff, Wong, & Greenwood, 1990; Olver & Wong, 2011), to have a larger and greater number of criminogenic needs (Olver & Wong, 2009; Simourd & Hoge, 2000), to show low motivation and treatment gain (Ogloff et al., 1990). Moreover, inappropriate interventions with offenders with psychopathic traits may even be associated with increased recidivism (Rice, Harris, & Cormier, 1992).
In the past 10 to 15 years, the doctrine that “nothing works” seems to be slowly shifting to one of “what works?” for offenders with prominent features of psychopathy. Simourd and Hoge (2000) noted that scrutiny of early psychopathy treatment studies demonstrated that few adhered to evidence-informed principles (e.g., risk, need, and responsivity) for modifying criminal behavior with offender populations. Salekin (2002) concurred in his first systematic review of the psychopathy treatment literature, noting that many early studies featured antiquated programs and also lacked a psychometrically tenable operationalization of psychopathy (see also D’Silva, Duggan, & McCarthy, 2004); however, when considering the balance of outcomes examined, such as reduction in criminal behaviors or in psychopathic characteristics more generally, there was little basis for ruling psychopathy to be an untreatable syndrome. Salekin, Worley, and Grimes (2010) have since updated this work and have noted in recent years for there to be an increase in evidence-informed cognitive behavior therapy (CBT)-based programs, use of a reliable operationalization of psychopathy such as the Psychopathy Checklist–Revised (PCL-R; Hare, 1991, 2003) or its variants, and examination of salient markers of progress such as reductions in recidivism.
Psychopathy and the Therapeutic Alliance
For treatment to work, clients first need to be engaged (Miller & Rollnick, 2002). Over one hundred years ago, Freud suggested that the transference in the client–therapist psychotherapy relationship was of critical importance to achieving effective results (Horvath, Gaston, & Luborsky, 1993). Since Freud, the notion of a working alliance has evolved and its importance in therapy has strengthened (Weissmark & Giacomo, 1998), such that it is almost axiomatic that the relationship between client and therapist is an important predictor of therapeutic success regardless of therapeutic modality or client characteristics (Castonguay, Constantino, & Holtforth, 2006; Horvath et al., 1993). Although Carl Rogers (1951) did not formally use the term alliance, he posited that therapist congruence, empathy, and unconditional positive regard were critical in driving therapeutic outcomes; the relationship, rather than technique, prevails (Horvath, 2000). Bordin (1994) subsequently made the case that successful therapeutic outcomes depend on a collaborative relationship between client and therapist; that the working alliance “is what makes it possible for the patient to accept and follow treatment faithfully” (Bordin, 1980, p. 2, as cited in Horvath & Greenberg, 1989). The working alliance does not in itself promote change, but rather, it provides the impetus to change through specific therapeutic strategies (Horvath & Greenberg, 1989).
In the language of effective correctional treatment (Andrews & Bonta, 2010), establishing a sound working alliance epitomizes the application of the responsivity principle, that is, adapting treatment in a flexible and sensitive manner to maximize client engagement. Indeed, DeSorcy, Olver, and Wormith (2016) found that stronger working alliances were associated with increased treatment completion and length of stay in a sample of 423 treated sexual offenders. High-risk offenders, however, (particularly those with prominent psychopathic features) often display characteristics that would not seem to be conducive to establishing strong therapeutic alliances. Consider characteristics such as emotional shallowness, selfishness, or an incapacity for remorse; individuals high in psychopathy are typified by difficulties forming strong relational ties (Hare, 1993, 2003). It is perhaps not surprising that high-risk, high psychopathy offenders are at risk for treatment noncompletion (Olver, Stockdale, & Wormith, 2011); a candidate reason for this may be difficulty forming therapeutic bonds. This idea was supported by Olver and Wong (2011) who found, in a sample of 154 treated sex offenders, those men who demonstrated callous and unemotional traits (i.e., high scores on the PCL-R Affective facet) had the highest rates of attrition. They posited that individuals who exhibited these traits were less likely to be able to form strong therapeutic bonds with their treatment providers and were likely viewed by treatment staff as callous and unemotional, aloof, and cold. Attempts to instill empathy or caring in these individuals are likely to fail and could ultimately lead to termination of treatment; however, the quality of alliance remains no less critical and arguably this can have important implications for treatment outcome.
Therapeutic Responses of Sexual Offenders With Psychopathic Traits
A growing literature has examined sex offender treatment outcomes among sexual offenders with and without high levels of psychopathic traits. Nearly 20 years ago, in a sample of 280 federally incarcerated sex offenders from the Warkworth Sexual Behavior Clinic (WSBC), Seto and Barbaree (1999) found that men scoring high on a measure of positive treatment behavior and 15 or higher on the PCL-R were 4 times more likely to violently recidivate than other offender groups. The authors suggested that individuals with higher PCL-R scores may have been more adept at manipulation and exploiting others or that they may have learned these skills in treatment, which were then used to commit new, more serious crimes in the community. There were important shortcomings in this study, however, including use of a low PCL-R cut score to identify psychopaths, short follow-up (32 months), and use of alternative information sources from Canada’s national criminal record database (Canadian Police Information Centre [CPIC]) to obtain recidivism data. Barbaree (2005) followed up with the same sample of sex offenders with an extended follow-up time and more complete recidivism data; in this instance, there were no differences in recidivism rates between psychopathic men who fared well in treatment and those who did not. Langton, Barbaree, Harkins, and Peacock (2006) extended this work on a sample of 418 sex offenders treated through the WSBC, using a 5-year follow-up, CPIC outcome data, and PCL-R cut score of 25. In contrast to earlier WSBC investigations, high PCL-R men exhibiting positive treatment behavior had significantly lower rates of sexual reconviction than similarly high-scoring men who displayed negative treatment behavior.
