
Abstract
Research has shown that victims of sexual assault are at a significant risk of revictimization. We use routine activity theory to predict how sexual victimization in adolescence relates to depression, substance use, and ultimately revictimization as a young adult. We frame our research within routine activity theory and predict that sexual victimization increases substance use and depressive symptoms, both of which increase the likelihood of revictimization. We test the hypotheses with three waves of data from the Longitudinal Study of Violence Against Women. Using structural equation modeling, we examine the direct and indirect effects of previous sexual victimization, depressive symptoms, and substance use on the odds of victimization during the sophomore year of college. Results suggest that sexual victimization during the sophomore year of college is predicted directly by previous sexual victimization and also indirectly through depressive symptomology, though not substance use. Although understudied in the literature, depression is shown to mediate the relationship between victimization and revictimization, and this finding is consistent with routine activity theory, as well as the state dependence perspective on revictimization. Our findings suggest that depressive symptoms, a long acknowledged consequence of sexual victimization, should also be understood as a source of revictimization risk, indicating the importance of depression screening and intervention for decreasing sexual victimization.
Sexual victimization is a common experience among adolescent women. According to national surveys, between 11% and 13% of young women aged 12 to 17 have experienced a sexual assault or forced intercourse (Hanson et al., 2008) and rates of sexual violence are consistently higher in adolescence than in any other age group (Planty, Langton, Krebs, Berzofsky, & Smiley-McDonald, 2013). Adolescent sexual victimization is also associated with increased risk of later sexual victimization—over a third of women sexually victimized in adolescence experience revictimization in college (Classen, Palesh, & Aggarwal, 2005; Gidycz, Coble, Latham, & Layman, 1993; Humphrey & White, 2000; Roodman & Clum, 2001). Findings from these studies are consistent with the larger literature that identifies previous sexual victimization as one of the strongest predictors of subsequent sexual victimization, even while controlling for other adverse events such as childhood physical abuse and neglect (Arata & Lindman, 2002; Classen et al., 2005; Gidycz et al., 1993; Nelson et al., 2002; Widom, Czaja, & Dutton, 2008).
Although it is widely acknowledged that adolescent sexual victimization places women at increased risk for young adult victimization, empirical research has not determined the mechanisms that link these victimization events (for overview, see Walklate & Clay-Warner, 2016). Several studies have examined the role of substance use in mediating victimization events, which is consistent with the strong associations between alcohol/drugs and sexual victimization (Gilmore, Stappenbeck, Lewis, Granato, & Kaysen, 2015; Mohler-Kuo, Dowdall, Koss, & Wechsler, 2004; Mouilso, Fischer, & Calhoun, 2012). There is a great deal of inconsistency in this literature, however, and many findings are based on cross-sectional or retrospective data, which precludes the establishment of time order (e.g., Arata & Lindman, 2002; Daigle, Fisher, & Cullen, 2008). Findings from the few longitudinal studies using adolescent samples are inconclusive or contradictory (e.g., Gidycz, Hanson, & Layman, 1995; Kilpatrick, Acierno, Resnick, Saunders, & Best, 1997; Raghavan, Bogart, Elliott, Vestal, & Schuster, 2004). For example, Kilpatrick et al. (1997) found that use of drugs (but not use of alcohol) mediated revictimization events, while Raghavan et al. (2004) did find support for alcohol use as a predictor of sexual victimization. In addition, research has largely failed to consider the role of depression in mediating sexual victimization events, which is surprising given the strong correlations found between depression and sexual assault (Neumann, Houskamp, Pollock, & Briere, 1996).
Identifying the mechanisms that link adolescent and adult sexual victimization is vital as doing so may lead to more effective interventions. Furthermore, understanding processes of repeat sexual victimization also contributes to the debate in the criminological literature regarding causes of revictimization more generally. This conversation focuses on whether state dependence or risk heterogeneity processes account for the high rates of revictimization. According to state dependence arguments, the victimization event itself changes either the individual or the social environment in ways that elevate future risk. According to the risk heterogeneity argument, the association between victimization events is spurious because the same underlying factors that caused the initial victimization event are also responsible for subsequent victimization experiences (see Clay-Warner, Bunch, & Mcmahon-Howard, 2016; Ousey, Wilcox, & Brummel, 2008).
We frame the issue of continuity in sexual victimization within routine activity theory (Cohen & Felson, 1979) and predict that depression and substance use mediate the relationship between adolescent sexual victimization and subsequent sexual victimization in early adulthood. We argue that depressive symptoms and substance use increase target attractiveness and exposure to motivated offenders in situations of reduced guardianship, thus facilitating revictimization. We begin by discussing routine activity theory and its implications for sexual revictimization. Then, we review the relevant empirical literature. Next, we describe our longitudinal data, measures, and analytic strategy before presenting our results.
Routine Activity Theory
Routine activity theory is a logical framework for understanding sexual revictimization. As presented by Cohen and Felson (1979), the theory proposes that crime is most likely to occur when suitable targets are in the presence of likely offenders in the absence of capable guardians. The theory contends that risk of victimization is affected by the daily activities in which one engages. There is general support for routine activity predictions, with studies finding that activities that increase one’s exposure to motivated offenders increase the likelihood of both violent and property victimization (e.g., Bunch, Clay-Warner, & Lei, 2015; Pizarro, Corsaro, & Yu, 2007; Pratt, Holtfreter, & Reisig, 2010; Tita & Griffiths, 2005).
