
Abstract
The objective of this study is to assess the effects that a specific type of severe violence—violence with femicide risk (VFR)—has on women’s physical and mental health, as well as the physical health of their children. I focus on Peru, a country in which 7 out of 10 women have been victims of some form of intimate partner violence. In Latin America, Peru is one of the countries with the highest rates of violence against women. Methodological gaps in the existing literature (sampling size, selection bias, and reverse causality) are covered using an important nationally representative sample (Demographic and Health Survey: N = 84,136) and the use of propensity score matching. Results show that VFR increases symptoms of depression, as well as alcohol and tobacco consumption. The children of victims of VFR had significantly more recent episodes of bloody stool, diarrhea, fever, and coughing. These effects are heterogeneous. They vary based on violence characteristics (history of sexual violence) and on victims’ socioeconomic status. According to the relevant literature, these effects can be understood to stem from somatization, stress, substance use (as a facilitator of violence), and neurological damage due to exposure to this type of violence. Results suggest VFR may have life-course altering effects given victims’ distinct coping strategies.
Introduction
The effects of intimate partner violence are broad. It causes the obvious physical harm arising from the aggression itself, along with increasing negative perceptions regarding quality of life of women (Beeble, Bybee, Sullivan, & Adams, 2009) and their children’s health (Riger, Raja, & Camacho, 2002; Wolfe, Crooks, Lee, McIntyre-Smith, & Jaffe, 2003). However, gaps still exist in this literature.
This article will examine how a specific type of severe violence—which I call violence with femicide risk (VFR)—affects the physical and psychological health of the victim and her children using methodological nuance. This study focuses on Peru, a country with an alarmingly high prevalence of violence against women.
The majority of the literature that has examined the impact of violence has failed to address certain methodological limitations and has examined either nonnationally representative populations or concentrated on Anglo Saxon countries, leaving cultural variation unexplained (especially in Latin America or Africa where inequalities and male domination have a larger presence). Moreover, the existence of mixed results regarding the effects of violence may be due, in part, to the homogenization of aggression types into one category. Rather, the effects of violence are heterogeneous. They vary in function of their severity (Dutton et al., 2006; Eberhard-Gran, Schei, & Eskild, 2007), the way in which violence was exerted (sexual violence), and certain characteristics of the women themselves (socioeconomic status).
To address these limitations, I use propensity score matching in a large sample to deal with selection bias and reverse causality in assessing VFR’s effects. Moreover, these results are discussed in terms of heterogeneous effects, as well as broken down by characteristics of the type of violence (sexual violence), and certain victim characteristics (socioeconomic status).
In Peru, 68% of women have been victims of any type of violence, which places the country at the top of international rates of comparable intimate partner violence; this coincides with Abramsky et al. (2011), who find rates of violence against women between 15% and 71% in 10 countries. VFR consists of aggressions that are similar to that of femicide (strangulation, burning attempts, using, or threat of using weapons), which includes 1.98% of victims in our sample (Peruvian Demographic and Health Survey [DHS]). Even if only a minor proportion of women are victims of VFR in Peru, its effects on women and their children represent a call for making this particular violence more visible and for creating more effective public policies for its prevention.
In Peru, violence against women is still assumed to be a normal phenomenon by a large part of the male population. Although 85% of men surveyed think that those who batter their female partner are mentally ill, almost half state that they would hit their partner, given a reason (46%), if she were guilty of something (34%), or if they were to lose control (57%; Vara-Horna, López, & Odar, 2017). This justification of the use of violence against Peruvian women has also been found to predict their femicide (Hernández, Raguz, Morales, & Burga, 2017).
Literature Review
Effects on Women’s Physical and Mental Health
Physical and mental health are related to a wide spectrum of conditions, ailments, and diseases, which are difficult to assess comprehensively. Research has proven that intimate partner violence is frequently associated with issues concerning both health consequences. However, data limitations constrain the possibility of exploring new areas where intimate partner violence may present negative outcomes. The most common effects of intimate partner violence on mental health are symptoms of depression (Dutton et al., 2006; Sarkar, 2008) and posttraumatic stress disorder (Bonomi et al., 2006; J. C. Campbell, 2002; Vos et al., 2006). This form of violence is related to previous and future depressive episodes (Beeble et al., 2009), and can triple the risk of depression (Devries et al., 2013) and even increase it eightfold (Golding, 1999).
Research on intimate partner effects has identified a long list of physical effects. Compared with women who have never experienced physical violence, those who have are more likely to suffer from headaches, backaches, digestive problems, loss of appetite, abdominal pain, constipation, diarrhea, and even, to a lower degree, sexual reproductive health problems such as vaginal infections, sexually transmitted infections and diseases, vaginal bleeding, pain during intercourse, pelvic pain, and urinary tract infections (J. Campbell et al., 2002; Coker, Smith, Bethea, King, & McKeown, 2000). A multinational study found that women who experienced violence were more likely to state that, in the past 4 weeks, they had problems walking and doing daily activities, as well as suffering from pain, memory loss, dizziness, anxiety, and vaginal discharge (Ellsberg, Jansen, Heise, Watts, & García-Moreno, 2008).
The use of alcohol and tobacco have negative consequences for one’s health, and have also been found to be related to intimate partner violence. Violence against women has been found to be associated with increases in the consumption of alcohol and tobacco (Vos et al., 2006). Alcohol consumption is also linked to depression (Pietraszek et al., 1991). Qualitative evidence suggests that battered women consume alcohol to numb their emotions (Riger et al., 2002), a strategy that reduces their chances of leaving the relationship. Problematic alcohol consumption can increase the risk of health problems and even exacerbate violence (Ellsberg et al., 2008). Few studies have examined the effect of violence on the consumption of tobacco. Rodriguez et al. (2008) found that in the months before pregnancy, Latina women exposed to intimate partner violence smoked more than nonvictims as an escape strategy. Although these effects seem to be consequences of intimate partner violence, the relationship between violence and alcohol may also be comorbid (Grant & Harford, 1995).
