
Abstract
Intimate partner violence (IPV) victimization is often associated with negative mental health outcomes; yet, little is known about the psychological well-being of women who experience IPV and receive civil legal services. Civil legal services are not specifically designed to focus on women’s mental health needs but Sullivan’s Social and Emotional Well-Being Framework helps to explain why women receiving this type of formal assistance may demonstrate positive changes in psychological well-being. Using a panel study design and data from 85 women who experienced IPV and sought civil legal services, we examined women’s psychological well-being over a one-year period of time. Approximately two thirds of the women received assistance from Iowa Legal Aid (ILA) for a civil protective order (n = 56) and the rest were represented in a family law matter. We used measures of mental health (depression, posttraumatic stress disorder [PTSD]) and well-being (social support, resilience, goal directed thinking, empowerment). Our hypotheses that women would experience a decrease in mental health symptoms and an increase in well-being were partially supported. Women reported a decrease in depressive and PTSD symptoms over one year but there were no changes in their goal-oriented thinking or resilience. Implications for practice and future research are included.
The substantial lifetime prevalence of intimate partner violence (IPV) victimization is well documented among women in the United States (Breiding et al., 2014). Findings from the 2010 National Intimate Partner and Sexual Violence Survey (NISVS) revealed that 35.6% of females experienced rape, physical violence, and/or stalking by an intimate partner at some point in their lifetime, with the majority experiencing physical violence (Black et al., 2011). In a nationally representative sample of males and females (N = 11,291), 15.6% reported their current partner used at least one emotionally abusive behavior in the past year (Outlaw, 2009).
IPV victimization is associated with negative mental health outcomes. The sequelae of IPV often includes significant mental health consequences, with a substantial percentage of adult female victims reporting increased levels of depression and anxiety (Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012; Black, 2011; Fergusson, Horwood, & Ridder, 2005; Mechanic, Weaver, & Resick, 2008) and posttraumatic stress disorder (PTSD; Jones, Hughes, & Unterstaller, 2001).
Among women who experience IPV, legal services are the second most reported need after medical care (Black et al., 2011). Examining the needs of women who experienced IPV six months after leaving shelter programs, Allen, Bybee, and Sullivan (2004) found that 59% of these women identified working on legal issues unrelated to the prosecution of the perpetrator or obtaining a protection order. Instead, these women were seeking divorces; working out child custody, support, and visitation issues; or dealing with landlord/tenant or housing matters that were related to IPV. Civil legal services are not specifically designed to focus on women’s mental health needs; yet, Sullivan’s (2018) Social and Emotional Well-Being Framework helps to explain why women who experience IPV and receive civil legal services may show improvements in their psychological well-being.
IPV and Women’s Psychological Well-Being
In a review of research on IPV and mental health, rates of PTSD among women ranged from 31% to 84%; and, the more severe or life-threatening the violence and the more current the abuse, the more severe the PTSD symptoms (Jones et al., 2001). More severe PTSD symptoms, in turn, have the potential to interfere with day-to-day functioning (Gorde, Helfrich, & Finlayson, 2004). Women who experience IPV also report increased depressive symptoms compared with women who have not experienced IPV (Follingstad, 2009; Jones et al., 2001; Renner, 2009; Renner, Cavanaugh, & Easton, 2015).
Despite substantial documentation of how IPV victimization negatively affects women’s mental health, researchers have demonstrated that women who experience IPV exhibit significant resilience (Anderson, Renner, & Bloom, 2017; Anderson, Renner, & Danis, 2012; Humphreys, 2003). Social support is also a critical resource and protective factor for women (Goodman, Dutton, Vankos, & Weinfurt, 2005), given the social isolation that is often created by IPV. More specifically, social support has been shown to buffer the negative mental health outcomes as a result of abuse (Beeble, Bybee, Sullivan, & Adams, 2009; Carlson, McNutt, Choi, & Rose, 2002; Coker, et al., 2002). Unfortunately, researchers often overlook indicators of healthy functioning (Sabina & Banyard, 2015), such as empowerment and goal-oriented thinking, and this line of inquiry is limited in many studies focused on women who experience IPV.
Civil Legal Services and Women’s Well-Being
Limited research has examined the effects of civil legal services on psychological well-being. After six weeks of working with law school advocates who provided assistance with a civil protective order (CPO) due to IPV, women reported small but significant increases in emotional support compared with women seeking a CPO without the additional advocacy support (Bell & Goodman, 2001). When looking at a range of services (e.g., domestic violence counseling, legal advocacy, and hotline services), women who experienced IPV reported increased support, perceived improvement in their decision-making ability, and increased self-efficacy and coping when participating in some or all of these services (Bennett, Riger, Schewe, Howard, & Wasco, 2004). In a national evaluation of legal assistance for a sample of 120 women and four men who experienced IPV, the majority of clients (94%) reported very high levels of satisfaction with their attorney, and those who were satisfied described their attorneys as knowledgeable and effective at keeping them informed about their case (Institute for Law and Justice, 2005). Clients also described relational aspects such as their attorney being sensitive to their needs, a good listener, and comforting. When asked how the legal assistance affected their well-being, 83% described their living situation as better, 77% reported feeling safer, and 66% reported their self-esteem had improved. Overall, most clients reported feeling empowered by their civil legal experiences. Looking more generally at women’s interactions with the court system, when women have empowering experiences interacting with the courts, they report improved quality of life and reduced depression—independent of the outcome of the court case or their expectations of the court (Cattaneo & Goodman, 2010). Greater contact with advocates, civil attorneys, and prosecutors in a criminal court setting was also found to be associated with increased “perceived victim voice” (their measure of empowerment) in the court process (Cattaneo, Goodman, Epstein, Kohn, & Zanville, 2009). Civil legal services also address other outcomes, such as economic self-sufficiency, that likely affect women’s longer term psychological well-being (Farmer & Tiefenthaler, 2003; Hartley, Renner, & Mackel, 2013).
