
Abstract
Currently, Latinos constitute the second largest and fastest growing minority group in the United States. Among this population, one in every six Latinas experience intimate partner violence (IPV) in her lifetime. Research has documented significant detrimental effects of physical, sexual, emotional, and psychological IPV on the physical, emotional, and cognitive well-being of various cultural/ethnic groups; however, few studies have focused on economic abuse, which may include tactics of economic control, economic exploitation, and employment sabotage. Research examining economic abuse against racial/ethnic minorities, particularly Latinos, is needed. To address these gaps, baseline data from a larger treatment outcome study were used to examine the associations between economic abuse and the mental health symptoms reported by 245 Latina IPV survivors in the United States. When examining the economic abuse experiences reported by Latinas in this sample, the results indicated that the most commonly reported form of economic abuse was economic control (e.g., restricting access to money and financial information). Multiple regression analyses revealed that economic abuse did not uniquely predict mental health after accounting for other forms of IPV victimization and sociodemographic characteristics. Limitations of this study are discussed, and directions for future research designed to enhance our understanding of economic abuse against various racial/ethnic groups (such as Latinas) are presented.
Intimate partner violence (IPV) remains a significant social and public health problem affecting millions of people around the world, particularly women. IPV is a pattern of abusive behaviors (which may include physical, sexual, psychological, and/or economic tactics) by one partner against another as a means of expressing or maintaining control (United States Department of Justice, 2017). Recent estimates indicate that approximately 36% of American women have experienced IPV (e.g., rape, physical assault, stalking) in their lifetime (Black et al., 2011). Research on IPV has documented numerous adverse mental health outcomes affecting survivors (Fedovskiy, Higgins, & Paranjape, 2008). Although considerable research has focused on the impact of physical, psychological, and/or sexual IPV on survivors’ well-being, few studies have examined the association between economic abuse and survivors’ mental health (Postmus, Huang, & Stylianou, 2012). Moreover, investigations of economic abuse against ethnic/racial minorities, particularly Latinos, are limited. To address these gaps, the present study sought to examine whether economic abuse victimization is related to survivors’ mental health while controlling for other forms of IPV as reported by a sample of Latina (i.e., Hispanic women) IPV survivors living in the United States.
IPV and Latinas
Currently, Latinos 1 constitute the second largest and fastest growing minority group in the United States, with approximately 54.2 million Latinos living in the United States at the time of the 2011-2015 American Community Survey (United States Census Bureau, 2015). Recent studies estimate that one in six Latinas in the United States experience physical, sexual, and/or emotional IPV in her lifetime (Sabina, Cuevas, & Zadnik, 2015). As with all victimization rates, these estimates should be considered with caution given that they are based on reported victimization. Moreover, it is possible that Latinas underreport their IPV victimization experiences due to sociocultural factors (e.g., immigration status, acculturation, language), as such factors have been found to be barriers to help-seeking and police reporting among Latina IPV survivors (Ammar, Orloff, Dutton, & Aguilar-Hass, 2005; Bauer, Rodriguez, Quiroga, & Flores-Ortiz, 2000).
Similarly, research has found that sociodemographic characteristics may increase risk of IPV victimization against Latinas in the United States (e.g., Sabina, Cuevas, & Schally, 2013; Sabina et al., 2015). For instance, studies indicate that Latinas who are U.S.-born and/or identify more with the Anglo-American culture are at increased risk of experiencing physical IPV, sexual IPV, stalking, and/or threat of IPV, as compared with Latinas who are first-generation immigrants and/or identify more with the Latino culture (Sabina et al., 2013; Sabina et al., 2015). The literature also indicates that higher rates of IPV against ethnic/racial minorities—particularly Latinas (relative to the White women)—can be explained by economic and structural factors such as low socioeconomic status, limited education, unemployment, immigration status, acculturation, as well as conditions such as poverty and discrimination (see Bent-Goodley, 2007, for a review).
IPV and Mental Health
The IPV literature has documented significant links between victimization and an array of mental health problems including symptoms of depression, anxiety, posttraumatic stress disorder (PTSD), dissociation, low self-esteem, and substance use (e.g., Beydoun, Beydoun, Kaufman, Bruce, & Zonderman, 2012; Bonomi, Anderson, Cannon, Slesnick, & Rodriguez, 2009; Cuevas, Sabina, & Picard, 2010; Hazen, Connelly, Soriano, & Landsverk, 2008). Investigations employing Latino samples also have found evidence of associations between IPV victimization and mental health problems (e.g., Basile et al., 2015; Kaltman, Green, Mete, Shara, & Miranda, 2010; Lara et al., 2014; Rodriguez et al., 2010; see Stockman, Hayashi, & Campbell, 2015, for a review; Valentine, Rodriguez, Lapeyrouse, & Zhang, 2011). For instance, Lown and Vega (2001) conducted a study examining the association between recent IPV victimization (physical or sexual) and self-reported mental health using a sample of Mexican American women (58.3% Mexican-born). The results revealed that abused women were significantly more likely to report poor mental health than nonabused women (Lown & Vega, 2001).
Relatedly, Fedovskiy and colleagues (2008) examined the associations between IPV victimization, PTSD, and major depression disorder (MDD) as reported by a sample of Spanish-speaking immigrant Latinas. Findings indicated that Latinas reporting an IPV history (physical, sexual, and/or psychological abuse) were approximately 3 times more likely to meet criteria for PTSD than Latinas without a history of IPV. In addition, the authors found that Latinas who met criteria for PTSD were 10 times more likely to report MDD (although no direct relationship was found between IPV victimization and MDD).
