
Abstract
The association of household composition with violence-related injury risk has not been explored in the at-risk urban adolescent population. We hypothesize that, similar to the unintentional risk association, higher adult:child ratio, lower household size, and the presence of a grandparent are protective and thus associated with lower risk for repeat fight injury in this population. This is a cross-sectional study of 10- to 15-year-old adolescents who were evaluated in two urban, pediatric emergency departments (EDs; Baltimore, MD, Philadelphia, PA) for a peer fight-related injury between June 2014 and June 2016. Logistic regression was used to test for associations between each household composition measure of interest and youth self-report of a medically attended fight-related injury within the prior 12 months. Of 187 eligible youth, 62 (33%) reported at least one such repeat fight-related injury. With control for potential confounders, youth with past fight injuries did not differ in adult:child ratio (adjusted odds ratio [adj OR] = 1.3, 95% confidence interval [CI]: [0.9, 1.9] ) or household size (adj OR = 0.9, 95% CI: [0.8, 1.1]) but were more likely to have a grandparent residing in the household (adj OR = 3.3, 95% CI: [1.4, 7.9]). Our data demonstrate a positive association between presence of a grandparent in the household and risk for repeat fight injury in urban adolescents without a corresponding association with adult:child ratio or total household size. Further study should explore differences among the households of urban adolescents with and without grandparent presence to further understand this association and define the mechanisms that may contribute to these findings.
Introduction
Unintentional and violence-related injuries are significant pediatric public health issues, accounting for a substantial proportion of mortality and morbidity during childhood and adolescence (Centers for Disease Control and Prevention [CDC], National Center for Injury Prevention and Control [NCIPC], 2018). Unintentional injuries remain the leading cause of death among children and adolescents in the United States throughout the pediatric age span, from ages 1 to 19 (CDC, NCIPC, 2018). Violence-related injuries disproportionately impact adolescents living in urban neighborhoods (CDC, 2012; Cohen, Davis, & Realini, 2016; Ingram & Chen, 2015), and nearly 400,000 youth aged 10 to 19 years are treated annually in EDs for injuries sustained from physical fights (CDC, NCIPC, 2018). Fight-injured adolescents are at risk for negative health outcomes, including future violence-related injuries and homicide, and those with repeat fight-related injuries are a particularly high-risk group (Cheng et al., 2003; Moeller, 2001; Parchment, 1995; Redeker, Smeltzer, & Kirkpatrick, 1995).
While there are important differences in the epidemiology of unintentional and violence-related injury risk, commonalities have also been identified. Interestingly, many sociodemographic factors associated with risk for unintentional injury are also associated with risk for violence-related injuries. These include age, gender, parental education level, and household income (Borse et al., 2008; Department of Health and Human Services, 2001; Dubow, Huesmann, Boxer, & Smith, 2016; Lipsey & Derzon, 1998; Morrongiello, McArthur, & Spence, 2016; Resnick, Ireland, & Borowsky, 2004; U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2018). Components of household composition, including the number of residents in a household, the ages of residents, and their relationships to each other, have also been shown to relate to risk for unintentional injury (Bishai et al., 2008; Celis, Gomez, Martinez-Sotomayo, Arcila, & Villasenor, 2003; Ryan et al., 2013). For instance, prior studies show that higher adult:child ratio, lower household size, and the presence of a grandparent are protective for unintentional injury risk in children, independent of socioeconomic status (Bishai et al., 2008; Celis et al., 2003; Ryan et al., 2013). It is thought that this protective association may reflect increased supervision (Morrongiello, Corbett, & Brison, 2009; Schnitzer, Dowd, Kruse, & Morrongiello, 2015). For instance, Ryan et al found that census blocks in Washington, D.C., with higher adult:child ratios had significantly lower rates of bone fractures (Ryan et al., 2013). Similarly, Celis et al found that lower household size significantly decreased risk for pedestrian injury in Mexican children 1 to 14 years of age (Celis et al., 2003). Finally, Bishai et al found that odds of medically attended injuries were decreased for toddlers who received care from grandparents (Bishai et al., 2008). These studies of diverse populations have shown that components of household composition are associated with risk for unintentional injuries in a variety of circumstances.