How IPV-Focused Services Support Women’s Psychological Well-Being
Sullivan’s (2018) Social and Emotional Well-Being Framework helps to explain how civil legal services likely have an impact on women’s psychological well-being. Based on the conservation of resources (COR) theory, Sullivan argues that for women experiencing IPV, psychological distress can be decreased if women experience gains in resources after suffering trauma-caused resource losses. COR theory also suggests that resource gains beget further resource gains, which explains why some researchers have found that women continue to benefit from advocacy services well past the receipt of those services (see studies cited in Sullivan, 2018). Sullivan posits that common program activities of domestic violence services—information provision, safety planning, skill building around coping, problem solving and resource attainment, empathy and respect, supportive counseling, and increased access to community resources—lead to intrapersonal (i.e., increased knowledge, skills and coping, decreased stress) and interpersonal and social changes (i.e., increased access to community resources and increased social support). The intrapersonal changes result in improved self-efficacy and hopefulness; and, the interpersonal and social changes lead to greater social connectedness, increased access to community and economic resources, increased safety, and improved physical and emotional health.
Expectations of Civil Attorneys Working With Women Who Experience IPV
Although civil legal services are not one of the typical domestic violence service programs referenced by Sullivan (2018), the American Bar Association (ABA; 2007) identified standards of practice for attorneys representing people who experience IPV in CPO cases. Attorneys are required to have competent knowledge of CPO laws as well as related legal issues such as housing, employment, child custody, and immigration issues that could also be affecting their clients. Yet, the standards go beyond mere legal competence. The ethical and legal standards of care require domestic relations (divorce, child custody, etc.) attorneys and attorneys representing clients in CPO cases to have competent knowledge of the dynamics of IPV (ABA, 2007; Burman, 2003) as well as an understanding of how a client’s cultural background or the impact of trauma may affect attorney–client communication and trust (ABA, 2007). Attorneys are expected to be familiar with and engage their clients in safety planning or work with domestic violence service providers to address client safety (ABA, 2007; Burman, 2003) and make referrals to mental health counseling or other community resources as needed.
Most significant, attorneys representing clients experiencing IPV should practice client-centered representation (ABA, 2007). This approach engages clients in active decision-making about their legal options. When advising clients of their legal options, attorneys are expected to remind clients that they are in control of their case and respect their client’s decisions regarding exercising those options. Attorneys are also directed to allow adequate time to communicate effectively with their clients through reflective listening during case preparation and in court proceedings (ABA, 2007). This holistic representation of clients clearly fits within Sullivan’s description of the key features of domestic violence programs of providing information, safety planning, skill building, emotional and concrete support, and increased access to community services. As such, it is reasonable to hypothesize that civil legal services have the potential to positively affect women’s psychological well-being.
To better understand changes in women’s psychological well-being as they engage in help-seeking efforts related to IPV, it is important to focus on women receiving different types of services, such as civil legal services—a type of formal assistance that is arguably underutilized and underrecognized as part of a coordinated response to IPV. It is also important to focus on changes in women’s social support, resilience, and empowerment in addition to measures of mental health. Thus, the purpose of our study was to examine changes in psychological well-being among women who experience IPV and receive civil legal services. We anticipated that women would report reductions in depressive and PTSD symptoms and increases in social support, resilience, goal-directed thinking, and empowerment over a one-year period.
Method
Data were taken from a two-year panel study of women who experienced IPV victimization and received civil legal services. Potential participants were self-identified victims of IPV who had contacted Iowa Legal Aid (ILA) for a civil legal matter. ILA is a nonprofit organization that provides civil legal services to low-income Iowans in all 99 counties from offices located in 10 Iowa cities. ILA handles approximately 20,000 cases per year, and addressing IPV-related issues is a long-standing priority. One third of ILA cases involve family law issues (divorce, custody, child support, etc.), with the majority of these involving IPV.
Data Collection
For this study, we recruited women who had a history of IPV and contacted ILA for services related to dissolution of a marriage (divorce), child custody and support issues, or a CPO. We looked at both the provision of family law services (divorce, child custody, child support) and CPOs, because after CPOs, family law services represent the largest category of legal services provided to women by legal aid offices (Institute for Law and Justice, 2005).
IPV was assessed by the ILA intake staff using a set of screening items focused on physical abuse (“Has your spouse or partner ever physically abused or threatened to harm you or your children?” and “Has your spouse or partner ever done any of the following to you or your children: pushed, hit, slapped, kicked, choked, threatened to hit you, threatened you with a weapon of any kind, thrown something at you, or grabbed you and stopped you from doing something?”), sexual abuse (“Has your spouse or partner ever forced you to have sex or engaged in unwanted sexual touching?”), stalking (“Has your spouse or partner ever done anything to make you feel that you were being stalked, such as following or spying on you, waiting for you outside of home/school/work, or making unwanted contact such as phone calls, mail, emails, or leaving gifts?”), and psychological abuse (“Has your spouse or partner ever done any of the following: threatened or attempted to kill himself or herself, destroyed your personal belongings, kept you from friends and family, told you where you are allowed to go, made you afraid of him or her, stopped you from leaving your house, or hurt your pets?”). Once a woman met ILA’s initial screening criteria for receiving services (a “yes” response to any of the screening items), inclusion criteria for the study were applied. Potential study participants (a) were female and 18 years of age or older; (b) were currently experiencing IPV, or had a recent history of being a victim of IPV; (c) had minor children in the home; and (d) had a civil legal service request for a family law–related issue or a CPO and their legal case was accepted by ILA.