Effects of intimate partner violence on women vary based on the severity of these violent acts. As more aggressive men inflict more serious physical damage (Holtzworth-Munroe, Meehan, Herron, Rehman, & Stuart, 2000), we should expect that victims of VFR suffer more severe consequences from this type of violence. Severe violence exacerbates the mental and health effects of intimate partner violence (Carbone-López, Kruttschnitt, & Macmillan, 2006); yet, these effects have only been found to intensify depression when the violence is sexual and/or severe in nature (Bennice, Resisck, Mechanic, & Astin, 2003; Sarkar, 2008).
These differences in the manifestations of the consequences of violence represent an important call to move beyond examining average population effects. Efforts must be made to identify pockets of women who are subject to more extreme consequences due to the severity and frequency of violence in their relationships. There is solid evidence that argues that some effects of intimate partner violence (the majority of which have not been referenced here; see J. C. Campbell, 2002; Coker et al., 2000) act as multipliers of collateral effects that appear specifically when violence is sexual or severe in nature (Bennice et al., 2003; Sarkar, 2008). However, prior studies have been limited in their ability to discover additional patterns given the nature of available data. The purpose of this study is to highlight the effects of a more severe type of violence on a woman and her children. In doing so, the hope of this article is to aid in improving policies of early detection of victims who may be at risk of death, as well as policies designed to reduce the effects of this particular type of VFR.
Effects on Children
Both qualitatively (Riger et al., 2002) and quantitatively (Wolfe et al., 2003), studies demonstrate that intimate partner violence affects children socially, emotionally, behaviorally, and cognitively.
The process by which children are affected is via somatization and stress (Arroyo, Lundahl, Butters, Vanderloo, & Wood, 2017). Children of abused women have higher scores of internalizing (anxiety, depression, withdrawal, and somatic complaints) and externalizing behavioral problems (aggressive behavior and rule-breaking actions) than children whose mothers were not abused (McFarlane, Groff, O’Brien, & Watson, 2003). These consequences on children may not necessarily manifest as serious illness. These effects may manifest as less serious physical health issues, and chronic or symptomatic conditions. For example, Ribero and Sánchez (2004) found that, in the Colombian context, there is a higher number of respiratory diseases, fever, and severe diarrhea in children whose mothers suffer from intimate partner violence. These same authors find that the children of victims of intimate partner violence are 19% more likely to be anemic and suffer from growth delays. Effects, such as somatization or stress, resulting from domestic violence may affect children who are not direct objects of abuse due to possible deterioration of the maternal relationship with the child, reflecting a decline in the mother’s concern and ability to identify her child’s interests and needs (Boeckel, Wagner, & Grassi-Oliveira, 2017).
But somatization as an impact mechanism may not be a conclusive finding. A study on a small sample of women (N = 80) and their children between 7 and 11 years old found that the mother’s experience of physical and emotional abuse did not affect scores on the parenting stress index (Sullivan, Nguyen, Allen, & Bybee, 2000). Rather, this same study found that abuse affected children’s behavior via increased aggression and withdrawal tactics. However, this study may have underestimated the effects of more severe forms of violence and the prevalence of posttraumatic stress disorder and depression in battered women (Bonomi et al., 2006; J. C. Campbell, 2002; Vos et al., 2006). It seems that generalized stress, and not that related to parenting, explains how the effects of violence are multiplied in children. Karamagi, Tumwine, Tylleskar, and Heggenhougen (2007) find that several symptoms in children, such as fever, diarrhea, cough, and rapid breathing, appear 2 weeks before the mother experiences violence, probably due to the increase in the number and perception of tense episodes. The authors also find evidence regarding the persistence of these symptoms throughout infancy in children whose mothers suffer from domestic violence.
Among the broad, and yet insufficiently explored, effects of intimate partner violence on children, special attention must be given to a less visible subject in this literature: temporary ailments seemingly unrelated to violence (e.g., bloody stools, diarrhea, fever, and coughing) in young children who have developed fewer coping mechanisms. These consequences not only directly affect the well-being of children and increase household health care spending but also the children may receive ineffective treatment when the underlying problem of violence fails to be addressed.
Heterogeneous Effects in the Literature
Violence does not have a homogeneous effect on all women, especially if it is severe (as is the case with VFR). According to related studies, effects vary not only based on the types of violence (severity and sexual violence) but also given certain characteristics of the woman herself (socioeconomic status). Severity shapes the effects of violence on women and their children (Dutton et al., 2006). The degree of the consequences of violence is also associated with severity, especially concerning depression, posttraumatic stress disorder (Pico-Alfonso, 2005), and the number of symptoms and illness experienced (Eberhard-Gran et al., 2007).
Sexual violence generates different effects from those of physical violence, although both forms also seem to interact. According to Golding’s research, rapes commonly lead to excessive menstrual bleeding, vaginal burning, pain during sexual intercourse, absence of sexual desire, and so forth (J. C. Campbell, 2002; Golding, 1999). Plitcha and Falik (2001) find that, compared with other types of violence, sexual violence is more highly associated with symptoms of depression and anxiety in the past 5 years.
Socioeconomic status also produces variation in the effects of violence. Violence against women may affect poor women differently than their wealthy counterparts. Violence has an even higher negative effect on health than poverty or their interaction (Janssen et al., 2003). Belonging to an ethnic minority (African American and Hispanic compared with Whites in the United States) is also associated with higher rates of intimate partner violence (Field & Caetano, 2004). The latter should not be used to relativize the particular effects of social and cultural contexts. Golding (1996) notes, for example, that the effects of sexual violence are more pronounced in women of African and Latin American origin, an effect that is related to cultural differences in the way that sexual violence is perceived.
The effects of violence are heterogeneous across several variables. Therefore, in this study, I explore the heterogeneous effects of VFR across two categories: sexual violence history and socioeconomic status, rather than treating all victims the same. This is especially important due to the implications these characteristics have for the development of public policy and treatment.