The association of household composition with violence-related injury risk has not been explored in the at-risk urban adolescent population. Such household factors could potentially influence risk for fight-related injury in a positive or negative way. For instance, higher adult:child ratio, lower household size, and the presence of a grandparent may lead to increased supervision of adolescents, which may reduce the risk for assault-related injury in a manner similar to that proposed for unintentional injury risk in younger children (Morrongiello et al., 2009; Schnitzer et al., 2015). Alternatively, presence of additional adults and increased household size may increase the potential for conflict within a household during adolescence, when youth are moving toward independence, may desire more privacy and space, and may be more oppositional. Similarly, prior work showing an inverse relationship between family size and youth educational outcomes suggests that resources may be “diluted” within families that have larger numbers of children (Black, Devereux, & Salvanes, 2005, 2010). Such dilution of resources could potentially increase risk for violence-related injury by negatively impacting factors associated with risk for perpetration of youth violence including family income, parental involvement, and/or the youth’s commitment to school and academic performance (CDC, 2012). However, given the paucity of research in this area, the relationship between household composition and violence-related injury risk is not well understood.
A better understanding of this relationship could inform prevention strategies by potentially identifying protective factors and stratifying risk for injury recidivism. For this reason, we undertook this study to evaluate the association between household composition and violence-related injury in adolescents. Specifically, we focus on the high-risk circumstance of repeat fight-related injuries in adolescents living in urban neighborhoods. We hypothesize that, similar to the unintentional risk association, higher adult:child ratio, lower household size, and the presence of a grandparent are protective and thus associated with lower risk for repeat fight injury in this population.
Methods
Design and Sample
This is a cross-sectional study of 10- to 15-year-old adolescents who were evaluated in two urban, pediatric EDs (Baltimore, MD, Philadelphia, PA) for a peer fight-related injury between June 2014 and June 2016 and were enrolled in a randomized-controlled trial of a mentoring intervention during early adolescence. The primary outcomes of the mentoring trial are number of fights and fight-related injuries. The adolescent’s parent/guardian was also enrolled in the study. Inclusion criteria for study participation were ability to speak and understand English, presence of the same household residence for the adolescent and the enrolled parent/guardian, and absence of an ongoing custody dispute or active Child Protective Services involvement. The institutional review boards at both institutions approved the study and a Certificate of Confidentiality from the National Institutes of Health was obtained.
Measures
After informed consent and assent were obtained, youth and parent/guardians completed baseline surveys at the time of enrollment and prior to randomization for the trial. Surveys took approximately 1 hour and were administered by trained research staff during an in-person interview that also included an audio-computer assisted self-interview questionnaire for questions subject to social desirability. Youth-parent dyads received compensation of $40 in gifts cards for completing the baseline surveys.
The youth and parent/guardian answered questions about sociodemographic characteristics, household characteristics, parental perception of the seriousness of the injury, parental monitoring knowledge, parent–child relationship quality, and youth fighting behaviors, using validated instruments. Sociodemographic information included age, gender, race, parental education level, and household income.
Household composition measures included adult:child ratio, household size, and the presence of a grandparent. Parental survey questions asked for a listing of all household residents, their ages, and their relationships to the child; this information was used to calculate adult:child ratio (total number of adult residents > 18 years of age divided by total number of child resident < 18 years of age) and household size (total number of adult and child residents). Responses were reviewed to determine if a grandparent resided in the home. To determine parental perception of the seriousness of the injury, parents were asked “How serious do you think your child’s injury is?” with “Very serious,” “Somewhat serious,” and “Not Serious” as options for responses. Parental monitoring was assessed using a modified version of Silverberg and Small’s Parental Monitoring Knowledge Scale (Li, Stanton, & Feigelman, 2000; Silverberg & Small, 1991). Responses to the 11 items (such as, “I know where my child is when he or she is not at home or at school.”) were based on a 4-point Likert-type scale from (1) strongly agree, (2) agree, (3) disagree, to (4) strongly disagree. A sum was calculated for this scale.