Moreover, Hazen and colleagues (2008) reported differential associations between types of IPV victimization and psychological functioning among a sample of Latinas (52.1% Mexican-born). Specifically, when various forms of IPV were considered simultaneously, the findings indicated that both physical IPV and psychological IPV were associated with symptoms of depression and hostility, whereas sexual IPV was significantly associated with only phobic anxiety. Similarly, Kelly (2010) examined the associations between various forms of victimization (e.g., psychological IPV, physical IPV, sexual IPV, as well as childhood sexual assault) and mental health variables, including PTSD (diagnosis, symptoms severity), MDD (diagnosis, symptom total), and comorbid PTSD/MDD. Findings revealed that sexual IPV victimization was not related to either PTSD or MDD symptoms/diagnoses. Nevertheless, significant associations were found between psychological IPV victimization and MDD (symptoms and diagnosis) and comorbid PTSD/MDD—but not with PTSD alone. Physical IPV victimization was associated with MDD diagnosis only. Overall, the literature shows differential links between type of IPV victimization and mental health problems.
Some studies have suggested that sociocultural and immigration-related factors may exacerbate the IPV victimization experiences of Latinas living in the United States (e.g., Ammar et al., 2005; see Bent-Goodley, 2007, for a review). Notably, the literature indicates that immigrant Latinas may be at greater risk of prolonged abusive relationships because of limited access to culturally appropriate public safety and mental health services (e.g., Ammar et al., 2005; see Bent-Goodley, 2007, for a review). Other identified help-seeking challenges experienced by Latina IPV survivors include poverty, cultural norms (e.g., emphasis on family privacy), and structural barriers (e.g., a lack of culturally competent staff; see Bent-Goodley, 2007, for a review).
In addition, the literature on Latinas’ experiences of IPV suggests that ethnic- and immigrant-specific factors may heighten Latinas’ susceptibility to the mental health consequences of IPV victimization. As speculated by Edelson, Hokoda, and Ramos-Lira (2007), economic stressors, a lack of English-language proficiency, and isolation from family and social support can intensify Latinas’ sense of hopelessness regarding their victimization situations, which may lead to more depressive symptoms. One logical extension of the finding that economic stressors contribute to mental health problems (e.g., greater hopelessness) among IPV survivors, is the notion that economic abuse by one’s intimate partner may uniquely exacerbate mental health problems (e.g., depression) among IPV victims. In light of the evidence suggesting that various forms of IPV impact mental health differently, the present study examined whether economic abuse by one’s intimate partner is related to mental health above and beyond psychological, physical, and sexual IPV, as well as sociodemographic factors.
Economic Abuse
While a large body of work has investigated the prevalence and consequences of physical, sexual, and psychological IPV, few investigators have explored economic abuse as a form of IPV (e.g., Adams, Sullivan, Bybee, & Greeson, 2008; Outlaw, 2009; Postmus, Huang, & Stylianou, 2012; Postmus, Plummer, McMahon, Murshid, & Kim, 2012; Postmus, Plummer, & Stylianou, 2016; Stylianou, Postmus, & McMahon, 2013). Although commonly overlooked or combined with psychological abuse, recent studies reveal that economic abuse is a distinct form of IPV that affects the lives of many individuals (Stylianou et al., 2013). In addition, the literature indicates that economic factors have a strong influence on IPV help-seeking, readiness to leave an abuser, and emotional well-being (e.g., Brabeck & Guzman, 2008; Klevens et al., 2007).
Economic abuse refers to any action intended to control or hinder the financial capabilities or resources of an intimate partner in order to make him or her financially dependent (Postmus, Plummer, et al., 2012). These tactics may include damaging the victims’ economic self-sufficiency and self-efficacy (Postmus, Plummer, et al., 2012). Subcategories of economic abuse include economic control (e.g., restriction of resources), economic exploitation (e.g., depletion of funds), and employment sabotage (e.g., blockage of opportunities; Adams et al., 2008; Postmus, Plummer, & Stylianou, 2016).
Research examining economic abuse against Latinas is very limited. One recent study suggested that employment sabotage may be a common tactic utilized by Latino batterers when attempting to control their partners or reestablish male dominance. During focus groups with male Mexican immigrant batterers and batterer intervention program facilitators (N = 24), Galvez, Mankowski, McGlade, Ruiz, and Glass (2011) identified on-the-job surveillance, job harassment, and work disruption as three common tactics utilized to control female partners. Although the focus of this study was not economic abuse per se, the findings provide evidence of the use of employment sabotage by Latino batterers. In addition, participants described work-related tactics not previously documented, such as not allowing partners to obtain a drivers’ license, restricting the use of automobiles, and sending partners back to their country of origin (Galvez et al., 2011). These findings indicated that like other forms of IPV, the specific tactics of economic abuse may be ethnic-specific and hence warrant further investigation.
Although scant, studies examining economic abuse within racially/ethnically diverse samples in the United States have indicated significant implications for the psychological well-being of victims. For instance, when examining the potential long-term consequences of physical, psychological, and economic IPV on mental health within a sample of mothers drawn from various locations within the United States, Postmus, Huang, and Stylianou (2012) found a significant link between economic abuse victimization and depression. Specifically, the results indicated that experiencing economic abuse during the first year postpartum was associated with depressive symptoms reported 5 years later. This relationship was significant even after accounting for age, ethnicity, education, as well as childhood and adult living arrangements (Postmus, Huang, & Stylianou, 2012). Notably, mothers who experienced economic abuse were 1.9 times more likely to experience depression than nonabused mothers, which was comparable to the odds of depression associated with psychological (1.4) or physical victimization (1.8). These results suggest that economic abuse may have significant long-term effects on depressive symptoms (Postmus, Huang, & Stylianou, 2012).
