
Abstract
Prescription drug misuse is increasingly common in the United States. To date, little is known about how prescription drug misuse relates to negative parenting behaviors like child maltreatment, even though use of illicit drugs increases rates of both child neglect and physical abuse. This study used secondary data from the Fragile Families and Child Well-Being Study (FFCWS), a clustered national sample of families at high risk for both prescription drug misuse and child maltreatment (n = 2,917). Data from mothers who participated in the 9-year follow-up of this study were used to create logistic regression models examining prescription drug misuse and physically aggressive and neglectful parenting, while controlling for demographic and psychosocial variables. Black, non-Hispanic mothers and mothers in worse health had higher odds of physically aggressive parenting. Mothers in worse health and those who used other illicit drugs had greater odds of neglectful parenting. There were no relationships between prescription drug misuse and either parenting outcome. The findings do not provide evidence that prescription drug misuse is a risk factor for child maltreatment. Further research examining this issue and potential progression from prescription drug misuse to other illicit drug use could help clarify whether this behavior is related to negative outcomes for children.
Prescription drug misuse (i.e., use of a prescription drug without or outside of a doctor’s prescription) has reached significant levels in the United States. Between 2004 and 2010, emergency room visits related to prescription drug misuse increased by 119% (Substance Abuse and Mental Health Services Administration [SAMHSA], 2012). Use of opioids, the most commonly misused class of prescription drugs, cost society an estimated US$55.7 billion in 2007 due to lost earnings from premature death or unemployment, health care costs, and criminal incarceration (Birnbaum et al., 2011). Popular media reports suggest that parents are increasingly misusing their own children’s medications (Samakow, 2012) or dying of prescription drug overdoses (Smith & Kounang, 2013). The stakes of prescription drug misuse are higher for primary caregivers of young children than for other populations, as they are responsible for ensuring the safety and healthy development of their children. It is currently unknown, however, whether prescription drug misusers are more likely to abuse or neglect their children.
On its own, child maltreatment remains a substantial problem in the United States, with approximately 686,000 children victims of maltreatment each year (U.S. Department of Health & Human Services [US DHHS], 2012). Child maltreatment has long-lasting and significant consequences for children and the greater society. Neglectful and abusive parenting has been linked to depression, anxiety, low social support, suicide, and cardiovascular disease in later life (Berglund, Balldin, Berggren, Gerdner, & Fahlke, 2013; Fuller-Thomson, Brennenstuhl, & Frank, 2011; Marshall, Galea, Wood, & Kerr, 2013; McCauley et al., 1997; Norman et al., 2012; Sperry & Widom, 2013). As a result, each year of confirmed cases of maltreatment results in approximately US$124 billion of costs to society (Fang, Brown, Florence, & Mercy, 2012).
Although the relationship between prescription drug misuse and child maltreatment is unknown, parental illicit drug abuse has been linked to abusive and neglectful parenting (Ammerman, Kolko, Kirisci, Blackson, & Dawes, 1999; Ekeus, Christensson, & Hjern, 2004; Freisthler, Gruenewald, & Price Wolf, 2015; Manly, Oshri, Lynch, Herzog, & Wortel, 2013; Onigu-Otite & Belcher, 2012; Walsh, MacMillan, & Jamieson, 2003). In addition, children of illicit drug-using parents are more likely to be abused again, remain in the child welfare system longer, and have worse long-term outcomes (Dunn et al., 2002; Laslett, Room, Dietze, & Ferris, 2012).
A recent study suggests that child welfare workers are more likely to substantiate cases of physical abuse and neglect if prescription drug misuse is present (Freisthler, Kepple, Price Wolf, Curry, & Gregoire, 2017). Overall, however, very little research has examined how prescription drug misuse relates to child maltreatment. One recent study suggests that mothers who misuse opioid prescription drugs score in the clinical range on self-reported parenting measures (Slesnick, Feng, Brakenhoff, & Brigham, 2014), indicating that like illicit drugs, prescription drug misuse impairs parenting behaviors.
