
Abstract
Sexual abuse prior to age 18 may put some women at risk for engaging in sexual risk taking. This association could exist, in part, as a result of the impact of posttraumatic stress symptoms on behavioral regulation. The current study utilized a path analysis to investigate the association between severity of sexual abuse before age 18, posttraumatic stress symptoms, poor behavioral regulation, and expected engagement in sexual risk taking among college women. The sample consisted of 88 college women with experiences of sexual abuse prior to the age of 18. Severity of sexual abuse predicted posttraumatic stress symptoms. In addition, posttraumatic stress symptoms predicted poor behavioral regulation, which in turn predicted expected engagement in sexual risk taking. These findings indicate functional mechanisms involved in sexual decision making of women who have had past sexual abuse and experience posttraumatic stress symptoms.
Sexual risk behaviors (SRBs) include sexual activity with multiple sexual partners, without the use of condoms or other contraceptives, and while under the influence of drugs or alcohol (Centers for Disease Control and Prevention [CDC], 2015). An important public health priority is the reduction of emerging adults’ SRBs because it leads to transmitting and contracting sexually transmitted infection (STIs; CDC, 2015). The goal of the current study was to examine severity of sexual abuse (SA) prior to age 18, posttraumatic stress symptoms (PTSS), and poor behavioral regulation as predictors of expected engagement in SRBs among emerging adult college women.
It is estimated that 16% of female college students experience attempted or completed SA before beginning college (Krebs, Lindquist, Warner, Fisher, & Martin, 2009). SA is associated with various psychological symptoms among adult college women including PTSS, anxiety, depression, and alcohol misuse (Peter-Hagene & Ullman, 2015; Tang & Freyd, 2012; Ullman, 2016). Certain characteristics of SA prior to age 14 were associated with greater symptom severity including greater degree of violence used by the perpetrator (Peter-Hagene & Ullman, 2015) and greater number of assaults (Ullman, 2016). In addition, SA prior to age 18 that involved closer relationship to the perpetrator was associated with greater PTSS (Tang & Freyd, 2012). Furthermore, severity of SA prior to age 14 based on such characteristics predicted SRBs with a regular dating partner and greater number of lifetime sexual partners among college women (Messman-Moore, Walsh, & DiLillo, 2010). In addition, overall PTSS (Munroe, Kibler, Ma, Dollar, & Coleman, 2010) and trauma-related intrusions (Walsh, Latzman, & Latzman, 2014) predicted greater SRBs among college students. Although SA and PTSS have been associated with SRBs, more research is needed to identify underlying mechanisms that can be targeted in prevention programs for college women with histories of SA prior to age 18.
Behavioral regulation is an important construct to consider in the context of SA occurring prior to adulthood because dimensions of temperament that form behavioral regulation develop early in life (Wills & Ainette, 2009) and behavior regulation is related to posttraumatic psychopathology (Nigg, 2017). Behavior regulation is theorized to be a dual-process construct, with an automatic/unintentional system and a separate controlled/effortful system that have unique pathways to health outcomes (Nigg, 2017; Wills, Pokhrel, Morehouse, & Fenster, 2011). In a prevailing model of behavior regulation, the automatic/unintentional system is termed poor behavioral regulation, which consists of tendencies to consider immediate rewards with less focus on future consequence of behavior, act quickly without restraint, and struggle with adapting behavior to the demands of situations (Wills et al., 2011). Poor behavioral regulation (i.e., impulsive system; disinhibition) is associated with functioning in reward-oriented brain regions (Bickel et al., 2007; Nigg, 2017). People with histories of SA may engage in risk behaviors because PTSS tax mental processes involved in constraining behavior and exacerbate individual differences in poor behavioral regulation (Miller et al., 2006). PTSS severity is associated with self-reported behavioral regulation difficulties (Contractor, Armour, Forbes, & Elhai, 2016) and behavior regulation difficulties predicted SRBs in college samples (Hahn, Simons, & Simons, 2016; Quinn & Fromme, 2010). Thus, there is a theoretical rationale that poor behavioral regulation may lead to SRBs among women with SA histories because PTSS impact ability to disengage from the immediate cues and consider distal consequences of behavior.
