
Abstract
Intimate partner violence (IPV) perpetrators commonly exhibit deficits in a wide range of cognitive domains, such as attention, memory, and executive functions. Executive dysfunctions tend to be related to a preference for disadvantageous decisions, which could be explained by a pattern of focusing on positive outcomes (gains) while disregarding negative ones. Nonetheless, it is less clear whether risk-taking and decision-making problems should be attributed to motivational and/or emotional causes or to cognitive deficits in attention and/or working memory. The main goal of the present study was to examine whether IPV perpetrators can be distinguished from non-violent controls based on their performance on attention, working memory, and decision-making tests from a computerized battery of tests. In addition, this study investigated the potential relationship between attention and working memory impairments in the decision-making abilities of IPV perpetrators. Our data indicated that IPV perpetrators perform worse than controls on measures of attention and sustained attention, processing speed, working memory, spatial span, and decision making. Moreover, IPV perpetrators’ preference for disadvantageous and risky decisions could be partially explained by attention and working memory impairments. Our study has enabled us to explore the cognitive deficits underlying IPV perpetration as key factors in reducing IPV risky decisions. Moreover, it reinforces the need to develop specific neuropsychological training in the attention-switching ability in general and working memory, which could lead to improvements in decision-making processes or other executive functions.
Keywords
Introduction
The extant literature on cognitive deficits in intimate partner violence (IPV) perpetrators shows that IPV perpetrators commonly exhibit deficits in a wide range of cognitive domains, such as processing speed, verbal and attention skills, abstract reasoning, and working and long-term memory, compared with non-violent men (Romero-Martínez & Moya-Albiol, 2013). Moreover, IPV perpetrators have been reported to present executive dysfunctions, such as high mental rigidity, low levels of inhibition, and poor ability to make decisions (Romero-Martínez, Lila, Catalá-Miñana, Williams, & Moya-Albiol, 2013; Romero-Martínez, Lila, Martínez, Pedrón-Rico, & Moya-Albiol, 2016; Romero-Martínez, Lila, & Moya-Albiol, 2016; Romero-Martínez, Lila, Sariñana-González, González-Bono, & Moya-Albiol, 2013; Romero-Martínez & Moya-Albiol, 2013).
Executive functions (EFs) include a set of cognitive processes that include decision making, cognitive flexibility, planning skills, inhibition, interference control, and working memory, among others (Diamond, 2013). Thus, alterations in EFs may decrease behavioral control and lead to the adoption of risky behaviors and pleasure seeking in a context of extreme impulsivity, anxiety, aggression, and low self-regulation (Hancock, Tapscott, & Hoaken, 2010; Hofmann, Schmeichel, & Baddeley, 2012; Holler & Kavanaugh, 2013), which is the case of IPV perpetrators (Romero-Martínez & Moya-Albiol, 2013). This poor behavioral regulation would, in turn, reinforce immediate gratification, regardless of the positive or negative future consequences.
Neuropsychological testing of people with executive dysfunctions has revealed that they tend to present a preference for disadvantageous decisions, which could be explained by a pattern of focusing on positive outcomes (gains) while disregarding negative ones (losses). Two complementary explanations for this phenomenon would be that they also show a tendency to focus on recent outcomes and ignore or rapidly discount past outcomes and that they may make random choices (Swami, 2013). Moreover, non-aggressive adults and males in prison characterized by high impulsivity tend to present behavioral disinhibition, aversion to delayed rewards, and rushed decision making without considering the consequences (Denson, Capper, Oaten, Friese, & Schofield, 2011; Meijers, Harte, Jonker, & Meynen, 2015). This dysregulation of the reward system could potentially contribute to risk-taking because delay aversion can lead to the avoidance of choices that are only beneficial in the longer term, and because behavioral disinhibition can easily lead to ignoring more advantageous alternatives. Hence, deficits in EFs often lead to inappropriate decision making and unnecessary risk-taking in situations such as substance abuse and criminal activities (Lee, Humphreys, Flory, Liu, & Glass, 2011). Nonetheless, it is less clear whether risk-taking and decision-making problems should be attributed to motivational-emotional causes or cognitive deficits in other process such as attention and/or working memory.