Elsewhere, Looman, Abracen, Serin, and Marquis (2005) examined treatment outcome among high psychopathy sexual offenders who attended the Regional Treatment Centre’s high-intensity sex offender program in Ontario, Canada. High PCL-R scoring men who were evaluated as having reduced their risk from sex offender treatment had lower rates of violent failure than those who had similarly high PCL-R scores but were evaluated as not having made such risk reduction. Finally, Olver and Wong (2009) examined the association of psychopathy, treatment dropout, change, and sexual/violent recidivism in a sample of 154 treated sex offenders who attended the Clearwater High Intensity Program in Saskatoon, Canada. Although psychopathy continued to be a robust predictor of recidivism, most high PCL-R scoring men completed treatment (73%); in addition, those high psychopathy men who completed treatment also had significantly lower rates of violent recidivism than noncompleters with similarly prominent psychopathic features. Moreover, positive treatment change, corresponding to risk reduction, was significantly associated with decreased sexual and violent recidivism after controlling for baseline risk and PCL-R score. The researchers suggested that this may be a result of a particular sex offender treatment program whose mandate was to pay particular attention to responsivity issues with moderate to high risk-need offenders. Although skepticism undoubtedly abounds when it comes to the treatment of high psychopathy sexual offenders, there is a small but growing body of empirical literature to suggest there may be some room for cautious optimism.
Present Study
Logic would dictate that offenders with prominent psychopathic traits would have difficulty forming the bond that is necessary to develop a strong positive working alliance. According to Bordin’s theory of the working alliance, all three elements including the tasks, bonds, and goals are required to form a positive therapeutic relationship. Given that individuals with prominent psychopathic traits are limited in their capacity to feel remorse, guilt, or empathy, often appear satisfied with themselves where they see little wrong with their attitudes and behaviors, and suffer little personal distress, forming a positive bond with a therapist seems unlikely. Rather, such individuals are often expert at manipulating and exploiting others, the antithesis of the qualities necessary to form a strong bond with people. Nonetheless, the relationship between the therapist and offender must remain respectful and professional in order to make any progress (Wong & Hare, 2005).
Building off previous working alliance research on a sample of treated sexual offenders who attended the Clearwater High Intensity Sex Offender Program, the present study extends this past work through examining the association of the working alliance, measured by the Working Alliance Inventory (WAI), with features of psychopathy in a subsample of offenders rated on the PCL-R. Research to this point has yet to examine the association of different constellations of psychopathic traits (e.g., interpersonal, affective) to aspects of the working alliance, or the relative linkages of psychopathy and the alliance to outcome. Thus, associations of the working alliance to sexual offender treatment completion and recidivism as a function of psychopathy are further examined.
Method
Participants
Participants included 111 adult male federal sexual offenders admitted to the Regional Psychiatric Centre (RPC), a multilevel security correctional treatment facility in Saskatoon, Saskatchewan, Canada, to participate in the Clearwater Sex Offender Program. The sample is a subset of approximately one quarter of admissions to the Clearwater Program between 1994 and 2005 (N = 427). All men were serving sentences of at least 2 years and are thus a responsibility of the Correctional Service of Canada (CSC), Canada’s federal correctional department. Approximately half (50.5%) of the sample was White, 47.4% self-identified from one of three ancestral Indigenous groups (First Nations, Métis, Inuit), and 1.8% was Black. The mean age of the sample at program admission was 37.0 years (SD = 10.5). Roughly half the sample (50.5%) was single and never married, 37.8% were in a current marital or common law relationship, and 20.7% were divorced or separated. Overall, 97.3% had an index conviction for a sexual offense, while the remaining 2.7% did not have an index sexual conviction but had prior histories of sexual violence. The average sentence length for individuals with a determinate sentence (n = 106) was 6.2 years (SD = 4.1), while five participants were serving life sentences.
Clearwater Sex Offender Program
The Clearwater Sex Offender Program has historically been offered as a high-intensity sex offender treatment program at the RPC (see Olver & Wong, 2013, for a detailed description of the program). The program’s mission has been to develop and provide effective and efficient treatment services for moderate-to-high-risk sexual offenders. Services are delivered through a multidisciplinary treatment team that includes nurses, psychologists, psychiatrists, social workers, and parole officers among other personnel. The program endeavors to follow Andrews and Bonta’s (2010) risk–need–responsivity (RNR) principles through appropriate selection of clientele and treatment dosage (risk principle), targeting criminogenic needs (need principle), and exercising flexibility in service delivery while following a general CBT model. Patients receive approximately 15 to 20 hours of clinical contact per week through group and individual treatment. Program participants are further provided with opportunities for educational upgrading and learning life and employment skills and to address interpersonal needs (e.g., attitudes, values) as appropriate. As per the responsivity principle, the Clearwater Program aims to attend to specific responsivity considerations such as cultural factors, low literacy and cognitive delay, and treatment readiness and motivation whenever possible. At the time of data collection, Clearwater was a 48-bed unit and programming lasted from 6 to 9 months, adapted to the needs of the individual. Previous Clearwater Program treatment outcome research has demonstrated successful program completion to be associated with reductions in sexual recidivism relative to comparable untreated controls (Nicholaichuk, Gordon, Gu, & Wong, 2000; Olver, Wong, & Nicholaichuk, 2009).