Moreover, the general literature on physical, sexual, and psychological IPV has consistently identified financial factors as significant barriers to escaping IPV, especially among ethnic/racial minority women (e.g., Brabeck & Guzman, 2008; Klevens et al., 2007; see Postmus, 2010, for a review). In a study exploring the IPV survival strategies employed by Mexican women, participants reported that the inability to save their own money due to their abusers’ economic control was an obstacle to escaping IPV (Brabeck & Guzman, 2008). Another study exploring factors associated with IPV among Latinos found that stress due to financial hardships or work was considered an important contributor to IPV (Klevens et al., 2007). Recent studies using samples of IPV survivors attending financial literacy programs have also indicated that economic abuse victimization is common among women who report experiencing physical and/or psychological IPV (Outlaw, 2009; Postmus, Plummer, et al., 2012; Stylianou et al., 2013). Overall, the literature on ethnic/racial minorities highlights the importance of advancing research on economic abuse to better inform screening and intervention practices for this type of victimization, particularly among disadvantaged populations such as Latinas and women suffering from other forms of IPV.
The Current Study
The purpose of this study was to contribute to the growing literature on IPV against Latinas by providing a cross-sectional view of the linkages between economic abuse and mental health symptoms (i.e., depression, anxiety, and PTSD). We also examined whether the association between economic abuse and mental health symptoms could be accounted for by other forms of IPV victimization (i.e., sexual, physical, and psychological) and/or the sociodemographic characteristics (i.e., age, immigration status, relationship status, financial responsibility for children, employment, and annual household income) of the respondents.
Method
Data for this study came from a larger, longitudinal randomized control study conducted to evaluate the effectiveness of a financial empowerment program for IPV survivors (i.e., Moving Ahead through Financial Management; see Postmus & Plummer, 2010, for a description of the parent study; see also Postmus, Plummer, & Hoge, 2013, for a final report). The curriculum for the program was sponsored and created by The Allstate Foundation and the National Network to End Domestic Violence (NNEDV) to provide survivors with the necessary knowledge and skills to understand economic abuse, financial fundamentals, and financial management (Postmus, Hetling, & Hoge, 2015; www.clicktoempower.org). Data were collected from 14 domestic violence agencies across seven states at four different time points across the span of 14 months. For the purposes of this study, only data collected during the first wave of interviews were used given that all IPV victims in this study received advocacy services from a domestic violence service agency after completing their baseline interview. Thus, the baseline data provided an opportunity to examine the relationships between economic abuse and mental health prior to the intervening influence of the financial literacy intervention.
Participants
In the “parent” or original study, participants were recruited from 14 different domestic violence agencies located in urban and suburban communities in the Northeast, Midwest, Texas, and Puerto Rico. Staff from all 14 programs agreed to support the study and to assist with the recruitment of participants. Program staff advertised the study within their agency through email, group announcements, staff meeting announcements, and/or individual discussions with clients. A sample flyer was provided to the agencies to use in the recruitment process. Across all sites, 456 IPV survivors participated in the baseline interviews for the parent study. The results presented in this article represent data reported by the subsample of 245 women who identified as Latina/Hispanic. The average age of the Latinas in this study was 35.6 years (SD = 8.0 years, age range = 19-57). A little over a quarter (26.1%) were born in the United States with the remaining born elsewhere. At the time of the interview, over half of the Latinas (53.9%) were in a relationship and most were financially responsible for children (87.3%). Half of the sample reported being employed (50.2%); however, almost half (49.8%) reported an annual household income of less than US$10,000.
Procedures
Institutional review board approval was obtained for the parent longitudinal study. While participants were interviewed at four time points over 14 months, the present analyses were limited to the data from baseline interviews. After informed consent was granted, participants engaged in face-to-face interviews with highly trained and experienced research assistants. During the interviews, researchers verbally asked participants the questions (i.e., demographics, IPV victimization, mental health, quality of life, financial literacy, economic empowerment, self-efficacy, and self-sufficiency) and recorded answers by typing them into a computer program (using SNAP©, a web-based survey). If Internet access was unavailable, researchers recorded answers on paper and upon gaining Internet access, transferred the answers to the web-based survey. In addition, all interviews were offered in English or Spanish; corresponding written documents were also available in English and Spanish. All translated scales were reviewed by several Latina researchers of Puerto Rican and/or Mexican descent to ensure that the language used in the survey was appropriate for women from different Latino subgroups. Other Latina research assistants then translated the instruments back to English to confirm content validity. Average completion time for the interview was approximately 1 hr. Participants were given a US$20 gift card for their participation in the baseline interview.
Measures
Ethnicity
Ethnicity was measured by asking participants to self-identify as belonging to one of the following ethnic groups: Latina/Hispanic, non-Hispanic White, Black, American Indian, Native Hawaiian/Pacific Islander, Asian, Multi-ethnic, or other. Data from those who selected the category “Latina/Hispanic” were included in the present study.
Mental health concerns
Three mental health outcomes from the parent study were employed as dependent variables: depression, anxiety, and PTSD.
Symptoms of depression were assessed using the Center for Epidemiologic Studies-Depressed Mood Scale (CES-D; Frazier, 1977). CES-D is a 20-item measure that assesses the frequency of specific depressive symptoms including “I felt lonely” and “I thought my life had been a failure.” Answers were based on the past week’s symptomatology and rated according to a 4-point scale ranging from 1 (less than 1 day) to 4 (5-7 days). Mean scores were computed with higher scores representing more frequent depressive symptoms. In this study, the CES-D scale demonstrated strong internal consistency (α = .92).
Symptoms of anxiety were measured using the Generalized Anxiety Disorder-7 (GAD; Spitzer, Kroenke, Williams, & Lowe, 2006). This is a 7-item questionnaire that assesses the frequency of anxiety-related feelings and thoughts. Responses were made on a 4-point scale ranging from 1 (not at all) to 4 (nearly every day). Sample items include “worrying too much about different things” and “feeling afraid as if something awful might happen.” Mean scores were computed with higher scores representing more frequent anxiety symptoms. As completed by the present sample, the GAD scale demonstrated strong internal consistency (α = .91), which is comparable to what Spitzer and colleagues (2006) found (α = .92).
