
Abstract
Previous research has documented that women who were sexually abused in childhood are also often victims of sexual abuse in adulthood. In the current study, we investigated the relationship between the phenomenon of sexual revictimization and personality organization (PO) conceptualized in accordance with the Otto Kernberg’s theory. The central hypothesis was that women with borderline personality organization (BPO) and neurotic personality organization (NPO) differ in terms of the occurrence of revictimization and its features. We predicted that women with BPO would experience revictimization more often, and that it would be characterized by features determining its higher severity than in women with NPO. In our study, 119 Polish adult women completed measures of PO and experiences of sexual violence in childhood and adulthood. The results supported the predicted relationships. After controlling for participants’ age, we showed that women with a close to borderline level of personality organization (cBPO) are at the greater risk of experiencing revictimization than those with NPO, in particular the revictimization involving penetration and by the previously known offender. Moreover, specific structural features related to BPO were found to have particular associations: Fear of Fusion (FF) was associated with the experience of revictimization; Identity Diffusion (ID), Primitive Defense Mechanism (PDM), FF, and Impaired Reality Testing (IRT) with penetration during revictimization; and PDM and IRT with revictimization by the previously known offender. Our findings suggest the importance of taking into account PO in estimating the risk of revictimization, as well as in therapy programs aimed at reducing this risk.
The Phenomenon of Revictimization Following Child Sexual Abuse (CSA)
CSA is a serious problem that occurs at significant rates of 8% and 31% among women worldwide (Barth, Bermetz, Heim, Trelle, & Tonia, 2013). Similar results were obtained for the Polish population, indicating rates ranging between 11% and 30.7% (Izdebski, 2012; Sajkowska, 2017).
Despite the significant scale of the problem, prior to the 1990s, it was not a subject of social discussion or research studies in Poland (Sajkowska, 2003). Nevertheless, since that time, both social and research interest has been primarily directed toward children. The psychological status of child sexual abuse survivors (CSAS) in adulthood has much less frequently been explored.
However, research has consistently indicated that adult victims of CSA suffer from different psychological and interpersonal problems (e.g., Cutajar et al., 2010; Jonas et al., 2011). The findings showed, among other things, linkages between CSA and later adult sexual assault (ASA) in women. According to literature reviews, CSAS are between 2 and 3 times more likely to experience sexual victimization as adults (e.g., Arata, 2002; Classen, Palesh, & Aggarwal, 2005; Messaman-Moore & Long, 2003; Roodman & Clum, 2001).
Numerous models that aim to explain this phenomenon of sexual revictimization have been developed up to date. These models describe the possible causal relationships between CSA and a heightened vulnerability to ASA. At the same time, it should be taken into consideration that the reported relationship between CSA and ASA might—to some extent—be apparent. For example, it could reflect a greater willingness among CSA survivors to report subsequent abuse. This issue was specifically addressed by Russell (1986) who, regarding incest victims, pointed out that CSAS are more sensitive to various types of sexual abuse and hence report it more often. However, as also indicated by Russell (1986), although this factor should be taken into account in revictimization analyses, it does not exclude the possibility of an actual relationship between CSA and ASA.
To date, most of the models attempting to explain the link between CSA and ASA have focused on the analysis of individual variables, and less often—on the integration of different factors (see Arata, 2002; Classen et al., 2005; Messaman-Moore & Long, 2003; Roodman & Clum, 2001). Among the most often analyzed variables are those related to affect and emotion regulation processes (e.g., Batten, Follette, & Aban, 2001; Filipas & Ullman, 2006; Messman-Moore, Walsh, & DiLillo, 2010; Messman-Moore, Ward, & Zerubavel, 2013; Orcutt, Cooper, & Garcia, 2005) and those related to information processing in interpersonal situations (e.g., Field et al., 2001; Messman-Moore & Brown, 2006; VanZile-Tamsen, Testa, & Livingston, 2005). Such studies are of great value, because they allow in-depth analysis of potential impact of the included variables to be conducted. However, the variables are often analyzed in mutual isolation, which could be seen as a limitation.
Regardless of the complexity of the models, studies have often provided conflicting results, which are typically explained by referring to the modifying effects of other variables or the specifics of the study group (see Arata, 2002; Classen et al., 2005; Messaman-Moore & Long, 2003; Roodman & Clum, 2001). In our view, the inconsistencies in results also support the need for consideration of more general constructs that could further allow combining the impact of more specific factors, or even the recognition of the possible heterogeneity of the paths of revictimization. Constructs covering diversity in patterns of mental functioning (e.g., types of personality structure) might be particularly valuable, because, hypothetically, each such single pattern could be associated with different specific risk factors for revictimization.
Previous studies were also limited in that they did not examine the characteristics of revictimization. The importance of this is, however, connected with the fact that certain features of sexual aggression have been found to affect the severity of its consequences. In particular, such features of ASA as abuse by a previously known offender (Campbell et al., 1999), higher numbers of incidents (Miller et al., 1978; Santiago, McCall-Perez, Gorcey, & Beigel, 1985), higher numbers of offenders (Machado, de Azevedo, Facuri, Vieira, & Fernandes, 2011), or ASA involving penetration (Koss & Dinero, 1989) were associated with more severe consequences in the victims such as more frequent and intense posttraumatic stress disorder (PTSD) or depression.