It has been hypothesized that attentional, working memory and decision-making impairments are not independent (McCabe, Roediger, McDaniel, Balota, & Hambrick, 2010). In fact, previous meta-analytic studies demonstrated that there is a certain overlapping between impairments in sustained attention and decision making in adults with attention deficit hyperactivity disorder (ADHD; Dekkers, Popma, van Rentergem, Bexkens, & Huizenga, 2016; Mowinckel, Pedersen, Eilertsen, & Biele, 2015). Moreover, the memory plays an important role in directing the attention and searching for strategies to anticipate changes (Afonso, Garganta, & Mesquita, 2012). Because working memory is required to compare new data with data previously stored in the memory, its impairment increases the risk of not adequately maintaining, monitoring, and evaluating relevant information for decision making (Afonso et al., 2012; Duarte et al., 2012). Thus, all these cognitive processes might support the functioning of other higher order cognitive processes such as decision making. Making good decisions requires rapid and accurate functioning, as well as the ability to deal with information overload. Nevertheless, to our knowledge, there is a gap in the scientific literature analyzing how risk-taking and decision-making problems in IPV perpetrators could be attributed to cognitive deficits such as attention and/or working memory impairments.
The main goal of the present study was to examine whether IPV perpetrators can be distinguished from non-violent controls matched on demographic variables, based on their performance on attention, working memory, and decision-making tests from a computerized battery of tests, the Cambridge Neuropsychological Test Automated Battery (Cambridge Cognition, 2012). Based on previous studies that analyzed these cognitive domains in IPV perpetrators (Romero-Martínez et al., 2013; Romero-Martínez, Lila, Martínez, et al., 2016; Romero-Martínez, Lila, & Moya-Albiol, 2016; Romero-Martínez & Moya-Albiol, 2013), we hypothesized that the IPV perpetrators would display worse attention and working memory abilities, longer decision latencies, and more risk-taking, reflecting worse decision making compared to non-violent controls. In addition, this study investigated the potential relationship between attention and working memory impairments in the decision-making abilities of IPV perpetrators. Based on data linking these cognitive processes (Dekkers et al., 2016; Duarte et al., 2012; McCabe et al., 2010; Mowinckel et al., 2015), we hypothesized that attention and working memory impairments would partially explain the risk-taking and decision-making problems of IPV perpetrators. The analysis of these variables and their relationships may offer a more complete explanation of the complex phenomenon of domestic violence and help to develop new neuropsychological intervention programs to complement the existing psychotherapeutic programs.
Method
Participants
The final sample was composed of 90 men without any organic and/or mental illnesses (51 IPV perpetrators and 39 controls) who participated voluntarily in the study. IPV perpetrators were volunteers recruited from men taking part in the Contexto psycho-educational and community-based treatment program (mandatory for male abusers). They had been sentenced to less than 2 years in prison and had no previous criminal record. Therefore, they had their sentence suspended on the condition that they attend an intervention program (Carbajosa, Catalá-Miñana, Lila, & Gracia, 2017; Catalá-Miñana, Lila, Conchell, Romero-Martínez, & Moya-Albiol, 2013; Lila, Gracia, & Catalá-Miñana, 2020; Lila, Gracia, Catalá-Miñana, Santirso, & Romero-Martínez, 2016; Lila, Oliver, Galiana, & Gracia, 2013). Controls were recruited via Internet advertisements and by posting flyers around our city from January 2016 to August 2016. They were matched on sociodemographic characteristics. The study was performed in accordance with the Helsinki Declaration and approved by the University of Valencia Ethics Committee (H1348835571691).