PTSD symptoms were measured using a revised version of the National Comorbidity Survey (NCS; 1992). The NCS includes nine questions that assess PTSD symptoms experienced in the past month. The prompt asked participants to indicate the frequency of certain feelings and behaviors as a result of being hurt by their loved ones or by other traumatic events. Sample items include “flashbacks or sudden, vivid distracting memories” and “feeling numb or unable to have feelings for others.” Responses were made on a 4-point scale ranging from 1 (never) to 4 (very often). Mean scores were computed with higher scores representing more frequent PTSD symptoms. As completed by the present sample, the NCS PTSD scale demonstrated strong internal consistency (α = .89).
Economic abuse
The main independent variable in this study was economic abuse, which was measured using the Scale for Economic Abuse-12 (SEA-12; Postmus, Plummer, & Stylianou, 2016). This is a 12-item scale that asks participants to rate the frequency of experiencing economic abuse perpetrated by a partner within the last 12 months. Postmus, Plummer, and Stylianou’s (2016) version of the SEA-12 consists of three subscales: economic control (five questions), economic exploitation (three questions), and employment sabotage (four questions). Responses were made on a 5-point scale ranging from 1 (never) to 5 (quite often). Sample items included “keep financial information from you” (economic control), “spend the money you needed for rent or other bills” (economic exploitation), and “demand that you quit your job” (employment sabotage). For this article, the mean response across all items on the SEA-12 was used as the main independent variable, with higher scores representing higher levels of economic abuse.
The SEA-12 and each subscale demonstrated adequate internal consistency (SEA-12, α = .88; Economic Control, α = .84; Economic Exploitation, α = .81; Employment Sabotage, α = .80), which is comparable to what Postmus, Plummer, and Stylianou (2016) reported (.89, .87, .89, and .86, respectively). An examination of the construct validity of the SEA-12 indicated a significant correlation between economic abuse scores as measured by the SEA-12 and the composite score for the Abusive Behavior Index (r = .775, p < .01; Postmus, Plummer, & Stylianou, 2016).
IPV
Frequency of psychological, physical, and sexual victimization was measured using a modified version of the Abusive Behavior Index (ABI-R; Postmus, Stylianou, & McMahon, 2016). The original ABI (Shepard & Campbell, 1992) has 30 items, with two main subscales: Physical and Psychological Abuse. Following further testing using confirmatory factor analyses and exploratory factor analyses, six questions were removed and three subscales were created to assess physical, psychological, and sexual IPV. All responses were made on a 5-point scale ranging from 1 (never) to 5 (very often). Sample items for psychological IPV included “called you a name and/or criticized you” and “told you that you were a bad person.” Sample items for physical IPV included “threatened to hit or throw something at you” and “used a knife, gun, or other weapon against you.” The three items classified as sexual IPV were “pressured you to have sex in a way that you didn’t like,” “physically forced you to have sex,” and “physically attacked the sexual parts of your body.” The original ABI was found to have good reliability and construct validity (Postmus & Severson, 2006; Shepard & Campbell, 1992). As completed by the present sample, each subscale had strong internal consistency: psychological IPV α = .92, physical IPV α = .93, and sexual IPV α = .85.
Sociodemographic characteristics
Participants were asked to indicate the following sociodemographic characteristics: their age (in years); whether they were born in the United States (yes/no); their current marital status (married, civil union/partnership, separated, divorced, widowed, or single); whether they were financially responsible for children (yes/no); their current employment status (yes/full-time, yes/part-time, or no); and average annual household income. The educational attainment of participants was not included as a sociodemographic variable because it was not assessed during the baseline interview.
Analytic Strategy
The analyses began with a missing value analysis using SPSS. This analysis showed that missing values were less than 3.5% across all variables. In addition, Little’s missing completely at random test was nonsignificant (p = .251) indicating that the pattern of missing data was not significantly different from a pattern of randomly missing data. Preliminary data analysis revealed that two of the economic abuse subscales (i.e., economic exploitation and economic control) failed to meet the normal distribution requirement; they were significantly skewed even after transformation. Therefore, the SEA-12 subscales were used in the descriptive analyses, but only the composite mean score of economic abuse derived from the entire SEA-12 was used in the regression analyses.
Next, descriptive statistics were generated for sociodemographic variables (i.e., age, immigration status, relationship status, financial responsibility for children, employment, and annual household income), mental health symptoms (i.e., depression, anxiety, and PTSD), and IPV scores (i.e., psychological, physical, sexual, and economic). Pearson’s correlations were calculated to assess the relationship between mental health symptoms, IPV scores, and participants’ sociodemographic characteristics (see Table 3).
Last, three hierarchical multiple regression models were conducted to examine whether the addition of economic abuse improved the prediction of mental health outcomes over and above participants’ sociodemographic characteristics and experiences of psychological, physical, and sexual IPV (hereafter referred to as IPV experiences). Prior to running the regression models, a series of tests were conducted to determine whether the data met the assumptions of multiple regression. The assumption of linearity was met, as assessed by examining partial regression plots and a plot of studentized residuals against the predicted values. The assumption of independence of residuals was met, as assessed by calculating Durbin–Watson statistics: 2.027 for Depression, 1.888 for Anxiety, and 1.848 for PTSD. The assumption of homoscedasticity was met, as assessed by visual inspection of a plot of studentized residuals versus unstandardized predicted values. There was no evidence of multicollinearity, as assessed by tolerance values greater than 0.1. There were no studentized deleted residuals greater than ±3 standard deviations and no values for Cook’s distance above 1. The assumption of normality was met, as assessed by P-P Plot. All regression analyses were conducted using SPSS Statistics 24.