Routine activity theory has previously been applied to sexual victimization. Schwartz and Pitts (1995) proposed that certain activities affected women’s likelihood of sexual victimization and found that, indeed, women who went out drinking more often and women who were friends of motivated offenders were more likely than other women to be sexually victimized. There is now a growing body of literature on sexual assault that is consistent with routine activity theory (Clodfelter, Turner, Hartman, & Kuhns, 2010; Fisher, Daigle, & Cullen, 2010; Lauritsen & Davis Quinet, 1995; Mustaine & Tewksbury, 2002; Schwartz, DeKeseredy, Tait, & Alvi, 2001). Activities that place women in close proximity to offenders and/or reduce their guardianship lead to greater risk of victimization (Clodfelter et al., 2010). Many of the locations in which sexual victimization of college women often occurs (e.g., bars, fraternity houses) are places in which there are few capable guardians and many potential offenders.
Researchers have not, however, tested the prediction that routine activities mediate the effects of a sexual victimization event on subsequent sexual victimization. Examining mediation is the most straightforward way to test whether—and how—changes in routine activities influence revictimization risk. Failure to test for mediation is due, in part, to the lack of longitudinal data, which is required for a true test of mediation. For example, Fisher et al. (2010) found that lifestyle factors did not differentiate single and recurrent victims of sexual violence. This finding suggests that the same routine activities that increase risk of initial sexual victimization continue to be risk factors for subsequent incidents of sexual victimization, supporting a risk heterogeneity perspective. They note, however, that they cannot dismiss the possibility that state dependence effects exist, as their cross-sectional data precluded tests of mediation (Fisher et al., 2010).
Here we argue that experiences of adolescent sexual victimization increase depressive symptoms and substance use, which increase target attractiveness and exposure to motivated offenders, while reducing guardianship. Research suggests that some offenders choose targets who have already been victimized due to perceptions that a previously victimized individual will be more vulnerable to revictimization (Farrington, 1993). This applies not only to victimization by the same offender, as other potential offenders could learn about a previous victimization through their local peer network (such as on a college campus). This argument is consistent with the state dependence perspective on revictimization (Bunch, Clay-Warner, & McMahon-Howard, 2014; Farrell, Phillips, & Pease, 1995; Ousey et al., 2008; Sparks, 1981). It is also consistent with the extant literature demonstrating that sexual victimization can bring about changes in victims’ demeanor and behavior (The White House Council on Women and Girls, 2014).
Depression as a Mediator of Sexual Victimization Events
Although research suggests that psychological states, such as self-blame, lack of assertiveness, maladaptive coping strategies, dissociation, and post- traumatic stress disorder may link victimization events (Classen et al., 2005; Filipas & Ullman, 2006; Messman-Moore & Long, 2003; Miller, Markman, & Handley, 2007), the role of depression as a mediator is understudied. This is surprising given that research consistently finds strong associations between depression and sexual victimization (Briere & Jordan, 2004; Maniglio, 2010; Neumann et al., 1996; Orava, McLeod, & Sharpe, 1996; Ouellet-Morin et al., 2015). Also, many of the factors found to mediate adolescent victimization and adult revictimization risk are, themselves, associated with depression—such as relationship difficulty and maladaptive coping (Classen et al., 2005; Filipas & Ullman, 2006; Messman-Moore & Long, 2003). A few studies have prospectively explored this relationship, albeit in a small sample of women who experienced childhood sexual abuse—not victimization as an adolescent (e.g., Waldron, Wilson, Patriquin, & Scarpa, 2015).
To establish that depressive symptomology mediates the effects of adolescent sexual assault on risk of adult sexual assault, we first examine research that demonstrates that adolescent sexual assault increases depression. Although research that examines adolescent victimization specifically is limited, there is considerable evidence that sexual victimization at any age increases risk of depressive symptoms. Kilpatrick et al.’s (2003) cross-sectional, national probability study found an increased likelihood of major depressive episodes among adolescents (ages 12-17) who had experienced sexual victimization. This study was cross-sectional and so cannot address causal ordering of sexual victimization and depression but does provide support for their association among adolescents. Weaver and Clum’s (1995) empirical review and Chen and colleagues’ (2010) meta-analysis also find a positive and significant effect of sexual abuse on a lifetime diagnosis of depression. More research is needed about how this link might be particularly strong if the sexual victimization is experienced during adolescence.
For the proposed mediating relationship to be supported, depression must also increase risk of sexual victimization. While some research specifically addresses depression as a covariate of sexual victimization in cross-sectional studies, we are unaware of longitudinal studies that examine depression as a predictor of sexual victimization. Although not examining depression directly, research suggests that having reduced risk perception, a trait often associated with depression, can be a precursor to sexual victimization (for review, see Gidycz, McNamara, & Edwards, 2006). For example, Chu (1992) studied victims of childhood sexual abuse whose dissociative and numbing symptoms from their initial trauma rendered them less able to perceive danger in their environment. This behavior increased their likelihood of experiencing sexual victimization in adulthood. If individuals do not recognize threat, they may not be able to remove themselves from a dangerous situation, thereby elevating victimization risk. Similarly, depressed affect could facilitate the “signals of vulnerability” that Lauritsen and Davis Quinet (1995) postulated make crime victims appear to be easier, more attractive targets, leading to repeat victimization. Recent research links negative affectivity, or a disposition to experiencing negative emotional states across situations and time, to victimization in the workplace (Kodellas, Fisher, & Wilcox, 2015).