Procedure
All the participants attended two sessions at the Faculty of Psychology at the University of Valencia. In the first session, participants were interviewed to exclude those with organic diseases that could interfere with the neuropsychological assessments, and sociodemographic data were collected through a semi-structured interview. Then, participants were asked about their alcohol and cigarette consumption, in terms of the amount consumed, using AUDIT to check for alcohol use frequency, and the Fragerström test of nicotine dependence to assess the addiction level. Only those individuals with an alcohol intake of less than 30 g/day and fewer than two Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) symptoms of alcohol use disorder and/or other substance use disorders (i.e., nicotine, cocaine, etc.) were included, as recommended by previous research in this field (Cao, Willett, Rimm, Stampfer, & Giovannucci, 2015; Cho, Lee, Rimm, Fuchs, & Giovannucci, 2012). Finally, they were asked if they had a history of traumatic brain injury, noting whether they had lost consciousness during the trauma; for example, if they had been involved in fights, and if so, how often this had resulted in head injuries or blackouts after these injuries (i.e., skull fracture, brain hemorrhage, subdural hematoma, intracranial hemorrhages, etc.). If participants reported head injuries with moderate to severe levels of loss of consciousness, they would be removed from the study. In fact, only those individuals who reported mild traumatic brain injury (TBI) without direct and/or indirect sequelae (i.e., infrequent and accidental soccer ball head impact, any accidental head impact in sports, casual head impacts at home, etc.) were included in our study.
In the second session, during the following week, a range of neuropsychological variables were assessed using traditional tests and the computer-based CANTAB. Attention was assessed with the Attention Switching Task (AST), Rapid Visual Information Processing (RVP), and Choice Reaction Time (CRT); memory with the Spatial Span (SSP); and decision making with the Cambridge Gambling Task (CGT). The end of the assessment was marked by a sign that said “Thank you very much.” Participants were paid €50 for their participation and told that they could leave.
Neuropsychological assessment
AST measures the ability to switch attention between the direction of an arrow and its location on the screen and avoid distracting events. Participants have to switch their attention from congruent (e.g., arrow on the right side of the screen pointing to the right) to incongruent stimulus (e.g., arrow on the right side of the screen pointing to the left) presentations. The dependent variable for this study was the percentage of correct responses (Cambridge Cognition, 2012).
RVP measures sustained attention. On this test, a white box appears at the center of the computer screen. Inside the box, digits from 2 to 9 are randomly presented. Subjects have to detect specific target sequences containing three consecutive digits (e.g., 2,4,6; 3,5,7; and 4,6,8). The dependent variable for this study was response accuracy (Cambridge Cognition, 2012).
CRT is a two-choice reaction time test that assesses attentional ability and reaction times. It includes a practice stage of 24 trials and two assessment stages of 50 trials each. Dependent variables for this study were correct latency in milliseconds and the percentage of correct responses (Cambridge Cognition, 2012).
The Spatial Span Test from the CANTAB measures working memory capacity. White squares are presented, some of which briefly change color in a variable sequence. The test ends when the subject fails three consecutive trials at any level. The maximum number of boxes correctly defines the final score obtained (Cambridge Cognition, 2012).
Decision making
CGT measures decision-making and risk-taking behavior. A row of 10 boxes appear across the top of the screen, some red and some blue. Rectangles containing the words “red” and “blue” are shown at the bottom of the screen. Participants then have to decide whether a yellow token is hidden in a red box or in a blue box. They are given a set of points with which to gamble, and these points are displayed on the screen in rising or falling order. Participants are allowed to place any bet they choose with the number of points they have, thus gambling on their confidence about their decision about where the token is hidden. The participants are told to earn as many points as possible (Cambridge Cognition, 2012).
Data analysis
After confirming the normality of the data, t tests were performed with Levene’s test for equality of variances to measure any differences in sociodemographic characteristics, health, addiction, or criminal history between the two groups.