Measures
PCL-R
The PCL-R (Hare, 1991, 2003) is a 20-item symptom-construct rating scale designed to assess psychopathy. Items are rated on a 3-point scale of 0 (absent), 1 (maybe, possibly present), and 2 (present). The items have traditionally been arranged into two correlated factors, with Factor 1 assessing the interpersonal-affective characteristics of psychopathy and Factor 2 the chronic irresponsible lifestyle and antisocial features. Recent research has generated support for a four-factor model of PCL-R–measured psychopathy which we use in the current study: Interpersonal (e.g., superficiality, deceitfulness), Affective (e.g., callousness, lack of remorse), Lifestyle (e.g., impulsivity, irresponsibility), and Antisocial (e.g., early behavior problems, poor behavior controls). Total scores range from 0 to 40 with scores of 25 (recommended for file-based ratings) or 30 (file plus interview) being used to characterize psychopathy (Wong, 1988). Several meta-analyses have demonstrated the predictive accuracy of the PCL scales for general and violent recidivism (Leistico, Salekin, DeCoster, & Rogers, 2008), sexual violence (Hanson & Morton-Bourgon, 2005), and institutional misconduct (Walters, 2003).
WAI
The long form of the WAI (Horvath, 1981; Horvath, 1994; Horvath & Greenberg, 1986, 1989), used in the present study, is a 36-item self-report measure designed to assess the strength and quality of the therapeutic relationship that develops between client and therapist. The instrument is grounded in Bordin’s (1979) model featuring the bond that develops between the client and therapist as well as the mutually agreed upon goals and tasks of therapy (Martin, Garske, & Davis, 2000); the WAI is thus comprised of three subscales: Task, Bond, and Goals. Each item is rated on a 7-point scale ranging from 1 (never) to 7 (always). Scores are generated by summing the items for the three subscales and the total score. With total scores ranging from 36 to 252, higher scores indicate more positive ratings and thus a stronger alliance. Three rater versions of the measure are available: client, therapist, and observer’s perspective. In the current study, the “client” refers to the offender participating in sexual offender treatment, while the “therapist” refers to the client’s primary therapist; the present study utilizes clients’ ratings of the alliance on the self-report version as it was this version of the tool that was used by the treatment program. The WAI is the most frequently used and prolifically researched measure of the therapeutic alliance (Skeem, Louden, Polaschek, & Camp, 2007). Horvath and Greenberg (1989) reported reliability estimates based on item homogeneity indexes that range from r = .85 to r = .93 and a scale alpha value of .93. Psychometric research also supports the convergent and discriminant validity of the tool (Horvath, 1994). WAI research has demonstrated the working alliance to have a positive impact on outcome and that a strong alliance between client and therapist facilitates engagement, trust, and mutual agreement on treatment objectives (Horvath & Greenberg, 1994).
Outcome Variables
Treatment completion
Program start and end dates were recorded to obtain the length of time in treatment for each offender. Whether or not the individual successfully completed the treatment program was explicitly stated in relevant fields on CSC’s national electronic file system, the Offender Management System (OMS). Reasons for noncompletion were typically provided in the final treatment summary. Treatment noncompletion was coded in a binary manner (0 = completer; 1 = noncompleter). As per Wormith and Olver (2002), the reason for noncompletion was also recorded, including whether it was client generated (e.g., low motivation and decided to withdraw), system generated (e.g., granted release prior to completion), or program generated (e.g., discharge for disruptive behavior).
Recidivism
Recidivism was operationalized as any conviction for a new offense following release to the community post program. Three recidivism outcomes were coded in a binary (1 = recidivism, 0 = no recidivism) manner. Sexual recidivism included any new conviction for a sexually motivated offense (e.g., sexual assault, sexual touching, exposure). Violent recidivism included any conviction involving threats or use of force upon a victim (e.g., robbery, nonsexual assault), including sexual offenses. General recidivism included a new conviction for any new offense, violent or nonviolent.
Procedure
Research ethics approval was obtained from the CSC and the University of Saskatchewan’s Behavioural Research Ethics Board. Permission to access offender records for research purposes was granted by these agencies in lieu of obtaining formal consent from each individual participant, given the archival nature of the project and the fact that most (if not all) had left the RPC several years prior and were no longer under CSC jurisdiction. The first author was provided with a list of men who had completed the WAI, which was done voluntarily approximately 3 months following their admission to the Clearwater Program. In so doing, the men were instructed to evaluate their relationships with their primary therapists. WAI subscale and total scores were recorded and entered electronically into a database by RPC research staff. Offender demographic and treatment completion information were gathered from OMS, while recidivism data were gathered via the CPIC by the first author. As noted previously, approximately one quarter (n = 111) of the 427 Clearwater Program admissions was sampled to obtain PCL-R ratings. Thirty-six of these cases had PCL-R ratings from a previous study (Olver & Wong, 2009, 2011), while the remaining 75 cases were randomly selected for inclusion in the present study to be rated on the PCL-R.
Planned Analyses
We conducted five sets of planned analyses. First, to examine the overall strength and quality of the alliance for high PCL-R scoring offenders, we performed simple bivariate comparisons of men scoring at or above or below the 25-point cutoff on the PCL-R on WAI Task, Bond, Goal, and total scores via MANOVA. We also computed standardized mean differences (Cohen’s d) on the WAI scales between the two groups. Second, to examine whether different components of the psychopathy construct were associated with the alliance in different ways, we computed zero-order bivariate correlations between scores on the four PCL-R facets and the WAI scales. To examine unique associations between PCL-R facet scores and the WAI, controlling for scores on the other facets, we computed semipartial correlations, that is, correlations between partialled facet scores and unpartialled WAI scores. To do this, we regressed a given facet score on the three other PCL-R facets, retained the residual (representing unique variance associated with a given facet), and correlated the PCL-R residual facet score with each WAI scale and subscale. All correlational analyses, zero order and semipartial, were performed using a one-tailed test given that we are making directional predictions, anticipating higher PCL-R facet and total scores to be associated with weaker working alliances and thus negative correlations.
Third, we examined the association of psychopathy to working alliance as a function of Indigenous ancestry through MANOVA. DeSorcy et al. (2016) found that men of Indigenous ancestry scored significantly lower than non-Indigenous men on the Bond scale of the WAI total. As such, the present investigation sought to examine whether differential associations may exist between working alliance and psychopathy among Indigenous and non-Indigenous men, through examination of the interaction terms in MANOVA.
