
Abstract
While social support is critical in helping intimate partner violence (IPV) survivors heal and build hope, social isolation is a frequent experience for survivors. For survivors residing in domestic violence (DV) emergency shelters, the isolation from social supports is often exacerbated by shelter rules and policies. This study uses a 20th century feminist framework to understand the ways in which social support networks are maintained and/or strained when survivors reside in DV emergency shelters. Among this sample of 76 survivors, 40 participants identified family members as their support system, with siblings and mothers most frequently identified, and 14 participants identified friends as their social support. Prior to entering the DV shelter, survivors reported that their support networks provided encouragement and motivation along with emotional support, financial and material support, and support with children. Participants spoke about the process of informing their support systems of the transition into a DV shelter, the positive and negative impacts of the transition on their support system, and the roles that frequent telephone calls and texts played in maintaining their support networks. Participants reported positive impacts of residing in a DV shelter including improved emotional and physical health, strengthened emotional relationships, and improved physical and emotional resource provision. For those participants reporting negative experiences, they frequently identified logistical barriers, including the inability to receive visitors at the shelter, the distance between them and their friends and family, and strict rules around curfew and child care. Our findings invite researchers and practitioners to consider further examination of best practices around programming that supports survivors in maintaining social supports while residing in shelter programs
Introduction
Intimate partner violence (IPV) is a significant social and public health concern. Nearly 25% of women experience IPV in their lifetime (Breiding, Chen, & Black, 2014). IPV includes psychological aggression, stalking, physical violence, and sexual abuse by a current or former intimate partner (Breiding, Basile, Smith, Black, & Mahendra, 2015) and has a significant impact on the survivor’s financial stability, physical health, mental health, and social networks (Bonomi et al., 2009; Devries et al., 2013; Dillon, Hussain, Loxton, & Rahman, 2013). For individuals experiencing IPV, formal or informal support systems provide relief and support (Goodman & Smyth, 2011; Sylaska & Edwards, 2014) with higher quality support systems demonstrating decreased survivors’ distress and increased physical and mental health recovery (Jose & Novaco, 2016; Kamimura, Parekh, & Olson, 2013).
For survivors residing in domestic violence (DV) emergency shelters, shelter rules and policies can create social isolation (Baker, Billhardt, Warren, Rollins, & Glass, 2010; Fisher & Stylianou, 2019; Glenn & Goodman, 2015). Survivors often identify the most difficult aspect of shelter life as isolation from their social supports (Glenn & Goodman, 2015) and indicate that isolation from social supports is a primary reason for leaving DV emergency shelters (Fisher & Stylianou, 2019). While research has demonstrated that DV shelter programs interfere with survivors’ ability to connect with their social networks, further understanding of the ways in which those social support networks are maintained and/or strained when residing in a DV emergency shelter is needed. Understanding how residing in a DV shelter impacts survivors’ ability to maintain social support networks can guide DV organizations to modify shelter programs to further support survivors as they rebuild their lives. To fill this gap in the literature, interviews were conducted with residents of DV emergency shelters to deepen our understanding of the ways in which social supports are strained and/or maintained as survivors transition into shelter programs.
Social Support and IPV
Social support is a phenomenon whereby individuals are part of a community that is reciprocal and where they feel cared for, valued, and loved (Cobb, 1976). Social support increases individuals’ ability for emotional mastery and contributes directly to women’s physical safety (Fleet & Hiebert-Murphy, 2013; Salazar, Valladares, Öhman, & Högberg, 2009). In addition, social support can decrease stress and increase physical and mental health recovery (Jose & Novaco, 2016; Kamimura et al., 2013).
IPV survivors seek support from social networks to cope with stress resulting from the abuse (Jose & Novaco, 2016; Kamimura et al., 2013; Sylaska & Edwards, 2014) and to end the abuse (El-Bassel, Gilbert, Rajah, Foleno, & Frye, 2001; Rose & Campbell, 2000; Sylaska & Edwards, 2014). Survivors often report abuse to at least one informal support person (Sylaska & Edwards, 2014) and are most likely to share with a friend or female relative (Overstreet, Gaskins, Quinn, & Williams, 2017; Rose & Campbell, 2000; Sylaska & Edwards, 2014). Informal supports may also include neighbors, coworkers, and classmates (Ansara & Hindin, 2010; Belknap, Melton, Denney, Fleury-Steiner, & Sullivan, 2009; Leone, Johnson, & Cohan, 2007).
Despite the importance of social support, survivors often report experiencing social isolation (Bonomi et al., 2006; Hadeed & El-Bassel, 2006; Katerndahl, Burge, Ferrer, Becho, & Wood, 2013). Abusive partners often take explicit and intentional steps to isolate their partners, demanding that their partners break contact with family, friends, and community members. Survivors who experience repeated cycles of abuse may experience the exhaustion of social supports (Goodman, Dutton, Weinfurt, & Cook, 2003). Supportive individuals, who can recognize the pattern of abuse, may feel frustrated or burnt out by the repetitive nature of the abusive relationship. Survivors may feel embarrassed to disclose abuse experiences or may worry about burdening family and friends, particularly if the abuse is repetitive (Dunham & Senn, 2000; Rose & Campbell, 2000).