Level of PO and Sexual Victimization
In this study, we focused on personality structure as a factor accounting for differences in rates and characteristics of revictimization in CSAS. We based our understanding of personality and its structure on Kernberg’s (1996, 2004) theory, which emphasizes the relationship between personality and functioning in interpersonal relations. In his model, Kernberg (1976, 1983, 1996, 2004) indicated how psychological structures develop based on early childhood relational experiences, while in adult life, they influence interpersonal relationships and therefore affect the further interpersonal experiences of the person. In our study, we were particularly interested in investigating the second of these dependencies.
The influence of personality structure on the sphere of interpersonal relations is linked to its superior, regulatory function. It involves conditioning the selection, perception, processing, and reaction to incoming interpersonal stimuli. The individual course of these processes is rooted in the type of personality structure, referred to as the level of PO. Kernberg’s (1996, 2004) theory provides descriptions of three levels of PO: neurotic (NPO), borderline (BPO), and psychotic (PPO), where an individual’s level of PO is determined by the course of their development and it is relatively stable over the course of life. In particular, each type of PO can be characterized with regard to the developmental level of the structural features of identity integration, reality testing, and maturity of defense mechanisms. Identity integration refers to the level of integration of concepts of self and significant others. Reality testing “refers to the capacity to differentiate self from nonself, intrapsychic from external stimuli, and to maintain empathy with ordinary social criteria of reality” (Kernberg, 1996, p. 120). Maturity of defense mechanisms refers to the dominant defensive propensities, with splitting and its derivatives being considered less mature than repression and its derivatives (Kernberg, 1996, 2004; Yeomans, Clarkin, & Kernberg, 2015).
Each PO level predisposes to a particular way of functioning, including creating particular relationships that favor specific experiences in these relationships. It can be assumed, therefore, that the level of PO will also affect the risk of sexual victimization. In the present study, we specifically concentrated on BPO and NPO. We decided to exclude individuals with PPO, as some features of their functioning (way of communicating, describing of self and one’s experiences) could impair the accuracy of collected data.
BPO differs from NPO in terms of a domination of the splitting defense mechanism, which organizes the internal world and is responsible for identity diffusion as well as vulnerable reality testing. As a result, individuals with BPO reveal different manifestations of ego weakness, such as impaired ability to regulate affects, poor anxiety tolerance, and poor impulse control, including of aggressive and sexual impulses. In consequence, individuals with BPO can be further characterized with major disturbances in interpersonal functioning: They present a rather superficial and fragmented image of the self and others that limits their understanding of their own and others’ motivations. Moreover, their functioning is based rather on wishful thinking than on a realistic judgment of oneself, others, and the situation. Hence, the ability to experience trust and comfort in interpersonal relations is also limited, which results in frequent changes of partners and the fulfillment of sexual needs in random relations (see Kernberg, 1996, 2004; Yeomans et al., 2015). Interestingly, the same features have been shown to increase the risk of sexual victimization. For example, diminished awareness of experienced affects may impair the ability to use emotions as a signal of potential risk (Messman-Moore et al., 2013), and increased sexual activity may result in attracting potential perpetrators and being perceived by them as an easy target (Mandoki & Burkhart, 1989; Mayall & Gold, 1995; Russell, 1986). Several studies have directly suggested that individuals with BPO indeed suffer from increased experiences of sexual victimization (Sansone, Chu, & Wiederman, 2011; Sansone & Sansone, 2011). However, no previous studies have addressed the relationship between PO and revictimization in CSAS.
In contrast, in individuals with NPO, where the splitting mechanism is replaced with the more mature repression mechanism, identity is relatively integrated and reality testing remains intact, even in stressful situations. As a result, individuals with NPO are able to regulate and process their affects more effectively. The images of self and others are, at the same time, multifaceted, complex, coherent, and realistic. These features lay the ground for the ability to formulate stable, satisfying, and intimate relationships, where sexuality is usually combined with emotional involvement. Individuals with NPO are able to care for both other people and themselves, which includes setting limits on one’s own aggressive impulses and in one’s relations with others. Therefore, the risk of sexual aggression seems to be decreased (see Kernberg, 1996, 2004; Yeomans et al., 2015).
Present Study
The purpose of the present study is to test two hypotheses. The first concerns the differences between individuals with BPO and NPO in terms of the occurrence of revictimization. Given the parallels between BPO and intrapsychic risk factors for sexual violence, we assumed that in the BPO group, the occurrence of revictimization would be significantly higher than in the NPO group. Furthermore, we wanted to ascertain which structural features of BPO are particularly related to the occurrence of revictimization.
Second, we sought to address the limitations of previous research by examining the characteristics of revictimization. Thus, the second hypothesis concerns the differences between individuals with BPO and those with NPO in terms of the qualities of revictimization: the number of episodes and offenders, the invasiveness of the experience understood as the level of involvement of the person’s body by the offender in the course of sexual activity (Beisert, 2012), and the proximity of the relationship between the victim and the offender.
For the purpose of the study, CSA was defined as the engaging of a child (a person not older than adolescence) by an adult (a person over 18 years of age) in any sexual activity, including that of noncontact form 1 ; ASA was defined—by analogy to CSA—as the engaging of an adult (a person over 18 years of age) in any nonconsensual sexual activity, including that of noncontact form. Consequently, revictimization was conceptualized as the experience of ASA (at least one such incident) by a person with CSA experience (at least one such incident). A detailed description of the forms of sexual activities taken into account for CSA and ASA is provided in Table 1, which outlines the methods used.
Subsequent Items of QESAC and QUSEA.