Previous research on trauma exposure and risk behaviors has primarily focused on emotion regulation and negative urgency (i.e., the tendency to act rashly when experiencing negative affect), with emphasis on theory that exposure to traumatic events leads to risk-taking due to difficulties with regulating behavior when distressed (Hahn et al., 2016; Messman-Moore et al., 2010; Weiss, Tull, & Gratz, 2014). Poor behavioral regulation is correlated with emotion regulation difficulties (Wills et al., 2011), but is not specific to regulating behavior in the context of processing and responding to emotional stimuli (Nigg, 2017). Moreover, there is preliminary evidence that poor behavioral regulation has a stronger association with health behaviors such as substance use compared with emotion regulation (Wills et al., 2011). Therefore, poor behavioral regulation may be a distinct pathway to SRBs among people with histories of SA that is not exclusive to situations that require regulating distress.
In summary, SA, PTSS, and poor behavioral regulation have been independently associated with SRBs (Messman-Moore et al., 2010; Munroe et al., 2010; Quinn & Fromme, 2010; Walsh et al., 2014). In addition, PTSS tend to be more severe among people with behavioral regulation difficulties (Contractor et al., 2016). However, poor behavioral regulation has been under-investigated as a potential mechanism underlying the association between SA severity, PTSS, and SRBs. To understand the impact of stress and regulation on women’s expectations of their own SRBs, severity of SA, PTSS, and poor behavioral regulation were examined as predictors of expected engagement in SRBs in a sample of college women with SA prior to age 18. It was hypothesized that severity of SA would predict expected engagement in SRBs via two paths. PTSS and poor behavioral regulation were hypothesized to mediate the relationship between severity of SA and expected engagement in SRBs.
Method
Participants and Procedure
The current investigation included 88 participants who endorsed a history of SA prior to age 18. Participants were part of a larger study of 450 female college students from a Midwestern University who completed an online survey on sexual aggression for extra credit in courses (Tirabassi, Caraway, & Simons, 2017). Participants were primarily White (White, 92.1%; Native American, 4.6%; Other, 3.4%) and 18 to 26 years old (M = 19.45, SD = 1.65). The Institutional Review Board (IRB) at the data collection site approved the current study.
Measures
The Computer Assisted Maltreatment Inventory (CAMI; DiLillo et al., 2010) measured severity of SA and used behaviorally specific items to assess for history of SA prior to age 18. Participants were determined to have a history of SA if they endorsed exposure to someone’s genitals or someone masturbating in front of them, fondling, and experiencing attempted or completed oral, anal, or vaginal intercourse before age 18 that occurred against their will or when they did not want it to happen, perpetrated by a family member, or was perpetrated by someone five or more years older. Participants who endorsed SA completed follow-up items that measured six indicators of severity. Each indicator was assigned a severity weight ranging from 0 to 3. Indicators included Relationship to the Perpetrator (1 = nonfamily, 2 = family/nonparent, 3 = parent), Frequency (1 = 1-2 times, 2 = 3-10 times, 3 = more than 10 times), Nature of Abuse (1 = noncontact or exposure to someone’s genitals/masturbation, 2 = contact without penetration or fondling, 3 = penetration or oral, anal, or vaginal rape), Duration (1 = less than 1 year, 2 = 1-2 years, 3 = 2 years), Force/Manipulation (0 = none, 1 = verbal tactics, 2 = threats of physical harm, 3 = physically held down), and Number of Perpetrators (1 = 1, 2 = 2, 3 = more than 2). Summing the scores on the indicators created total scores, ranging from 5 to 18, with higher scores indicating more severe SA. Participants who had more than one experience of SA were asked to rate the indicators for up to three assault experiences and the highest rating was used for each indicator.
The Posttraumatic Stress Disorder Checklist–Civilian Version (PCL-C; Weathers, Litz, Huska, & Keane, 1994) assessed reexperiencing, avoidance, and hyperarousal symptoms to stressful life experiences using criteria from the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994). The 17 items in the scale were summed to create total scores and demonstrated excellent internal consistency in previous research (Adkins, Weathers, McDevitt-Murphy, & Daniels, 2008; Weathers et al., 1994). A cutoff score of 45 or greater indicated possible PTSD (posttraumatic stress disorder; Adkins et al., 2008). As the study was completed, a newer version of the PCL was created based on Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). Therefore, the current measure does not include more recent diagnostic criteria including items assessing for changes in cognitions.
Poor behavioral regulation was assessed with 37 items adapted by Wills et al. (2011) from several preexisting measures that were reported in previous research to form a reliable latent structure with acceptable internal consistency. The measure of poor behavioral regulation consisted of six subscales: Impatience, Distractibility, Impulsiveness, Poor Delay of Gratification, Present Time Perspective, and Self-Criticism items. The respondents rated the items on a 5-point Likert-type scale ranging from 1 (not at all true) to 5 (very true). Per recommended scoring procedures, standardized scores for each subscale were averaged to create the score for poor behavioral regulation.