Prescription drug misuse requires time, financial resources, and a suitable space to use the drug, all of which can affect parenting. Although little is known about prescription drug misuse among parents, a qualitative study of heroin users suggests that drug-using parents find it difficult to balance child care needs with the time spent obtaining, using, and recovering from the effects of drugs (Hogan, 2003). Due to child care demands, most parents used drugs in their own home, and locked their bedroom doors or ordered children to leave the home so that the children would not witness their drug use. Children could consequently be left unsupervised due to prescription drug misuse, leaving them vulnerable to risks both inside and outside their home, such as burns or poisoning. Misuse of sedating drugs, which can cause drowsiness and lethargy (Manubay, Muchow, & Sullivan, 2011), could lead parents to sleep during daytime hours when their children are awake, leaving children inadequately supervised. Alternatively, feelings of wellness that are achieved when misusing these drugs might also calm parents and reduce risk of physical abuse. As a result, misuse of prescription drugs such as tranquilizers and opioid analgesics might be more related to child neglect than physical abuse. This study is unique in examining whether the relationship between misuse of sedating prescription drugs and child maltreatment differs by type of maltreatment. It is hypothesized that prescription drug misuse will result in higher odds of neglectful parenting, but not physical abuse. Establishing the magnitude of this relationship could identify important screening and intervention needs for vulnerable families.
Method
Data Overview
The data for this study were from the Fragile Families and Child Well-being Study (FFCWS). The FFCWS, which was designed to follow families at risk of poverty and other negative outcomes (Reichman, Teitler, Garfinkel, & McLanahan, 2001), is a longitudinal survey of 4,898 new parents and children recruited between 1998 and 2000. The data were sampled in three stages. First, stratified random sampling based on labor market conditions, child support, and welfare policies was used to sample 20 large (population over 200,000) U.S. cities. Second, hospitals within cities were sampled to be representative of hospital births within that city. Finally, stratified random sampling was used to select married and unmarried births within those hospitals. Unmarried women were oversampled, resulting in a sample that overrepresents low income and minority children and families with nonresidential fathers.
Although the FFCSW is a longitudinal study, the proposed exploratory study is cross-sectional. However, demographic characteristics assessed at other time points will be utilized. Approximately 4,688 families who completed the baseline survey were deemed eligible for the 9-year follow-up (excluding families lost to follow-up, where the child had died, or had been permanently adopted). Of those families, 72% completed the home visit component of the study (n = 3,391; Bendheim-Thoman Center for Research for on Child Wellbeing, 2001). As mothers were the default parent who was administered the child maltreatment questions, analyses were limited to mothers. Data were collected between August 2007 and April 2010, when the focal child was approximately 9 years old.
Measures
Child maltreatment
The proposed study focuses on two outcome variables: (a) child neglect was measured via five items assessing the frequency of which mothers (1) left their child home alone, (2) did not show appropriate affection to their child, (3) did not ensure their child received the food they needed, (4) did not take their child to the doctor’s office, or (5) were so drunk or high they were not able to care for their child. These items comprise the neglect index of the Conflict Tactics Scale, Parent–Child version (CTSPC; Straus, Hamby, Finkelhor, Moore, & Runyan, 1998). The CTSPC captures the frequency of several rare behaviors, with the occurrence of any of these behaviors indicating neglect. As a result, this measure is best viewed as an index of the frequency of neglectful behaviors than as a scale. For each question, respondents are asked to report the number of times in the last year that they have done the behavior, with response categories ranging from “never” to “more than 10 times.” To create a yearly prevalence score, neglect was coded as 0 = no incidence of any neglectful behaviors and 1 = any instance of neglectful behaviors in the past year (Straus et al., 1998). (b) Child physical abuse was measured by five items from the physical assault index of the CTSPC. Similar to the neglect questions, respondents selected how often they used physically abusive behaviors on the focal child of the study in the past year (ranging from “never” to “more than 10 times”), including: (1) slapping on the face, head, or ears; (2) hitting on the body with a hard object; (3) knocking the child down; (4) hitting or kicking; and (5) hitting on the bottom with a belt, hairbrush, or other hard object. As recommended for this subscale (Straus et al., 1998), a yearly prevalence dichotomous variable (0 = no use of physically abusive behaviors and 1 = any use of physically abusive behaviors in the past year) was created.