Substance Use as a Mediator of Sexual Victimization Events
Like depression, substance use may increase women’s risk of sexual victimization by making them more attractive victims. Studies have shown that more than half to three quarters of college-aged adult rape victims were using alcohol or were intoxicated prior to their assault (Abbey, 2002; Messman-Moore, Ward, & Brown, 2009; Resnick et al., 2012; Testa & Parks, 1996). Alcohol and drugs inhibit cognitive and motor processes, impairing an individual’s ability to detect, recognize, escape, or resist sexual aggression (Testa & Parks, 1996). Lifestyle factors associated with substance use also provide the opportunity for increased exposure to potential perpetrators, as drinking and drug use often occurs in high-risk environments (Kilpatrick et al., 1997). In addition, predatory assailants may target women with substance use problems because they view substance use as an indication of increased vulnerability (Parks, Hequembourg, & Dearing, 2008). Abbey (2002) specifies additional pathways through which alcohol increases the likelihood of sexual assault among acquaintances including beliefs about alcohol and gender (stereotypes that men will be more powerful, sexual, and aggressive after drinking alcohol and that women are sexually promiscuous if they drink in bars), a decreased ability for women to assess and react to risk effectively when intoxicated, peer norms that provide a justification for heavy drinking and forced sex, and assailants’ reduced perceptions of responsibility.
Although research has established that substance use is associated with sexual victimization, only limited research has examined whether alcohol mediates the effect of sexual victimization in adolescence on victimization in early adulthood. Results of these few studies have produced inconsistent findings. In a prospective study of first-year college women, Mouilso et al. (2012) found that alcohol use in adolescence increased risk of sexual assault in early college, but they did not find evidence that experiencing a sexual assault increased alcohol consumption. In contrast, Testa, Hoffman, and Livingston (2010) found in their prospective study that alcohol partially mediated the effects of high school sexual victimization on victimization risk in college. They note, however, the need for additional longitudinal research testing the role of alcohol in sexual revictimization.
The Current Study
In this study, we examine the roles that substance use and depressive symptoms play in mediating the effects of adolescent sexual victimization on repeat victimization in young adulthood. We use longitudinal data, allowing us to establish causal ordering. Our focus is specifically on the effects of adolescent sexual victimization on victimization during the first 2 years of college, which is a particularly vulnerable time for women (Fisher, Cullen, & Turner, 2000; Krebs, Lindquist, Warner, Fisher, & Martin, 2007).
Consistent with previous literature, we predict stability in victimization over time (Classen et al., 2005; Roodman & Clum, 2001). Specifically, we predict that experiencing sexual victimization during adolescence will increase risk of sexual victimization during the first year of college, and that experiencing sexual victimization during the first year of college will increase risk of sexual victimization during the second year of college. We also predict that substance use and depressive symptoms will be associated with sexual victimization within time periods. That is, both substance use and depressive symptomology during one time period will be positively associated with sexual victimization during that same time period.
In our focal predictions, we examine mediation. First, we predict that depressive symptoms will mediate the relationship between sexual victimization in adolescence and young adulthood. Experiencing depressive symptomology may cause victims to display subtle signs of vulnerability, such as flattened affect, emotional numbing, delayed response to threat, and lower assertiveness (Breitenbecher, 2001; Wilson, Calhoun, & Bernat, 1999; Yeater, Treat, Viken, & McFall, 2010). Second, we predict that substance use will mediate the relationship between victimization events, an association that has been supported by some research (e.g., Grice, Brady, Dustan, Malcolm, & Kilpatrick, 1995; Kilpatrick et al., 1997) but that other studies have been unable to document (e.g., Merrill et al., 1999). Being inebriated limits one’s ability to focus on potential threats or danger cues and limits physical ability to resist perpetrators (Kilpatrick et al., 1997; Steele & Josephs, 1990). When an individual is intoxicated, he or she is also likely to be surrounded by others who are incapacitated, which reduces the ability of bystanders to engage in capable guardianship, and places individuals in close proximity to potential offenders (Armstrong & Hamilton, 2013). The logic of our mediating predictions is consistent with routine activity theory, as both depressive symptoms and substance use increase vulnerability, which increases target attractiveness.
Method
Data
To test our hypotheses, we use data from the Longitudinal Study of Violence Against Women (LSVAW), which was designed to investigate the developmental antecedents of physical and sexual violence against young women (White & Humphrey, 2002). This is a panel study of female college students at a southeastern state university from 1990 to 1995 that is available through the National Archive of Criminal Justice Data (NACJD). The researchers administered the survey to all students who attended the first day of student orientation and simultaneously contacted by phone all first-year students who did not attend. Approximately, 84% of the class provided usable surveys, and follow-up retention rates for Waves 2 and 3 were 89% and 84%, respectively. At the end of each spring semester, all students (including those who had withdrawn from the university or lived out of town) were invited to complete a follow-up survey on-campus or via telephone or mail and received payment for their time. The current study utilizes three waves of data: Wave 1 was collected at the very beginning of the freshman year of college, Wave 2 was collected at the end of the freshman year, and Wave 3 was collected at the end of the sophomore year of college. Most of the sample was between the ages of 17 and 19 at Wave 1 (37% were 17 years old, 47% were 18 years old, and 14% were 19 years old). This means most of the respondents were around 19 years old at Wave 2 and around 20 years old at Wave 3. The racial make-up of the sample is 75% White, 22% Black, and 3% other minorities, which aligns exactly with census data from the same year and state (U.S. Census Bureau, 2010). After listwise deletion for missing data, 1 the sample size for the current study is 1,171 women.