Methodological Problems
Although evidence that intimate partner violence has negative effects on women and their children is overwhelming, unresolved methodological issues in this literature persist and relate to three aspects: sampling issues, selection bias, and reverse causality. The majority of these studies have several sampling problems, including small sample size, intentional sampling, and nonrepresentative samples. But selection bias is a much more important problem and few efforts have been deployed to properly address it. Some studies collect information where there is a higher probability (and bias) of finding victims: safe-houses or domestic violence shelters (Bennice et al., 2003; Boeckel et al., 2017; Pico-Alfonso, 2005) and primary health care services (J. Campbell et al., 2002; Coker et al., 2000). Others build their samples based on techniques that can increase nonresponse and systematic bias, such as dialing surveys (Carbone-López et al., 2006) and newspaper advertising (Graham-Bermann & Perkins, 2010; Sutherland, Sullivan, & Bybee, 2001).
There are three strategies that can be used to address selection bias. First, population-based studies seem to be the best way to deal with these problems as they use larger, representative, and random samples. However, due to inferential and sampling characteristics, they have a hard time getting at groups in the tails of the distribution, where violence is more severe and has more serious effects (Kelly & Johnson, 2008). A second viable solution is that of controlling for confounding variables. Most studies rely on controls via the use of sociodemographic variables (Ellsberg et al., 2008; Pico-Alfonso, 2005), regardless of the risk of obtaining spurious or inflated relationships, or identifying how the use of these controls affects the obtained outcomes. Just a few studies control for potential key confounding factors (stress; alcohol, cigarette, and drug consumption; previous instances of violence; etc.; Devries et al., 2013). A third way to deal with selection bias is through the use of proper statistical methods, such as propensity score matching, instrumental variables, or control groups. Surprisingly, seldom do studies use this third strategy (Boeckel et al., 2017; J. Campbell et al., 2002; Pico-Alfonso, 2005; Sarkar, 2008).
A final unresolved methodological issue present in this literature is that of reverse causality. Women exposed to physical or sexual violence are not only more likely to exhibit somatic symptoms but also more likely to report them (Eberhard-Gran et al., 2007). However, there is no agreement on whether the (long list of) effects of violence are due to other conditions that share the same risk factors and consequences of intimate partner violence—such as poverty (Goodman, Smyth, Borges, & Singer, 2009).
The present study attempts to overcome these methodological issues through the use of a large national representative sample, propensity score matching, and different matching algorithms to obtain robust results.
Method
Data
Data from the 2010 to 2015 DHS for Peru is used. The large sample size (N = 84,136) reduces—but does not eliminate—the probability of excluding more severe types of violence. This nationally representative sample on urban and rural areas collects information about a woman (between the ages 15 and 49) and her children. She is randomly selected at the household level to answer questions regarding intimate partner violence (pertaining to the current or most recent partner). Intimate partner physical violence rates in urban and rural areas in Peru are similar (29% and 33%, respectively, according to the Peruvian DHS), despite the stronger presence of sexist culture and traditional gender roles in rural areas. Race and ethnicity in Peru are quite complex concepts, and are usually measured by a respondent’s mother tongue. Using this approach, only 9% of women in the sample did not have Spanish as their mother tongue, and, therefore, could be considered indigenous. However, due to widespread and historic racial mixing in the country (Contreras, Gruber, & Mazzeo, 2012), the operationalization of ethnicity and/or race into fixed categories is problematic. Self-identification questions have been used to attempt to measure these categories (“would you say you are . . . White, Indigenous, Black”), and their results call into question the utility of using questions regarding mother tongue (Valdivia, 2011). As the available data rely exclusively on questions regarding language as proxies for race/ethnicity, this study is unable to robustly examine the effects of race/ethnicity on VFR, something that should be addressed in future studies.
The survey is in response to a U.S. Agency for International Development (USAID) international initiative, which took place in several Latin American, African, and Asian countries. The questions in the violence module are a modified and shorter version of the Conflict Tactics Scale, which has important cross-cultural reliability (M. A. Straus, 2004). As well as in other countries, the Peruvian DHS measures psychological (nine items), physical (seven items), and sexual violence (two items), and presents an acceptable internal consistency (Cronbach’s α = .80, .78, .72, respectively). Quality standards for fieldwork were implemented in all countries; in Peru, protocol guarantees respondent protection and minimizes nonresponse. The violence module is asked at the end of the survey and only if privacy conditions are adequate (no nearby relatives, including the partner). This has led to a low noncompletion rate, in which only 2.6% of surveys were interrupted or could not be finished.
Building the VFR Variable
The interest of this research lies in identifying the effect of a particular type of violence, VFR. The use of this type of violence involves a higher risk of mortality, and is more likely to have serious consequences for the victim and her children.
A woman is classified as a victim of VFR if (a) she was the victim of attempted strangulation or burning; (b) she was attacked with a knife, gun, or other weapon; or (c) she was threatened with a knife, gun, or other weapon.
The choice of these variables in building the concept of VFR is based on the literature regarding how femicides are committed (the parts of the body attacked), investigated, and measured. It follows from the literature on the forms and predictors of femicide (Beyer, Wallis, & Hamberger, 2015; J. C. Campbell, Glass, Sharps, Laughon, & Bloom, 2007; Glass, Laughon, Rutto, Bevacqua, & Campbell, 2008; Mouzos, 1999), as well as the Latin American Model Protocol for the investigation of gender-related killings of women (femicide/feminicide; UN Women, 2015). More important, the variables used to build VFR represent the more severe forms of intimate partner violence under the Conflict Tactics Scale (M. Straus, Hamby, Boney-McCoy, & Sugarman, 1996). The theoretical and methodological development of this variable is coherent, given the three variables tend to load on the same factor (Calvete, Corral, & Estévez, 2007; Cascardi, Avery-Leaf, O’Leary, & Smith Slep, 1999), have correlated errors (Newton, Connelly, & Landsverk, 2001), and cluster nearby in common item characteristic curves (Reichenheim, Klein, & Moraes, 2007; Schafer, 1996).