The first step for each model was a multivariate regression looking at the relationship between sociodemographic characteristics (i.e., age, born in the United States, relationship status, financial responsibility for children, employment status, and annual household income less than US$10,000) and mental health (i.e., depression, anxiety, and PTSD). In the second step, psychological IPV, physical IPV, and sexual IPV were entered. In the final step, economic abuse was entered. By simultaneously controlling for other forms of IPV and sociodemographic factors, the third step provided the most stringent test of the association between economic abuse and mental health outcomes.
Results
Frequency of Mental Health Symptoms and Economic Abuse
Descriptive statistics revealed that on average, the sample experienced modest symptoms of PTSD (M = 2.5, SD = 0.7), anxiety (M = 2.4, SD = 0.9), and depression (M = 2.3, SD = 0.7; see Table 1). The most frequent symptoms endorsed on each mental health scale were “flashbacks or sudden, vivid distracting memories” for PTSD, “worrying too much about different things” for anxiety, and “feeling happy” (item reversed coded) for depression.
Participant Characteristics (N = 245).

Note. PTSD = posttraumatic stress disorder; IPV = intimate partner violence.
When examining the economic abuse experiences of Latinas participating in this financial empowerment program, the results indicated that the most frequent form of economic abuse noted was economic control (M = 3.1, SD = 1.2), followed by economic exploitation (M = 2.6, SD = 1.3), and employment sabotage (M = 2.0, SD = 1.1). The most typically experienced tactics for each subtype were “make important financial decisions without talking to you first” for economic control, “spend the money you needed for rent or bills” for economic exploitation, and “do things to keep you from going to your job” for employment sabotage (see Table 2).
Economic Abuse Means and Standard Deviations for Latinas (N = 245).
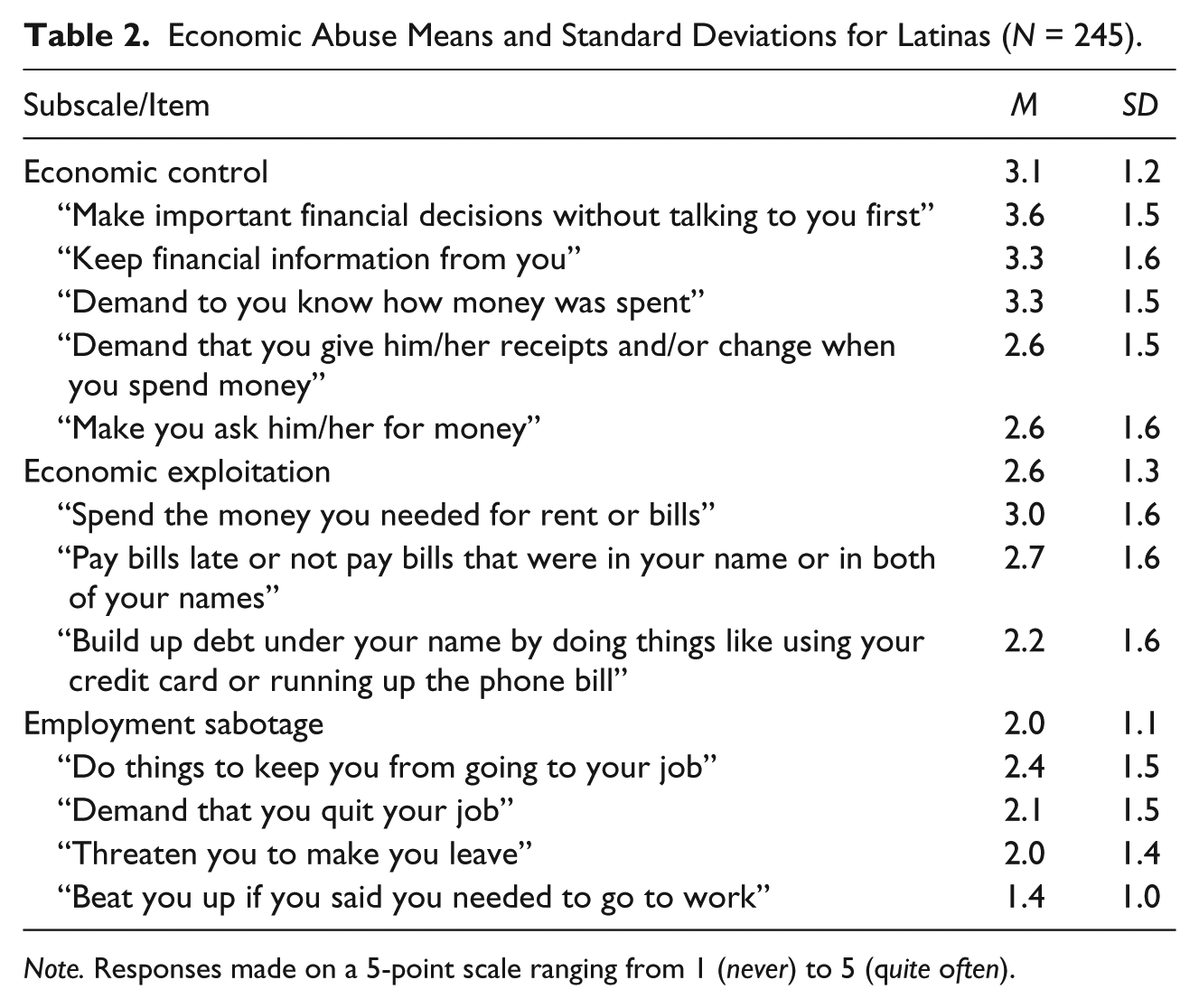
Note. Responses made on a 5-point scale ranging from 1 (never) to 5 (quite often).
Relationship Between Economic Abuse and Mental Health Symptoms
As shown in Table 3, the results showed that depression, anxiety, and PTSD were significantly correlated with each other (ps < .01). Likewise, significant associations were found among physical, psychological, sexual, and economic forms of IPV (ps < .05). All forms of IPV victimization were also significantly associated with each mental health outcome (ps < .01). As already described, regression models were run for each mental health outcome of interest (i.e., depression, anxiety, and PTSD).