Measures
Sexual victimization
At each wave, participants completed the Sexual Experiences Survey (SES; Koss, Gidycz, & Wisniewski, 1987). The SES is the most frequently used self-report measure of sexual assault victimization (Kolivas & Gross, 2007). We consider sexual victimization to have occurred if the respondent answered “at least once” to any of the sexual victimization questions, which include both attempted and completed assaults. In the initial survey, respondents were asked about sexual victimization in childhood before the age of 14. In addition, the initial survey asked respondents about unwanted sexual experiences from the time they were 14 years old until the present, accounting for sexual experiences during high school. The subsequent surveys ask about sexual experiences since the previous survey administration, describing sexual experiences during each year of college.
Depressive symptoms
The Depression subscale of the Mental Health Inventory (MHI) is a 10-item mean scale with high reliability (W1: α = .93; W2: α = .94; W3: α = .95), and this was used to measure depression. Respondents were asked to “consider how you have been during the past month and rate how descriptive each statement is of you”: (1) not at all like me, (2) a little like me, (3) somewhat like me, (4) mostly like me, and (5) very much like me. The questions included items such as “low or very low spirits,” “felt depressed,” “downhearted and blue,” and “felt cheerful, lighthearted” (reverse-coded). The means and standard deviations for depression for each wave are as follows: Wave 1: M = 2.405, SD = 0.9408; Wave 2: M = 2.334, SD = 0.9373; Wave 3: M = 2.304, SD = 0.9527.
Substance use
A three-item mean scale measured substance use. The first question is “How often do you drink alcohol?” with answer choices including (0) I never drink or have not drunk in the past school year, (1) I drink less than once a month but at least once in the past school year, (2) I drink one to three times a month, (3) I drink one to two times a week, and (4) I drink more than twice a week. The other two questions are “In an average month, how many times do you have 5 or more drinks in a row?” and “How many times did you become drunk or pretty high in an average month during the past school year?” The answer choices are (0) never, (1) one time, (2) two to five times, (3) six to nine times, and (4) ten or more times. The Cronbach’s alpha for these three items is high at each wave (W1: α = .89; W2: α = .90; W3: α = .89). The means and standard deviation for substance use are as follows: Wave 1: M = 0.9727, SD = 0.9871; Wave 2: M = 1.029, SD = 0.9893; Wave 3: M = 1.014, SD = 0.9509.
Childhood sexual victimization
In all of our models, we also control for childhood sexual victimization. In addition to the detailed questions about sexual victimization during adolescence, the first wave of the survey asks about victimization before the age of 14. These are three separate statements that address the sexual experiences of (a) being touched in a sexual way, (b) attempted intercourse, or (c) intercourse occurring before the age of 14. Respondents who answered “at least once” to any of the above three questions were considered to have experienced childhood sexual victimization.
Analytic strategy
We used structural equation modeling (SEM) in MPlus Statistical Software Version 7 (Mutheén & Mutheén, 2012) to conduct a path analysis. We modeled longitudinal associations between victimization, depressive symptomology, and substance use frequency and intensity. Because our focal dependent variable (sexual assault) is binary, we used a modified version of the conventional measurement model for continuous indicators, running a path analysis with categorical dependent variables using the Theta parameterization. In the Theta parameterization, residual variances for continuous latent response variables of observed categorical dependent variables are allowed to be parameters in the model, but scale factors for continuous latent response variables are not. Estimates for binary dependent variables are obtained in logits and can be interpreted as log odds ratios with proper conversion (Mutheén & Mutheén, 1998-2012).
Results
The sample size for this study is 1,171. Thirty-five percent of respondents reported experiencing a sexual victimization at some point during high school (Wave 1). Twenty-two percent reported victimization in their freshman year of college (Wave 2), while 19% of respondents reported sexual victimization in their sophomore year of college (Wave 3). Forty-two percent of the sample (n = 488) reported never experiencing sexual victimization, 26% (n = 301) of the sample reported experiencing sexual victimization at one point in the life course, and 29% (n = 338) of the sample reported sexual revictimization across multiple waves of data.
We used measures of comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and χ2 to check for model fit. The Bentler CFI is an incremental fit index that measures the relative improvement in the fit of the researcher’s model over that of a baseline model (Kline, 2011, p. 208). Relative fit indices such as the TLI compare a chi-square for a particular model with the null model and generally should be 0.95 or higher to indicate close fit. The RMSEA is a scaled “badness of fit” index where a value of zero indicates the best fit (Kline, 2011, p. 205). Finally, the chi-square (χ2) difference statistic can be used to test the statistical significance of the decrement in overall fit and a lower number indicates a better fit (Kline 2011, p. 215). Although the χ2(80.897, df = 18) is significant (p = .000), the RMSEA is .048, which is below the value that Browne and Cudeck (1992) indicate as a close fit (.05) and well within the bounds of a reasonable error of approximation (below .08). In addition, Hu and Bentler (1999) recommend a cutoff value close to 0.95 for both the TLI and the CFI. In this model, the TLI (.908) is below that cutoff value, and the CFI (.963) is very close to that cutoff value. Taken together, these statistics indicate that the model fits the data well.