Femicide is a (statistically) rare phenomenon in Peru. This is consistent with global intimate partner femicide rates, as only a small proportion of women are victims of this type of violence (Stöckl et al., 2013). Just a minor group (1.98%) of women were victims of VFR in our data. As seen in Table 1, on average, victims of VFR are 35.7 years old, and 4 years younger than their partner. Low education levels are extensive (32% completed only primary studies), most cohabitate (53%) instead of being married (35%). Few of these women smoke (4.1%) and a minor proportion had a father who abused the victim’s mother (7.9%). As expected, VFR is more common among victims of severe violence (11.7%). These women are a little older (37.9) and less educated than nonvictims (and the same relationship is true of their parents). There is no major difference in marital status and smoking habits. VFR is also present in victims of sexual violence. Finally, VFR is more than twice as common in low socioeconomic status households (2.4%) than in high socioeconomic status households (1.1%). All variables tend to be more negative among low socioeconomic status victims, though a few differences exist in the percentage of women who are employed. More interparental violence was reported in women of higher socioeconomic status.
Descriptive Statistics on Prevalence on VFR.
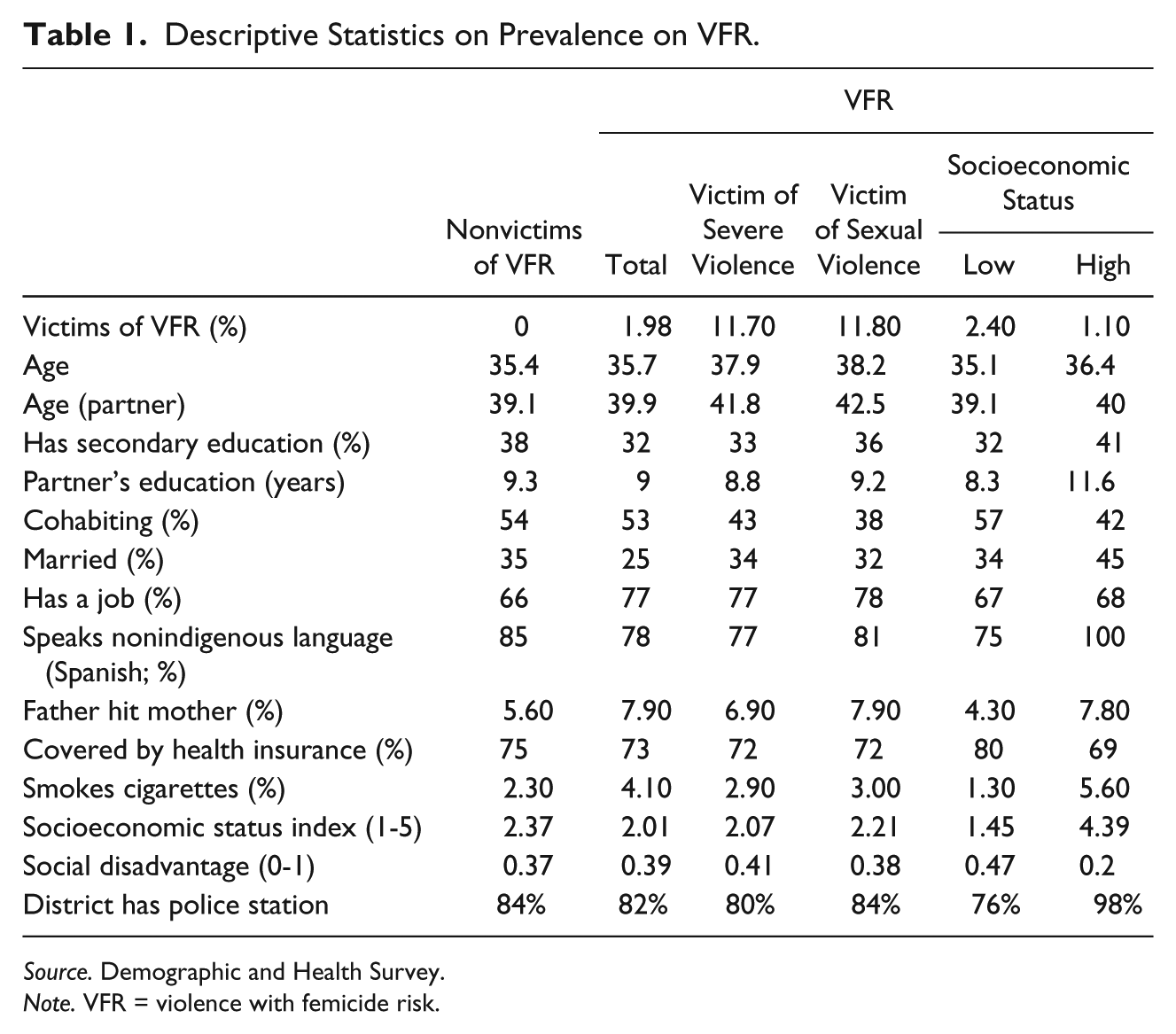
Source. Demographic and Health Survey.
Note. VFR = violence with femicide risk.
Outcome Variables
The DHS provides an important sample of victims, but at the same time, it only collects a limited number of questions on mental and physical health. Operationalizing these variables is hence constrained by the available questions in the survey. The mental health of the women is examined with a nine-item depression scale (Patient Health Questionnaire). Women are asked about the scale while thinking of two points in time: the past 14 days (recent depression) and the last 12 months (past year depression). The scale has satisfactory internal consistency (Cronbach’s α = .87). Physical health could only be assessed in this sample through questions regarding alcohol and tobacco use, using different indicators of frequency of consumption. Children’s physical health was measured via indicators of illnesses that are unrelated to nonserious diseases (ailments): recent diarrhea, bloody stool, fever, and cough over the past 2 weeks. These questions are only presented to mothers of children below 4 years old.
Analytical Strategy
This study attempts to answer the following question.