Parent–child relationship quality was assessed by parent report using questions from the National Longitudinal Study of Adolescent Health (Resnick et al., 1997). Examples of questions included “How much do you think your child cares about you?” and “Overall you are satisfied with your relationship with your child?” Responses to the six items were based on one of two Likert-type scales, depending on the specific question: (1) strongly agree, (2) agree, (3) disagree, and (4) strongly disagree or (1) not at all, (2) very little, (3) somewhat, (4) quite a bit, and (5) very much. A sum was calculated for this scale. To determine youth fighting behaviors, youth were asked the following questions: “Not including your ER visit, how many times were you in a physical fight in which you were injured and needed to be treated by a doctor or nurse in the last 12 months?,” “Not including your ER visit, how many times were you in a physical fight with persons other than your brother(s) or sister(s) in the last 30 days?” and “Not including your ER visit, how many times were you in a physical fight with persons other than your brother(s) or sister(s) in the last 12 months?” Responses to these questions were classified as a Yes (≥ 1 fight reported) or No (0 fights reported).
Data Analysis
Data were entered in Microsoft Excel for Mac 2011 (Microsoft Corporation, Redmond, WA) and analyzed by using SPSS Statistics 23.0 (SPSS Inc., Chicago, IL). Comparisons between youth who reported at least one medically attended fight-related injury in the 12 months before this injury and youth who reported no such events during that time period were made using descriptive statistics, t tests, and chi-square analysis.
Logistic regression was used to test for associations between each household composition measure of interest (adult:child ratio, household size, and the presence of a grandparent) and youth self-report of a medically attended fight-related injury within the prior 12 months (not including the fight for which they were enrolled in the study). The first regression analysis included control for potential confounders associated with risk for injury including demographics (age and gender) and measures of socioeconomic status (parental education level and household income). The second regression analysis controlled for these same variables (age, gender, parental education level, and household income) with the addition of other potential modifiers of medically attended injury, including parental perception of the seriousness of the injury, parental monitoring, and parent–child relationship quality.
Results
Of 188 youth enrolled in the study, 187 responded to the survey question “Not including your ER visit, how many times were you in a physical fight in which you were injured and needed to be treated by a doctor or nurse in the last 12 months?” and were included in the final analysis. Overall, the youth were 61% male and 96% Black/African American; the mean age was 13.2 + SD 2.2 years. Within the study population, 125 youth (67%) reported no additional medically attended fight-related injuries in the past 12 months and 62 youth (33%) reported at least one such repeat fight-related injury. Characteristics of these groups are summarized in Table 1. There were no significant differences between the groups in terms of age, gender, race, parent marital status, parental education, and household income. Youth who reported a past fight injury were more likely to report physical fighting in both the prior 30 days (58% vs. 20%, p < .01) and prior 12 months (77% vs. 34%, p < .01). Youth reporting a past fight injury were more likely to report that a grandparent resided in the home (24% vs. 9%, p < .01), were more likely to have both a grandparent and parent in residence (23.0% vs. 6%, p = .02), and parent responses indicated more parental monitoring (18.3 ± 5.0 vs. 16.7 ± 4.7, p = .03). These youth also had a trend of a higher adult:child ratio in the household (1.2 ± 0.8 SD vs. 1.0 ± 0.5, p = .09) and no difference in overall household size.
Characteristics of Youth With and Without a Self-Reported Medically Attended Fight Injury in the Preceding 12 Months.

For continuous variables in which means are compared with t tests, the statistical value noted is a t value. For categorical variables in which proportions are compared with chi-square analysis, the statistical value noted is a chi-square value.
Tables 2 and 3 summarize the results of the multivariate logistic models demonstrating associations with past medically attended fight injury. In Table 2, with control for demographics and measures of socioeconomic status, youth with past fight injuries did not differ in adult:child ratio (adjusted odds ratio [adj OR] = 1.3, 95% confidence interval [CI]: [0.9, 1.9]) or household size (adj OR = 0.9, 95% CI: [0.8, 1.1]), but were more likely to have a grandparent residing in the household (adj OR = 3.3, 95% CI: [1.4, 7.9]). In Table 3, presence of a grandparent in the household remained significantly associated with risk for past medically attended fight injury (adj OR = 3.4, 95% CI: [1.4, 8.5]) with control for demographics, socioeconomic status, parental perception of the seriousness of the injury, parental monitoring, and parent–child relationship quality. Past medically attended fight injury was also significantly associated with increased parental monitoring but not associated with parental perception of the seriousness of the injury and parent/child relationship quality.