Potential participants were recruited for the study after ILA decided to take their case. ILA staff tracked client cases through an intake system, and once the case was accepted, they contacted the clients to inquire whether they would be willing to share their contact information with the researchers. The recruitment and data collection period was from June 2012 through November 2015. For the 383 women who agreed to learn more about the study during this time period, ILA staff transferred contact information for these women to the researchers using a password-protected web file transfer service. A research assistant contacted women to explain the study and ask whether they were interested in participating. Women who verbally agreed to participate were assigned to an interviewer in their geographic area of the state, who contacted them to schedule the first interview. Contract interviewers in seven locations around the state conducted in-person interviews with participants using a structured interview guide. Interviewers conducted an initial assessment interview (Wave 1) and up to four follow-up interviews at 6, 12, 18, and 24 months (Waves 2-5). Women received a US$75 gift card for the first interview and a US$65 gift card for each follow-up interview. Women provided informed consent through a signed consent form at the first in-person interview. The study was approved by the University of Iowa Institutional Review Board.
A total of 150 women completed a Wave 1 interview. Approximately 75% (n = 112, 74.7%) of the Wave 1 sample was retained for Wave 2. Comparably, 75.9% (n = 85) of the Wave 2 sample was retained at Wave 3. However, these retention rates were not calculated based on the Wave 1 sample because women were not recruited as a single cohort. Rather, recruitment was ongoing and continued throughout the entire study. As such, some women were never able to be interviewed in later waves (e.g., a woman was recruited one month prior to the end of the study) and, thus, not able to be retained because the study ended.
Attrition analyses were conducted to explore associations between demographic variables and the presence of missing data at each wave. We also explored whether attrition was related to the study outcomes. To do this, we used chi-square tests and t tests to examine whether data from the preceding wave (Wave X) was associated with continued participation in the current wave (Wave X + 1). Retention at Wave 2 was influenced by education level and rurality, with women in rural settings and women with college degrees more likely to remain in the study. Women living in rural settings were also more likely to remain in the study at Wave 3. None of the study well-being outcomes or other characteristics (e.g., race/ethnicity, age, education, employment, legal case type) was related to whether participants remained in the study. Due to the limited number of women who were retained in Waves 4 and 5 (n = 56 and n = 32, respectively), the analyses were limited to data from Waves 1 through 3 to ensure the statistical validity of the findings. The final sample includes 85 women who participated in Waves 1, 2, and 3.
Sample
Table 1 presents the Wave 1 demographic and IPV-related descriptive statistics for the final sample. The mean age of the 85 respondents was 31.65 years (SD = 7.23 years). All the women had children, with the number ranging from one to nine, and an average of 2.53 (SD = 1.63). The majority of women in Wave 1 identified as non-Hispanic White (n = 73, 85.9%), although the percentage of non-Hispanic Black and Hispanic women was slightly higher than rates in the state as a whole (sample non-Hispanic Black = 5.9%, state = 3.4%; sample Hispanic = 7.1%, state = 5.6%; U.S. Census Bureau, 2015). Almost three quarters of the women had more than a high school education and only a little more than half of the women were working at least part time.