Obviously, this question is impossible to answer. Because the woman was already a victim of violence, it is infeasible to examine the counterfactual. But, in methodological terms, it is possible to recreate it. This is the strength of the contribution of this study. To create and measure the counterfactual, I use propensity score matching. Each woman who was exposed to VFR was compared with her counterfactual, or control group (a woman who had not experienced this type of violence), when both women shared an equal likelihood of this potential victimization. The principal advantage of this technique is the capacity to control for selection bias through the use of observed variables and, in doing so, attempt to approximate causal relationships.
The construction of the control group is key, and is formed through the determination of the likelihood of being a victim of VFR among those who were not victims: Pr(X) = Pr(T = 0|X). This method matches women who experience VFR with those from the control group. This matching is based on the Pr(X). Once matched, the difference between the outcome variable (Y) between the group of women with and without violence represents the average effect of VFR.

The propensity score was estimated using a logit model, based on a group of observable variables at the individual level (X: age, marital status, ethnicity, education, justification of the physical punishment of children, partner alcohol consumption, parental history of intimate partner violence, justification of violence, partner respect for the woman’s wishes and desires, as well as her rights, and a socioeconomic status index). Two variables were also included to measure the characteristics of each woman’s district. An indicator of social disadvantage was used to identify the sociostructural effects that could have an impact on violence (Sampson, Morenoff, & Gannon-Rowley, 2002) as well as a variable to measure the presence of police stations in the district. These variables account for potentially dissuasive institutional resources in the estimation of the probability of violence against women (Miller & Segal, 2014).
The propensity score has an important function of balancing the observable characteristics of the treatment group with those of the control group. To do so, two conditions must be met (Ho, Imai, King, & Stuart, 2007). First, the distributions of the propensity scores between the groups with and without VFR must overlap (as seen in the appendix, this condition was satisfactorily achieved). This controls for heterogeneity in the sample and ensures an adequate number of treated and control observations across the distribution of the propensity scores. Second, the ignorable treatment condition is necessary as it implies that without VFR, the resulting variables would be constant across the two groups. The matching techniques used were nearest neighbors (with replacement) and Kernel matching (among nearest neighbors). Both techniques are strengthened by the large sample used, which allows for robust effects.
To summarize, the combination of the use of variables linked to the antecedents of violence and district variables, along with the advantage of propensity score matching, bring us closer to finding causal effects than traditional methods. At the same time, it allows for a strong reduction in the possibility of spurious correlations. Although the method used offers more than purely correlational results, given the cross-sectional nature of the data, the results cannot be interpreted as causal.
Results
Effects on Depression
As expected in the literature, VFR affects symptoms of depression (Table 2). Recent depression increases between 16 and 22 percentage points (using nearest neighbor and Kernel matching, respectively) compared with the control group. In the case of the former matching method, each item in the depression index increased. The robustness of these results is important. When using Kernel matching, only one item in the scale did not vary significantly.
Impact of Violence With Femicide Risk on Women’s Mental and Physical Health and Children’s Physical Health.
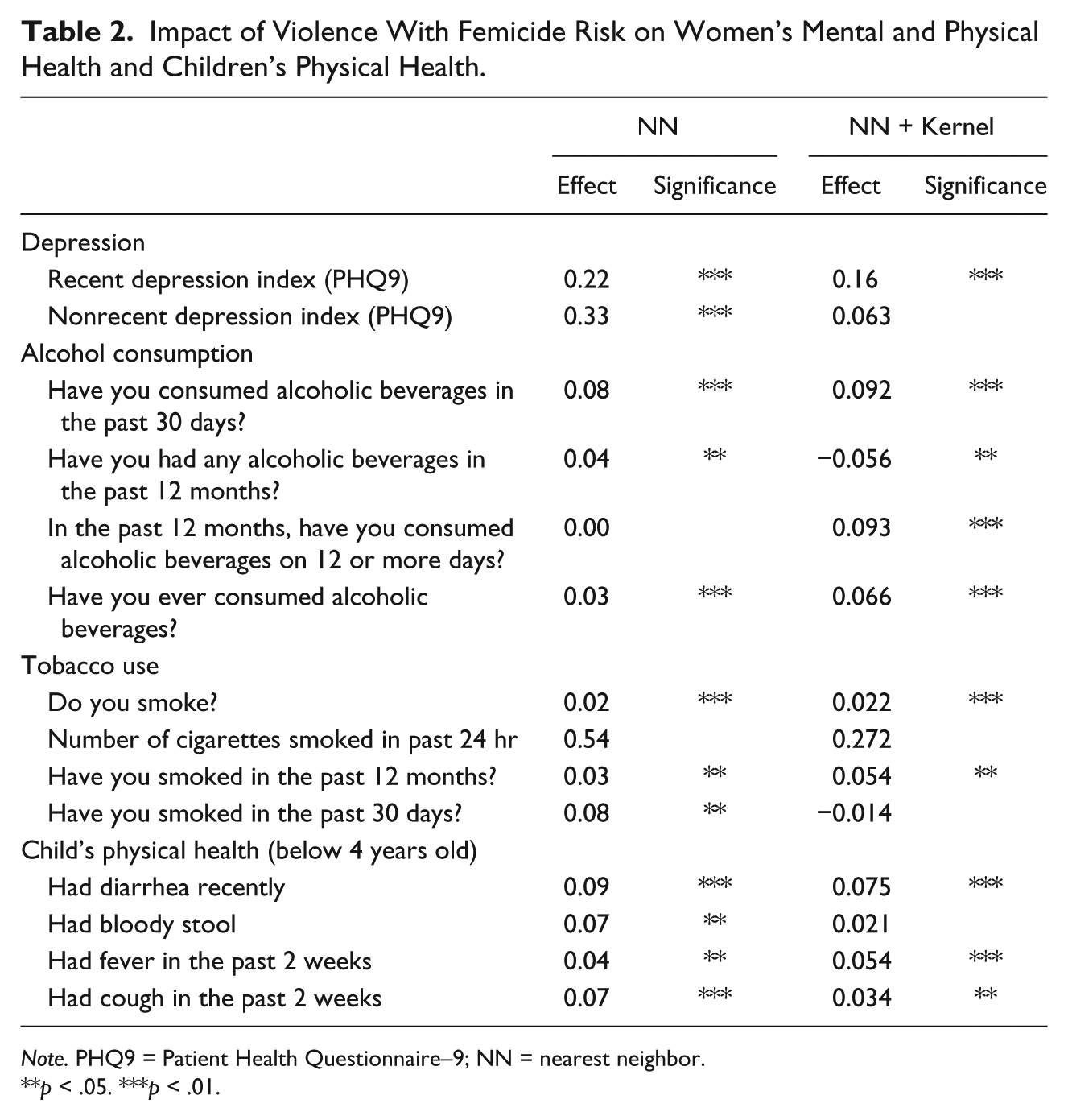
Note. PHQ9 = Patient Health Questionnaire–9; NN = nearest neighbor.