Multivariate Logistic Regression Analyses Demonstrating Independent Household Composition Associations With Repeat Medically Attended Fight Injury.
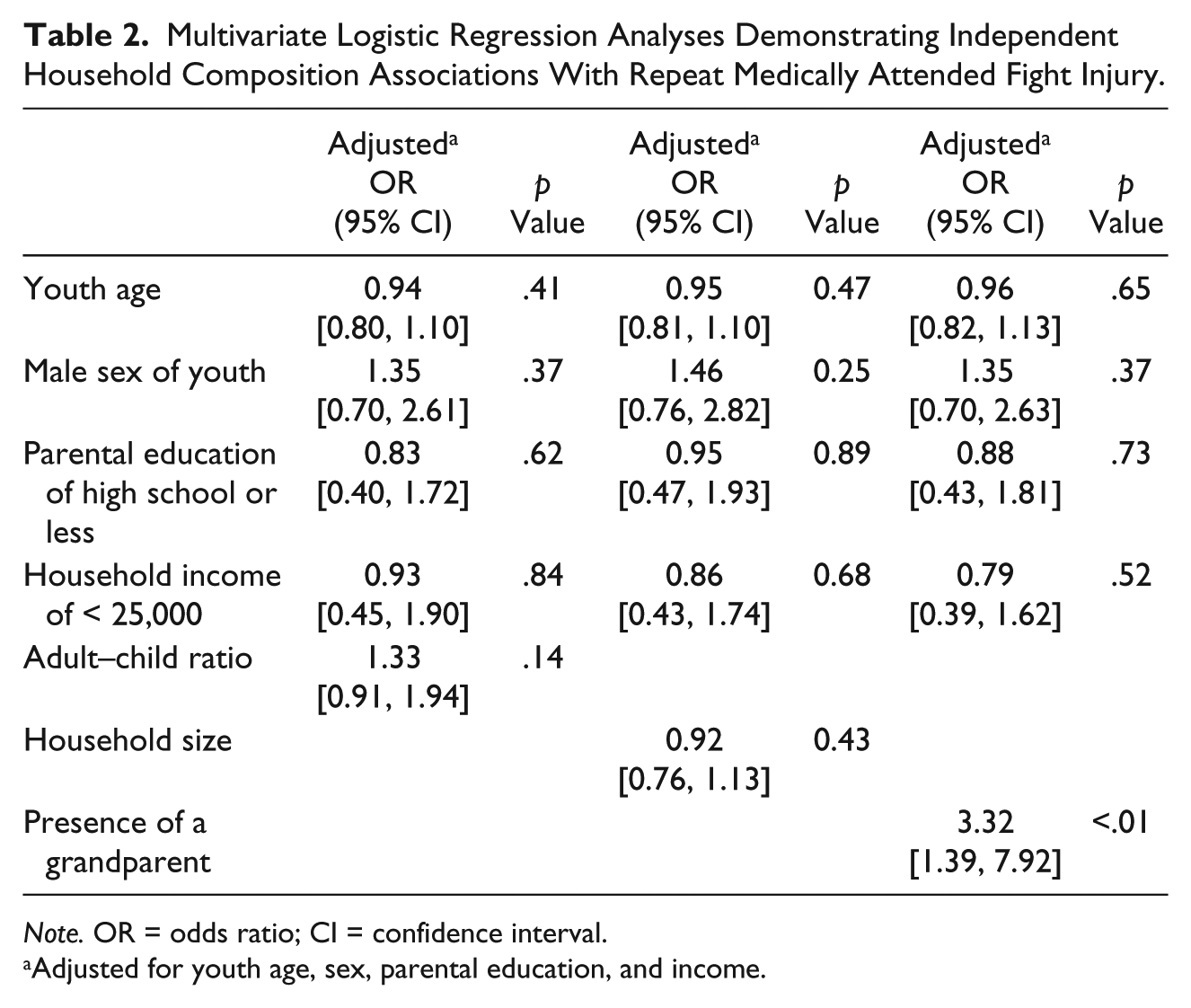
Note. OR = odds ratio; CI = confidence interval.