Note. For each item, women were asked to answer, if it described their experience, and—if confirmed—mark its relevant characteristics in terms of frequency and number of offenders: (a) one incident, (b) a few (2-4) incidents by the same offender, (c) a few (2-4) incidents by different offenders, (d) many incidents by the same offender, or (e) many incidents by different offenders, as well as the type of relationship with the offender: (a) a close relative, (b) a distant relative, or (c) an acquaintance/unknown offender. QESAC = Questionnaire of the Experiences of Sexually Abused Child; QUSEA = Questionnaire of Unwanted Sexual Experiences in Adulthood.
An additional variable that was controlled for was the age of the participants, as we assumed this to have an association with the number of possible situations that an individual might encounter in a lifetime in which they might have been victimized. In other words, the participants’ ages could confound the association between PO and revictimization in adulthood, as with younger individuals, less time would have elapsed for revictimization to have occurred (see Muehlenhard, Highby, Lee, Bryan, & Dodrill, 1998). Another variable with a potentially confounding influence is the physical disability, which has been described as increasing the risk of sexual victimization (Alriksson-Schmidt, Armor, & Thibadeau, 2010; Martin et al., 2006). However, as none of the participants had any type of physical impairment, this variable was not included in the analysis.
Materials and Methods
Data were collected as part of a larger study on the determinants of sexual revictimization in the lives of female CSA survivors (Izdebska, 2016).
Participants and Procedure
The research group consisted of Polish women. The inclusion criteria consisted of experience of CSA, age above 23 years, and BPO or NPO. The lower age limit was chosen on the assumption that a certain period of time (take as 5 years) had to pass for the revictimization to possibly occur.
Women with PPO were excluded on the basis of their psychiatric treatment history. As suggested in the literature (Kernberg, 1984; Sandell & Bertling, 1996), we assumed that individuals with PPO had a high probability of a history of periods of psychiatric hospitalization. These individuals were thus identified on the basis of such experiences—namely, psychiatric hospitalization of longer than 6 months. 2 This period was taken as the threshold to differentiate individuals with relatively short-lasting episodes of decompensation, from those with more severe and chronic disorders, which could carry a higher risk of confounding their responses. As, in Poland, most patients falling into the first category are hospitalized for no longer than 10 weeks, we assumed that a history of more than 6 months of treatment would suggest more chronic and severe disturbances in functioning, including those with a psychotic background.
The study was entirely anonymous and only volunteers who expressed their informed consent were included. The participants were not issued any tangible incentives for their involvement.
The study design was approved by the Ethics Committee for Research Designs at the authors’ University. All the assessments were performed by psychologists experienced in conducting research projects, and in conducting psychological interventions. Each participant was also entitled to a few nonpaid individual therapeutic meetings in case of lasting discomfort connected with participation in the study.
The research was conducted between March 2013 and March 2014 and proceeded in two stages.
Preliminary study
The main objective of this stage of the study was to select women who met the inclusion criteria. For this purpose, the questionnaire on CSA was administered, joined by the questionnaire on PO and personal data, including psychiatric treatment history. Women were provided with detailed information on the purpose and procedures of the study, and if they agreed to take part in the further stage of the study, they were requested to leave their phone numbers or email addresses.
To increase sample diversity, we recruited participants in two ways:
Using direct contact among female students of Adam Mickiewicz University of Poznań and the University of Social Sciences and Humanities - University Campus in Poznań. After providing informed consent, the participants received envelopes containing questionnaires and briefing sheets. They took part in the study as an optional class activity. The completed questionnaires were returned to the researcher in a sealed envelope.
Using the Internet. Computer versions of the assessment tools were constructed and made accessible online. Information on the study was spread through online and street advertisements. Those who accessed the study website, after providing their informed consent, were directed to the briefing sheet and questionnaires.
In-lab study
The main stage of the study consisted of individual personal meetings with research assistants, during which the women completed the rest of the study materials. The current study represents part of a larger project on sexual revictimization, and each meeting lasted 45 to 75 min. At the end of the appointment, participants were thanked for their participation, asked about their current comfort levels, and reminded of the availability of nonpaid sessions with a therapist.
A total of 1,363 women over 23 years of age took part in the preliminary study, and 451 of them reported CSA. Given that the focus of the study was on revictimization, the remaining participants were excluded from further proceedings. Of the 451 women, 250 initially expressed interest in further participation in the study by leaving their contact data; six of these were excluded due to their history of psychiatric treatment; 125 resigned later either by not answering phone calls or emails, or by not showing up for the meeting. The final study sample consisted of the remaining 119 women. On account of the research procedure, consisting of the individual assessment sessions during the main stage of the study, no subject needed to be excluded due to missing data. An overview of the specific inclusion and exclusion criteria is given in Figure 1.