Many survivors report feeling dissatisfied with the quality and quantity of support from their social networks (El-Bassel et al., 2001; Goodkind, Gillum, Bybee, & Sullivan, 2003). To understand IPV survivors’ barriers to seeking social support, Rose and Campbell (2000) interviewed 31 women in abusive relationships in a large urban city in the United States. Among this sample, participants reported feeling isolated, either by unhelpful responses from family and friends or because of the abusive partners’ attempts to control them. Survivors identified three main barriers to social support including (a) societal stigma, (b) reluctance to engage informal supports, and (c) negative responses from friends and family (Rose & Campbell, 2000).
In addition to facing barriers to seeking social support, survivors often find that helpful social networks are not consistently helpful across all areas of need. Trotter and Allen (2009) interviewed 48 female IPV survivors seeking services from a community agency in central Illinois. Survivors reported that individuals were supportive when they provided emotional support, helpful advice or information, and practical forms of aid. Survivors described unsupportive individuals as emotionally unavailable and reported that unsupportive individuals blamed the survivors for the abuse, distanced themselves, minimized the impact of the abuse, criticized the survivors’ choices, told the survivors what to do, and refused or failed to provide practical assistance. In addition, the more attempts survivors make to separate from their abusive partners, the less likely they receive emotional support from family or friends (Goodkind et al., 2003). These negative reactions from family and friends significantly predict the quality of life for the survivors, even when controlling for emotional support, psychological abuse, and physical abuse experiences (Goodkind et al., 2003).
Researchers examining racial differences of social support among IPV survivors have noted racial and ethnic differences in social support responses. Given the tradition of strong social support and communalism that is rooted in the African American community, researchers have noted that African American survivors report family and friends are often willing to provide tangible aid and services such as child care, transportation, and shelter (Morrison, Luchok, Richter, & Parra-Medina, 2006). However, stigma around victimization and help seeking among the African American community can be a hindrance to accessing social support for survivors. African American survivors have noted that family and friends are, at times, hesitant to get directly involved or are emotionally unsupportive (Morrison et al., 2006).
Similarly, researchers have found that Latina women are likely to seek help from family, but less likely to seek help from friends (Flicker et al., 2011). Traditional Latino family values that emphasize keeping family problems within the family in fear of shame may contribute to this finding (Flicker et al., 2011). Despite the potential racial differences in how survivors engage with support networks, survivors experiencing IPV are more socially isolated than individuals who are not experiencing IPV (Bonomi et al., 2006; Hadeed & El-Bassel, 2006; Katerndahl et al., 2013).
DV Shelter Life and Social Support
While many survivors leave abusive relationships, other survivors face barriers to separating including social isolation, financial dependence, and lack of financial and social resources. DV shelters, therefore, have an important role in helping survivors leave abusive relationships by offering services, safety, and a place to review options (Grossman & Lundy, 2011; National Network to End Domestic Violence [NNEDV], 2016). IPV survivors who utilize DV shelters often have the most needs as they report severe and frequent abuse experiences (Lyon, Lane, & Menard, 2008), increased rates of mental health struggles (Helfrich, Fujiura, & Rutowski-Kmitta, 2008), and significant lack of social and financial resources (Krishnan & Hilbert, 1998) compared with IPV survivors who do not seek shelter services.
For many survivors with significant safety, emotional, and/or financial needs, shelters are an essential intervention (Lyon et al., 2008; Messing, O’Sullivan, Cavanaugh, Webster, & Campbell, 2017). Survivors report feeling satisfied with shelter programming and often report that residing in shelter is the most effective service to help end the abuse (Few, 2005; Sullivan & Virden, 2017). In addition, researchers have found that DV shelter use is significantly associated with ending abusive relationships (Panchanadeswaran & McCloskey, 2007; Perez, Johnson, Walter, & Johnson, 2012).
However, residing in DV emergency shelters can also be an isolating experience for survivors (Bonomi et al., 2006; Goodman & Smyth, 2011; Hadeed & El-Bassel, 2006; Katerndahl et al., 2013). Shelter policies increase isolation, such as confidentiality policies, which often require survivors to live far away from their support network and community and prevent survivors’ friends and families from visiting the shelter (Baker et al., 2010; Haaken, 2010). These policies can create barriers for survivors attempting to access their social networks. Curfew regulations make it difficult for survivors needing to travel to their community of origin, and some shelter programs require survivors to quit their job, limit the use of the telephone, or refrain from contacting social supports for the first few days, if not longer.