Adjusted for youth age, sex, parental education, and income.
Multivariate Logistic Regression Analyses Demonstrating Independent Household Composition Associations With Repeat Medically Attended Fight Injury.
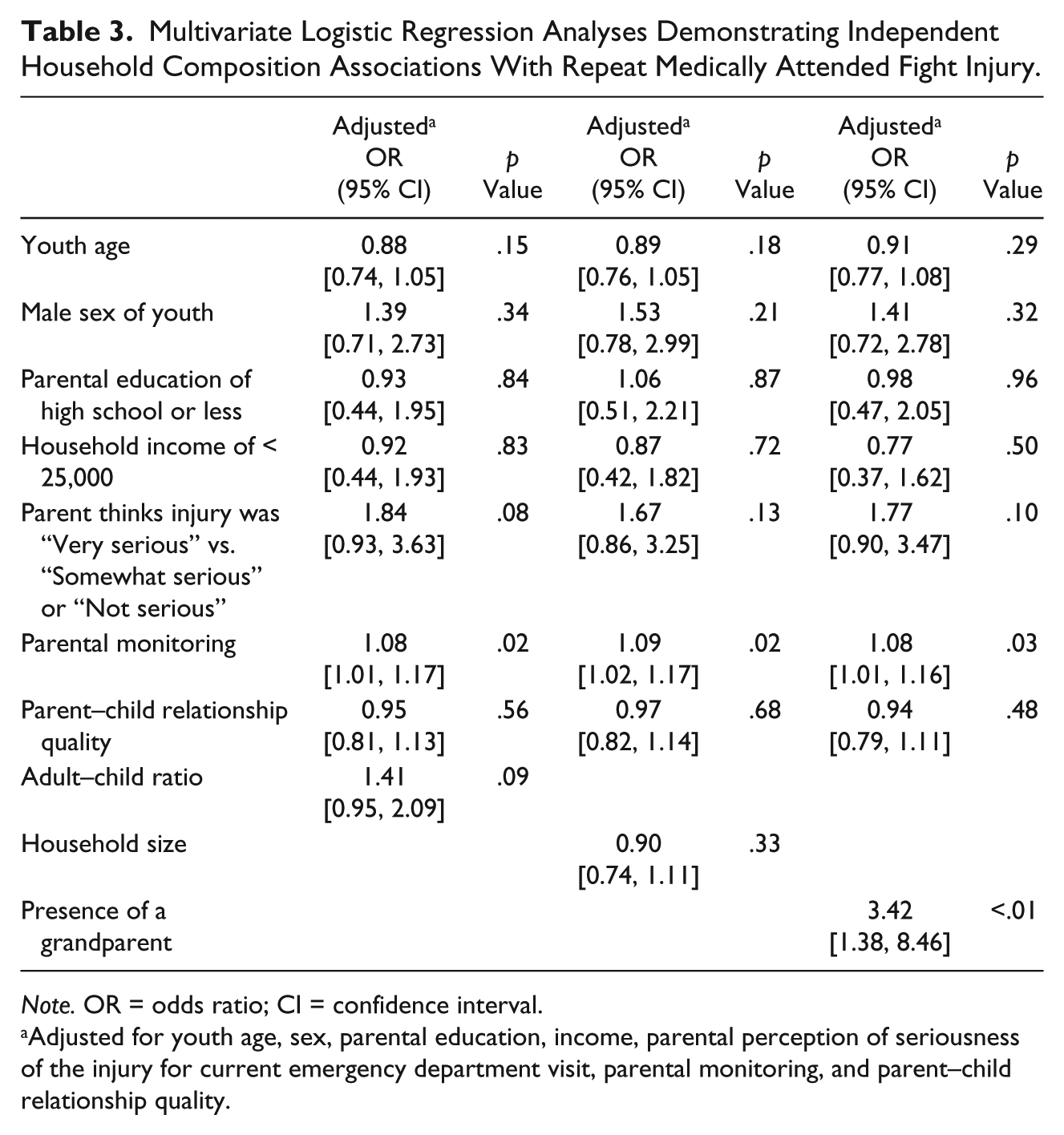
Note. OR = odds ratio; CI = confidence interval.