Next, t tests were employed to measure any differences in working memory, attention, and decision making between the two groups. One-way ANCOVAs were performed with “group” as the between-subject factor and TBI, due to their importance in cognitive performance, as covariate. Greenhouse–Geisser corrections for degrees of freedom were applied where appropriate. For significant results, partial eta-squared (
Previous studies have suggested that basic cognitive processes (i.e., attention, speed processing, and memory) support higher order cognitive processes such as decision making (Dekkers et al., 2016; Mowinckel et al., 2015), but there is a lack of scientific literature analyzing the relationships between these variables in IPV perpetrators. Moreover, stepwise regressions were conducted to assess which specific neuropsychological assessment variables were predictive of each specific decision-making subscale within each group, the IPV perpetrators and the control group, yielding a total of 12 regression models.
Data analyses were carried out using IBM SPSS Statistics for Windows (version 22.0). The threshold for statistical significance was set at p values ≤.05. Average values are reported in the tables as mean ± SD.
Results
Descriptive characteristics and sociodemographic variables for IPV and controls are presented in Table 1. Results for the two groups were similar on all the anthropometric and sociodemographic variables.
Characteristics of the Sample.
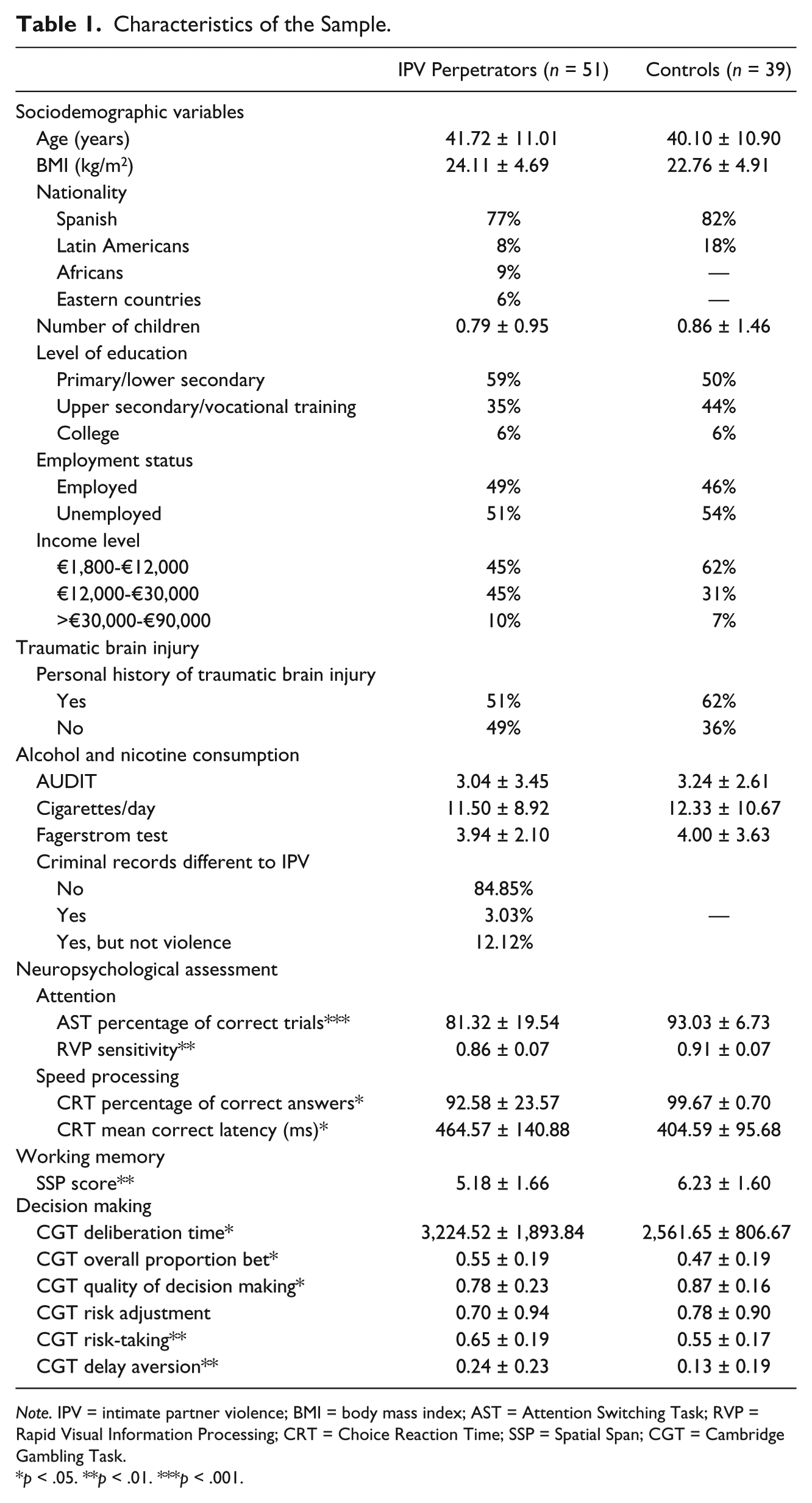
Note. IPV = intimate partner violence; BMI = body mass index; AST = Attention Switching Task; RVP = Rapid Visual Information Processing; CRT = Choice Reaction Time; SSP = Spatial Span; CGT = Cambridge Gambling Task.
p < .05. **p < .01. ***p < .001.
Attention
AST performance differed significantly between IPV perpetrators and controls on the AST percentage of correct trials or the proportion of successful stops, t(64.66) = −3.98, p = .001, d = .85, with IPV perpetrators presenting less accuracy than controls. After including TBI as covariate, differences between groups were still significant, F(1, 89) = 12.33, p = .001,