Wave 1 Descriptive Statistics and Abuse Characteristics (N = 85).
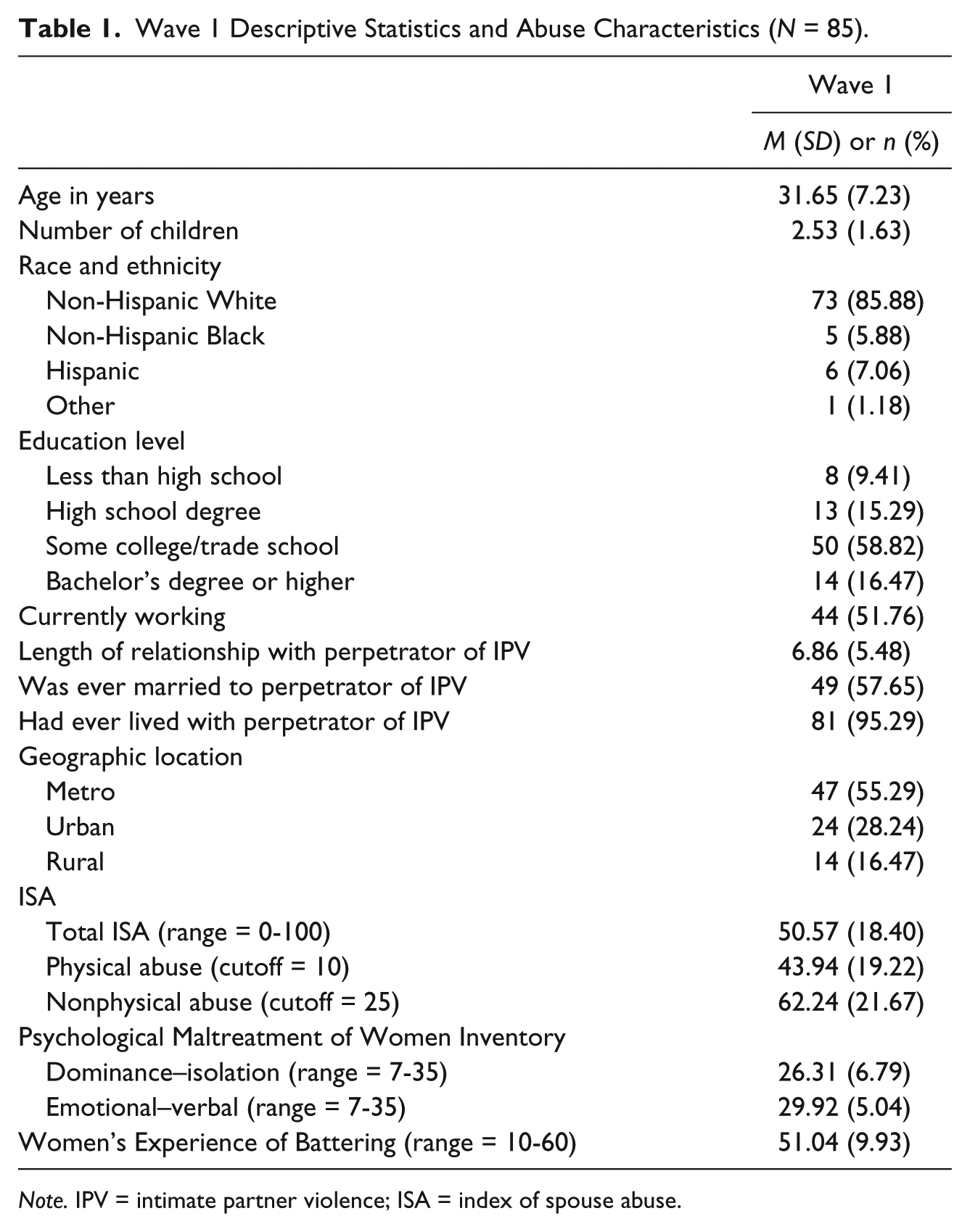
Note. IPV = intimate partner violence; ISA = index of spouse abuse.
All women had male partners who perpetrated violence against them. The average length of the relationship between the woman and her partner was 6.86 years (SD = 5.48 years). Almost all the women reported having lived with the perpetrator of IPV at some point (n = 81, 95.29%) but only 58% were ever married to him (n = 49). Approximately 66% of women (n = 56) received assistance from ILA for a CPO, whereas 34% (n = 29) sought services for a family law problem. The average amount of billable hours spent on a CPO case was 12.10 (SD = 6.46 hr, range = 3.50-35.30 hr) and the average hours spent on a family law case was 35.06 (SD = 28.14 hr, range = 10.50-137.65 hr). Each woman’s zip code was used to discern her county of residence at Wave 1. Counties were identified as metro and nonmetro (i.e., urban or rural) based on 2013 Rural Urban Continuum codes. Approximately 45% of the women lived in nonmetro/rural areas (n = 38, 44.71%).
At Wave 1, women in the sample reported high levels of physical and nonphysical IPV (Table 1). All the women were above the clinical cutoff scores on the Index of Spouse Abuse (ISA; Hudson & McIntosh, 1981) physical abuse subscale (cutoff of 10) and 94% were above the cutoff of 25 for the nonphysical abuse subscale. Emotional–verbal abuse and dominance–isolation were measured by the short form of the Psychological Maltreatment of Women Inventory (PMWI-F; Tolman, 1999) and also indicated high levels of abuse, with means for both subscales above 26 (range = 7-35). Finally, the mean score on the Women’s Experience of Battering (WEB; Smith, Smith, & Earp, 1999) was 51.04 on a scale of 10 to 60.
Measures
Depressive symptoms
Depressive symptoms were measured by the 20-item Center for Epidemiologic Studies–Depression (CES-D) Scale (Radloff, 1977) total score. The CES-D measures the frequency of depressive symptomatology in the past 7 days. Items include “I felt I was just as good as other people,” “I felt that everything I did was an effort,” and “I had trouble keeping my mind on what I was doing.” Response options range from rarely or none of the time to most or all of the time. Positive items were reverse coded and all 20 items were summed. Total scores range from 0 to 60, with higher scores indicating higher levels of depressive symptoms. The CES-D has demonstrated high construct and concurrent validity when compared with clinical diagnostic criteria, as well as good internal consistency and test–retest reliability (Radloff, 1977). Cronbach’s alpha for the CES-D in this sample was .92, .89, and .91 for Waves 1, 2, and 3, respectively.
PTSD
The Impact of Event Scale–Revised (IES-R; Weiss & Marmar, 1996) was used to measure subjective distress to traumatic events. The 22-item IES-R measures the level of symptomatic response to traumatic stressors in the last seven days across three subscales: Intrusion (eight items), Avoidance (eight items), and Hyperarousal (six items). Example items include “You were jumpy and easily startled” and “You tried not to think about it.” Each scale item uses a 5-point response option ranging from not at all to extremely. Average scores, ranging from 0 to 4, were computed. The IES-R had good reliability for all three subscales for all waves (Wave 1 Cronbach’s αs = .92, .84, and .89 for the Intrusion, Avoidance, and Hyperarousal subscales, respectively; Cronbach’s αs for Waves 2 and 3 were as follows: Intrusion = .95 and .94, Avoidance = .87 and .89; and Hyperarousal = .92 and .90).