Prescription drug misuse
Parents were asked about their use of prescription drugs without a prescription, in larger amounts than prescribed, or for longer periods than prescribed in the past 12 months. Categories include sedatives (e.g., barbiturates, sleeping pills), tranquilizers (e.g., Valium, Xanax), analgesics or other prescription painkillers (e.g., Percodan, Codeine, OxyContin), and amphetamines or other stimulants (e.g., Ritaline, Dexedrine). Primary caregivers were divided into those who misused sedatives, tranquilizers, or analgesic prescription drugs in the past year coded as 1 and no misuse of sedating prescription drugs coded as 0. As use of prescription stimulants is low in this sample (less than 1%), we did not examine stimulant prescription drug misusers. As there were no prescription drug-specific frequency measures in the FFCWS, frequency of prescription drug misuse was not assessed.
Control variables
Demographic and psychosocial characteristics were included in the analyses as controls. Some of the demographic variables were measured at the time of the child’s birth and include mother age and race/ethnicity (White, Black, Hispanic, and Other). Education level (less than high school, high school, some college, college or higher), depression (adapted by the FFCWS from the Composite International Diagnostic Interview–Short Form (Kessler, Andrews, Mroczek, Ustan, & Wittchen, 1998), household income-to-needs ratio (Brooks-Gunn, Schneider, & Waldfogel, 2013), relationship status, current health status, tangible support, emotional support, past year binge drinking (i.e., four or more drinks in one drinking episode), and other illicit drug use (i.e., marijuana, heroin, cocaine) were measured at the 9-year follow-up.
Data Analyses
Respondents who had intact information for study variables were retained in the analytic sample (n = 2,917). To correctly calculate variance estimates, replicate weights (available in the Fragile Families data set) were used. These weights were created by the random groups approach (Wolter, 1985), making parameter estimates generalizable to the cities sampled by the study (Reichman et al., 2001). To account for the clustering of participants within hospitals and cities, all models allowed for