A main effect of group was found for RVP sensitivity, t(88) = −3.05, p = .003, d = .65, with IPV perpetrators presenting lower sensitivity than controls. We included TBI as covariate, and the differences between the groups remained significant, F(1, 89) = 8.15, p = .005,
Significant between-group differences were observed in the CRT percentage of correct answers, t(86.91) = −2.40, p = .018, d = .52, and mean correct latency (ms), t(50.11) = −2.14, p = .037, d = .61, with IPV perpetrators presenting a lower percentage of correct answers and slower stop signal reaction times than controls. Then, TBI was included as covariate, but group differences remained significant for the percentage of correct answers and mean correct latency (ms), F(1, 89) = 8.14, p = .007,
Working memory
With regard to the SSP, a significant group effect was found, t(88) = −3.04, p = .003, d = .65, with IPV perpetrators presenting lower spatial span than controls. After including TBI as covariate, differences between groups were still significant, F(1, 89) = 7.55, p = .008,
Decision making
CGT performance differed significantly between IPV perpetrators and control participants on the following outcomes: deliberation time, t(88) = 2.25, p = .044, d = 0.48; overall proportion bet, t(88) = 2.04, p = .044, d = 0.43; quality of decision making, t(88) = −2.07, p = .041, d = 0.44; risk-taking, t(88) = 2.52, p = .013, d = 0.54; and delay aversion, t(88) = 2.44, p = .017, d = 0.52. The IPV perpetrators displayed worse decision making, tended to take more time to react, and had a higher mean proportion of points bet across all the trials. The size of their bets was determined more by their presentation sequence than by deliberation, and they took greater risks than controls, regardless of the probability of a favorable outcome. However, there were no significant group differences in risk adjustment, t(88) = 1.09, p = .275. Afterward, TBI was included as covariate, but group differences remained significant for deliberation time, F(1, 89) = 3.32, p = .027,
The calculated Type II error ranged from 1% to 17% in all the analyses.