p < .05. ***p < .01.
The impact is less consistent with regard to depression in the past 12 months. Using the nearest neighbor matching method, not only was the average index score affected but so were each of the items. However, the same phenomenon did not take place with the Kernel matching estimates (only two items were significant: feeling down, depressed, or hopeless; and poor appetite or overeating).
Effects on Alcohol and Tobacco Consumption
Different indicators of the frequency of alcohol and tobacco consumption were used, as their effects are most significant when taken together (Table 2). The majority of alcohol consumption indicators increased, although the magnitude of the effect was not very strong. Both recent (in the past month) alcohol consumption and consumption in the past year increased, as did the indicator for consumption over 12 times in the past year. The effect of VFR on the use of cigarettes is similar to that of alcohol consumption. Almost all the frequency indicators increased, including in the past 24 hr, in the past month, and in the past year. Even more important, having been the victim of VFR increased (albeit slightly) the declared habit of smoking cigarettes.
Effects on Children’s Physical Health
VFR increased all negative health indicators in children (below 4 years old; Table 2). This follows the assumption that the effects of witnessing VFR result in the somatization of these illnesses (Eberhard-Gran et al., 2007). Other evidence regarding the somatization of the effects of intimate partner violence supports this finding (McFarlane et al., 2003; Ribero & Sánchez, 2004), including Wolfe et al.’s (2003) meta-analysis of 41 studies on children’s exposure to domestic violence. Of all the variables examined in this study, the presence of recent diarrhea, fever, and cough in the past 2 weeks was significant (9 percentage points and 6 percentage points, respectively), whereas the presence of bloody stool was only significant with one of the matching algorithms.
Heterogeneous Effects
History of sexual violence
As can be seen in Table 3, the effects of VFR are varied and stronger among women who do not have a history of sexual violence. The effect on recent depression varies between 25.3 and 31.6 percentage points in women who have never been victims of sexual violence. Among those who were, the effect barely reaches 5.1 percentage points. Depression in the past year follows the same pattern, the difference being that in both cases, the impact of VFR is high; it varies around 36 percentage points in women without a history of sexual violence, and 14.7 and 19.5 percentage points among those with such a history.
Impact of Violence With Femicide Risk, by History of Sexual Violence.

Note. Only significant effects are reported. Disaggregated items were not included for ease of reading. PHQ9 = Patient Health Questionnaire–9; NN = nearest neighbor.
p < .05. ***p < .01.
The effect of VFR on the consumption of alcohol and tobacco has clear heterogeneous effects regarding a woman’s history of sexual violence. It affects almost all indicators of tobacco consumption in women who have not been victims of sexual violence, but the effect is only pronounced in one indicator of alcohol consumption. In the latter indicator, however, there is an opposite effect on both groups. Among women who had a history of experiencing sexual violence, VFR increased the consumption of 12 or more alcoholic beverages in the past year (between 8.9 and 12.8 percentage points), whereas among those without this history, consumption declined (−9 percentage points). Tobacco use, however, only had significant effects on the group of women who experienced sexual violence. The impact is both on the number of cigarettes consumed over the past 30 days (approximately two additional cigarettes) and over the past year (around 14 cigarettes more). Also, VFR was found to strongly increase the proportion of women who state that they smoke.
Finally, VFR affected the health of children below 4 years old, both among women who were and were not victims of intimate partner sexual violence at some point in their lives. The impact, however, was higher among the latter. The effect of VFR increased both the presence of recent diarrhea, between 13 and 16 percentage points, and that of fever and cough (over the past 2 weeks) by between 5.2 and 9.4 percentage points. Among women who never experienced sexual violence, VFR only increased the presence of bloody stools among their children (11.8-12.5 percentage points).
Socioeconomic status
Among women at both the upper and lower levels of the socioeconomic status index, VFR has an impact on depression (Table 4). However, whereas the effect on depression in the past year is higher among women with low levels of socioeconomic status (between 32.2 and 42.4 percentage points, compared with 30.5 percentage in those with higher levels), the effect is always higher among those with a high level of socioeconomic status (44 percentage points).
Impact of Violence With Femicide Risk, by Socioeconomic Status.