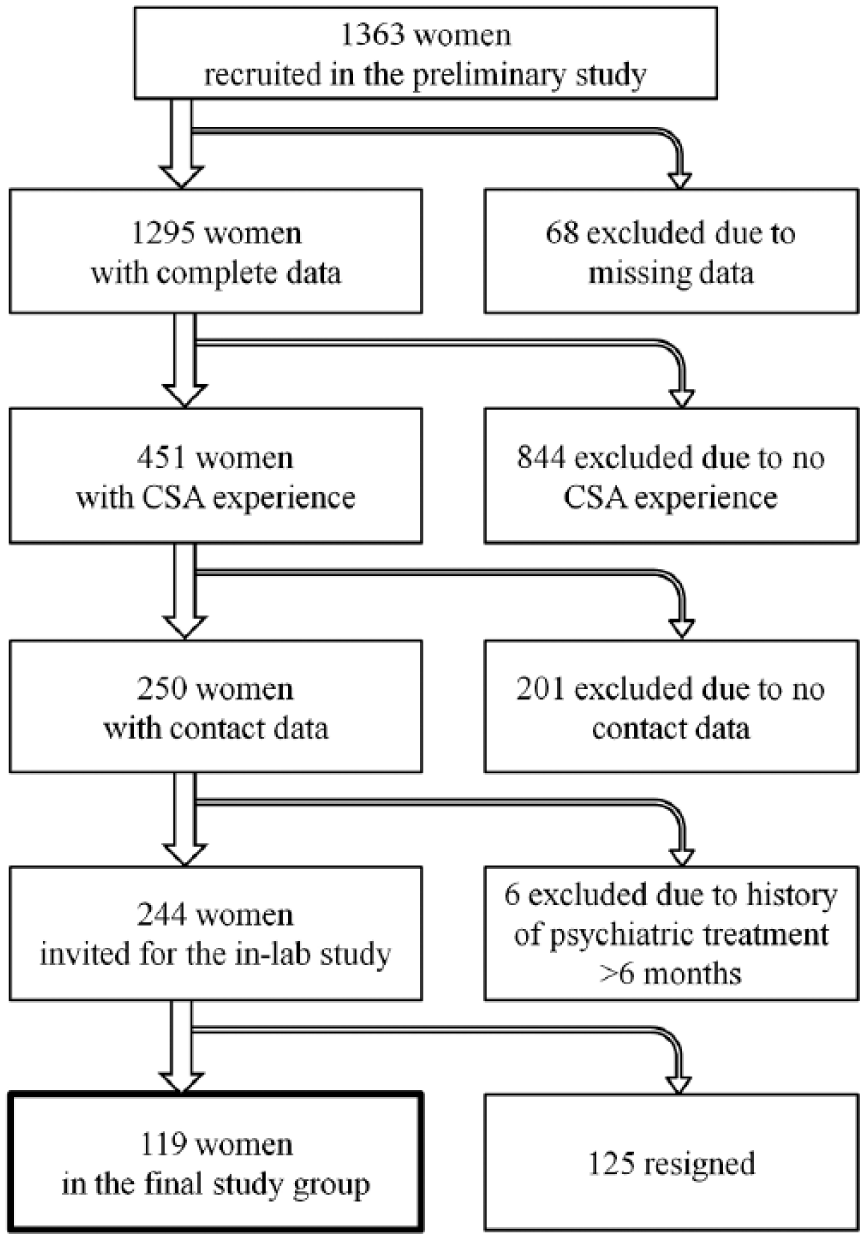
Inclusion and exclusion criteria for study population.
Measures
The following methods were used to measure the variables:
Experience of CSA was measured by means of the Questionnaire of the Experiences of Sexually Abused Child (QESAC), a modified version of a scale constructed by Beisert (2012). This instrument allows for assessing whether the person was exposed to sexual abuse during childhood (until the age of 11-12) by an adult (a person over 18 years of age) and—if tested positive—for evaluation of the features of the abuse: intrusiveness, frequency, type of relationship with the offender, and number of offenders. QESAC is similar in construction to the method of Finkelhor (1979), but was developed by the Polish author, meaning that it can be considered linguistically and culturally appropriate for a Polish population. It consists of 16 items describing different forms of sexual activities, arranged in line with growing invasiveness (Table 1) and organized in the form of a table. For each such item, women were asked to answer, if it described their experience, and—if confirmed—mark its relevant characteristics in terms of frequency and number of offenders: (a) one incident, (b) a few (2-4) incidents by the same offender, (c) a few (2-4) incidents by different offenders, (d) many incidents by the same offender, or (e) many incidents by different offenders, as well as the type of relationship with the offender: (a) a close relative, (b) a distant relative, or (c) an acquaintance or an unknown offender.
Only minor modifications of the original tool by Beisert (2012) were made, and they consisted primarily of adapting it to the specifics of the current study. For example, an instruction was altered to indicate that childhood was to be regarded as a period lasting until about 11 to 12 years of age; in the original version, this was extended to 15 years of age. There were also some changes made to the description of individual items: For example, two separate items from the original version (witnessing sexual intercourse and witnessing exposure of intimate parts and sexual activities) were combined into one item.
Experience of ASA was measured by means of the Questionnaire of Unwanted Sexual Experiences in Adulthood (QUSEA), which is formally and essentially an equivalent of QESAC for assessing experience of sexual violence in adulthood (after the age of 18) and—if tested positive—for evaluating its features. The items of QUSEA correspond to those of QESAC. Respectively—for the experience of adulthood—the instruction accompanying the method was reformulated: The subjects were asked to indicate whether any of the activities enumerated in the tool ever occurred in their lives after 18 years of age against their will.
Both categorical and dimensional PO scores were obtained by means of the Borderline Personality Inventory (BPI) of Leichsenring (1999) in the Polish adaptation of Cierpiałkowska (2001). BPI is a self-description measure based on Kernberg’s structural theory of personality. BPI is recommended for screening of BPO and for borderline personality classifications (Chabrol & Leichsenring, 2006; Leichsenring, 1999).
The BPI consists of 53 items followed by a “yes–no” response format, and provides an overall score and four subscale scores for: (a) Identity Diffusion (ID), which refers to the individual’s sense of confused identity; (b) Primitive Defense Mechanism (PDM), which refers to the dominance of splitting and its derivatives; (c) Impaired Reality Testing (IRT), which refers to perceptual abnormalities; and (d) Fear of Fusion (FF), which refers to fear of close, intimate relationships. Another scale of the BPI is referred to as the Cut-20 scale; this was empirically separated as a collection of the 20 items with the strongest discriminative power for the purpose of determining borderline personality disorder.