The Cognitive Appraisals of Risky Events–Revised (CARE-R; Katz, Fromme, & D’Amico, 2000) measured participants’ intention to engage in SRBs over the next 6 months and has been reported to demonstrate acceptable internal consistency. Participants were asked to rate the 11 items (e.g., “Sex without a condom with someone I just met or do not know well.”) on a 7-point Likert-type scale ranging from not at likely (0) to very likely (6). Higher scores indicate greater expected involvement in SRBs.
Statistical Analyses
Descriptive statistics were conducted in STATA 15 (StataCorp, 2017). The path analysis was conducted using full information maximum likelihood in Mplus 7.3 (Muthén & Muthén, 2013). Indirect effects were calculated for this path analysis using bias-corrected bootstrap confidence intervals (CI), which are a sensitive test to detecting indirect effects and increase the likelihood that the population value of the indirect effect is contained within the interval (MacKinnon, 2008). Significant CIs are those that do not contain zero. The model for the current study included 10 free parameters. It is recommended that the target ratio of participants per free parameter should be 5:1 (Bentler & Chou, 1987; Kenny, 2015). The current model was estimated using 88 participants (i.e., participant to parameter ratio of 8.8:1) and should provide adequate power for the path analysis.
Results
Common characteristics of SA were penetration by a nonfamily perpetrator (76.1%). In all, 61.4% of participants reported their first SA was perpetrated by a male friend or acquaintance. The most severe methods used by perpetrators included physical force or drugs/alcohol (48.9%), threats of harm (5.7%), and verbal tactics (19.3%). The majority of the sample reported SA perpetrated by one perpetrator (61.4%), followed by three (25.0%) and two perpetrators (13.6%). Participants reported SA occurred 1 to 2 times (23.9%), 3 to 10 times (22.7%), or more than 10 times (53.4%). Participants most commonly reported that SA occurred for a period of time that was less than 1 year (39.8%), followed by occurring during a 1- to 2-year period (34.0%), and during 2 or more years (27.3%). The age of onset for first (M = 13.42; SD = 3.90), second (M = 13.47; SD = 4.26), and third (M = 14.91; SD = 2.91) SA ranged from 4 to 17 years. Among the 88 participants, 28 reported (32.9%) a SA experience before age 14 and 30% of the sample had possible PTSD. Internal consistencies for measures ranged from acceptable to excellent, and SRBs were significantly associated with PTSS and poor behavioral regulation (see Table 1).
Descriptive Statistics and Correlation Matrix (N = 88).

Note. CSA = child sexual abuse; PTSS = posttraumatic stress symptoms; SRB = sexual risk behaviors.
p < .01. ***p < .001.
For the path analysis, direct paths were specified from SA severity to PTSS, and PTSS to both poor behavioral regulation and expected engagement in SRBs. Finally, a direct path was specified from poor behavioral regulation to expected engagement in SRBs. The overall model showed a good fit: X2(2, N = 88) = 1.15, p = .563; root mean square error of approximation (RMSEA) = .000; comparative fit index (CFI) = 1.000; standardized root mean square residual (SRMR) = .028 (see Figure 1). As hypothesized, SA severity had a significant direct effect on PTSS. PTSS symptoms had a significant direct effect on poor behavioral regulation. The path from PTSS to expected engagement in SRBs was fully mediated via poor behavioral regulation. There was a significant indirect effect of SA on expected engagement in SRBs, 95% CI = [.209, .873]. There were two significant indirect paths from SA to expected engagement in SRBs. The first was through PTSS (95% CI = [.018, .691]). The second significant path was via PTSS and poor behavioral regulation (95% CI = [.026, .513]). A significant indirect effect of PTSS on expected engagement in SRBs was also detected via poor behavioral regulation (95% CI = [.006, .185]).
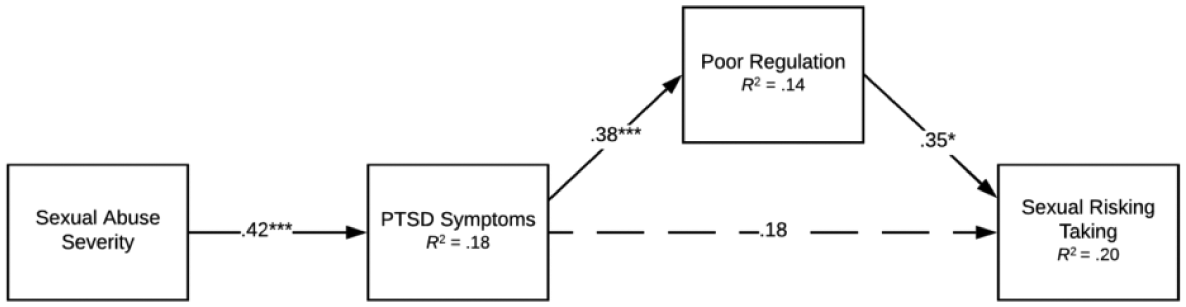
Path model (N = 88).