Fourth, we examined rates of attrition for high and low PCL-R scoring men as well as examining the prediction of attrition specifically as a function of PCL-R and WAI total scores. Research by Olver and Wong (2011), on an overlapping sample, demonstrated PCL-R total and facet scores to predict attrition, while DeSorcy et al. (2016) found WAI total and subscale scores predicted attrition on the larger sample of 427 offenders. Thus, the present study aimed to build on this through examining the incremental associations of PCL-R and WAI scores to attrition through hierarchical logistic regression analyses, in which these predictors were entered in this order in separate steps, followed by the interaction term in the third step. The addition of the interaction term would enable the examination of whether rates of attrition differ among men with different levels of psychopathy as a function of WAI score; for instance, do high PCL-R scoring men with stronger alliances evince lower rates of attrition than psychopathic men with weaker alliances? Owing to the relatively small sample size and the low rates of attrition in the study (see Results for details), these predictors were analyzed in continuous manner for all regression analyses.
In turn, our fifth and final set of analyses examine the association of psychopathy and working alliance to postprogram recidivism through hierarchical logistic regression analyses using a similar ordering of predictors, including the interaction term, as outlined previously. DeSorcy et al. (2016) found WAI scores to be weak predictors of recidivism in the overall sample, while Olver and Wong (2009) found high PCL-R scorers who completed sex offender treatment had lower rates of violent recidivism than similarly scoring men who did not. As such, the present study intended to extend these findings to ascertain whether psychopathy and working alliance differentially predict recidivism, or perhaps interact in the prediction of postrelease outcomes; for instance, do men scoring higher on the PCL-R but who have stronger alliances have lower rates of recidivism outcomes than similar PCL-R scoring men with weaker alliances?
Results
Psychopathy and Working Alliance
Individuals were divided into high (25+) and low (<25) PCL-R total score groups and compared on the basis of their WAI subscale and total scores (Table 1). The results of a one-way MANOVA demonstrated no significant overall main effect for psychopathy group membership, F(3, 107) = 0.59, p = .624, or differences between high and low PCL-R scoring men on the WAI Task, Bond, Goal, or total scores. Cohen’s d showed generally small in magnitude differences between high and low psychopathy groups on WAI score, with the highest (albeit nonsignificant) difference found on the Bond scale (d = .19), or about one fifth of a standard deviation. Dimensional PCL-R total scores were also not significantly correlated with WAI total or subscale scores. The relatively high WAI total and subscale scores are further worth noting. On average, the men scored between 5 and 6 points per scale item (out of a maximum 7) for each WAI index, with each of the three subscales containing 12 items. This would indicate generally strong self-reported working alliances, even for high PCL-R scoring sexual offenders.
MANOVA: PCL-R Psychopathy Group Comparisons on WAI Measures.
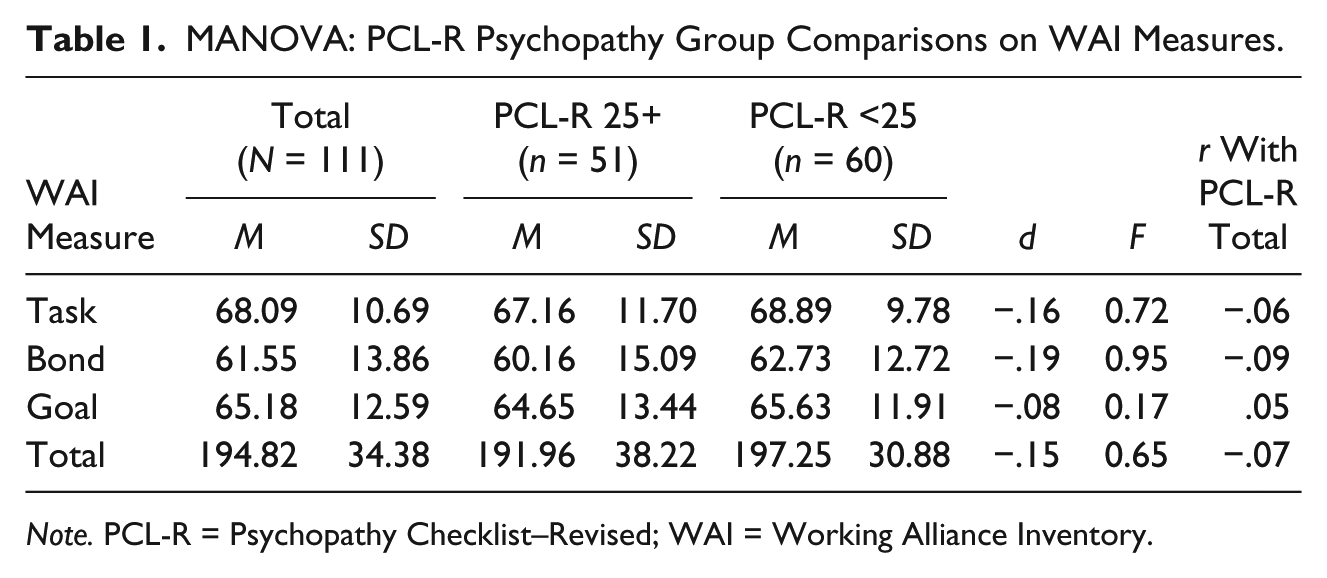
Note. PCL-R = Psychopathy Checklist–Revised; WAI = Working Alliance Inventory.
The association of psychopathy and working alliance was examined in finer grained detail through correlating the PCL-R facet scores with each WAI index (Table 2). Zero-order correlations demonstrated that the Affective facet was significantly correlated with the WAI Bond, Goal, and total scores, while the Lifestyle facet was significantly correlated with Task, Goal, and total scores. Semipartial correlations, controlling for all other PCL-R facet scores, demonstrated similar patterns of associations with WAI score. Controlling for the three other facets, the Affective facet was significantly uniquely associated with lower WAI Bond, Goal, and total scores, while the Lifestyle facet was uniquely associated with lower WAI Task, Goal, and total scores. No other semipartial correlations were significant.