Shelter residents often report isolation from their social supports as the hardest part of living in DV shelters. Survivors describe the emotional distress caused by isolation from their social supports and express frustration toward shelter rules that limit contact with their social support networks (Glenn & Goodman, 2015). Displacement from one’s home and community is a primary reason cited by survivors for wanting to leave DV shelters (Fisher & Stylianou, 2019). Survivors often report losing their support systems when they relocate to leave their abusive partners. Some survivors even intentionally cut off connections with family and friends to reduce the possibility that the abusive partner can find them. Other survivors describe how loved ones reject their desire to seek safety, which results in the loss of social support (Thomas, Goodman, & Putnins, 2015).
The DV field can benefit from deepening our understanding of the informal supports utilized by survivors and the ways in which those support networks are maintained and/or strained while survivors reside in DV emergency shelters. This knowledge can be used by DV shelter programs to design and/or modify programming to support survivors remain connected to family, friends, and community as they rebuild their lives.
Conceptual Framework
This study uses a 20th century feminist framework to understand the ways in which social support networks are maintained and/or strained when survivors reside in DV emergency shelters. This lens acknowledges the impact of oppression and the role of mutual relationships and self-determination in addressing and healing from trauma (Kulkarni, Kennedy, & Lewis, 2010). Researchers applying a feminist lens focus on the strengths of participants and aim to capture women’s lived experiences and provide space for women’s voices to serve as the source of knowledge (Campbell & Wasco, 2000). Twentieth century feminist theory acknowledges that while women worldwide can have diverse personal and cultural histories, some patterns occur nearly universally. These patterns include a dominant history of political oppression, an assignment to caring labor, and increased risks of victimization (Donovan, 2012). The feminist framework is used in analyzing the data to inform our understanding of the context in which women seek safety and the ways in which seeking safety impacts relationships with social support networks. While this study includes one biologically born male participant, he also identifies as a gay man of color. Due to this intersectionality of multiple historically marginalized identities in mainstream society and as a male survivor of IPV, the researchers felt that feminist theory is applicable to his narrative.
In our analysis, we focused on each woman’s story and on understanding each woman’s resilience to creating safety and rebuilding hope. Resilience is a multidimensional dynamic process between each woman and their social and cultural environment (Masten & Wright, 2010; Ungar, 2008) that allows for the voices of survivors to shed light on suffering and surviving simultaneously. Researchers examining resilience among survivors have depicted the resilience process as being impacted by a context dependent continuum in which a number of factors can either increase or decrease resilience (Crawford, Liebling-Kalifani, & Hill, 2009). In using the feminist lens, we wanted to understand the ways in which social support networks are maintained and/or strained when IPV survivors reside in DV emergency shelters. In particular, the following research questions guided this study:
Method
Procedures
The data for this study were originally collected as part of a longitudinal needs assessment conducted by one large urban nonprofit operating six DV emergency shelter programs in the northeast United States. Evaluators conducted three interviews with DV survivors over a nine-and-a-half month period. At Time 1, 83 residents completed in-person baseline interviews within the first 2 weeks of entering the DV shelter. The initial interviews were conducted between May through December of 2014, during which 379 new residents entered the shelter system. Approximately four-and-a-half and nine-and-a-half months after entering shelter, the evaluators conducted the second and third interviews.
To recruit for the study, shelter staff distributed flyers to residents as they entered shelter. In addition, the evaluators attended orientation groups at the shelters to explain to new residents the needs assessment project. The participant eligibility criteria required that the resident be 18 years of age or older and a new resident residing in the DV emergency shelter. Incentives were provided to participants for their time in increasing amounts with a US$10 gift card at Time 1, a US$15 gift card at Time 2, and a US$25 gift card at Time 3. Evaluators trained in interviewing DV survivors conducted the interviews. Written consent for participation was obtained which informed residents that (a) participation was voluntary and they had no obligation to participate, (b) their decision to participate or not would not affect the services they received, and (c) they could refuse to answer questions or stop the interview at any time.
The data for this study utilized responses from the Time 1 qualitative portion of the interviews. The qualitative questions were asked at the end of the interview, after completion of quantitative items, and the evaluators typed the participants’ responses into SurveyMonkey®. As the participants could view what the evaluators were typing during the interview, the evaluators asked the participants whether anything was entered inaccurately. The average length of the Time 1 interviews was 62 min and ranged from 30 min to 110 min.