Correlations Among IPV Scores, Mental Health Symptoms, and Participant Characteristics (N = 245).
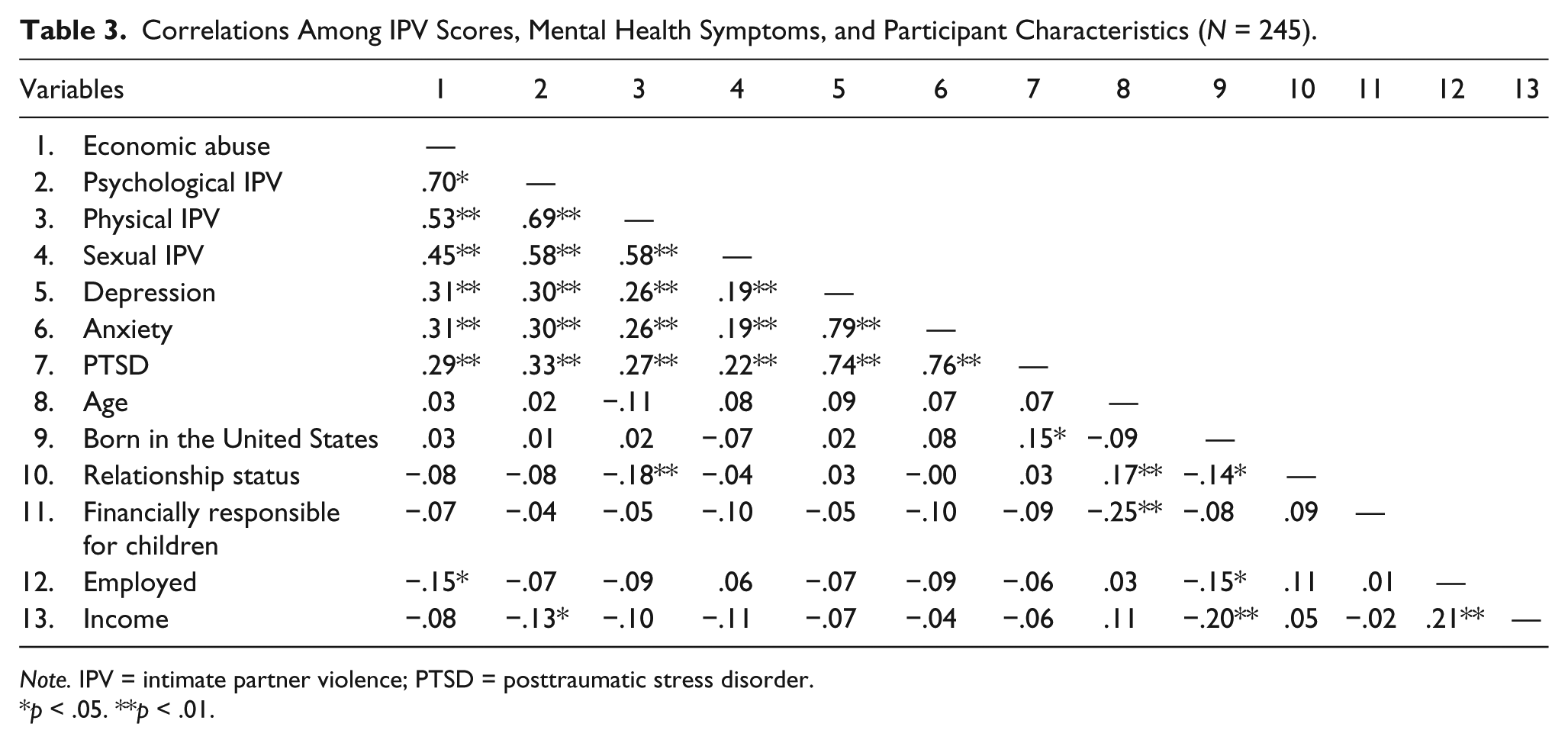
Note. IPV = intimate partner violence; PTSD = posttraumatic stress disorder.
p < .05. **p < .01.
Depression
In the model predicting depression, Step 1 (which included only sociodemographic characteristics) was not statistically significant, R2 = .022, F(6, 232) = .855, p = .529; adjusted R2 = −.004. The addition of IPV experiences to the prediction of depression (Step 2) led to a significant increase in R2 of .084, ∆F(3, 229) = 7.187, p < .001. However, the addition of economic abuse to the prediction of depression (Step 3) did not lead to a statistically significant increase in R2, ∆R2 = .014, ∆F(1, 228) = 3.566, p = .060 (see Table 4).
Hierarchical Multiple Regression Predicting Depression, Anxiety, or PTSD From Participant Characteristics and Abuse Experiences (N = 245).