Support
The Interpersonal Support Evaluation List (ISEL; Cohen & Hoberman, 1983; Cohen, Mermelstein, Karmarck, & Hoberman, 1985) is a 40-item scale that was used to measure women’s perceived availability of tangible assets support, appraisal support, self-esteem support, and belonging support. Tangible assets support captures the perceived availability of material aid; appraisal support is the perceived availability of someone to discuss issues of personal importance; self-esteem support is the perceived availability of others with whom one compares favorably; and belonging support is the perceived availability of others to interact with socially. All answers are given on a 4-point scale ranging from definitely false to definitely true. Scores on each subscale range from 0 to 30, with higher scores indicating higher levels of support. The measure has good reliability for the current sample for all subscales for all waves. Wave 1 alphas for the subscales ranged from .85 (self-esteem support) to .91 (appraisal support). Cronbach’s alpha for the ISEL subscales for Waves 2 and 3 were tangible assets support = .92 and .91, appraisal support = .90 and .89, self-esteem support = .83 and .79, and belonging support = .89 for both waves.
Resilience
The Connor Davidson Resilience Scale (CD-RISC; Connor & Davidson, 2003) was used to measure women’s resilience. The CD-RISC is a 25-item self-report scale addressing psycho–social–spiritual aspects of resilience displayed in the last month (e.g., “I am able to adapt when changes occur” and “I am not easily discouraged by failure”). Response options are based on a 4-point scale that ranges from not true at all to true nearly all the time. Responses were summed to create a total score that could range from 0 to 100, with higher scores representing greater levels of resilience. The CD-RISC has been tested in the general population as well as clinical samples and has demonstrated sound psychometric properties (Connor & Davidson, 2003). The CD-RISC has also previously been used with survivors of IPV (Anderson et al., 2012). Cronbach’s alpha for the CD-RISC in this sample were .93, .93, and .94 for Waves 1, 2, and 3, respectively.
Goal-directed thinking
The State Hope Scale (Snyder et al., 1996) is a six-item measure of ongoing goal-directed thinking with an 8-point response scale ranging from definitely false to definitely true. The total score is a sum of all six items, and two subscales are created to represent women’s agency (belief in self-capacity to initiate and sustain actions) and pathways (belief in self-capacity to generate routes) to reach their goals. The total score can range from 6 to 48, with each subscale score ranging from 3 to 24. Higher scores indicate greater degrees of goal-directed thinking. Reliabilities for Wave 1 were acceptable, with alphas of .85 for the total measure, .82 for agency, and .72 for pathways. Cronbach’s alphas for the Wave 2 and Wave 3 total score were .88 and .90, respectively; and .79 and .85 for the Agency subscale and .85 and .84 for the Pathways subscale.
Empowerment
The Personal Progress Scale–Revised (PPS-R; Johnson, Worell, & Chandler, 2005) measured empowerment defined as the ability to access skills and resources to cope with current and future stress and trauma. The 26 items are rated on a 7-point scale based on the women’s perceptions of how true (almost never true to almost always true) each item is as it applies to her now. The total score is an average of all items with higher values indicating a greater sense of empowerment. Cronbach’s alpha for the PPS-R in this sample was .99, .90, and .90 for Waves 1, 2, and 3, respectively.
Civil legal services
The type of legal representation was defined as either family law (e.g., divorce, custody) or CPO, which was entered into the analyses as a dichotomous variable. Although clients receive free legal services, legal aid attorneys are required to record the amount of time spent on each case. The amount of service time was defined as the number of billable hours recorded by ILA, and this was entered into the analyses as a continuous variable.
Demographic variables
Information on demographic variables was collected at Wave 1. These variables included women’s age, number of children, race/ethnicity, highest education level, employment status, length of the relationship with the person who perpetrated the IPV, and ever married to or lived with the perpetrator of IPV.
Data Analysis
To describe the sample and provide information on key variables, we performed descriptive and bivariate analyses. Descriptive statistics for the psychological well-being measures at each wave are presented in Table 2. To meet the study purpose, a repeated measures ANOVA was conducted with each well-being variable to examine changes over time. For these analyses, we focused on the depressive and PTSD symptoms, support, resilience, goal-directed thinking, and empowerment measured at Waves 1, 2, and 3. We further examined changes in well-being by taking into account the type of civil legal service (CPO or family law) and the amount of service hours (i.e., billable hours or time spent on a case) received; although we had no hypotheses related to the type or amount of services. Thus, for each outcome, up to two models were fitted. The first model was a repeated measures ANOVA using Waves 1, 2, and 3, with no covariates. If significant overall main effects were found, post hoc t tests were conducted to determine the pattern of change over time. This was also followed by a model where two covariates, the type of legal services and the amount of service hours, were entered. Assumptions of compound symmetry were met for all models and the sphericity assumptions (using Mauchly’s test) were met for all the repeated measures ANOVA models, except one. For the self-esteem support variable, Mauchly’s test indicated that the assumption of sphericity had been violated, χ2(2) = 7.84, p < .05; therefore, the Greenhouse–Geisser estimate of sphericity was used. All analyses were performed using SPSS version 22.
Means and Standard Deviations for Psychological Well-Being Measures at Each Wave (N = 85).