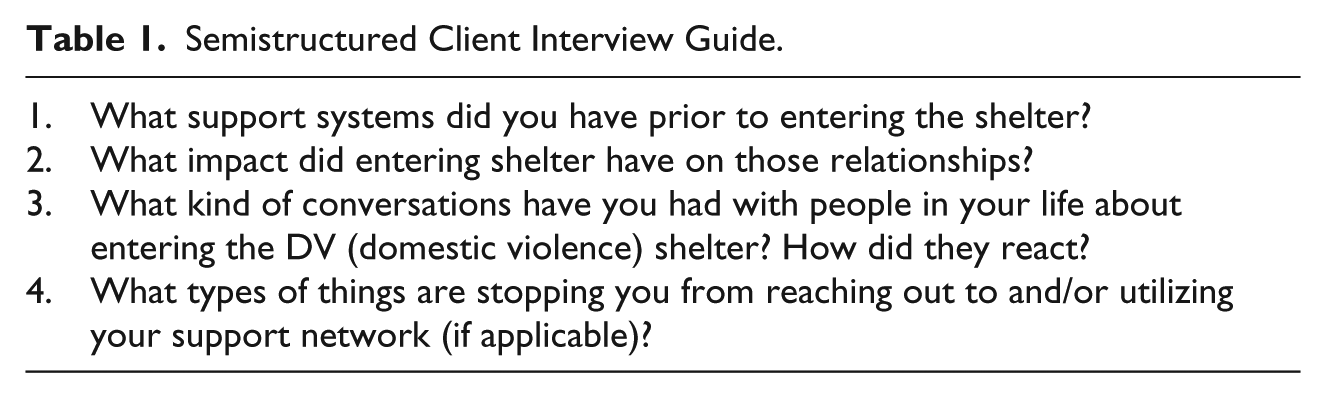
Interview questions analyzed for this study focused on understanding the support networks of IPV survivors and the ways in which social support networks were maintained and/or strained after entering the DV emergency shelter. Table 1 outlines the semistructured interview guide.
Semistructured Client Interview Guide.
Data Analysis
According to Bernard Berelson (1952), content analysis is “a research technique for the objective, systematic, and quantitative description of the manifest content of communication” (p. 18). It is a research method for “making replicative and valid inferences from data to their context” (Weber, 1990, p. 21) with the goal of developing knowledge and understanding of the topic of study. For this study, a combination of conventional content analysis and summative content analysis were used to derive findings directly from the data and to understand quantifiable findings within the underlying context of the women’s narratives (Hsieh & Shannon, 2005).
First, key words were coded and quantified in NVivo to identify participants’ sources of informal support, the types of informal support received, and the factors that impacted participants’ decisions on whether or not to inform social support networks of the transition into a DV emergency shelter. Next, an inductive analysis of the data was conducted. The text was read and re-read to achieve immersion and obtain an overall sense of all participants’ responses. Data were read word for word and open coded to capture key concepts. The evaluators continued to re-read the text and grouped open codes with similar concepts to develop initial coding themes. Finally, the coding themes were organized and grouped into meaningful clusters (Patton, 2002). This data analysis approach provided a flexible, pragmatic method for developing knowledge on the informal support networks of IPV survivors and the ways in which those networks were maintained and/or strained as survivors transitioned into DV emergency shelter programs.
Participant Characteristics
Of the 83 residents who completed the baseline interview, 76 residents (92%) responded to the questions regarding social support networks. The ages of the participants ranged from 19 years to 54 years, with an average age of 28.6 years. The majority of the participants identified as female (n = 75) and as straight/heterosexual (n = 68). All participants were individuals of color with 30 participants identifying as African American/Black, 31 participants as Hispanic/Latina, nine participants as multiracial, two participants as West Indian, one participant as Caribbean, and one participant as Native American. Two participants did not identify their race/ethnicity. The majority of participants (n = 66) had minor children.
Approximately a third (n = 28) of participants had not achieved a high school degree, 44 participants had a high school diploma or GED, and four participants had a college degree. At the time of the first interview, over half (n = 61) of the participants were unemployed, seven participants were employed full-time, seven participants were employed part-time, and one participant did not provide information on employment status. Seven participants were students with five attending full-time and two attending part-time. The participants were financially vulnerable with 31 participants reporting an annual income of less than US$10,000, 22 participants reporting an annual income between US$10,001 and US$35,000, six participants reporting an annual income above US$35,000, and 13 participants reporting they did not know their annual income. Four participants did not answer the income question. In addition, 53 participants received food stamps, 31 participants received public assistance, 32 participants received WIC (Women, Infants, and Children), and 11 participants received supplemental security income or social security disability insurance.
Results
Informal Support Networks
Half (n = 40) of the participants reported that family members formed the basis of their support system. While some participants referred to their entire family as their support network, participants more frequently identified specific family members. The frequently reported supportive family members were siblings (n = 16), mothers (n = 15), fathers (n = 8), aunts (n = 4), children (n = 3), godmothers (n = 2), cousins (n = 2), and fathers of the participants’ children (n = 2).