Zero-Order and Semipartial Correlations Between WAI and PCL-R Facet Scores.
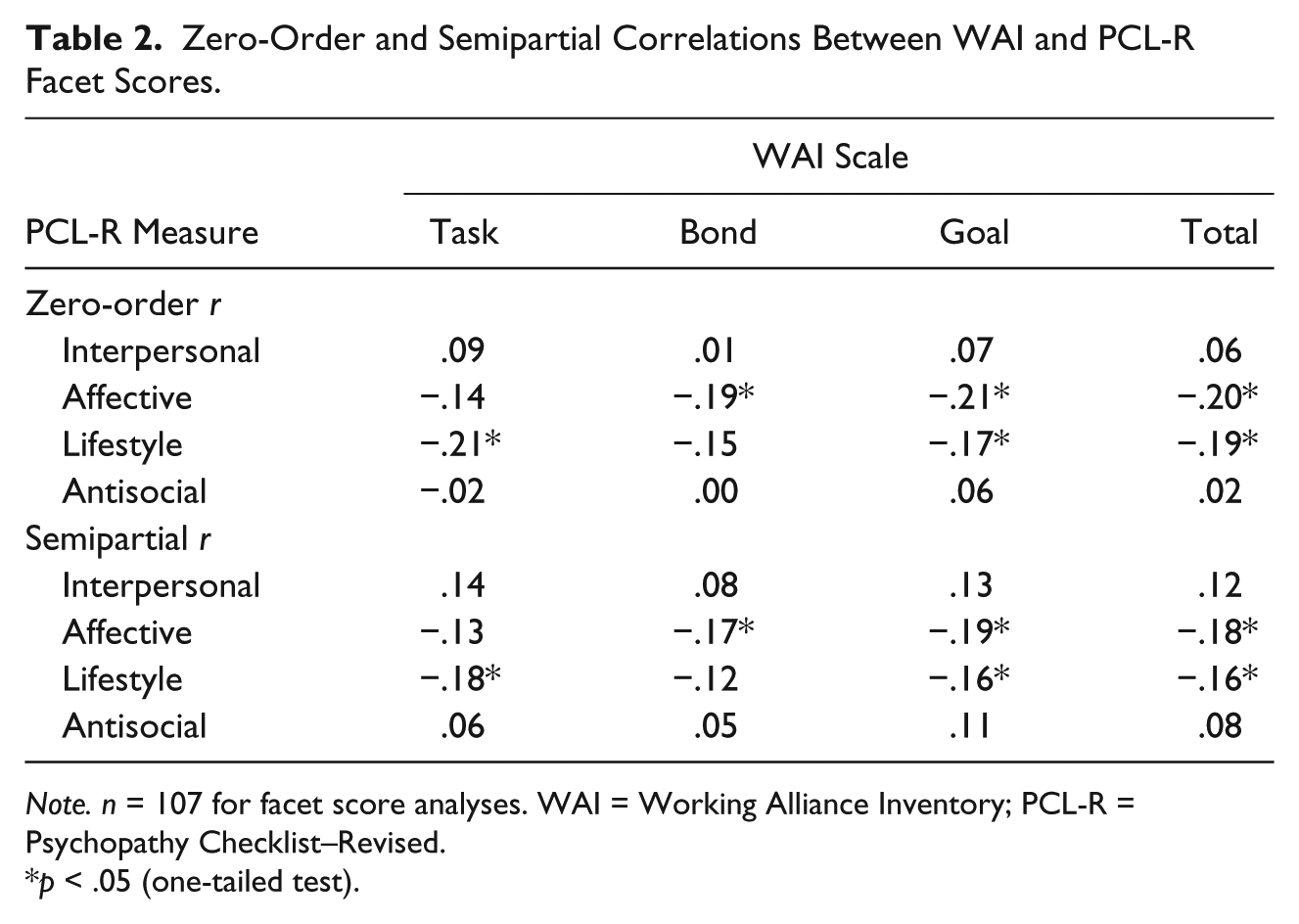
Note. n = 107 for facet score analyses. WAI = Working Alliance Inventory; PCL-R = Psychopathy Checklist–Revised.
p < .05 (one-tailed test).
Psychopathy, Indigenous Ancestry, and Working Alliance
The next set of analyses sought to examine whether PCL-R–measured psychopathy may have a different association with indicators of working alliance as a function of Indigenous ancestry. A 2 (high vs. low psychopathy) × 2 (Indigenous vs. non-Indigenous ancestry) MANOVA was conducted examining differences among four groups on the WAI measures (see Table 3). The main effects for psychopathy group membership, F(3, 105) = 0.53, ns, and Indigenous ancestry, F (3, 105) = 0.53, ns, were not significant, although the omnibus interaction term for the model trended toward significance at F(3, 105) = 2.47, p = .066. Table 3 reports the results for the interaction of psychopathy and ancestry and the WAI means and standard deviations within each of the subgroups. As seen in Table 3, differences in working alliance between high and low PCL-R scoring men were higher among non-Indigenous men, although none of the interaction terms attained significance.
MANOVA: Group Comparisons on WAI Measures as a Function of PCL-R Psychopathy and Indigenous Ancestry.