The dimensional scores were computed by summing the points in each of the subscales. The categorical diagnostic evaluation was completed on the basis of the result on the Cut-20 scale. Originally, Cut-20 results ≥ 10 were recommended as the cutoff point for the proper classification of BPO. However, due to the low average results obtained in the study population, we used Cut-20 ≥ 8. This value creates a higher risk of misallocating people without BPO to this group than 10 or 9 points. 3 In consequence, we could not assume that all individuals qualified for the interval were characterized by BPO, but only that the intensity of the structural features of BPO was relatively high in this group. The participants in this group were thus referred to as characterized by a level of personality organization close to borderline (cBPO). For assignment to the NPO, we used Cut-20 scores ≤ 4. Individuals who obtained 5 to 7 points on the Cut-20 scale were excluded from the analyses comparing NPO with cBPO. The number of participants in each group is shown in Table 2.
The Criteria for the Classification of Subjects Into Compared Groups Based on the Cut-20 Results and Their Numbers (N = 119).

Note. cBPO = close to borderline personality organization; NPO = neurotic personality organization.
Cierpiałkowska (2001) reported a Cronbach’s alpha of α = .85 for the ID subscale, α = .78 for the PDM subscale, α = .60 for the IRT subscale, α = .73 for the FF subscale, and α = .86 for the Cut-20 subscale. These measures are comparable with the internal consistency of the original version of BPI (α = .85-.68; Leichsenring, 1999).
A brief demographic form assessing age, education level, marital status, and history of psychiatric treatment was included as well.
Data Analysis
The statistical analysis was performed as follows:
To test for relationship between categorical PO scores (NPO/cBPO) and revictimization (revictimization/no revictimization) and its features (intrusiveness: penetration/no penetration, number of perpetrators: more than one/one, relationship with perpetrator: previously known/unknown), we performed chi-square tests of difference. To determine the differences of revictimization and its features on dimensional PO scores, we used the Mann–Whitney U test with revictimization and its features as independent variables and PO scores as dependent variables. The nonparametric test was used due to the nonnormal distributions of the PO dimensions.
To estimate the relationship of PO to revictimization and its features, independently of participants’ age, we performed binary logistic regressions with participants’ PO features and age as independent variables and revictimization and its features as dependent. Statistical significance was defined as p < .05.
All statistical analyses were performed using the statistical package SPSS 22.0.
Results
Among the 119 women included in the final study group, 98 (82.4%) reported an experience of revictimization. The mean ages were 31.2 years (SD = 8.71) for the revictimized women and 26.7 years (SD = 3.81) for the nonrevictimized. Other demographic characteristics of the study group, stratified by the experience of revictimization, are given in Table 3.
Demographic Data of Study Participants.

Level of PO and Experience of Revictimization
A significantly higher proportion of women classified as cBPO (96%) than those classified as NPO (79.2%) reported revictimization, odds ratio (OR) = 6.32, 95% confidence interval (CI) = [0.79, 50.54], p = .04, Fisher’s exact test. The result remained significant after controlling for participants’ age. Specifically, women with cBPO were 10.57 more likely to experience revictimization compared with women with NPO, 95% CI = [1.24, 90.28], p < .05 (Table 5).
With regard to the structural properties of personality, the results show that FF was significantly higher in revictimized than in nonrevictimized women, U = 692.50, z = −2.40, r = .22, p < .05 (Table 4). Again, the result was also significant after controlling for participants’ age, adjusted odds ratio (AOR) = 1.75 [1.18, 2.58], p < .01 (Table 5). In contrast, the differences in other structural properties between revictimized and nonrevictimized group were not significant (Tables 4 and 5).
Means, Standard Deviations, and Mann–Whitney U Test Statistics for Structural Features of Personality Regarding Revictimization.

Note. Experience (1—revictimization, 0—no revictimization), Frequency (1—more than one incident, 0—one incident), Intrusiveness (1—penetration, 0—without penetration), Number of perpetrators (1—more than one, 0—one), and Relationship with perpetrator (1—previously known offender, 0—unknown offender). ID = Identity Diffusion; PDM = Primitive Defense Mechanism; FF = Fear of Fusion; IRT = Impaired Reality Testing.
p < .05. **p < .01.
Standardized Regression Estimates of Revictimization Variables by Structural Features of Personality and Age.

Note. AOR = adjusted odds ratio (age adjustment); CI = confidence interval; PO = personality organization; R2 = pseudo R2 (Nagelkerke); ID = Identity Diffusion; PDM = Primitive Defense Mechanism; FF = Fear of Fusion; IRT = Impaired Reality Testing.
p < .05. **p < .01. ***p < .001.
Level of PO and Characteristics of Revictimization
Among those participants who reported revictimization, 74 (91.4%) experienced it more than once, 64 (79%) from more than one offender, 40 (49.4%) from the offender they previously knew, and 24 (29.6%) described it as involving penetration. Taking into account the small number of individuals who reported the experience of one revictimization incident (eight women), the analyses related to the frequency of ASA were omitted, as the results would not be accurate.
In the group with cBPO, revictimization was experienced significantly more often from the previously known offender, χ2(1) = 4.08, p = .04, and more likely involved penetration than in the group with NPO, χ2(1) = 5.64, p = .02. The results remained significant after controlling for participants’ age (for relationship with perpetrator, AOR = 2.85 [1.03, 7.89], p < .05, and for intrusiveness, AOR = 5.16 [1.66, 16.08], p < .01; see Table 5); however, in case of the relationship with perpetrator, the overall model for PO was insignificant which can indicate that the influence of the PO on this aspect of revictimization is minor. There was no significant difference in terms of number of offenders between the cBPO and NPO groups, χ2(1) = 0.84, p = .36 (see also Table 5).