My sister is the one that made me stay above water. I can speak to her about everything and she’s more my support system. I can speak to my mom too, but more my sister . . . I can get support from them. They just tell me to stick in there and things will work out. My mom, she is very protective of me and my kids. She helps a lot . . . I do not go back because my baby’s father was just released and knows the area. My mom, the house she lived in is where the incidents happened. When he got arrested, she ended up moving from there and I ended up leaving as well.
While the majority of participants identified supportive family members who lived nearby, 13 participants referenced family members who lived out of state. These participants reported speaking regularly with their supportive family members but also stressed that the distance was a barrier to experiencing many of the positive effects associated with a supportive relationship. As one participant shared, I have family but they live in [another state] . . . My sister is there as an emotional support. Only my brother knows that I am in shelter. I do not want them communicating with my ex. I want him to assume that I am still in [another state]. My brother hates that I am here but he knows that I am okay, he understands.
Approximately one in five participants (n = 14) identified friends as their social supports. Participants who identified as African American/Black were almost twice as likely to identify friends in their supportive network (n = 9) compared with participants who identified as Hispanic/Latina (n = 5). Four participants identified individuals who held formal roles in their life as providing their main source of support. These participants identified church members, a professional counselor, a supervisor at work, and a parent advocate as critical formal supports.
Absence of Support
A quarter of the participants (n = 21) reported they had no support system. While six participants did not elaborate further on this statement, three subthemes emerged from those who shared with more detail. The first subtheme highlighted this lack of support due to the involvement of their abuser, who had controlled their access to any relationship with friends or family. One participant shared, “I had no support before. He [ex-partner] kept me isolated from the world. When I came here [the DV shelter], it was more freedom.” The second subtheme was a historically strained or poor relationship with family members.
I do not have friends anymore. No continuous or dependable support. Most of them do not know I am in shelter . . . I am going to start crying, because this is too much. They’re mostly cut off. I don’t really speak to anybody. I have one friend that I speak to and that’s just that. I don’t want to tell them because I don’t want them to tell him. They are mostly his family. I could tell her (a friend) but I just didn’t. People look down on you when you are in shelter because they don’t know what a shelter is like.
The third subtheme included participants who spoke to the ways in which the abusive relationship created barriers within their support networks.
I was going through a lot of abuse and torture. The only person that I was emotionally attached to was my mom. She’s in another state and she’s not well. I really didn’t even like to call her about stuff because my trials and tribulations would have made her sicker. My parents know about the abuse and we really don’t talk about it anymore. It used to be a discussion, but it isn’t anymore. I guess that’s more so because I am, I was still in the relationship and a lot of the times you can’t tell a person what to do or how to do something once they’re in it. Once they come out of it you can see things differently, you know that’s what I’m learning now. I’m out of that situation and I can look back at it and see it differently.
Types of Support Provided
Of those participants who reported receiving social support, five subthemes of the types of support emerged. While there was no clear pattern as to which relationships provided what type of support, the themes that emerged included (a) supportive friends and family who encouraged, suggested, or motivated the participant to go to the shelter; (b) disclosure that the family/friend also experienced IPV; (c) emotional support; (d) financial and material support; and (e) support with children.
Encouragement and motivation to go to shelter
Nine participants identified family members and eight participants identified friends who encouraged them to leave their partner and enter a DV emergency shelter. Five participants reported that their mom encouraged them to enter shelter to protect themselves and increase their safety while other participants identified sisters, fathers, and aunts who encouraged them to seek shelter. One participant shared, “My mom she supported me but as far as anyone else she is the only one that responded. She said that if coming to the shelter was going to protect me and my child to go for it.”
The eight participants who identified supportive friends spoke of the ways in which friends “pushed” participants to leave the abusive relationship. As one participant described, My best friend, I’m really close with her. I talk to her about everything. She actually pushed me to get out of this abusive situation. It was kind of like we both did, because she’s also dealing with it, so once we both got rid of these people from our lives . . . We’ve been keeping each other lifted, almost on a positive level to avoid, I don’t know, feeling like we’re going to go back to them or anything, so I feel like that was really helpful.
Shared experiences of abuse
Five participants shared stories in which individuals in their support network had their own personal experiences of IPV and these shared experiences strengthened the relationships and support for the participants. As one participant shared, “They’re really supportive. They know about the situation. My cousin went through the same thing. I was in a DV shelter as a kid with my mom.” Another participant stated, My mother was a really good support system. I consider her to be my best friend. My mother too was a victim of domestic violence when she was younger, that was when she was pregnant with me . . . When my mom shared her experience, I guess we connected more. She was like wow, I can’t believe my son is going through the exact same thing I was going through except the fact that there are no children involved. Whenever I felt like I needed to talk to her or I felt like I was having one of my episodes, she knew what to do to keep my calm and what to say, she knew exactly what to do, so I’m grateful for that.