between-city random effects and were conducted with the use of Stata 15. A multicollinearity analysis revealed no significant multicollinearity issues with the study variables. A series of logistic regression models with maximum pseudolikelihood estimation were created. These models assessed whether prescription drug misuse was related to (a) physical aggression and (b) child neglect.
Results
Demographic characteristics of the sample are displayed in Table 1. The majority of the sample was non-White (71%) and had some education beyond a high school diploma (59%). Approximately 4% of the sample had engaged in prescription drug abuse in the past year, while 58% had used physical aggression against their child, and 22% had at least one instance of neglectful parenting.
Weighted Frequencies or Means of Demographics Characteristics of Analytic Sample of Mothers From FFCWS 9-Year Follow-Up Interview (n = 2,917).
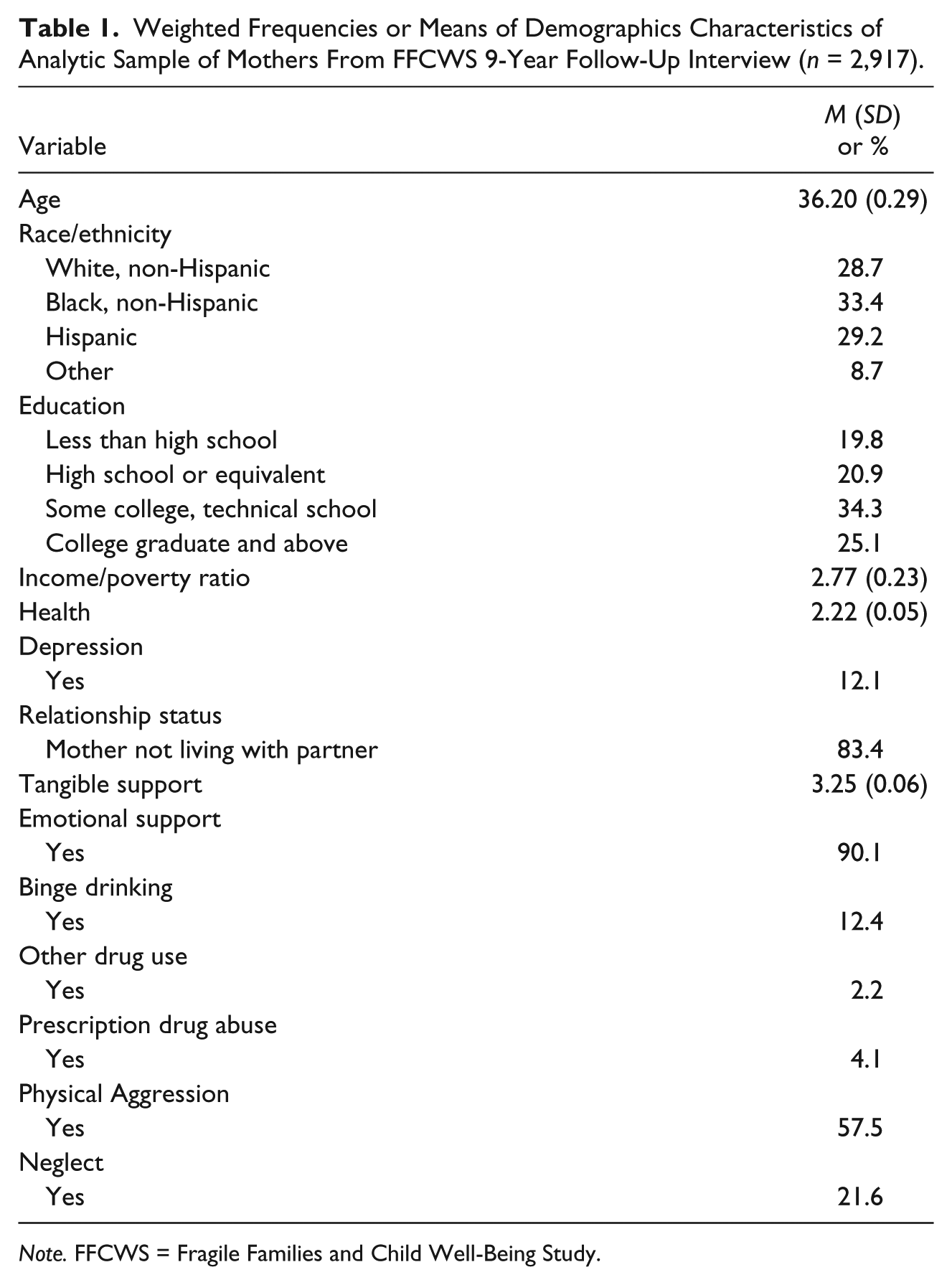
Note. FFCWS = Fragile Families and Child Well-Being Study.
Physical Abuse
The results of regression analyses are in Table 2. Black, non-Hispanic mothers had 2.18 odds of using physically aggressive parenting in the past year than White, non-Hispanic parents (95% confidence interval [CI] = [1.28, 3.70]). Mothers with worse health also had higher odds of physical aggression (1.30, 95% CI = [1.17, 1.45]). There was no association between prescription drug misuse in the past year and physically aggressive parenting.
Weighted Logistic Regression Analyses Examining Prescription Drug Misuse, Physical Aggression, and Neglect, Using the FFCWS (n = 2,917).
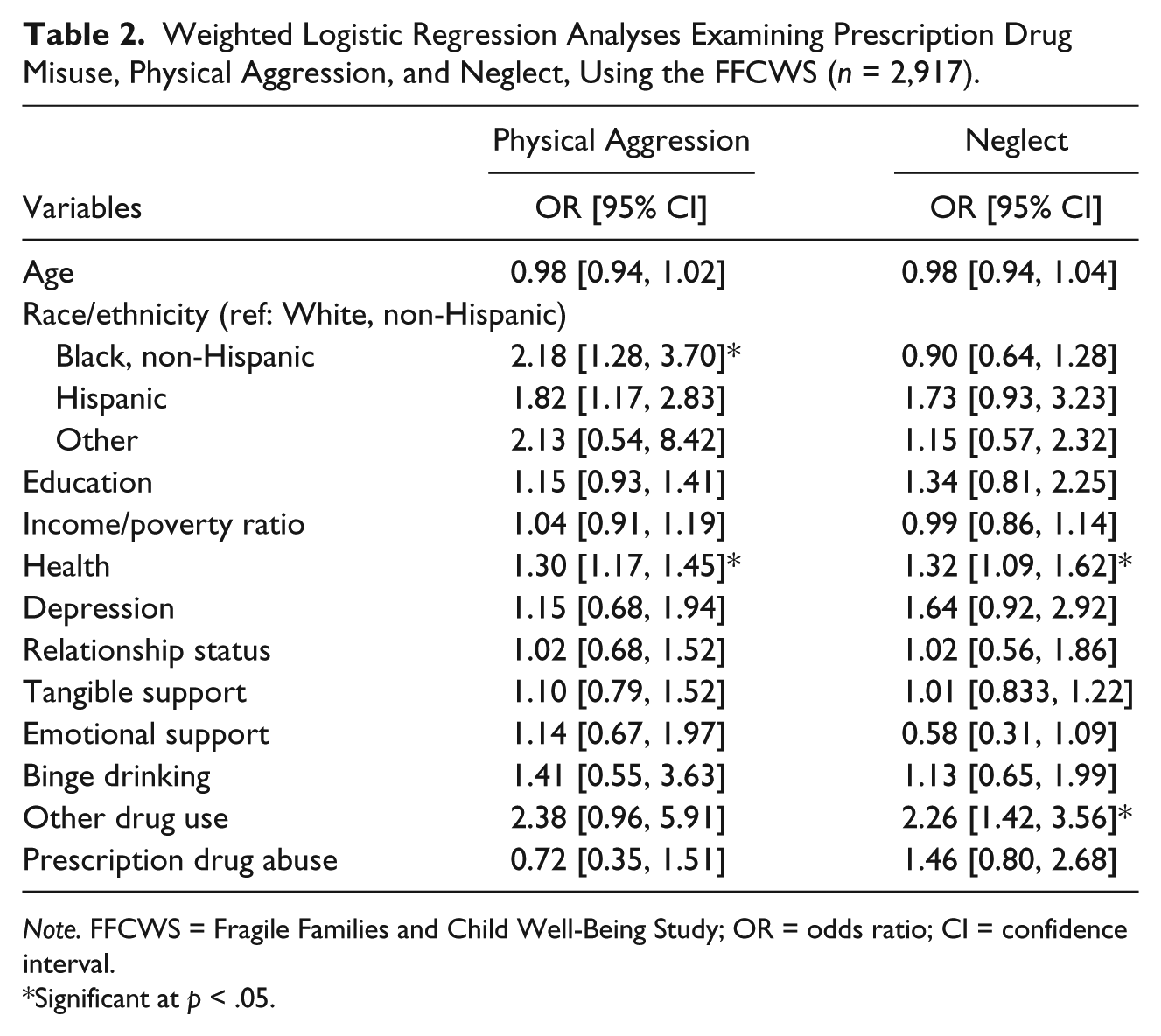
Note. FFCWS = Fragile Families and Child Well-Being Study; OR = odds ratio; CI = confidence interval.
Significant at p < .05.
Neglect
Mothers in worse health had greater odds of physical aggression (1.32, 95% CI = [1.09, 1.62]). There was no association between misuse of prescription drugs and physically aggressive parenting, although mothers who used illicit drug use had 2.26 odds of physical aggression (95% CI = [1.42, 3.56]).
Discussion