With regard to the structural properties of personality, ID, PDM, and FF were significantly higher in women who were revictimized with penetration than those whose experience did not involve penetration, U = 716.00, z = −2.14, r = .22, p < .05; U = 693.50, z = −2.31, r = .23, p < .05; U = 618.00, z = −2.90, r = .29, p < .01, respectively (Table 4). The difference in IRT was not significant (Table 4). After controlling for participants’ age, the results for ID, PDM, and FF remained significant; however, the results for IRT turned out to be of significance as well (for ID, AOR = 1.49 [1.10, 2.00], p < .01; for PDM, AOR = 1.42 [1.08, 1.85], p < .05; for FF, AOR = 1.73 [1.26, 2.36], p < .01; and for IRT, AOR = 2.08 [1.06, 4.06], p < .05; see Table 5). In turn, only PDM and IRT were significantly higher in women who were revictimized by the previously known offender, in comparison with those revictimized by the unknown offender, U = 840.00, z = −2.60, r = .26, p < .01; U = 996.00, z = −2.42, r = .24, p < .05, respectively (Table 4). After controlling for participants’ age, the results remained significant (for PDM, AOR = 1.32 [1.03, 1.68], p < .05; for IRT, AOR = 3.57 [1.19, 10.77], p < .05; see Table 5). However, after controlling for the participants’ age, the overall model for PDM turned insignificant which—again—can indicate that the influence of PDM on this aspect of revictimization is minor. The differences in ID and FF were not significant (Tables 4 and 5). In terms of the number of offenders, there were no significant differences between the groups (Tables 4 and 5).
Discussion
We found that more revictimized women are characterized by cBPO than by NPO and that the structural feature particularly differentiating the revictimized women from the nonrevictimized is FF. This result is both in line with the findings of previous empirical studies that showed higher levels of violence experienced by individuals with BPO (e.g., Critchfield, Levy, Clarkin, & Kernberg, 2008; Sansone et al., 2011; Sansone & Sansone, 2011) and fits well with Kernberg’s conceptual framework (Clarkin, Yeomans, & Kernberg, 2006; Kernberg, 1976, 2004). Specifically, the characteristics of functioning of individuals with BPO—with special emphasis on the relevance of FF—may lay the ground for the vulnerability to revictimization.
FF occurs in BPO as projected, and thus expected, hostility and aggression are reacted to in an acquiescent way. Hence, the fear of loss of separate identity is triggered as relationships feel powerfully defining of the person with BPO. This state is then managed through different strategies that, along with the consequences of their introduction, might increase the risk of sexual victimization.
First, FF is dealt with by avoidance of closeness in relationships. As demonstrated by the study of Critchfield et al. (2008), the increased levels of anxiety and the tendency to avoid closeness in relationships in Borderline Personality Disorder (BPD) were in fact positively associated with an expectation of hostility and aggression from others. As a consequence, individuals with BPO might be inclined to be involved only in superficial relationships that are rather based on the exchange of interests than trust and a solid sense of togetherness (see Kernberg, 1995). The perception of relationships in terms of exchange, in turn, may favor mutual exploitation, including exploitation of sexuality. Moreover, the tendency to expect aggression from others may not necessarily contribute to greater security. Indeed, studies show that functioning based on a lack of trust, linked with a tendency to control others and continuously increased vigilance, does not constitute an adaptive strategy to protect against harm (Marx, Heidt, & Gold, 2005). The characteristic compulsion and stiffness resulting from such attitudes hamper the adequate assessment of real threats and the ability to respond to them. For instance, Schry and White (2016) described the association between anxiety in social relations and increased vulnerability to sexual victimization due to increased passivity during sexual situations.
Second, increased FF and the related difficulty in establishing close relationships limit the circle of people available to provide support in difficult life situations. Meanwhile, as has been indicated in previous studies (e.g., Collins, 1998), satisfaction with interpersonal relationships and the presence of supportive friends and family are important protective factors that reduce the risk of victimization.
Third, the difficulty sustaining engagement can result in frequent changes of partners and an orientation toward short-term mating. Such functioning may lead to sexual needs being fulfilled in relationships where sex is not associated with closeness and tenderness, and to exposure to random people—including to those mainly interested in obtaining their own satisfaction and inclined to pursue sexual coercion (Himelein, 1995; Koss & Dinero, 1989; Mayall & Gold, 1995; Merrill et al., 1999).
Interestingly, in our study, the experience of revictimization was not linked with the ID, PDM, or IRT dimensions. However, this result is not consistent with the expectations based on literature. It seems that it should not be explained only in relation to the limitations of the study, such as the overall low level of borderline features in the study population. This level was in fact sufficiently high that a significant relationship could be demonstrated with FF, whereas for the other structural properties, the results did not even approach the trend level. It thus seems justified to conclude that FF may be a key aspect of personality structure related to revictimization. It is possible that the experience of revictimization as an interpersonal phenomenon is primarily associated with this feature of personality, which most directly refers to the sphere of intimate relations.