Emotional support
Thirty-six participants discussed the importance of emotional support from their support networks. Participants described supportive individuals as people who were emotionally present and supportive; talked, called, and/or texted them; kept them motivated and focused; knew exactly what to say; encouraged them to seek help; provided positive feedback; wanted them and their children to be safe; and provided support without being asked. Emotional support was critical during this difficult time, and supportive individuals supported participants in staying positive and by providing safe opportunities for them to vent their thoughts, feelings, and experiences.
My godmother is the only one I’ve told. She was there the last time something happened and she saw that I was hurt. She’s content that I moved myself out of that situation. I haven’t spoken to her in a few days, but she calls and texts me to check in and make sure I’m doing okay.
Financial and material support
Six participants identified receiving financial and material support from their support networks including money, food, clothing, diapers and wipes, and a place to stay.
My friends, my mom, they would help me with any and everything I needed, whether it was groceries, whether it was clothing, whether it was a few dollars, just anything. I have my aunt, but they were waiting for me to make that first move of leaving his father. Now they see I made the first step and they are willing to help me a lot more than they did when I was with him. They came and saw me already in [community name], gave me money, food, pampers and wipes and stuff like that.
Support with children
Four participants identified receiving support with their children. Specifically, participants mentioned child care as a helpful support.
My aunt is the only one who helps me with my kids . . . If I have a job their aunt is able to pick them up. I have a brother that lives here in NY, he has been a great support for my oldest son because he is a teacher he is putting my son in his school. That is the best support, my children going in the right direction.
Social Networks While Residing in DV Shelter
Once the participants entered DV shelter, they reported three themes that related to the experience of social support. Participants discussed (a) the process of informing their identified support system of the shelter transition, (b) the impact of the transition on their support system, and (c) the role of frequent telephone calls and texts.
Process of informing support members of the shelter transition
Nearly half of the participants (n = 37) told members of their support system they had entered the DV shelter. The majority of participants reported receiving positive feedback and feeling “happy,” “proud,” or “validated.” One participant stated, “[they] were very happy. They were like ‘thank God.’ It was a big relief for everybody.”
[Mom] was proud that I’m taking the steps that are necessary, not only for my safety, but for my future, like, you know as far as, I’ve always been a responsible and independent person . . . I’m doing something about, not just staying in a relationship that’s unhealthy or taking chances with my life.
Seven participants reported receiving negative feedback from their support system. The themes of this negative feedback included members of the support system feeling shocked at the news; feeling bad, sorry, or pity for the participant; and expressing negative emotions that the participant had to “resort” to being in a shelter.
My mom was depressed. She did not want me to take her grandbaby away from her. I left her house before coming here. She is upset I decided to come. I feel as though I needed something that she could not provide and I had to do it on my own.
Ten participants chose not to tell their supports that they entered a DV shelter. Participants identified a number of reasons why they did not share their new residence with their family and friends including (a) privacy, (b) not wanting to bother or upset their social supports, and (c) wanting to avoid being “looked down upon.” However, the primary reason was fear of the abusive partner. For some participants, they reported already being isolated from their support system by the abuser. Other participants wanted to keep the information private as to not alert their abusers to their current whereabouts. One participant explained, “but the truth, out of my community, I haven’t told anyone because the person lives in that same area, and we share a lot of friends, so if I tell someone I know that they’re going to let him know.”
The impact of the transition/shelter stay on the support system
Transitioning to the shelter had a significant impact on the social support system for many participants, but the type of impact it had fell on a wide spectrum. For the seven participants who reported a positive impact, themes included improved emotional and physical health of members of their support system, strengthened emotional relationships, and improved physical and emotional resource provision for the participant by the support system.
My mother isn’t having anymore anxiety attacks [now that I’m in shelter]. Her blood pressure has gone down.
For the 10 participants who reported a negative experience, their responses clustered around logistical barriers. These included the inability to receive visitors within the shelter, an increased mileage/physical distance from family/loved ones, and strict rules around curfew or child care. Five participants commented that the loss of support due to their move left them feeling lonely and isolated.
[It’s been] strenuous on previous relations because you cannot tell them where you live. Any quality time that you were spending is not the same because there is a part of your life that is a secret. It branches into other things, if you visit them, they cannot drop into your home or in the vicinity . . . it’s not as accessible . . . you are totally out of your element. What I did have was mainly my sister but she is in [another state]. She is upset I decided to come. I feel as though I needed something that she could not provide and I had to do it on my own . . . I don’t have any friend no family here, it make it kind of lonely but it is okay because it give me time to rediscover me.
Other participants discussed how the move into shelter impacted their children: My family says it’s okay, but they are angry with the fact that the kids cannot go over there. My grandma is sick, these are her great grandkids. She loves them. It’s a little upsetting that she is not allowed to see her grandchildren. I used to visit them often. I can still talk to them [family] . . . but I can’t see them. My [adolescent] brother, he cried a lot. My son, I had to [leave him with his father] because he, he basically wanted his dad . . . I left a lot of things behind, it’s not even clothing or these items or my son’s items that matter, because I’m not a materialistic person or a money-hungry person. It’s just, that’s my son.