Predictors of decision making in IPV perpetrators
Prediction models of the attention and working memory scores for each score on the decision-making test can be seen in Table 2. In general, poor attention and processing speed (AST, RVP, and CRT) and working memory performance (SSP) predicted worse scores on several of the decision-making performance subscales in both groups, although predictions were higher in IPV perpetrators than in the control group.
Stepwise Regression Models: Decision-Making Performance Measures Regressed on Neuropsychological Assessment Variables Among IPV Perpetrators and Control Participants Separately.

Note. IPV = intimate partner violence; CGT = Cambridge Gambling Task; RVP = Rapid Visual Information Processing; SSP = Spatial Span; CRT = Choice Reaction Time; AST = Attention Switching Task.
Finally, the analyses were repeated with TBI as covariate, and the models were still significant for IPV perpetrators and controls (p < .05, for all).
Discussion
In the present study, we compared the performance of IPV perpetrators and non-violent controls matched on demographic variables on specific cognitive processes, such as attention, working memory, and decision making, using a computerized battery of tests. The results obtained in this study indicated that IPV perpetrators have worse scores than controls on measures of switching (changing their attentional focus from one stimulus to another) and sustained attention (maintaining attentional focus on a specific stimulus for a prolonged time), processing speed (or the time an individual spends doing a mental task), working memory (a group of cognitive processes that allow the person to mentally retain information for later processing), spatial span (working memory specifically for processing visuospatial information), and decision making (group of cognitive processes that allow us to select/make a final choice among multiple alternatives), supporting Hypothesis 1. We also found that impaired attention and working memory functioning in IPV perpetrators was associated with worse decision making.
IPV perpetrators showed substantially larger switching costs (i.e., spending more time), greater difficulties in sustaining attention (i.e., maintaining attention over time on this specific task), and less ability to inhibit inappropriate responses than controls. Moreover, they tended to respond slowly (present longer reaction times on the CRT test) than controls, but in an inaccurate way, which suggests that IPV perpetrators may be specifically impaired in the ability to actively maintain and select task sets, and they may have a slow processing speed. In fact, these inattention deficits could compromise the ability to change perspectives or set-shift and the ability to accurately interpret facial expressions with emotions, as previously reported in several neuropsychological studies with IPV perpetrators (Romero-Martínez, Lila, Catalá-Miñana, et al., 2013; Romero-Martínez, Lila, Martínez, et al., 2016; Romero-Martínez, Lila, & Moya-Albiol, 2016; Romero-Martínez, Lila, Sariñana-González, et al., 2013; Romero-Martínez & Moya-Albiol, 2013). Thus, this inattention profile of IPV perpetrators or other violent males could explain their increased difficulties in contemplating different alternatives to address problems or switching from inadequate to more suitable behaviors (Meijers et al., 2015; White & Shah, 2006).
Although attention and working memory have been considered separate cognitive concepts, several studies have demonstrated that attention plays an important role in the maintenance and manipulation of working memory (Engle, Kane, & Tuholski, 1999; Kane, Bleckley, Conway, & Engle, 2001). However, another explanation is that working memory can conversely influence visual attention. Despite these apparently contradictory hypotheses, it can be concluded that there is an intimate linkage or even certain overlapping between attention and working memory (Chen, Ye, Xie, Xia, & Mo, 2017). Our data support the link between these cognitive domains due to the fact that IPV perpetrators presented both attention and working memory impairments. These processes are necessary for maintaining motivation and goal-directedness throughout complex tasks, enabling concentration on relevant (and not irrelevant) stimuli and inhibiting stereotypical and automatic thinking. Hence, it seems logical to think that attention and working memory impairments constrain the ability to learn, remember, and adaptively utilize associations, reasoning, and problem solving, which may lead to ignoring possibly advantageous choices without avoiding unnecessary risks in decision-making situations (Afonso et al., 2012; Satpute, Badre, & Ochsner, 2012; Verschure, Pennartz, & Pezzulo, 2014).