Discussion
In the current study, poor behavioral regulation mediated the association between PTSS and expected engagement in SRBs among a sample of women with histories of SA prior to age 18. Results suggest that women with SA histories prior to age 18 may engage in SRBs with nonregular partners due to the impact of PTSS on poor behavioral regulation. Results are novel because poor behavioral regulation is distinct from other forms of regulation that have been more frequently researched in samples of women with SA histories including emotion regulation difficulties and impulsivity based on Whiteside and Lynam’s (2001) five factor model (Weiss et al., 2014). Poor behavioral regulation is different than emotion regulation difficulties because it does not limit ability to engage in goal-directed behaviors to situations when feeling distressed. In addition, poor behavioral regulation is distinct from the five-factor model of impulsivity because (a) the positive and negative urgency facets of impulsivity are more closely related to forms of emotion regulation than poor behavioral regulation and (b) the lack of premeditation, lack of perseverance, and sensation-seeking factors are based on low scores on planfulness and persistence indices of impulsivity, which are different pathways to risk-taking than the tendencies involved in poor behavioral regulation (Wills et al., 2011). In fact, research supports that good behavioral regulation (i.e., constraint), which is theorized to be an effortful system that involves conscious processing of information and is measured with high scores on planfulness and persistence, forms a two-factor structure with poor behavioral regulation (Wills et al., 2011). Therefore, the current study broadens the focus of the association between PTSS and SRBs to novel tendencies of poor behavior regulation (e.g., distractibility, impatience, present focus). To further clarify mechanisms that contribute to SRBs, researchers should examine whether poor behavioral regulation predicts additional emotion and behavioral regulation constructs, such as negative urgency, which may subsequently lead to SRBs.
Although a significant bivariate association is not a prerequisite for a meaningful indirect effect (MacKinnon, Fairchild, & Fritz, 2007), it was unexpected that SA severity was not associated with expected engagement in SRBs because SA has been associated with SRBs by previous researchers (Walsh et al., 2014; Weiss et al., 2014). However, other researchers have reported results consistent with the current study. For example, Messman-Moore and colleagues (2010) reported that severity of SA prior to age 14 was associated with SRBs for known partners, but not strangers, and that SA was indirectly associated with SRBs with strangers via emotion regulation. Therefore, the association between SA and SRBs likely depend on the specific contexts in which SRBs occur, including age of onset. This is particularly important to consider in the current study because approximately two thirds of participants reported that SA occurred between ages 14 and 17. Furthermore, certain indicators of SA such as relationship to the perpetrator may be better predictors of SRBs than the overall construct of SA severity. More research is needed to understand the characteristics of SA that lead to specific types of SRBs.
Results should be interpreted within the contexts of limitations. The outcome measure assessed expected engagement in SRBs; therefore, results cannot be translated to actual risk-taking behavior; however, results provide insight into women’s intended engagement in high-risk behaviors. The sample was primarily White and identified as heterosexual. It is imperative that researchers examine these relationships with more diverse samples. Finally, PTSS were assessed for stressful life experiences rather than specifically anchored to SA, and experiences of SA after age 18 and other traumatic life events were not accounted for in the model. As there was not a comparison group of people who had PTSS from non-SA events, it is possible that results are not specific to people who have experienced SA and may (or may not) translate to PTSS stemming from other types of potentially traumatic events.
In conclusion, results support targeting poor behavioral regulation in prevention of SRBs among college students with histories of SA prior to age 18 and PTSS. It is imperative to recognize that the majority of women reported peers perpetrated sexual assault. Therefore, the most effective prevention for SRBs among women exposed to SA is to reduce risk for peer perpetration.
Footnotes
Authors’ Note
Austin M. Hahn is now affiliated with Medical University of South Carolina, Charleston, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health under Grant T32MH018869, National Institue of Drug Abuse under Grant 5T32DA007288-27, and National Institue of Alcohol Abuse and Alcoholism under Grant F31AA027143.