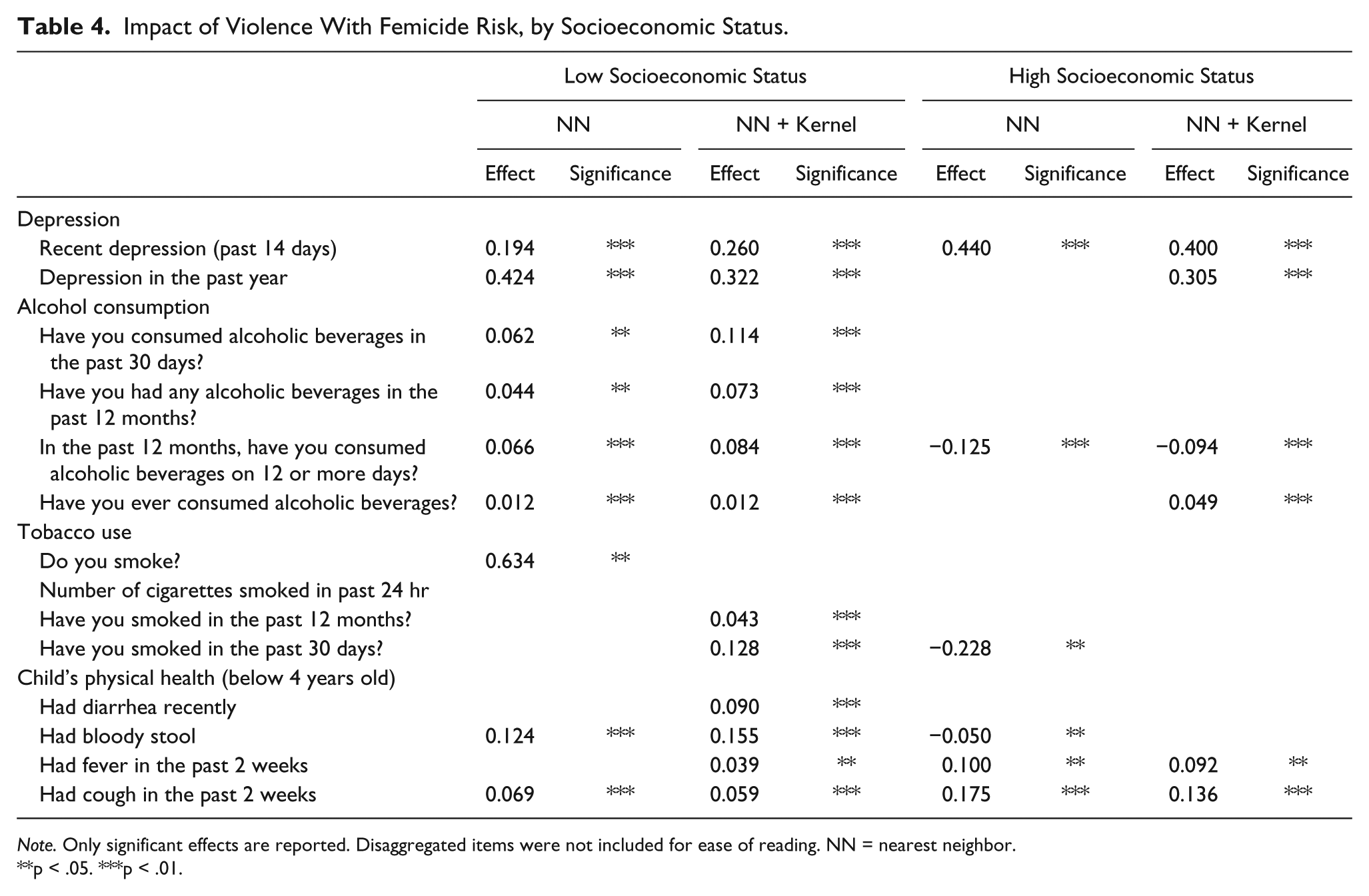
Note. Only significant effects are reported. Disaggregated items were not included for ease of reading. NN = nearest neighbor.
p < .05. ***p < .01.
The strongest effects of VFR on the consumption of alcohol and tobacco are also found among women of low socioeconomic status. This type of violence increased almost all indicators of alcohol consumption (over the past 30 days, in the past year, by quantity and incidence). Conversely, among women with a high level of socioeconomic status, VFR reduced the consumption of alcoholic beverages on 12 or more occasions in the past year (−9.4 percentage points), although it did increase the number who stated to have ever consumed alcohol. Also among women of low levels of socioeconomic status, VFR also increased certain indicators of tobacco use, such as admitting to smoking (63.4 percentage points), smoking over the past year (4.3 percentage points), and having smoked in the past 30 days (12.8 percentage points). Just as with the effect on alcohol, there were few significant indicators of the impact of VFR on smoking in women of high socioeconomic status, whereas some had opposite signs compared with their counterparts.
The effect of VFR affects the health of children (below 4 years old) of women at lower and higher levels of socioeconomic status. In both cases, fever (3.9 percentage points in women of low socioeconomic status and 10 percentage points of high socioeconomic status) and coughing (6 percentage points in women of low socioeconomic status and between 13.6 and 17.5 percentage points of high socioeconomic status) were more likely to be noted in the past 2 weeks. The effect on the presence of bloody stool was only found among the children of women of low socioeconomic status (9 percentage points). Among these women, VFR increased the incidence of bloody stool by 12.4 and 15.5 percentage points, but was reduced in the children of women of high socioeconomic status (−5 percentage points).
Discussion
To quantify the effects of violence against women, this study created a variable that measures a severe form of violence with high risk of death: VFR. The impact of this type of violence on the physical and mental health of women, and the physical health of their children was then examined. The results suggest that VFR has various consequences on these outcome variables.
These results are in line with previous evidence. Effects are robust regarding depression and increased consumption of alcohol and tobacco in women who have been victims of VFR. Children are also affected. Many minor afflictions in children below four were found to be significantly related to VFR. These effects relate to what Sarkar (2008) calls second- and third-order effects of violence, or, in other words, effects on the well-being of the woman herself, and effects on third parties (her children) who are not directly affected by violence.
VFR does not have homogeneous effects across all groups of victims. Rather, the effects of this type of violence varies based on a victim’s history of sexual violence and her socioeconomic status. First, women with history of sexual violence present fewer negative health consequences than those without such a history. Similar effects were found with regard to their children. Future research should examine these counterintuitive results, especially to clarify whether these effects are related to how long ago these episodes of sexual violence occurred (an issue not addressed in this study due to data limitations).