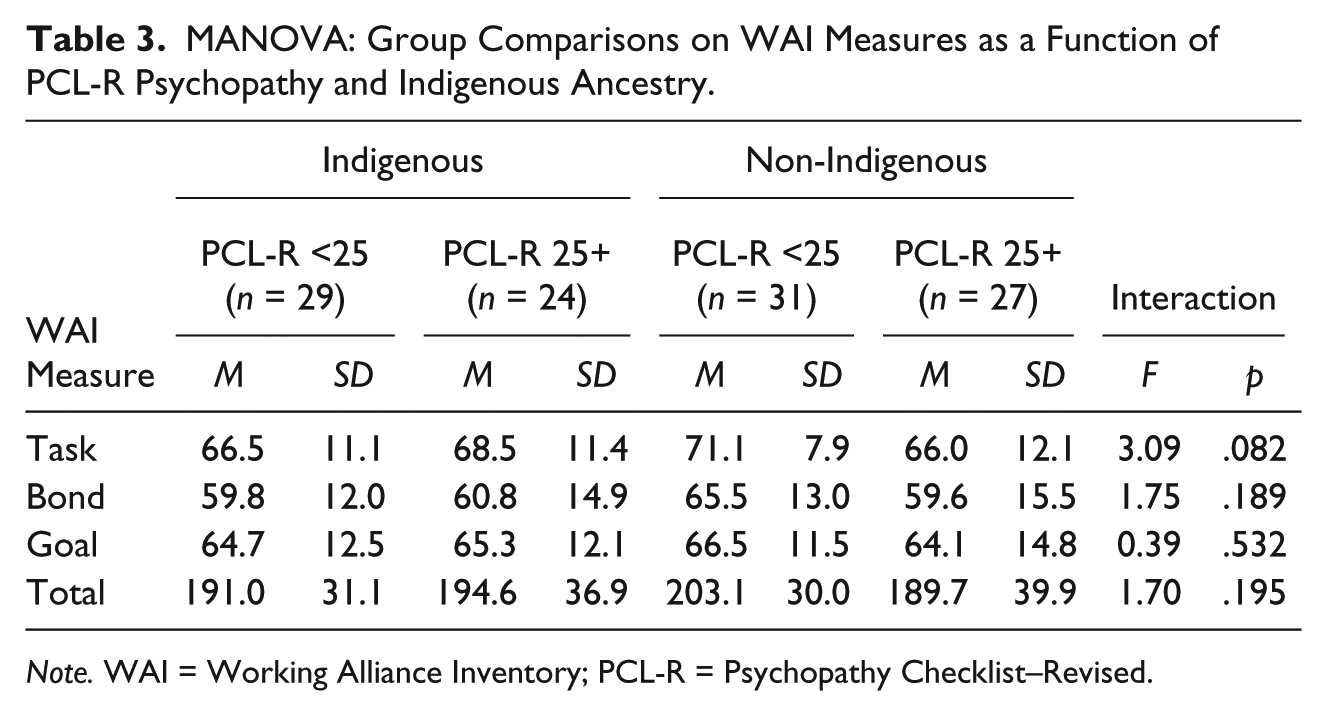
Note. WAI = Working Alliance Inventory; PCL-R = Psychopathy Checklist–Revised.
Psychopathy, Working Alliance, and Treatment Outcome
Linkages between psychopathy, working alliance, and treatment outcome (treatment completion and recidivism) were examined through hierarchical logistic regression analyses.
Sex offender treatment noncompletion
The sample demonstrated a low rate of sex offender treatment noncompletion (10.8%), with 89.2% (n = 99) of the men successfully completing the Clearwater Program. Of the 12 cases that did not successfully complete treatment, six were attributable to poor participation and progress, two were transferred out of the institution, two were early releases, one withdrew, and one was suspended. The average length of treatment stay was 191 days (SD = 54.9). In all, 84.3% of men with PCL-R scores of 25 or higher completed the program (15.7% did not complete), while 93.3% of men scoring below 25 similarly completed (6.7% did not complete); this difference was not significant, χ2(1, N = 111) = 2.33, p = .127, ϕ = .15. PCL-R total score was entered in the first step into the logistic regression equation, followed by WAI total score in the second step, and the PCL-R × WAI interaction in the third step. As seen in Model 1 of Table 4, none of these predictor variables significantly uniquely predicted noncompletion. As such, high psychopathy offenders, irrespective of quality of working alliance, were not significantly less likely to complete treatment.
Hierarchical Logistic Regression Analyses: Psychopathy and Working Alliance Prediction of Treatment Noncompletion and Recidivism.