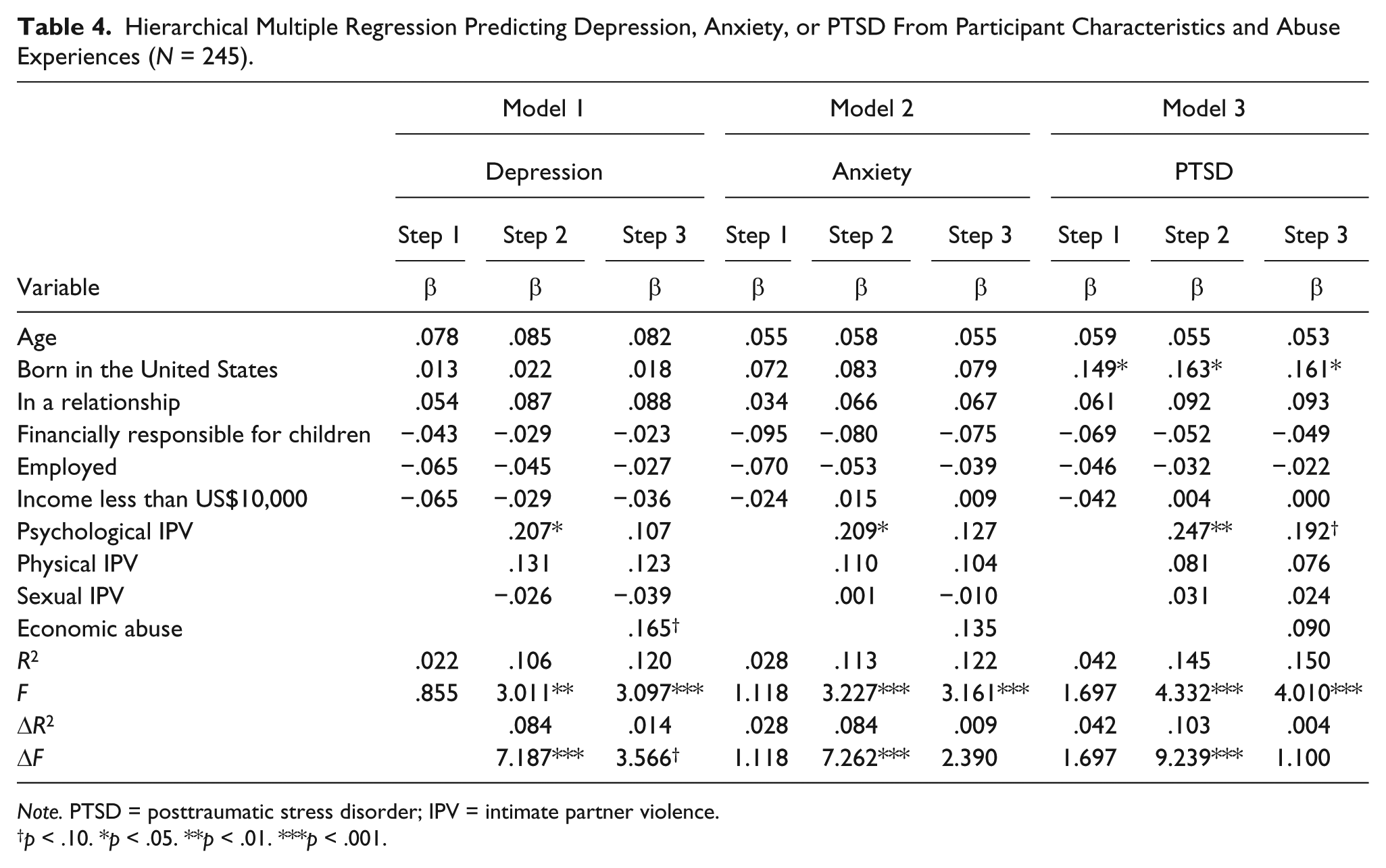
Note. PTSD = posttraumatic stress disorder; IPV = intimate partner violence.
p < .10. *p < .05. **p < .01. ***p < .001.
Anxiety
In the model predicting anxiety, Step 1 (which included only sociodemographic characteristics) was not statistically significant, R2 = .028, F(6, 232) = 1.118, p = .352; adjusted R2 = .003. The addition of IPV experiences to the prediction of anxiety (Step 2) led to a statistically significant increase in R2 of .084, ∆F(3, 229) = 7.262, p < .001. However, the addition of economic abuse to the prediction of anxiety (Step 3) did not lead to a statistically significant increase in R2, ∆R2 = .009, ∆F(1, 228) = 2.390, p = .123 (see Table 4).
PTSD
Similarly, in the model predicting PTSD, Step 1 (which included only sociodemographic characteristics) was not statistically significant, R2 = .042, F(6, 232) = 1.697, p = 122; adjusted R2 = .017. The addition of IPV experiences to the prediction of PTSD (Step 2) led to a statistically significant increase in R2 of .103, ∆F(3, 229) = 9.239, p < .001. However, the addition of economic abuse to the prediction of PTSD (Step 3) did not lead to a statistically significant increase in R2, ∆R2 = .004, ∆F(1, 228) = 1.100, p = .295 (see Table 4).
Discussion
The present study provides much needed information about the economic abuse experiences reported by a sample of Latinas seeking domestic violence advocacy services. Inspection of the mean responses to items assessing economic abuse revealed that economic control—the abuser’s attempts to control or restrict the victim’s resources—was the most common form of economic abuse reported. The second most common economic abuse strategy reported was economic exploitation, which involves the depletion of existing funds and/or unilateral creation of debt by the abuser. A number of Latinas also reported employment sabotage as a tactic used by their partners, which includes doing things to keep them from working outside of the home (Stylianou et al., 2013). These results are consistent with findings reported by Galvez and colleagues (2011), indicating that Latino batterers engage in work-related tactics to control their partners.
Interestingly, inspection of the mean ratings across subtypes of economic abuse revealed that employment sabotage was reported less often relative to other types of economic abuse in this sample. It should be noted that nearly half of the Latinas in this sample were low-income and unemployed at the time of the study. Hence, it is unclear whether employment sabotage victimization played a role in their unemployment status or vice versa. That is, it could be that the socioeconomic characteristics of this sample can explain the limited experiences of employment sabotage victimization reported in this study. Additional research is needed to better understand when and how employment sabotage is used as a form of economic abuse against Latinas, particularly low-income women.
The primary research question examined in this study was whether experiencing economic abuse is associated with mental health symptoms above and beyond other forms of IPV, as reported by a relatively large sample of Latina IPV survivors seeking advocacy services. On average, this sample reported experiencing modest symptoms of depression, anxiety, and PTSD. Inspection of the simple correlations suggested that economic abuse was positively associated with self-reported symptoms of depression, anxiety, and PTSD. However, when examined in regression models, economic abuse did not contribute significantly to the prediction of mental health above and beyond sociodemographic variables and other forms of IPV (although a trend was noted in the model predicting depression). It is possible that significant relationships between economic abuse and mental health could become more apparent with a larger sample, or with a sample that reports a wider range of mental health symptoms.