The role of phone calls and texts
The importance of regular, even daily phone calls and texts was mentioned by twenty-two of the participants. This regular communication was key in maintaining positive relationships and mitigating some of the negative factors of entering the shelter. Participants referenced whom they called, how frequently they called, and how these calls were helpful. Participants most frequently referenced speaking on the phone with their mothers. One participant shared, “My mother calls me every morning. I call her every morning. If I go out, I call her when I return.” Another participant shared that entering the shelter changed the context of her phone calls, “My friend is able to call me and actually hold a full conversation with me without being disrupted, so those relationships are a lot better.”
Discussion
This study aimed to contribute to the literature by understanding how IPV survivors’ social support networks were maintained and/or strained when residing in a DV emergency shelter. Consistent with the literature, this study found that many survivors frequently sought support from informal social networks (Jose & Novaco, 2016; Kamimura et al., 2013; Sylaska & Edwards, 2014). Among this sample of 76 survivors, 40 participants identified family members as their support system, with siblings and mothers most frequently identified. This finding mirrored the literature, which has found that survivors are most likely to reach out to friends or relatives (Overstreet et al., 2017; Rose & Campbell, 2000; Sylaska & Edwards, 2014). However, it did not align with the literature that documents survivors reach out to neighbors, coworkers, and classmates (Ansara & Hindin, 2010; Belknap et al., 2009; Leone et al., 2007). In addition, this study challenges the findings of Belknap and colleagues (2009), Overstreet and colleagues (2017), and Sylaska and Edwards (2014) who found that survivors of IPV more frequently disclose abuse experience to a friend before disclosing to a family member. Participants in this study identified family members as their support system nearly 3 times more often than they identified friends. However, approximately one in five participants identified friends as their social supports with African American/Black participants almost twice as likely to identify friends in their supportive network compared with Hispanic/Latina participants.
Conversely, a quarter of the participants reported having no support system. Among this subsample, survivors described the ways in which their abusive partner controlled or actively discouraged their involvement with friends and family. Participants spoke to a history of strained relationships with family and the ways in which the move to the DV shelter created barriers within their support networks. Among this subsample, themes from the literature around the isolation of IPV survivors were highly relevant (Dunham & Senn, 2000; Goodman et al., 2003; Rose & Campbell, 2000). Goodman and colleagues (2003) have highlighted the exhaustion of social supports that often occur among IPV survivors, and in particular among survivors with repeated cycles of abuse experiences.
Social Supports Prior to DV Shelter
Prior to entering the DV shelter, survivors reported that their support networks provided encouragement and motivation along with emotional support, financial and material support, and support with children. Participants identified family members and friends who encouraged them to leave their partner and enter a DV shelter. Five participants shared that individuals within their support network had their own personal experiences of IPV, which strengthened both their relationship and their support. Almost half of the participants discussed the importance of emotional support and described supportive individuals in their lives who were emotionally present, reached out to check on them, motivated and focused them, and provided positive feedback. While the literature often highlights the ways in which IPV experiences isolate survivors from their support networks (Dunham & Senn, 2000; Goodman et al., 2003; Rose & Campbell, 2000), many of the participants in this study highlighted the ways in which their support networks guided them through the process of leaving an abusive relationship.
Social Supports While Transitioning Into DV Shelter
When discussing their transition to DV emergency shelter, participants spoke about the process of informing their support systems of the transition, the positive and negative impacts of the transition on their support system, and the roles that frequent telephone calls and texts played in maintaining their support networks. Nearly half of the participants reported that they told their support networks about their transition into a DV shelter, most of whom reported receiving positive feedback. Participants detailed how support networks responded by validating their decisions and by providing positive feedback.
In contrast, seven participants reported receiving negative feedback. Participants within this subsample described family and friends who felt shocked and expressed negative reactions toward participants’ decisions to move into a DV shelter. Ten participants chose not to tell their support network that they entered a shelter program because they wanted to maintain their privacy, did not want to upset their support system, or because they did not want their friends and family to look down on them. These findings parallel the findings from Rose and Campbell’s study (2000) which found that IPV survivors identified stigma, reluctance to engage friends and family, and negative responses from their supports as main barriers to utilizing their social support networks.
Social Supports While Residing in DV Shelter
There was a wide spectrum of responses in describing the impact of residing in a DV shelter on the relationships with survivors’ support networks. Participants reported positive impacts including improved emotional and physical health, strengthened emotional relationships, and improved physical and emotional resource provision. For those participants reporting negative experiences, they frequently identified logistical barriers, including the inability to receive visitors at the shelter, the distance between them and their friends and family, and strict rules around curfew and child care. The negative experiences expressed in this subsample described messages consistent in the literature on the negative impact of residing in DV shelter (Baker et al., 2010; Fisher & Stylianou, 2019; Glenn & Goodman, 2015).