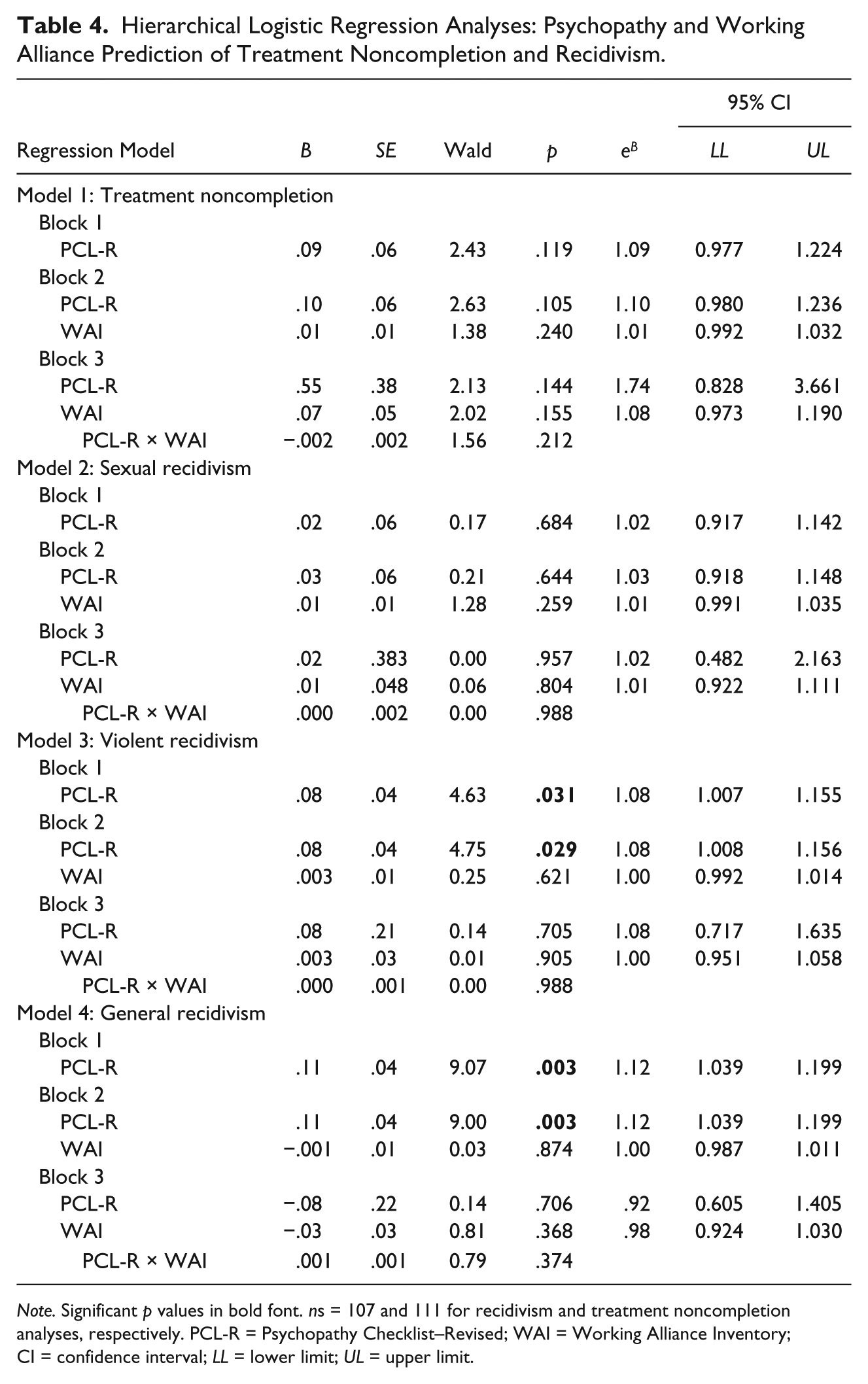
Note. Significant p values in bold font. ns = 107 and 111 for recidivism and treatment noncompletion analyses, respectively. PCL-R = Psychopathy Checklist–Revised; WAI = Working Alliance Inventory; CI = confidence interval; LL = lower limit; UL = upper limit.
Recidivism
The men were followed up for a mean 10.4 years (SD = 3.1), during which 10 individuals were convicted for a new sexual offense (9.3%), 46 (43%) were convicted for any new violent offense, and 63 (58.9%) were convicted for any new offense. The association of psychopathy and working alliance to these three outcomes posttreatment were examined in Models 2 to 4 (see Table 4). As above, PCL-R score was entered in the first step, followed by WAI total score in the second step, and PCL-R × WAI interaction in the third step. Psychopathy, working alliance, and their interaction did not significantly predict sexual recidivism (Model 2) in any of the steps. PCL-R total score significantly uniquely predicted increased violent and general recidivism (Models 3 and 4, respectively), with and without controlling for the WAI; their interaction, however, did not predict either recidivism outcome. In sum, although psychopathy predicted broader recidivism outcomes, consistent with past research, quality of working alliance did not significantly influence this association with outcome.
Discussion
The present study examined the association of PCL-R–measured psychopathy to the quality of working alliance between client and therapist (measured by the full-length WAI) in a Canadian sample of 111 federally incarcerated sexual offenders who attended the Clearwater High Intensity Sex Offender Program.
Psychopathy and Working Alliance: Implications for Treatment Retention and Recidivism
By and large, the sample demonstrated strong self-reported working alliances as evinced by high total and subscale scores, equating to an average item value of about 5 or 6 out of 7. Interestingly, this was observed across subgroups of high psychopathy and low psychopathy men. Evidently, even high PCL-R scoring men demonstrated the capacity to establish working alliances with their primary therapist within the context of sex offender treatment. It is anticipated that with mean differences between high and low psychopathy men of approximately one fifth to one sixth of a standard deviation across most of the WAI indexes, these may have attained significance with a larger study sample; still, this does not change the fact that the magnitude of difference is ultimately small.
Although there are important limitations to the use of self-report, such as demand characteristics when a patient is placed in the role of evaluating the quality of relationship with their primary therapist, these results are compelling when interpreted in conjunction with the low treatment noncompletion rates from the sample as a whole, and among psychopathic offenders in particular. Indeed, 85% of men scoring 25 or higher on the PCL-R successfully completed the Clearwater Program, while 93% of the remainder of the sample similarly completed; given the high retention rate, psychopathy did not significantly predict treatment attrition in the present study. This high retention rate (see meta-analysis by Olver et al., 2011), regardless of psychopathy status, arguably speaks to the Clearwater Program’s attention to the responsivity principle, including a commitment to retain challenging clientele in treatment. It is further possible that there may be external contingencies or forces at work as well, such as positive consequences for completion (e.g., granting of conditional release).
A similar study by Walton, Jeglic, and Blasko (2016) found no significant relationship between PCL-R scores and total WAI scores for either client or therapist ratings, although when ratings across two time points were averaged, the PCL-R scores were significantly negatively correlated with the Bond scale; however, associations between the four PCL-R facets and working alliance were not examined nor were linkages to outcome. The psychopathy construct, as operationalized by the PCL-R, is very broad and is underpinned by four intercorrelated domains that comprise it. These domains may have differential associations with criteria of importance, which is precisely what the present study found. Examination of PCL-R facet scores showed that ultimately Affective facet scores had the strongest and most consistent inverse associations with WAI total and subscale scores, followed by the Lifestyle facet; neither of the remaining PCL-R facets or the total score had significant linear relations with working alliance.