Analysis of the higher rate of revictimization found in individuals with cBPO should, however, take into account yet another potential substrate of this result. As indicated by Kernberg (1975, 1983), BPO can contribute to more distorted memories of past experiences, which—due to the use of the mechanism of projection of aggressive impulses onto others—are particularly hostile. Thus, higher rates of revictimization in individuals with cBPO may not necessarily reflect the actual frequent experience of violence, but the impact of distortions of memory and the difficulty of differentiating fantasy from reality. The effect of this mechanism on the results cannot be totally eliminated, but it seems that it is not dominant with respect to the study population. Kernberg’s (1983) observations concern, first and foremost, individuals with severely disturbed personality. Our study participants, however, were characterized by a relatively low level of intensity of BPO features. In particular, there was no relationship between revictimization and IRT—the structural feature, which directly refers to difficulties in distinguishing intrapsychic from external phenomena.
As for the relationship of PO with the characteristics of revictimization, significant links were found only in the case of invasiveness and the proximity of relationship with the revictimizing offender: More individuals who experienced revictimization involving penetration, as well as those revictimized by the previously known offender, were found in the group with cBPO than in the group with NPO. As the proximity of the relationship with the offender and the invasiveness of the sexual activity result in more severe consequences for the victim (e.g., Campbell et al., 1999; Koss & Dinero, 1989), it can be concluded that people with a more disordered structure are at the same time subject to stronger, further disturbing experiences of abuse.
Interestingly, for both invasiveness and proximity of relationship to the offender, the strongest association was revealed for IRT dimension (after controlling for age). In the case of BPO, IRT is usually limited to the sphere of social relations, in particular to close relationships which activate anxiety and intrapsychic conflicts leading to more disturbed functioning. Deficits in reality testing in this group often manifest as an impairment in the adequate interpretation of signals in the context of interpersonal exchanges, wishful thinking, perception of others through the prism of own’s needs, and—under the influence of particularly strong affect—transient episodes of decompensation (Gamache et al., 2009; Kernberg, 1984, 2004), in which the ability to adequately assess the situation is even more distorted. These characteristics distinguish BPO from NPO, in which the domination of repression over the splitting mechanism allows for a more rational, less based on a distorted assessment of reality, functioning in close relationships. These differences, in turn, may explain why revictimization in closer relations is more frequent for individuals with cBPO where, at the same time, more invasive forms of violence often occur. It thus seems understandable that IRT is more associated with the proximity of relationship to the offender and invasiveness of revictimization than with the actual occurrence of the revictimization, for which, in turn, FF was more crucial.
In explaining the lack of association between PO and the number of offenders of revictimization, the effect of dichotomization of variables describing the characteristics of revictimization must be considered. It is possible that incorporating this as continuous variable—thus increasing the variance—would allow a relationship to be revealed. On the contrary, the lack of relationship between the PO and the number of offenders of revictimization may suggest that the relationship of the personality structure with the characteristics of revictimization relates primarily to its qualitative features (specifically, the proximity of the relationship with the offender and invasiveness) rather than to its quantitative features.
In summary, it seems justified to extract two areas of the relationship of PO with revictimization. The first concerns the occurrence of revictimization itself. In this case, the key personality dimension turned out to be FF, which attains higher intensity in individuals with BPO, who therefore become revictimized more often. The second area concerns the characteristics of revictimization, in particular its qualitative features. In this case, the key personality dimension turned out to be IRT, which also attains higher intensity in individuals with BPO, who therefore become revictimized in a more invasive form and more often by the previously known offender.
As this study was based on retrospective accounts, no clear causal conclusions with regard to the link between PO and revictimization can be made. Indeed, the literature suggests that the association might be bidirectional. For example, Schilling (2011), who examined female victims of domestic abuse, found a positive relationship between abuse duration and severity and BPO scores. However, in accordance with Kernberg’s theory, BPO is rooted in disturbances in the early stages of development where the mechanism of splitting organizes the psychological functioning. In our view, although this early determination is essential to the constitution of BPO, some later experiences can also influence the personality structure by either increasing its maturity (e.g., psychotherapy) or deepening its disturbance. Hence, it might be considered that personality structure determines the experience of revictimization, which then—as a vital interpersonal experience—influences the structure, strengthening the organization, which promotes such experiences again. Intrapsychic structures and interpersonal experiences in relation with the environment thus constitute a dynamic self-reconstructing system that determines the specific course of life of an individual (Mischel & Shoda, 1995, 1999). In the case of CSAS with BPO, the high probability of subsequently experiencing sexual violence is likely to be an element of their life course. In the case of CSAS with NPO, such experience is less likely; however, if it does occur, it will probably be less invasive and by someone they have not been in any relation with.
Limitations
There are a number of weaknesses in this study that should be mentioned.
First, the statistical power of conducted analyses was limited due to the relatively small sample size. Specifically, only 21 individuals reported that they had not experienced revictimization, and only eight individuals reported the experience of one revictimization incident (as opposed to more than one). These numbers are interesting in that they indicate how few CSA survivors have not experienced revictimization, or have only experienced one incident of revictimization; they were, however, problematic across the analyses. As a result, the analyses related to the frequency of ASA was omitted, whereas some of the calculated statistics might have showed weaker associations or even turned out to be not significant, while larger effects or even additional associations may be detectable with larger samples.
Second, the limited representativeness of the study group, specifically its relatively good level of adaptation, should be noted. The study population was characterized by a relatively low intensity of the structural characteristics of BPO, no history of psychiatric treatment longer than half a year, prevailing higher level of education, as well as the ability to regulate emotion that allowed for participation in the survey involving a direct contact with a researcher. Replying to questions about sexuality, and especially sexual violence, may in fact activate strong emotions, including embarrassment and anxiety. The study was conducted only on those who—despite the probable activation of these states—expressed their wish to participate in it. As the relevant stage of assessment consisted of a direct meeting with researchers, it can be assumed that the people who decided to take part in it belonged to the group of those who were more effectively coping with emotional arousal. However, good psychological adjustment is not prevalent in CSAS (see Cutajar et al., 2010; Jonas et al., 2011). For this reason, the generalization of the study results is possible, but only when limited to those better adapted.