First, we will present results that test our cross-sectional predictions. The correlation matrix presented in Table 1 indicates that reports of sexual victimization, depressive symptoms, and substance use are correlated at each wave. Victimization during sophomore year of college (W3) is correlated with depressive symptoms (r = .14, p < .001) and substance use (r = .14, p < .001) within the same wave. Victimization during freshman year of college (W2) is correlated with depressive symptoms (r = .13, p < .001) and substance use (r = .16, p < .001) within the same wave. Finally, individuals reporting sexual victimization during adolescence (W1) also were more likely to report depressive symptomology (r = .11, p < .001) and substance use (r = .25, p < .001) during adolescence. These findings provide support for our cross-sectional predictions regarding the association between sexual victimization, depressive symptoms, and substance use.
Correlation Matrix for Study Variables (N = 1,171).
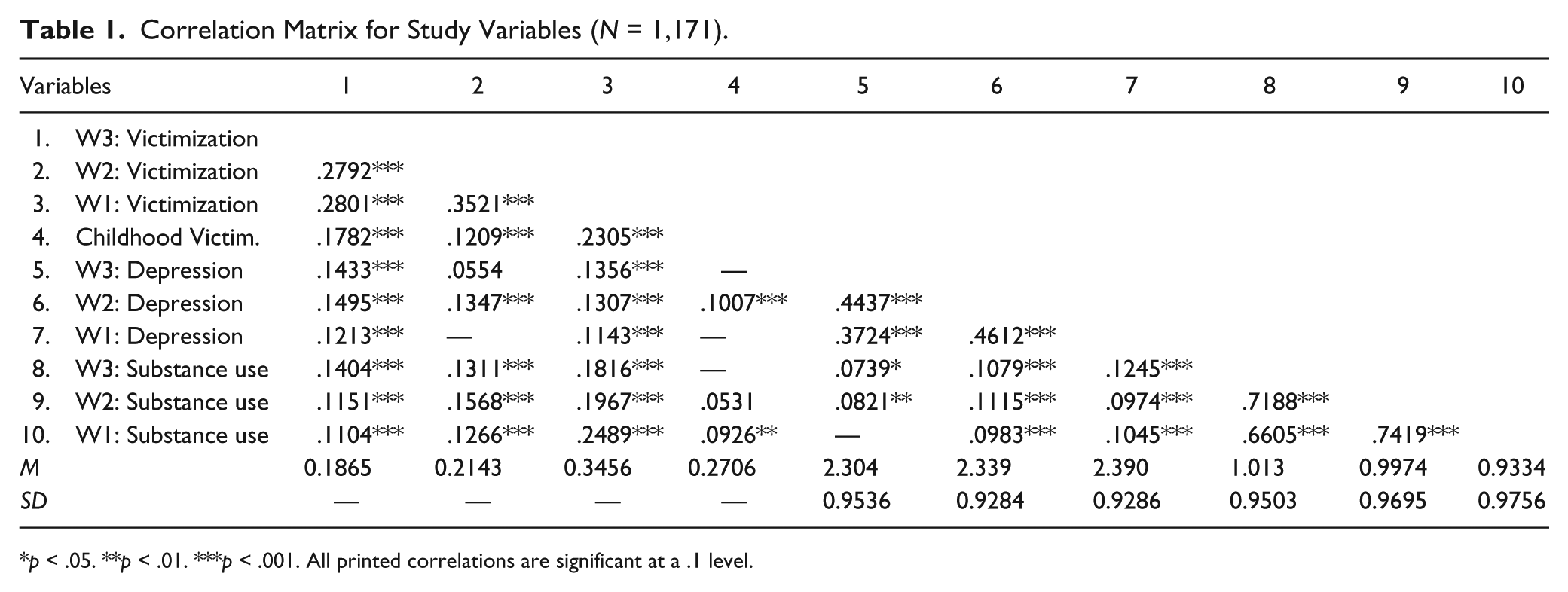
p < .05. **p < .01. ***p < .001. All printed correlations are significant at a .1 level.
We also predicted stability in victimization experiences over time, and our results support this prediction (see Figure 1). Consistent with results reported by the original researchers (White & Humphrey, 1997), we found that experiencing sexual victimization during adolescence doubled the odds of experiencing sexual victimization during the first year of college (b = .710, p < .001). In other words, women who experienced victimization during adolescence were twice as likely to be revictimized during the first year of college than women who did not experience victimization during adolescence. Furthermore, women who experienced sexual victimization during their first year of college had more than one and half times greater odds of experiencing sexual victimization during their second year of college than women who did not experience sexual victimization during the first year of college. Stated differently, experiencing sexual victimization during the first year of college (W2) is associated with a 60% increase in the odds of experiencing sexual victimization as a sophomore (W3) (b = .465, p < .001).