According to our results, IPV perpetrators’ decisions were characterized by taking more time to make a decision, displaying more points bet across all trials, bet sizes determined more by their presentation sequence than by deliberation, and greater risk-taking, regardless of the probability of a favorable outcome, compared with controls. It seems that this preference for disadvantageous decisions could be partially explained by diminished attention, processing speed, and working memory abilities. Although the pattern of predictions was similar for both groups, there was a clear relationship between these deficits in basic cognitive processes and risky decisions in IPV perpetrators. In this regard, IPV perpetrators presenting low processing speed (CRT) would have to take more time to make a choice on the CGT. Moreover, a low ability to process visual information (SSP performance) would constrain their ability to make good choices (CGT overall proportion bet). Finally, IPV participants’ difficulties in switching their attention (AST) between different stimuli would diminish the quality of their decisions (CGT quality of decision making) and entail acceptance of greater risk (CGT risk-taking). Nevertheless, due to the fact that different neuropsychological factors predict different decision-making variables, replication studies should be carried out to determine whether the pattern of results would be the same in future studies, especially in studies with larger sample sizes where more potential sources of spuriousness could be controlled in the regressions.
According to previous results, future studies could analyze whether specific neuropsychological training in attention-switching and working memory could lead to improvements in decision-making processes or other EFs. Indeed, previous studies suggested that the attention-switching ability can be improved in several populations, such as individuals with ADHD or older adults, and applied to solving different and new problems/tasks that were not practiced during cognitive training (Dowsett & Livesey, 2000; Kramer, Hahn, & Gopher, 1999; Kray & Lindenberger, 2000; White & Shah, 2006). Moreover, it would be interesting to study whether these improvements lead to higher treatment adherence, thus reducing the risk of IPV recidivism.
This is the first study to examine how specific cognitive impairments would affect decision making in IPV perpetrators. Moreover, we strengthen our findings with computerized neuropsychological tests, which do not present the limitations of psychological assessments often biased by social desirability. On the contrary, the main limitation of this study is the limited sample size, thus diminishing the representativeness and generalization of the results, which would have helped to confirm the observed results. Furthermore, IPV decision making was only assessed by a neuropsychological test, instead of considering other kinds of real decisions. Moreover, our study is based on a clinical sample, and so we should be cautious about generalizing our results to the general population. Furthermore, it is possible that the selected group of IPV perpetrators who present a pattern of cognitive deficits are more likely to be detected and sent for treatment, whereas IPV perpetrators without these impairments may be more likely to evade the system. Finally, performance on several neuropsychological tests, especially in the control group, presented a lower standard deviation compared with IPV perpetrators. Hence, it makes sense to imagine that the neuropsychological deficits of the group of IPV perpetrators would explain the prediction pattern between variables. Therefore, this fact should be considered a bias in our study. Thus, future studies will benefit from larger and more structured assessments of different cognitive domains with a neuropsychological battery, as well as analyzing all the variables in controls with and without a history of violence (i.e., employing the general population, other clinical samples, etc.). In addition, it would be interesting to study whether these cognitive domains remain stable after different IPV perpetrator intervention modalities or programs.
In conclusion, this study shows that specific cognitive deficits in IPV perpetrators could constrain their decisions. In fact, their risky decisions (e.g., risky sexual behaviors, drug misuse, pathological gambling, etc.) would be partially explained by impaired cognitive processing. Moreover, our study indicated that specific neuropsychological training in attention-switching and working memory could lead to improvements in decision-making processes or other EFs. Finally, our study has enabled us to explore cognitive deficits that might be key factors in reducing the risk of IPV risky decisions and/or recidivism.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project supported by a 2018 Leonardo Grant for Researchers and Cultural Creators, BBVA Foundation. The Foundation accepts no responsibility for the opinions, statements and contents included in the project and/or the results thereof, which are entirely the responsibility of the authors.