Another important limitation is the retrospective nature of the study, as well as the fact that it relied solely on self-report measures. These factors could primarily affect the values of the variables relating to CSA and ASA. In particular, it is possible that some participants—either due to obliviousness of their experience or an unwillingness to disclose it—falsely stated that they had not experienced CSA or ASA. Such respondents would have consequently been assigned to the incorrect group. Second, among those who remembered the experience of violence, and decided to disclose it, the possibility of distorted memories should also be considered.
Further Research and Practical Implications
Regardless of the limitations, we believe that our study can contribute to broadening our knowledge of both sexual violence and PO, and also lay the ground for further investigations into the determinants of sexual revictimization.
First of all, our study showed that although individuals with NPO experience revictimization less often than do those with BPO, there was also a group of subjects with NPO and ASA experience. Hence, it would be valuable to determine whether NPO and BPO could be associated with different risk factors for revictimization. This dissimilarity might further result in different characteristics of the ASA experience. We believe that our study provides the basis for assuming the existence of such different patterns of revictimization.
Second, the current study was carried out in a group of adult women and focused only on revictimization experiences of adulthood. However, it can be expected that in the case of many individuals, subsequent incidents of sexual abuse also took place in the later stages of childhood and in adolescence (Boney-McCoy & Finkelhor, 1996). Thus, it would be worthwhile to examine revictimization not only in the context of the already formed personality structure but also in the context of the ongoing process of its development, taking into account its specificities in different stages of development.
It would also be undoubtedly valuable to carry out an analogous project in a group of men. Such a study will certainly be much more challenging and time-consuming, as—according to the literature—more girls than boys experience CSA (Kloppen, Haugland, Svedin, Mæhle, & Breivik, 2016; Sajkowska, 2017), and there is also a stronger resistance to disclosing such experience among men (Widom, 1997). Nevertheless, the results of the few studies of revictimization which included men indicate the significant scale of this phenomenon, which justifies giving it more attention (Sorenson, Siegel, Golding, & Stein, 1991; Stevenson & Gajarsky, 1991).
The findings of this study should not be interpreted as blaming the victims for sexual violence perpetrated against them. The offenders bear complete responsibility for sexual assault. Nonetheless, the results may have potential practical implications in helping women decrease their vulnerability. The results of the study can be useful for psychological practice, in particular for the counseling and psychotherapy of women who report CSA.
First of all, a thorough assessment of the PO of the patient should allow for the estimation of the risk of reexperiencing sexual violence, as well as its possible nature, that is, its invasiveness and the likelihood that it may arise in the context of their current relations. When dealing with individuals diagnosed with BPO, the counselor or a therapist should be particularly alert for the occurrence of such experiences and therefore focus not only on the internal world of the patient but also on their external reality. In situations of particularly high risk or occurrence of subsequent violence, the temporary abandonment of the position of therapeutic neutrality should be seriously considered along with replacing it with direct interventions aimed at the patient’s decisions or actions (e.g., Chu, 1992). Even though such interventions entail considerable effort in restoring the position of neutrality afterward, failure to present such an active attitude may limit the efficiency of the therapy. Subsequent experiences of violence actively strengthen the disturbed personality structure and, as such, constitute force opposing the influence of the therapy.
Second, linking the occurrence and characteristics of revictimization with personality creates a background for shifting the proposals of psychotherapy from those focused on trauma to those focused on the structure of personality. In other words, single therapy programs developed for CSAS (e.g., Draucker & Martsolf, 2006) may be less effective in terms of reducing the risk of revictimization than programs that are diversified and adapted with regard to the patient’s PO.
In the case of BPO, the transference-focused psychotherapy (TFP) model (Yeomans et al., 2015), which is designed specifically for this group of patients, seems to be worth considering. In TFP, the main emphasis is initially focused on the patient’s current experience and reactions. Past traumas are discussed only in the later stages of treatment, when the risk of decompensation and of the dangerous acting out of tensions triggered by the issues is lower (Levy et al., 2006). In our view, the utility of this therapy specifically with regard to minimizing the risk of revictimization of CSA survivors may be related to two factors. First, TFP allows the external reality of the patient to be dealt with, providing the possibility of temporarily abandoning the position of neutrality and providing a description of restoring it (Yeomans et al., 2015). It thus allows the therapist to intervene in the situation of real danger of further violence. Second, studies of the efficiency of TFP indicate that it can result in changes in the factors that, according to our study, are related to the occurrence of revictimization. Although lasting changes in individuals’ PO are possible within the framework of many years of therapy, Levy et al. (2006) found that 12 months of TFP for patients with borderline personality disorder can lead to significant increase in rates of secure attachment. Considering the role of FF as a factor associated with the experience of revictimization, we assume that these results support the idea of applying TFP in addressing the problem of further victimization in patients with BPO.
In contrast, for patients with NPO, the focus on CSA and its impact on current functioning—including the context of possible revictimization—may occur relatively early in therapy. In this group, the affective response, which may be activated by discussing traumatic experience, should not imply a risk of decompensation or dangerous acting out behaviors.
Footnotes
Acknowledgements
The authors thank the research assistants who helped to collect the data for the study. They also express their gratitude to all the women who decided to take part in the study and share their difficult experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Polish National Science Centre (NCN; Grant Number DEC 3535/B/H03/2011/40).