While economic abuse might not contribute to a mental health functioning after taking sociodemographic factors and other forms of IPV into account, it should be noted that economic abuse likely has other negative implications with respect to survivors’ well-being. For instance, the literature on IPV consistently shows that financial hardships represent important obstacles to help-seeking and ending abusive relationships, particularly among economically disadvantaged victims (e.g., Bauer et al., 2000; Hass, Dutton, & Orloff, 2000). Hence, financial dependence that is the result of economic control tactics may put individuals at risk of prolonged exposure to abusive experiences and may exacerbate the financial barriers (e.g., poverty, job loss) that prevent Latinas from escaping abusive relationships.
Furthermore, similar to previous research (e.g., Hazen et al., 2008; Kelly, 2010), this study found evidence to suggest differential impacts of psychological, sexual, physical, and economic IPV on mental health. Although all forms of IPV included in the study were related to depression, anxiety, and PTSD at the bivariate level, only psychological IPV remained a significant predictor of depression, anxiety, and PTSD after accounting for sociodemographic characteristics. Nevertheless, more research is needed to continue examining the differential impact of different forms of IPV victimization on the mental health symptoms of Latinas.
It is also noteworthy that our findings are consistent with research indicating that physical IPV is positively associated with experiences of economic abuse, a pattern that is important to recognize when working with IPV survivors (Outlaw, 2009). Routine screening for economic abuse should be performed among women seeking services from IPV agencies and other healthcare providers (see Postmus, Plummer, et al., 2012, for discussion). The association between economic abuse and physical IPV highlights the importance of financial empowerment in IPV interventions, as studies examining the effectiveness of financial empowerment programs have shown improvements in financial literacy, financial behavior, economic self-efficacy, and economic self-sufficiency among IPV victims (Postmus et al., 2015; Postmus & Plummer, 2010; Postmus et al., 2013). Finally, the results of this study have implications for policymakers. Specifically, more direction is needed in federal policies such as the Violence Against Women Act and the Victims of Crime Act to encourage greater attention to economic abuse and economic empowerment in the practice arenas.
Limitations
As with most studies, there are a number of limitations that should be considered when interpreting the findings of the present study. First, because the data examined were cross-sectional in nature, we cannot determine direct cause-and-effect relationships. Second, although IPV victimization (including economic abuse) was linked to symptoms of depression, anxiety, and PTSD at the bivariate level, IPV victimization along with sociodemographic factors accounted for only modest variance in mental health problems. Thus, other interpersonal, sociocultural, socioeconomic, and sociopolitical factors need to be considered when attempting to understand the factors that influence the mental health of Latina survivors. In addition, as with all self-reported retrospective measures, the data gathered for this research may have been influenced by recall problems, response distortion due to social desirability, and/or reluctance to report certain personal problems (e.g., emotional symptoms, victimization experiences).
It should also be noted that our sample was not representative of the larger population of Latina survivors in the United States. Given that all participants were recruited from agencies that provide help to IPV survivors, data from women who were not receiving assistance from a domestic violence agency were not gathered in the present study and were not represented in our analyses. Thus, it is unknown whether our findings generalize to Latina IPV survivors who do not seek assistance from domestic violence agencies. For example, it is possible that economic abuse may influence mental health more strongly among IPV survivors who are not involved with domestic violence agencies.
Moreover, most of the women in our sample reported being financially responsible for children, only half were employed, nearly half reported an annual household income of less than US$10,000, and all were living in the United States. These factors (e.g., living in poverty with dependent children) are important to keep in mind when thinking about the generalizability of the associations observed in this study. Future investigations should examine experiences of economic abuse and associated mental health symptoms in a more diverse sample of Latina IPV survivors.
In addition, it should be noted that the category of “Latina” includes a heterogeneous group of women with respect to country of origin and cultural heritage. Future research examining economic abuse and mental health would do well to distinguish between women from Mexico, Puerto Rico, Cuba, Central and South America, and other Hispanic origins. Similarly, future research should include non-Latino samples (African Americans, non-Hispanic Caucasians) to determine whether our findings generalize across ethnic/racial groups. Furthermore, though the scales and other materials were translated into Spanish using rigorous translation and back translation methods, additional psychometric work is needed to further establish the validity of these measures in Latina samples.
Finally, it should be noted that recent studies indicate a potential influence of educational attainment on the economic abuse experiences of women (Postmus, Plummer, et al., 2012). Unfortunately, the data set utilized for the present study did not contain information on the educational attainment of participants. Additional research is needed to examine the role that educational attainment might play in the association between economic abuse and mental health symptoms.
Conclusion
There are few investigations on economic abuse in the general U.S. population, and even less is known about economic abuse perpetrated against Latinas in the United States. The present study attempted to fill these gaps by examining the relationship between economic abuse victimization and mental health symptoms in a sample of Latinas seeking IPV advocacy services in the United States. Overall, the results of the present study suggest that economic abuse may not contribute significantly to symptoms of depression, anxiety, or PTSD after considering the influence of sociodemographic factors and other forms of IPV. Nonetheless, additional research is needed to advance our understanding of how economic abuse influences victims’ general functioning, their help-seeking behaviors, and their victimization experiences over time.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by The Allstate Foundation, Economics Against Abuse Program. The opinions and conclusions expressed herein are solely those of the authors and should not be construed as representing the opinions or policies of The Allstate Foundation. America L. Davila was supported by grants from the NASA New Jersey Space Grant Consortium (NJSGC) through the Research in Science & Engineering (RiSE) program at Rutgers University.