Adjusted for youth age, sex, parental education, income, parental perception of seriousness of the injury for current emergency department visit, parental monitoring, and parent–child relationship quality.
Discussion
Our data demonstrate an association between presence of a grandparent in the household and increased risk for medically attended repeat fight injury in adolescents living in urban neighborhoods without a corresponding association with adult:child ratio or total household size. These findings differ from the protective associations shown for these factors with unintentional injury risk (Bishai et al., 2008; Celis et al., 2003; Ryan et al., 2013) and may reflect limitation in family resources, other risk factors for violence within these households, and/or differences in caregiver styles for which grandparent residence may be a risk factor. This is supported by studies of African American families that show that the most common reasons for grandparent co-residence were financial challenges experienced by the parents of the grandchild, and the inability of the grandchild’s parents to independently manage a home, that is, due to parental maturity and cognitive abilities, parental employment, or school enrollment (Baker, Silverstein, & Putney, 2008; Minkler & Fuller-Thomson, 2015). Another study showed that the majority of African American grandparent caregivers living in poverty did not receive public assistance that they were eligible for, suggesting that these families may be underresourced (Samuel et al., 2017). Other studies have shown that grandparent residence in the household may negatively influence dietary intake and weight status in their grandchildren and this may reflect differences in family dynamics (Young, Duncanson, & Burrows, 2018). A systematic review of the role of grandparents on dietary intake of grandchildren demonstrated significant associations between grandparent cohabitation and increased rates of child overweight and obesity (Young et al., 2018). Although the mechanism of this association has not been clearly defined, it is hypothesized that caregiver styles, specifically more permissive practices by grandparents, may account for these findings (Young et al., 2018). It is feasible a similar mechanism could contribute to increased risk for injuries related to peer fighting.
Our outcome was limited to medically attended fight injuries and many factors may impact the decision to seek medical care for injuries. Other possible explanations for an increased risk of a medically attended fight injury (as opposed to fight injuries in general) are that the injuries sustained in the fights were more severe, and necessitated medical care, or that the threshold for seeking care was lower due to caregiver styles and unrelated to injury severity. It is also possible that the decision to seek medical care for an injury may either reflect increased supervision, communication, and/or awareness that an injury has occurred. Our findings did not show a significant association between parental perception of the seriousness of the injury for the ED visit related to study enrollment and the report of medically attended fight injury in the prior year, although the “seriousness” of the prior injuries were not queried. Grandparent presence (i.e., frequent grandparent interactions) has been associated with earlier diagnosis of children with developmental disorders (Sicherman, Loewenstein, Tavassoli, & Buxbaum, 2018), which may indicate a lower threshold to seek medical evaluation for concerns and/or differences in caregiver styles. While we did not find an association with parent–child relationship quality, higher levels of parental monitoring were associated with repeat medically attended injury, which may lend support to the theory that supervision may influence the decision to seek medical evaluation. Although the grandparent effect remained significant after controlling for parental monitoring, in households in which parents and grandparents are present, there may be additional supervision provided by the grandparents, above and beyond the extent to which parents themselves are monitoring/supervising their children. It is also possible that this positive association could be due in part to caregivers having increased their supervision and monitoring in response to past fighting behavior and fight-related injuries. Finally, parental report of their own parental monitoring may be inaccurate (Abar, Jackson, Colby, & Barnett, 2015) and potentially subject to social desirability bias; thus, parents of youth with multiple fight injuries may overstate their own parental monitoring.