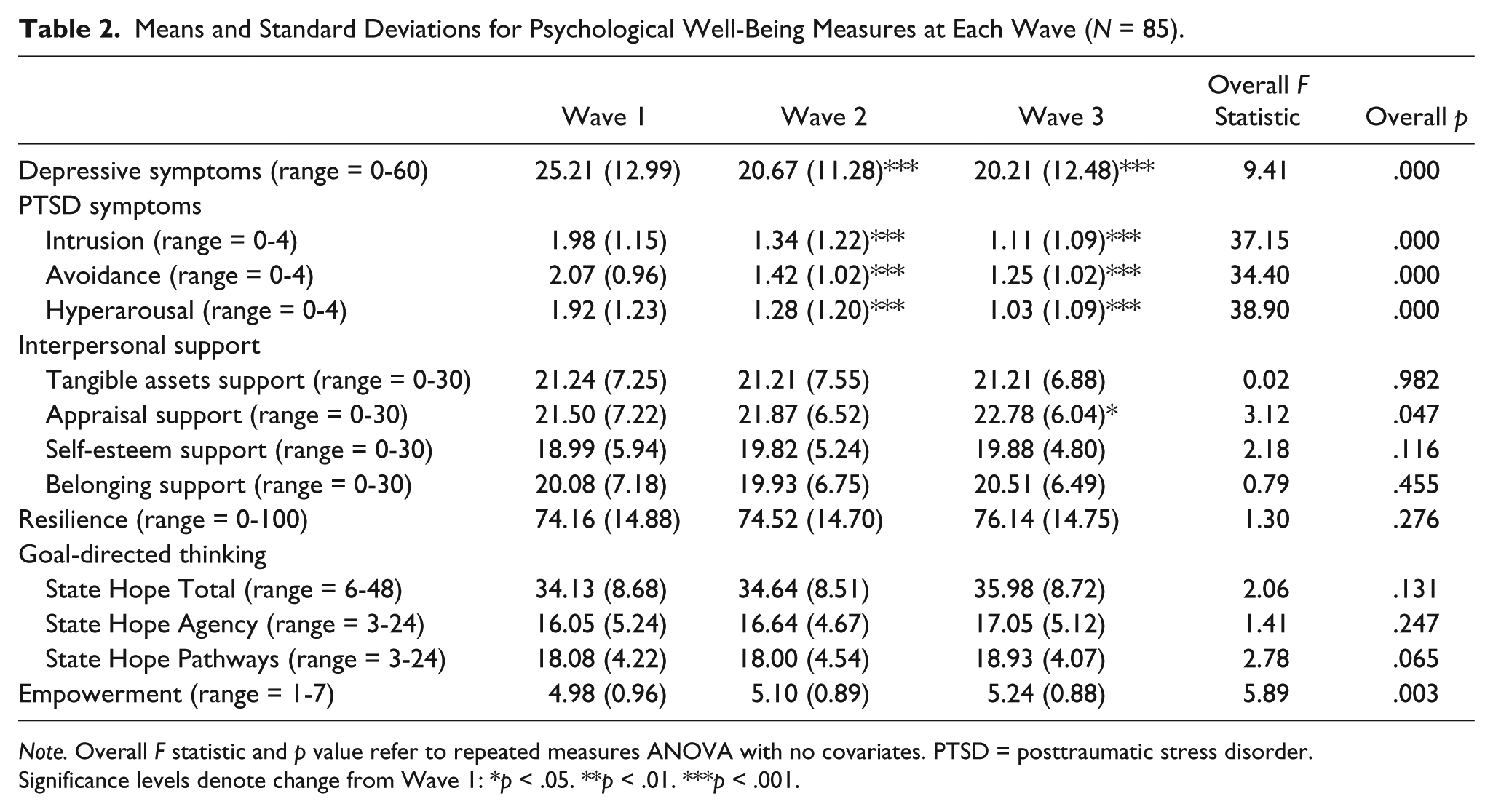
Note. Overall F statistic and p value refer to repeated measures ANOVA with no covariates. PTSD = posttraumatic stress disorder.
Significance levels denote change from Wave 1: *p < .05. **p < .01. ***p < .001.
Results
A statistically significant decrease in women’s depressive symptoms scores between Waves 1 and 3, F(2, 168) = 9.41, p = .000, was found. Post hoc paired-samples t tests showed that depressive symptoms scores at Wave 1 were significantly higher than scores at each of the subsequent time points: Wave 1/Wave 2: t(84) = 3.70, p = .000; Wave 1/Wave 3: t(84) = 3.79, p = .000. There was no significant mean difference in depressive symptoms scores between Wave 2 and Wave 3. The significant decrease in depressive symptoms scores over time was maintained after adding two covariates into the model, F(2, 164) = 6.05, p = .003; however, there was no statistically significant difference associated with the types of legal services, F(2, 164) = 0.80, p = .452, or the amount of services, F(2, 164) = 0.97, p = .380.