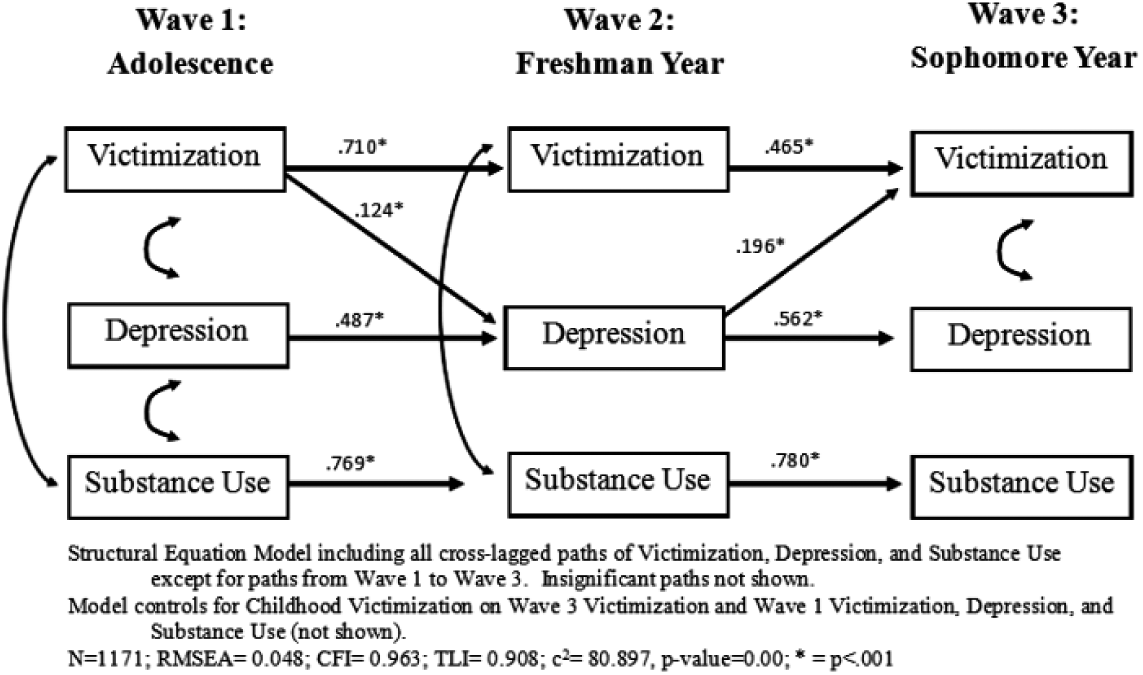
Structural Equation Model.
There is also stability over time in depressive symptomology (see Figure 1). Severity of depressive symptoms during adolescence was a significant predictor of severity of depressive symptoms during the first year of college (b = .487, p < .001). Specifically, for a one-unit increase in depressive symptomology at Wave 1, participants experienced a 1.6-point increase in depressive symptomology at Wave 2. Furthermore, for every one-unit increase in depressive symptoms at Wave 2, individuals experienced a 1.75-point increase at Wave 3 (b = .562, p < .001). Higher levels of depression in adolescence are associated with higher levels of depression during the first year of college which, in turn, are associated with higher levels of depression during the second year of college.
There is a similar pattern for substance use—higher levels of substance use at one wave were associated with higher levels of substance use at the following wave. Specifically, a one-unit increase in substance use during adolescence is associated with a 2.15-point increase in substance use during the first year of college (b = .769, p < .001). Similarly, higher levels of substance use during the second year of college were significantly more likely if participants reported substance use during the first year of college (b = .780, p < .001). These findings indicate continuity across waves in victimization, depression, and substance use.
Next, we test longitudinal hypotheses about depressive symptomology and substance use at one wave being associated with sexual victimization at the next wave. Table 2 presents the standardized and unstandardized path estimates in the model as well as the exponentiated path estimates that can be interpreted as the odds of experiencing victimization at Wave 3. The variables with direct paths to sexual victimization at Wave 3 are sexual victimization at Wave 2, depression at Wave 2, alcohol use at Wave 2, and sexual victimization as a child. As discussed above, victimization during freshman year of college (W2) is associated with victimization at sophomore year of college (W3) (b = .465, p < .001). Also predictive of victimization as a sophomore in college (W3) is reporting experiencing victimization as a child. Women who reported sexual victimization as a child have almost one and a half times greater odds of experiencing sexual victimization as a sophomore in college than women without a history of childhood sexual abuse (b = .377, p < .001).
Effect of Victimization, Depression, and Substance Use on Sexual Victimization at Wave 3 (N = 1,171).

p < .05. **p < .01. ***p < .001.
We also find that higher levels of depressive symptoms during freshman year of college (W2) are significantly related to experiencing victimization during sophomore year of college (W3) (b = .196, p < .001). Specifically, every one-unit increase in the severity of depression at Wave 2 is associated with a 22% increase in the odds of experiencing victimization at Wave 3. This is consistent with our prediction that depressive symptoms at one wave will increase the likelihood of victimization at the following wave. Yet, we also note that depressive symptoms in adolescence (W1) is not associated with an increased odds of experiencing victimization during the freshman year of college (W2). Thus, the association between depression and victimization may not be consistent across the life course. Contrary to our prediction about substance use and revictimization, substance use during freshman year (W2) is not a significant predictor of experiencing sexual victimization during sophomore year (W3).