A subsample of participants spoke to the ways in which distance from family members led to social isolation. Participants described how living away from family created barriers to accessing support for them and their children. These themes support the literature on the isolating experiences that IPV survivors often experience when residing in DV shelters (Fisher & Stylianou, 2019; Goodman & Smyth, 2011). Finally, participants highlighted the critical role of telephone calls and texts in maintaining their social support networks, with two thirds of the participants highlighting this as a main form of communication.
Utilizing a 20th century feminist framework, the results of this study focused on capturing the lived experiences of IPV survivors and specifically their experiences with informal support networks as they resided in DV shelters. This study highlights the ways in which both experiences of IPV and residence in DV shelter programs strain relationships with informal support networks. However, the study equally highlights the resilience of both survivors and their friends and families and the ways in which social support networks are maintained, and at times strengthened, through the transitions into DV shelter programs.
Organizations offering DV shelter can use these findings to inform program enhancement efforts aimed at minimizing barriers survivors face in maintaining their social support networks. Such enhancements may focus both on discussing the maintenance of social supports as a critical and ongoing facet of safety planning and through the modifications of program design. Safety planning on a continual basis through active engagement with the survivor prior to and after entering a DV shelter can identify informal support options, particularly safe people with whom they are already connected, brainstorm around the types of support their network can provide, and strategize around ways to maintain support networks throughout their transition process.
The findings of this study support Goodman and Smyth’s (2011) proposed network-oriented practice model in which a partnership is created between staff member and resident with each person utilizing their skill-set to improve individual and community functioning. Network-oriented practice program modifications can focus on improving social support between shelter residents and staff through positive regard and an open-door office policy as well as having an understanding of and working directly with other network practitioners to provide effective long-term, network-based support. Social support can also grow between residents through both shelter community events and support groups (Allen, Robertson & Patin, 2017; Goodman & Smyth, 2011) where residents can feel validated in their experiences of abuse, reduce the associated stigma and stress, improve feelings of empowerment and self-efficacy, and provide support to others.
Program modifications can focus on decreasing system barriers that survivors face in maintaining their support networks, including reducing strict curfew and confidentiality regulations, creating open shelter models in which survivors can invite supportive individuals to visit them and their children, and decrease regulations around overnight stays and child care restrictions. Two state coalitions, the Washington State Coalition Against Domestic Violence (WSCADV; 2015a, 2015b) and the Missouri Coalition Against Domestic Violence & Sexual Violence (MCADVSV; 2011), have led in the development of rules reduction strategies within shelter programs. Early evidence illustrates that low-barrier, voluntary DV service policies positively influence survivor empowerment and service quality (Nnawulezi, Godsay, Sullivan, Marcus, & Hacskaylo, 2018). However, shelters considering rule reduction approaches must maintain focus on survivor safety.
These results challenge service providers to examine current shelter programming through a survivor-focused, strengths-based, feminist lens and to redesign systems that support and bolster survivors’ support networks. This is especially important in light of research that documents the positive impact of strong social support network for survivors, including research highlighting the ways in which social support networks can decrease survivors’ distress and increase physical and mental health recovery (Jose & Novaco, 2016; Kamimura et al., 2013).
Limitations
This qualitative study was designed to inductively broaden our conceptual understanding of the ways in which survivors’ social networks are maintained and/or strained while residing in a DV shelter. The questions used in the interview guide were broad and subjective in nature, and only a limited number of residents receiving services from one urban organization were interviewed. Participation was voluntary, and those who agreed to be interviewed may have been different from residents who did not. Therefore, findings must be understood within the context of a sample of survivors residing in shelters operated by one organization. Generalizability and objectivity is neither assumed nor expected. Further research is needed to determine whether findings are generalizable to the greater population of residents in DV emergency shelters. In addition, research is needed to explore these findings among a larger sample of diverse survivors to explore cultural, ethnic, and racial differences between survivor support networks and the impact on those networks while residing in DV shelter.
Conclusion
Survivors of IPV in this qualitative study highlighted the importance of informal social support networks in the healing process for survivors and their children. Survivors spoke about the ways in which residing in a DV emergency shelter program maintained and/or strained their relationships with informal social supports. Our findings invite researchers and practitioners to consider further examination of best practices around programming that supports survivors in maintaining social supports while residing in shelter programs. Additional research should also further examine the ways in which shelter residence impacts survivors’ social support networks across samples that are more diverse.
Footnotes
Authors Note
Elisabeth Counselman-Carpenter is also affiliated to Department of Social Work, Southern Connecticut State University, New Haven, CT, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research,authorship, and/or publication of this article: This work was made possible by the generous donation of Joann and Todd Lang and family.