With respect to the intrusive thoughts related to PTSD, a statistically significant decrease in intrusion scores between Waves 1 and 3, F(2, 168) = 37.15, p = .000, was found. Post hoc paired-samples t tests showed that intrusion symptom scores at Wave 1 were significantly higher than scores at each of the subsequent time points: Wave 1/Wave 2: t(84) = 5.84, p = .000; Wave 1/Wave 3: t(84) = 8.86, p = .000; with a significant decrease also found between Wave 2 and Wave 3: t(84) = 2.14, p = .035. This significant decrease in symptoms over time was retained after adding the covariates, F(2, 164) = 19.96, p = .000; however, the type of legal services, F(2, 164) = 0.98, p = .379, and the amount of hours spent on a case were unrelated to intrusive thoughts, F(2, 164) = 1.53, p = .219. The repeated measures analysis for the avoidance outcome also showed a statistically significant decrease in avoidance scores between Waves 1 and 3, F(2, 168) = 34.40, p = .000. Post hoc paired-samples t tests showed that avoidance symptom scores at Wave 1 were significantly higher than scores at each of the subsequent time points: Wave 1/Wave 2: t(84) = 6.45, p = .000; Wave 1/Wave 3: t(84) = 7.22, p = .000. This change over time was maintained after adding the two covariates, F(2, 164) = 18.37, p = .000. There was a statistically significant decrease in hyperarousal scores between Waves 1 and 3, F(2, 168) = 38.90, p = .000. Post hoc paired-samples t tests showed that hyperarousal symptom scores at Wave 1 were significantly higher than scores at each of the subsequent time points: Wave 1/Wave 2: t(84) = 6.27, p = .000; Wave 1/Wave 3: t(84) = 8.21, p = .000; with a significant decrease also found between Wave 2 and Wave 3: t(84) = 2.51, p = .014. Again, this change over time was maintained after controlling for the type and amount of services, F(2, 164) = 17.89, p = .000. There were no statistically significant changes in the avoidance and hyperarousal outcome based on the type or amount of legal services received.
A statistically significant increase in appraisal support scores between Waves 1 and 3, F(2, 166) = 3.12, p = .047, was found. Post hoc paired-samples t tests showed that appraisal support scores at Wave 1 were significantly lower than scores at Wave 3: Wave 1/Wave 3: t(83) = −2.63, p = .010. There were no significant differences between other points of comparison. In models with no covariates yet added, there were no significant changes in reports of tangible support, F(2, 166) = 0.02, p = .982, self-esteem support, F(1.83, 152.12) = 2.18, p = .121, or belonging support, F(2, 166) = 0.79, p = .455, over time. After adding in the two covariates to the repeated measures ANOVA with the appraisal support outcome, there was no longer a statistically significant change in appraisal support scores between Waves 1 and 3, F(2, 162) = 0.36, p = .699, and no statistically significant differences between the types of legal services, F(2, 162) = 0.24, p = .785, or the amount of service hours, F(2, 162) = 0.41, p = .663.
For all three State Hope Scale outcomes, the Agency, F(2, 168) = 1.41, p = .247, and Pathway, F(2, 168) = 2.78, p = .065, subscales and the total score, F(2, 168) = 2.06, p = .131, the repeated measures results showed no statistically significant change in scores between Waves 1, 2, and 3, with no covariates included. Results of a repeated measures ANOVA with no covariates also showed no statistically significant change in women’s resilience (CD-RISC) scores from Wave 1 to Wave 3, F(2, 168) = 1.30, p = .276.
A statistically significant increase in women’s empowerment scores from Waves 1 to 3, F(2, 168) = 5.89, p = .003, were found. Post hoc paired-samples t tests showed that empowerment scores at Wave 1 were significantly lower than scores at Wave 3: Wave 1/Wave 3: t(84) = −3.22, p = .002. There was no significant mean difference in empowerment scores between Wave 1 and Wave 2 (p = .112) or between Wave 2 and Wave 3 (p = .06). After adding in the two covariates to the repeated measures ANOVA, there was no longer a statistically significant change in empowerment scores between Waves 1 and 3, F(2, 164) = 2.16, p = .119, and no statistically significant differences between the types of legal services, F(2, 164) = 1.19, p = .307, or the amount of service hours, F(2, 164) = 0.17, p = .846.
Discussion
The purpose of this study was to examine changes in psychological well-being among women who experience IPV and received civil legal services. We anticipated that women would report reductions in depressive and PTSD symptoms and increases in social support, resilience, goal-directed thinking, and empowerment over a one-year period.
At the Wave 1 interview, many women reported psychological well-being scores that might raise clinical concerns. Sixty-seven percent of women met the clinical criteria for depression and 64% of women met the clinical criteria for PTSD. Women reported modest levels of social support and resilience; and, despite the presence of IPV, depressive symptoms, and PTSD symptoms, most women still reported adequate levels of goal-directed thinking and empowerment.
We expected women receiving civil legal services to have improvements in psychological well-being over a one-year period of time. Our overall hypothesis was partially supported. Women’s depressive symptom score decreased by 19.83% between Wave 1 and Wave 3, and significant decreases in PTSD symptoms were also reported over this same one-year period (decreases in intrusion, avoidance, and hyperarousal scores were 43.95%, 39.61%, and 46.35%, respectively). Women’s goal-oriented thinking, resilience, and social support levels did not significantly change from Waves 1 to 3, with the exception of scores on the Appraisal Support subscale, which increased by 5.95% over a one-year period. However, these indicators of well-being were quite high at Wave 1 and there was little room for improvement. In fact, women’s scores on the resilience measure were between 74.2 and 76.1 across Waves 1, 2, and 3; and, the average score for the U.S. population is 80.4 (Connor & Davidson, 2003). Thus, the women in the study were quite resilient and displayed many strengths, which is not unlike findings from other studies (e.g., Anderson et al., 2012), which show high levels of resilience among women who experience IPV.