This study used a large, diverse, national sample of mothers to examine relationships between prescription drug misuse and two types of child maltreatment. The study analyses did not find any statistically significant associations between prescription drug misuse and either physical abuse or neglect, contrary to hypotheses. This indicates that although previous studies suggest prescription drug misuse may impact parenting negatively (Slesnick et al., 2014), it may not reach the threshold of physically aggressive or neglectful parenting. Other illicit drug use, however, was positively related to neglectful parenting, suggesting that mothers who used drugs such as marijuana, heroin, and cocaine had greater odds of committing at least one act of neglectful parenting in the past year. As some longitudinal research suggests that prescription drug misuse can lead to initiation of heroin use (Martins, Santaella, Marshall, Maldonado, & Cerda, 2015), further research could examine whether prescription drug misuse carries potential risk as a “gateway” substance to other drugs that negatively impact parenting.
Mother’s health was related to both child maltreatment outcomes, with poorer health increasing risk. It could be that the stress or symptoms of poor health led mothers to practice neglectful behaviors or harsh physical discipline. While health and misuse of prescription drugs or other illicit drugs were not highly correlated in this data set, further research might investigate whether mother’s may self-medicate with these substances, potentially raising risk for maltreatment.
This study has some limitations. Like most longitudinal studies, the FFCWS had attrition in subsequent follow-ups. In addition, the amount of missing values in the data set may affect the generalizability of these results. The number of prescription drug misusers in this sample was small (n = 184), potentially indicating a lack of power to detect relationships between the independent and dependent variables. However, power analyses taking into account the design effect of the FFCWS and an alpha of .05 suggested approximately .90 power to detect a small effect size using logistic regression. Future studies should further examine this relationship before any conclusions about these relationships are reached.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the College of Health and Human Services, California State University, Sacramento.