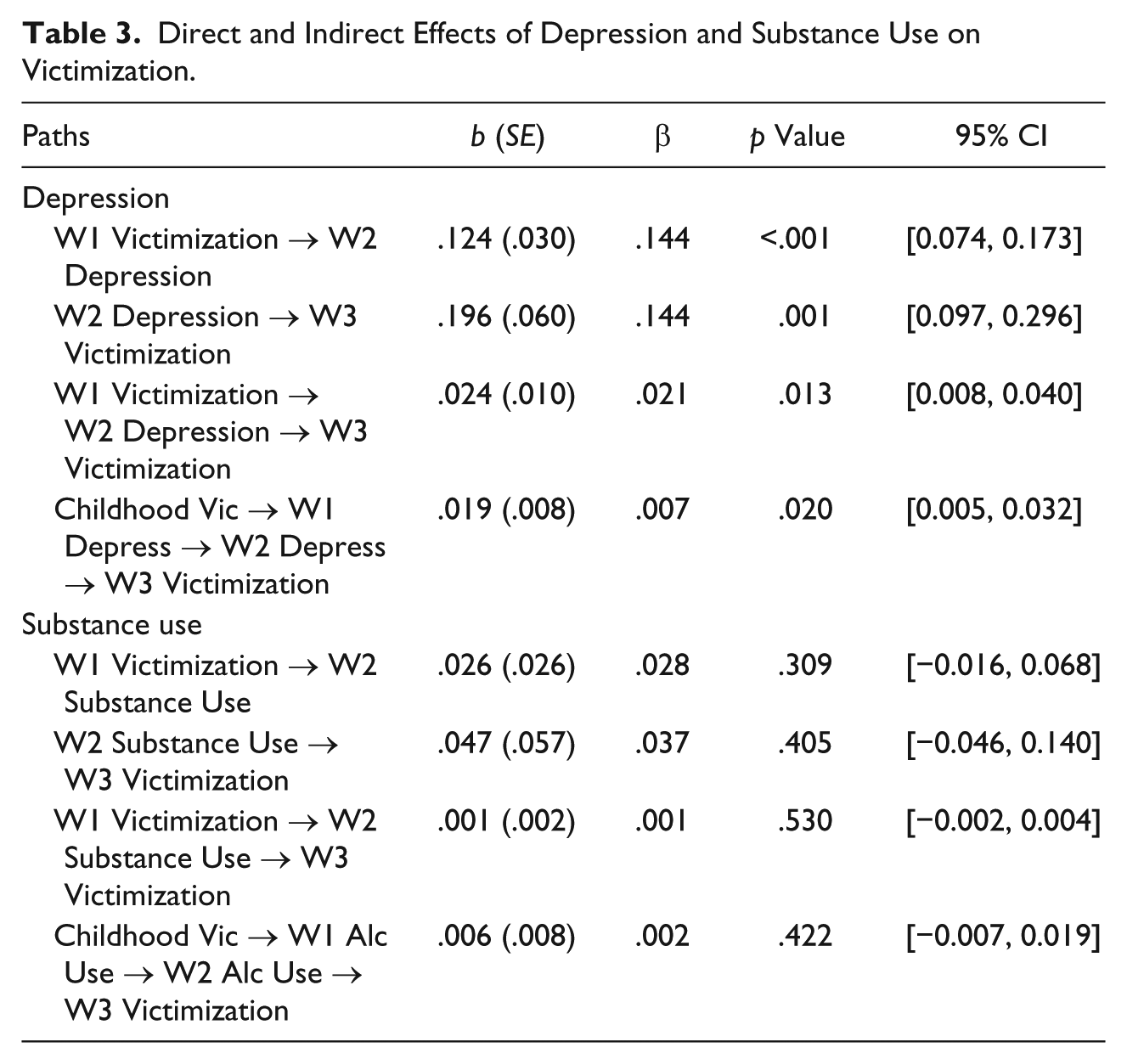
Finally, we examine whether depressive symptomology and substance use mediate the relationship between sexual victimization in adolescence and sexual victimization in college. Table 3 shows the significance of both the direct and indirect effects of depressive symptoms and substance use on the relationship between victimization at an earlier wave and victimization at a later wave. The paths for depressive symptomology are significant, while the paths for substance use are not significant. In support of our prediction, we find that depressive symptoms at Wave 2 partially mediate the relationship between victimization at Wave 1 and victimization at Wave 3. These results indicate that continuity in sexual victimization over time can be explained, in part, by increases in depressive symptoms following a victimization event. There is no evidence, however, that victimization in adolescence increases substance use or that substance use at Wave 2 increases risk of victimization at Wave 3 once prior substance use is controlled.
Direct and Indirect Effects of Depression and Substance Use on Victimization.
The final model includes all cross-lagged paths except for paths between Wave 1 and Wave 3. Figure 1 shows only the paths that are statistically significant. In support of our predictions, the expected paths between depressive symptomology and victimization are significant for Waves 2 and 3, but not for Waves 1 and 2. For every one-unit increase in the severity of depression for individuals during their first year of college, there is a 22% increase in the odds that they will experience sexual victimization in their second year of college (b = .196, p < .001). However, contrary to our predictions, the expected paths linking substance use and victimization are not significant across any waves.
Discussion
Previous research has examined the correlates of sexual revictimization to determine why experiencing sexual victimization increases risk of future victimization (Classen et al., 2005; Fisher et al., 2010; Testa et al., 2010). Very little research, though, has used longitudinal data, which is necessary to establish causality and determine mediating relationships (but see Gidycz et al., 1993; Greene & Navarro, 1998; Kilpatrick et al., 1997). This study contributes to this literature by examining, in a longitudinal dataset, substance use and depressive symptomology as potential explanations for the high incidence of sexual revictimization among college women. Our theoretical reasoning is consistent with routine activity theory. Findings indicate that not only are depressive symptoms associated with an increased likelihood of sexual victimization at a later time point but also depressive symptoms partially mediate the effects of primary and recurrent sexual victimization at a later time point. We do not find support, however, for our prediction that substance use mediates sexual victimization events.
Our findings are consistent with the existing empirical literature but also add to this research in important ways. Consistent with the large literature on substance use and sexual victimization, our study finds that substance use is associated with experiences of sexual violence (Abbey, 2002; Kilpatrick et al., 1997; Parks et al., 2008; Resnick et al., 2012). By using longitudinal data, however, we also to speak to the more limited research on substance use as a mediator of sexual victimization events (Mouilso et al., 2012; Testa et al., 2010). We find that despite strong associations between substance use and sexual violence within waves (see Table 1), there is no evidence of mediation. Instead of finding that sexual assault increased substance use, which increased risk of subsequent victimization, we found consistency in substance use over time.