Our overall hypothesis was supported by the fact that women showed improvements in various facets of psychological well-being over time, although we found no relation between the type or amount of legal services received and changes in women’s depressive symptoms, traumatic stress responses, or other measures of well-being. This lack of findings related to the amount or type of services received might seem curious at first, particularly given the fact that the amount of time attorneys spent on women’s cases ranged from as little as 3.5 hours to more than 130 hours; and, for half the women receiving assistance with a CPO, the number of billable hours was 10 or less. However, the lack of any significant association between the type or amount of civil legal service received and women’s psychological well-being is consistent with Sullivan’s Social and Emotional Well-Being Framework, in that, it is not the type or amount of services received, but rather the nature of the activities and supports provided in the course of providing civil legal services that influence changes in psychological well-being. Thus, any receipt of services through legal aid that are focused on reducing IPV or increasing individual and/or family well-being, regardless of type of case or amount of time spent on a case, should positively affect women’s well-being.
Study Strengths and Limitations
One strength of this study was the focus on a sample of women who experience IPV and were receiving civil legal services, which is lacking in extant literature. However, selection bias in the initial recruitment may have limited the generalizability of the results. We were not able to examine possible nonresponse bias of women who declined to share their contact information as information about nonparticipants was not available to us. ILA also has income restrictions for case eligibility and they must prioritize cases due to limited resources. Thus, the results of our study may only apply to lower income women experiencing IPV who were dealing with more imminent legal needs due to the IPV. Finally, the sample focused only on women whose primary contact with ILA was for one of the two most commonly sought types of legal services by women experiencing IPV: assistance with a CPO or a family law case (divorce, child custody, and/or child support). Our results might be different if women seeking other types of legal services, such as employment and housing discrimination, consumer law, tort claims, and administrative cases pertaining to denials of income benefits, were the focus. In addition, we cannot claim that improvements in psychological well-being were caused by receiving civil legal services. In the future, researchers are encouraged to design studies with a control group to more effectively examine the benefits of receiving legal services.
Another potential limitation is that nearly all the variables were based on women’s self-reports and may be limited by recall and social desirability. Women were the sole respondents regarding their victimization and mental health and there was no way to triangulate and assess the reliability of their responses. A strength of the study, however, was the vast array of concepts that were measured. Women who experience IPV are not a homogeneous group, and as such, we included instruments that allowed for a continuum of psychosocial measures of mental health, empowerment, resilience, and goals. Rather than operate from a deficit-oriented lens, we largely selected measures that focused on women’s strengths, which is an underrecognized focus of IPV research.
Retention was also a challenge in our study, which might influence the results. As stated previously, only 75% of the current Wave 1 sample was retained for Wave 2, and the retention rate in subsequent waves was less than this. However, it is important to note that some women were not retained in the study only because the time allowed for the study had ended. Although whether women were retained in the study or not was not significantly associated with their psychosocial functioning or most demographic characteristics, there may be traits among the study participants that accounted for their improvements in well-being that were not captured in this data collection. Despite the significant attrition rate over time, however, one strength of our study remains its longitudinal design and repeated measures. Cross-sectional studies are often ill equipped to establish temporal ordering among variables of interest or to address research questions that rely on data from multiple time points.
Implications for Practice
Examining civil legal services as part of a coordinated response to IPV continues to be largely absent from criminal justice and social service research and practice literature (Hartley et al., 2013); yet, we know that IPV has a “radiating impact” (Riger, Raja, & Camacho, 2002) on multiple areas of women’s lives. Although civil legal services are not specifically intended to address women’s psychological well-being, the receipt of such legal assistance has been shown to play a role in helping to stabilize women’s safety and economic situations (Hartley & Renner, 2016), which may in turn, help improve their psychological well-being. Thus, it appears that civil legal services are a critical component of a coordinated community response to IPV that can enhance women’s longer term quality of life. As such, civil legal services should be included along with the more recognized community responses of the criminal justice system, social service agencies, and domestic violence shelters.
Implications for Future Research
In this study, we focused on two types of civil legal services, family law and CPOs, in a state with a mostly homogeneous population. Researchers can build on our study in a variety of ways. Although family law and CPO cases represent the largest service requests of women experiencing IPV, there are other legal needs that have the potential to address longer-term safety and empowerment of survivors as well, such as employment and housing discrimination, tort claims, and even Title IX violations. Future research should expand the focus to the full range of civil legal remedies available and also examine civil legal representation for enforcing victim’s rights in criminal proceedings.
Future studies focused on women who experience IPV and receive civil legal services need to include more diverse samples and even national probability samples that are more representative of women in other locations. This study only included lower-income women who met the income means test for legal aid services. In the future, researchers should examine the legal needs of women who are not income eligible for legal aid services to determine if and where they are getting their legal needs met. If methodological and ethical challenges can be addressed, comparative studies of the effects of civil legal services for women who did and did not receive services would also be beneficial.
Footnotes
Acknowledgments
We would like to thank Shellie Mackel, Dennis Groenenboom and the AmeriCorps workers at Iowa Legal Aid for their support and contributions to the project. We also thank the research assistants and interviewers who devoted so much time and effort to the project. Finally, we thank the women who participated in the project and shared their experiences. Their strength and courage are truly remarkable and we hope this, and all publications from this project, honors their voices.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Award No. 2010-WG-BX-0009, awarded by the National Institute of Justice, Office of Justice Programs, U.S. Department of Justice. The opinions, findings, and conclusions or recommendations expressed in this publication are those of the authors and do not necessarily reflect those of the Department of Justice.