A possible explanation for these unexpected results is victim resilience. According to Anderson, Renner, and Danis (2012), victims of recent and past episodes of intimate partner violence present not only trauma symptoms but also signs of resilience: This may also affect their ability to cope and adjust as survivors of domestic violence. Piispa (2002) states that certain forms of violence are substitutes; victims of intimate partner violence may experience one type of violence more severely, as a compensatory effect. This may suggest that some women who are not victimized sexually may suffer from more severe physical violence. It may also be that previous experience with sexual violence may indicate these women had a greater need to find coping strategies, venting and support networks in the past. The use of formal and/or informal support networks may, in turn, partially mitigate the effects of VFR.
Another possible explanation for these counterintuitive results is that women who experienced sexual violence have internalized this and other violent behavior as a “new state of normal.” Several studies—including multicountry studies (Abramsky et al., 2011) and meta-analysis (Stith, Smith, Penn, Ward, & Tritt, 2004)—have found that victims are more likely to explicitly accept wife beating (Gage, 2005) or opt for silence as a coping strategy (Tankink & Richters, 2007). More research is needed to better understand coping strategies taken by women victims of severe violence on different cultural settings.
Second, there is difference in the effect of VFR across women of high and low socioeconomic status. Past year depression as well as increased consumption of alcohol and tobacco were higher in women of low socioeconomic status, which may be explained by the fact that poorer women have poorer self-esteem and inadequate emotional support (largely stemming from reliance on nonprofessionals; Bassuk, Dawson, & Huntington, 2006). High income women have better access to preventive and mental health services. Increased use of tobacco and alcohol in women of low socioeconomic status may not only be related to their lower access to institutional health networks but also, because these women have poorer coping strategies, greater isolation and weak support networks (friends or family). In other words, when poverty intersects with intimate partner violence, coping strategies are constrained (Goodman et al., 2009). The strong effects in the children of women with high levels of socioeconomic status suggest that their use of better coping strategies may not be effectively channeled toward protecting their children.
Although not examined in this article, ethnicity could also be a source of heterogeneous effects. More research is needed to take into account how gender, cultural, and social differences are associated with the underlying effects of VFR and intimate partner violence in general. Also, the joint increase in alcohol and tobacco use in victims of VFR highlights the need for new studies that explore their life-course interaction as well as when these variables change from having individual to joint impacts.
The results of this study must be understood via the impact mechanisms of violence: stress (Faye, Heng, Collomp, & Peroux, 2003), the somatization of certain symptoms (Eberhard-Gran et al., 2007), substance use that facilitates certain types of violence (Burke, Thieman, Gielen, O’Campo, & McDonnell, 2005), as well as neurological damage due to physical violence (Campbell & Lewandowski, 1997). In this context, it is important to highlight three needs of current public policies.
First, the need to study severe violence and its serious consequences. Research tends to focus on the average woman, ignoring probable heterogeneous effects and limiting the scope and patterns of the effects of intimate partner violence. This heterogeneous principle has been well understood in the typology of batterers’ literature (Langhinrichsen-Rohling, 2005), but has not yet influenced the rest of the body of studies on intimate partner violence.
Second, there is a need to strengthen the focus on VFR—or severe forms of violence—in policies dealing with its causes and consequences, both in women and in their children. Mixed solutions, which combine community interventions (aimed at mitigating risk factors and promoting protective factors through parenting support and education) with focused interventions on higher risk groups may be a good solution (Herrenkohl, Higgins, Merrick, & Leeb, 2015). Third, public policies need to link VFR with the social learning mechanisms and major depressive disorders related to the intergenerational transmission of violence. It has been empirically proven that social learning constructs work well on intimate partner violence (Cochran, Maskaly, Jones, & Sellers, 2017), and that depression magnifies its effects (Bennice et al., 2003) and allows for somatization in children (Arroyo et al., 2017). However, in Latin American countries measures to reduce severe violence and femicide have traditionally been reactive (prosecution and legislation). By not addressing the sociocultural norms that promote violence against women—the underlying cause of violence (Joseph, 2017)—severe violence and femicide rates will continue to be problematic.
Policy makers should examine the ways in which this research can contribute to the creation of better policies aiming at women at risk of severe violence. Getting women to turn to health care systems implies several challenges. First of all, severely battered women tend to establish relationships with men who are more likely to retaliate than allow the relationship to end (Holtzworth-Munroe et al., 2000). Moreover, Black (2011) states that along with the urgent need to integrate an intimate partner violence perspective into health care studies, we must also support training for medical personnel. Health care professionals have a hard time identifying these women (Varjavand, Cohen, & Novack, 2002), and most women who use these health services claim that the physical effects of violence are not properly addressed (Plichta, 2004). This is important for victims of VFR as depression—an effect found in this study as well as in the literature—could lead to an incorrect medical diagnosis. Particularly in patriarchal societies, such as Peru, where the effects of violence are intensified, public policies must take into account that women in these contexts are less likely to get help for their symptoms or for violence in general.
One option to get more victims of VFR to turn health care systems to resolve issues related to violence lies in universal screenings for risk factors and symptoms of intimate partner violence to detect it among women with a low likelihood of reporting, or even recognizing, the problem (Black, 2011; Plichta, 2004). Risk assessment tools, such as the Danger Assessment (J. C. Campbell, 1995) or the Domestic Violence Screening Instrument (Williams & Grant, 2006), are extremely helpful to that purpose and even better if they are culturally adapted to the specific country or local culture to be assessed. Peruvian authorities have not been reluctant to implement risk assessment tools. The problem is that they have not been universally implemented in all public health services. This represents an important limitation, but not necessarily the most pervasive one. In Peru, violence against women is extensively justified both by men and women. Distorted thinking about women is common among batterers, and even more frequent in the most aggressive men who exert forms of violence similar to femicide (Loinaz, Ortiz-Tallo, Sánchez, & Ferragut, 2011). Preventive policies are weak, not effective and not based on evidence.
Finally, focusing on the effects of VFR in women and their children is crucial to recover the social functioning of these women in society. However, at the same time, it cannot take the place of the more important discussion of how to reduce and prevent intimate partner violence. More work needs to be done regarding the latter.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.