Our finding that depressive symptoms are not only a correlate of sexual victimization but also mediate victimization events is consistent with previous literature reporting that psychological distress accompanies sexual victimization (Maniglio, 2010; Ouellet-Morin et al., 2015; Weaver & Clum, 1995). Most of this literature, however, focuses on other forms of psychological distress such as self-blame, dissociation, and post-traumatic stress disorder (Classen et al., 2005; Filipas & Ullman, 2006; Gidycz et al., 2006; Messman-Moore & Long, 2003). Thus, we contribute by identifying depression as an important predictor of sexual revictimization, which may assist practitioners in intervention efforts. At the same time, as we do not find effects of adolescent depression on victimization during the freshman year of college, it may well be that the mediating effects we document are specific to a particular life course stage or to victimization contexts in college. Additional research is needed to tease out these effects.
Finally, our research speaks to the well-established finding that sexual victimization at one time point is associated with a higher likelihood of victimization at a later time point. However, much of the previous literature on sexual revictimization relates childhood sexual victimization to adulthood victimization. Our research examines the connection between adolescent sexual victimization and revictimization in early adulthood, while controlling for childhood victimization. Our study adds to the limited literature on stability in sexual victimization across adolescence/young adulthood, even when controlling for sexual abuse experienced during childhood (Humphrey & White, 2000). This suggests that though the power dynamics of adolescent victimization and childhood sexual abuse are different (Arata & Lindman, 2002), both forms of sexual violence have consequences for revictimization risk.
By using routine activity theory as a framework to explain sexual revictimization, we contribute more broadly to understanding sources of revictimization risk, as well as speak to the state dependence versus population heterogeneity debate. Our findings for depressive symptomology are consistent with the state dependence explanation for revictimization—specifically, that sexual victimization in adolescence increases the likelihood of experiencing depressive symptoms, which, in turn, puts individuals at greater risk for revictimization in young adulthood. These findings are also consistent with routine activity theory, as depression is associated with a number of behaviors that may make one a more attractive target, such as appearance of vulnerability and reduced risk perception. In contrast, we did not find evidence that substance use increased following sexual victimization in adolescence, nor that earlier substance use increased victimization at the next wave. We did find, however, that substance use at Wave 2 was associated with sexual victimization at Wave 2, suggesting that substance use is a likely risk factor, as many others have documented (Abbey, 2002; Kilpatrick et al., 2003; Resnick et al., 2012).
Directions for Future Research
Our study suggests a number of areas for future research. First, though our data are longitudinal, the length of time between waves may be too long to capture the cycle of victimization, substance use, depressive symptoms, and subsequent revictimization. Previous research has suggested that sexual revictimization is most common within the same month of the original incident (Daigle et al., 2008). Ideally, future studies would collect data from respondents more frequently—asking questions about victimization, substance use, and depression on a monthly or even weekly basis.
Second, future research should utilize data from a more diverse sample. First, we are not able to account for sexual orientation, which is a known predictor of sexual assault. Lesbian, gay, bisexual, transgender, and queer (LGBTQ) young adults are significantly more likely to experience sexual victimization than their straight counterparts—one study reports a twofold increase in incidence of sexual assault among sexual minorities (24.3%) as compared with nonsexual minorities (11%) (Edwards et al., 2015; Wood, 2001). Second, it is important to examine the role of depression in mediating sexual assault events among a more racially diverse sample, given variation in assault across race and ethnicity (Bromberger, Harlow, Avis, Kravitz, & Cordal, 2004). Third, our study used data collected in the early- to mid-1990s. Research indicates that the prevalence of sexual victimization has not significantly decreased since the time of data collection, and recent studies continue to find links between depression, substance use, and victimization (Carey, Durney, Shepardson, & Carey, 2015; Krebs et al., 2007; Walker, Freud, Ellis, Fraine, & Wilson, 2019). It is nonetheless important to replicate our findings in a more recent sample.
Third, this study examines the correlates, precursors, and effects of any sexual victimization experience with depression and substance use. We do not differentiate sexual victimization experiences based on severity or frequency. Previous research indicates that particular types of sexual assault, such as those involving penetration, are associated with a higher likelihood and severity of negative effects for victims (Messman-Moore et al., 2009; Roodman & Clum, 2001). This suggests that future research should evaluate how severity and frequency of sexual victimization experiences are longitudinally related to depression and substance use. Finally, these findings are based on a sample from a single university and it would be important to replicate these findings with respondents from other universities or in a non–college student population of young adults.
Conclusion
Depression has long been considered a consequence of sexual victimization (Brown, Testa, & Messman-Moore, 2009; Weaver & Clum, 1995). The role that depression plays in facilitating revictimization, though, is underexplored. In finding that depressive symptoms partially mediate the relationship between adolescent and young adult victimization, we have demonstrated that depression is a source of revictimization risk. Thus, clinicians should be aware that the depressive symptoms that many women experience following a sexual assault are not only disruptive—and potentially debilitating—but increase the likelihood that women will be victimized again. This suggests the importance of depression screening and intervention to reduce risk of sexual revictimization.
Footnotes
Acknowledgements
The authors would like to thank Tara E. Sutton for her invaluable advice on methodological issues, although any errors remain our own. We also thank the JIV editors and anonymous reviewers for their constructive comments on an earlier draft of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.