An intriguing finding was that high Affective facet scores were associated with weaker therapeutic bonds, as measured by the Bond scale of the WAI; it was the only PCL-R facet significantly correlated with this WAI domain, and it remained the strongest unique predictor after controlling for scores on the three other facets. This association makes sense conceptually in a number of respects, as ultimately the bond component of the alliance is a domain in which high psychopathy men could be expected to struggle (Olver & Wong, 2011; Wong et al., 2012). Representing the callous and unemotional features of psychopathy, individuals with high Affective facet scores are unlikely to excel in developing a strong emotional connection to the therapist or to experience warmth, empathy, and compassion for others. Indeed, past research on a larger extension of this sample demonstrated Affective facet scores to be a particularly robust predictor of sex offender treatment noncompletion (Olver & Wong, 2011), and in a sample of treated violent offenders, it was uniquely associated with decreased therapeutic progress (Olver, Lewis, & Wong, 2013).
The significant linkages between the Affective facet and the Goal subscale are somewhat less intuitive. The Goal subscale represents the extent to which client and therapist have mutually agreed objectives in treatment; although the focus may vary from group to group or from session to session, generally there is an overarching understanding that the purpose of a high-intensity sex offender program is to help the individual manage their risk in order to prevent future violence, sexual or otherwise. It is possible that some men with high Affective facet scores do not see it as their responsibility to manage their own risk and take responsibility for changing their own behavior; if one perceives themselves to have few problems that require changing, it seems plausible that this could manifest in a clash over the appropriate goals of treatment. A further possible explanation is that the lack of agreement on treatment goals is simply consistent with the detachment individuals high on callous–unemotional traits experience in the therapeutic relationship. Otherwise, to admit to sharing something common with the therapist may create dissonance for emotionally detached men.
The Lifestyle facet also featured prominently in the present research and had its strongest links to lower scores on therapeutic tasks of the WAI (Task subscale). It makes sense that men exhibiting higher levels of impulsivity, irresponsibility, lack of goals, parasitism, and the like would be more likely to struggle with participating in relevant therapeutic activities in treatment. Rather, it would seem such men may be inclined not to complete homework or required therapeutic activities, fail to practice skills, and eschew constructive activity within sessions, given the features that typify the Lifestyle facet. As the goal of most treatment programs is to engender their clientele with skills to be used outside the session and ultimately incorporated into their day-to-day life to prevent relapse, such an association underscores the importance of utilizing strategies (e.g., motivational interviewing) to maximize therapeutic buy-in.
The present study may also have diversity implications. DeSorcy et al. (2016) found that men of Indigenous ancestry demonstrated weaker therapeutic bonds than non-Indigenous men as measured by the WAI and had higher rates of program attrition. Thus, it stood to reason that psychopathy may have a differential association with working alliance among Indigenous and non-Indigenous men. Although none of the group differences between high and low psychopathy scoring attained significance on the WAI, there was a pattern toward non-Indigenous, low psychopathy men scoring particularly high on the measure and its subscales compared with the other three subgroups. Tentatively, it is possible that in a program staffed by predominantly White, urban, university-educated mental health personnel, cultural and demographic similarities helped augment client ratings of the alliance for non-Indigenous men, particularly if they were not high in psychopathy. This merits further research on a larger sample to ascertain whether such differences persist to inform clinical implications for strengthening the alliance when working with persons of diversity.
Finally, WAI scores did not significantly predict any recidivism outcomes irrespective of controls for psychopathy; however, high PCL-R scores continued to significantly predict violent and general recidivism, but not sexual recidivism, consistent with extant meta-analytic findings (Hawes, Boccaccini, & Murrie, 2013). A possible reason for the lack of observed relationship may be the nature of the outcome itself—recidivism. The null findings indicate that a strong alliance did not necessarily correspond to making positive treatment gains in the form of risk reduction. If it did, then stronger alliances should predict decreased recidivism. Thus, the association between quality of alliance and treatment change merits further research.
Strengths, Limitations, and Conclusions
The present study has a number of strengths and limitations with implications for future research. In terms of strengths, the study featured prospective administrations of the WAI in the course of routine services, while the PCL-Rs were rated independently from file to prevent criterion contamination. The present study serves as one of very few examinations of linkages between the structural features of psychopathy and components of the therapeutic alliance. There are at least three shortcomings, however. First, the sample size was limited; although the cases were randomly sampled for PCL-R scoring to reduce bias, some analyses may have been underpowered owing to insufficient n, inflating the Type II error rate. Naturally, the present findings should be replicated and extended to other samples and settings. Second, the WAI was administered in a static manner, that is, at only a single time point; thus, there was no opportunity to examine possible changes in the alliance or to obtain a more temporal measure of alliance toward the end of treatment which may have also been more predictive of outcome. Future work in this area may benefit from repeated administrations of the WAI to track and measure change. Finally, the possibility of demand characteristics cannot be overlooked. It was possible that the men inflated their ratings of the alliance, given that their primary therapist also had the responsibility of evaluating the men’s treatment progress. Related to this, the WAI was also completed voluntarily by the men, and thus it is possible that such circumstances also inflated WAI ratings, decreased variance, and attenuated associations with criterion variables.
In conclusion, the relationship between the correctional client and therapist matters. A stronger alliance can translate into increased client retention and decreased attrition. Although positive working alliances did not have strong associations with reductions in recidivism in the present study, in order for correctional clients to benefit from risk reduction treatment, they need to be retained in treatment. The present findings demonstrate that having prominent psychopathic traits does not preclude the formation of a healthy working alliance or successful retention in treatment. Rather, service providers may be well advised to prioritize the task and goal components of the alliance when working with high psychopathy clientele to maximize treatment retention and gain.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.