Contrary to our hypothesis, we did not find a statistically significant association between adult:child ratio or household size and repeat medically attended fight injury. Prior studies show associations for these household factors with unintentional injury risk in children as well as other noninjury outcomes (Black et al., 2005, 2010; Celis et al., 2003; Ryan et al., 2013). Thus, our study also provides further evidence that, despite some commonalities, the epidemiology of urban violence-related injury is distinct from that of unintentional injury risk. This may reflect difference in the at-risk age groups (younger for unintentional and older for intentional) and the developmental implications within these phases. This information is important as further elucidation of the epidemiological factors associated with intentional injury may identify new strategies to reduce youth violence and injury recidivism.
This study has several limitations. First, the use of two sites in relative geographical proximity to each other, the exclusion of non-English speakers, the focus on early adolescence (ages 10-15 years), and the near racial uniformity of the predominantly African American study sample may limit generalizability of the results. Similarly, generalizability may be further limited as this is a highly specific sample of patients that sought medical treatment for the youth’s injuries and consented to participate in an intervention study to participate in a mentoring intervention intended to reduce fighting behavior. On one hand, this sample may reflect a particularly at-risk group of adolescents, as fight-injured youth are at increased risk for negative outcomes (Cheng et al., 2003; Moeller, 2001; Redeker et al., 1995). Alternatively, given the interest in study participation, these youth and families may be a highly motivated subgroup of the population that is treatment-seeking, both for the acute injuries and the exposure to violence. All of these factors contribute to limitations in generalizability. Second, our survey results reflect self-report by the participating youth and/or guardian, which may impact accuracy of the responses, including accounts of events over the past year. It has been shown that injury history accuracy may be suboptimal (Gabbe, Finch, Bennell, & Wajswelner, 2003) and that social desirability bias may influence adolescent response to either underestimate (due to fear of repercussion) as well as overestimate (due to desire for attention or if behavior is associated with perception of increased status) self-reported health risk behavior (Brener, Billy, & Grady, 2003). Our study also focused on “physical fighting” and used this terminology, which did not specifically define how this may or may not differ from circumstances in which physical violence occurs without “fighting.” Individual perceptions of what “physical fighting” means could have biased responses toward overestimation or underestimation, depending on the interpretation of the youth. In addition, it is possible that participating youth could have interpreted the question “Not including your ER visit, how many times were you in a physical fight in which you were injured and needed to be treated by a doctor or nurse in the last 12 months?” to indicate injuries that “needed” medical attention regardless of whether medical attention was actually obtained. However, given that the current ER visit was referenced, we suspect that participants were likely to have interpreted the question as having received medical attention. Finally, our outcome was limited to medically attended fight injuries. As discussed earlier, many factors may impact the decision to seek medical care for injuries, including a lower threshold for seeking medical evaluation and access to care, and thus use of this measure may not reflect severity or clinical significance of the injury. Similarly, inclusion of youth who have sought medical evaluation may omit at-risk youth with significant injuries that are not medically attended; these youth may be at higher risk for negative outcomes due to low resources and support. To address these limitations, future research could be conducted in school and community settings that may offer other measures of physical fighting and violence exposure. Newer data are becoming available in cities that track school events as part of school safety initiatives, as well as police incidents (rather than arrests). These could offer the opportunity for others to enhance or confirm these results in different populations.
Conclusion
Our data demonstrate a positive association between presence of a grandparent in the household and risk for repeat fight injury in adolescents living in urban neighborhoods without a corresponding association with adult:child ratio or total household size. These findings differ from the protective associations shown for these factors with unintentional injury risk and may reflect limitation in family resources, differences in family dynamics, or other risk factors for violence within these households. Further study should explore differences among the households of adolescents living in urban neighborhoods with and without grandparent presence to further understand this unexpected association and define the mechanisms that may contribute to these findings.
Footnotes
Acknowledgements
The authors appreciate the administrative support of Bonnie Addison, Carol Murray, Cecelia Harrison, and the rest of the Take Charge Team as well as the youth and their families that participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has been funded in whole or in part with Federal funds (P20MD000198) from the National Institute of Minority Health & Health Disparities. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.