
Abstract
Cyberbullying is a public health concern worldwide, including China. Cyberbullying victimization has negative effects on adolescents’ health and mental health. This study examined the associations between cyberbullying victimization and several health and mental health problems among adolescents in China. A total of 3,232 adolescents aged 15 to 17 were recruited from 18 high schools in Xi’an, China, using a stratified random sampling method. Self-report data were collected via survey from adolescents in Xi’an, China. In total, 22.2% and 6.3% of the sample reported having experienced cyberbullying victimization in their lifetime and the past year, respectively. Ordinary least squares (OLS) regression revealed that lifetime and preceding-year cyberbullying victimization was, respectively, significantly associated with poorer health (β = −1.58, p < .001; β = −2.22, p < .001), more severe depressive symptoms (β= 3.74, p < .001; β = 4.48, p < .001), and posttraumatic stress disorder (PTSD) symptoms (β = 7.16, p < .001; β = 4.77, p < .001). Binary regression revealed that lifetime and preceding-year cyberbullying victimization was, respectively, significantly related to higher odds of problem drinking (odds ratio [OR] = 1.64, p < .001; OR = 1.84, p < .01), cigarette smoking (OR = 1.69, p < .001; OR = 2.21, p < .001), and gambling engagement (OR = 1.35, p < .05; OR = 1.97, p < .01). Furthermore, greater levels of parent–child attachment were a protective factor against the negative effects of cyberbullying victimization on adolescents’ depressive symptoms (p < .001) and PTSD (p < .05). It is critical to develop and implement prevention and early intervention programs that are tailored to address the needs of adolescents in China. Parental involvement needs to be incorporated into interventions for cyberbullying victimization.
Keywords
Introduction
Cyberbullying
Increased Internet access makes younger generations more familiar with, reliant on, and wired into the Internet. Nearly 200 million Chinese youth under age 19 accessed the Internet in 2017 (China Internet Watch, 2017). Youth use the Internet for a variety of activities including texting, using social media, watching videos and livestreams, listening to music, playing video games, and posting on discussion boards. Widespread Internet access can substantially benefit youth by enhancing their access to a broad range of information and creating avenues for education, social communication, and recreation. However, Internet also creates an environment in which some children are victimized by bullying and harassment. Cyberbullying refers to intended and repeated harm via cyberspace (Hinduja & Patchin, 2008). Perpetrators of cyberbullying can psychologically and/or emotionally hurt others without a face-to-face encounter. Cyberbullying happens primarily in relational and verbal interactions in the form of insults, gossip, mockery, online harassment, cyberstalking, exclusion, and exposing others’ personal information on the Internet (Willard, 2006). Children who experience cyberbullying victimization can be threatened, humiliated, embarrassed, or otherwise targeted by someone they know or strangers on the Internet via computers, mobile phones, and other electronic devices.
Prevalence of Cyberbullying Victimization
Cyberbullying victimization has become an alarming global and cross-cultural problem. The estimated prevalence rates of cyberbullying victimization vary depending on the samples and measurement instruments adopted to assess cyberbullying victimization. In a systematic review of 75 studies, Tokunaga (2010) suggested that the prevalence rates of cyberbullying victimization among youth worldwide range from 20% to 40%. A national study in the United States revealed that 9.1% of adolescents aged 12 to 18 years old have experienced cyberbullying victimization (Payne & Hutzell, 2017). A recent survey of 2,128 adolescents in Belgium showed that 11.2% reported being cyberbullied within the past 6 months (Pabian & Vandebosch, 2016). In addition, a study of 1,530 Australian children reported that 11.5% had experienced cyberbullying victimization (Sakellariou, Carroll, & Houghton, 2012). Cyberbullying is also a common phenomenon in China. It is estimated that cyberbullying victimization among adolescents is as high as 68% (Huang & Chou, 2010; Leung, Wong, & Farver, 2018; Rao et al., 2019; Wong, Chan, & Cheng, 2014; Zhou et al., 2013). Rao and colleagues (2019) found that 44.5% of adolescents reported cyberbullying victimization within the past 6 months using a large, representative sample from one city in China. Given the reported high prevalence of cyberbullying victimization in China, it is imperative for researchers to investigate the impact of this issue on Chinese adolescents’ health, as well as potential mechanisms that can be targeted to reduce the harm of cyberbullying victimization among Chinese adolescents.
Adverse Effects of Cyberbullying Victimization on Adolescents’ Health and Mental Health
Cyberbullying victimization is associated with a number of negative health and mental health outcomes that can effect adolescents’ development (Kowalski, Giumetti, Schroeder, & Lattanner, 2014). The effects of cyberbullying victimization are similar to traditional bullying and include feelings of anger, sadness, fear, and low self-esteem (Hamm et al., 2015; Hoff & Mitchell, 2009; Patchin & Hinduja, 2010). These negative feelings and emotional difficulties may lead to increased mental health problems. The association between cyberbullying victimization and depression among adolescents has been documented in the literature (e.g., Hamm et al., 2015). Specifically, a number of longitudinal studies found that exposure to cyberbullying predicted increased depressive symptoms over time (Gámez-Guadix, Orue, Smith, & Calvete, 2013; Machmutow, Perren, Sticca, & Alsaker, 2012). In addition, victims of cyberbullying may develop posttraumatic stress disorder (PTSD) symptoms (Ranney et al., 2016). Depressive and PTSD symptoms are important distal outcomes in adolescent’s development given that these mental health problems may play a role in the development of general health issues, substance misuse, and suicidal ideation and attempts (Ranney et al., 2016).
Negative effects of cyberbullying victimization on physical health include sleeping problems, headaches, and stomach pain (Kowalski & Limber, 2013). Furthermore, cyberbullying victims are at an elevated risk of using substances including alcohol, tobacco, and illicit drugs (Hinduja & Patchin, 2008; Mitchell, Ybarra, & Finkelhor, 2007). Victims may use substances to avoid or escape from the emotional difficulties, social isolations, and interpersonal stress caused by cyberbullying. Research has shown that childhood victimization is an etiological factor in the development of problem gambling (Blaszczynski & Nower, 2002). However, limited research has explored the specific relationship between cyberbullying involvement and gambling engagement among adolescents.
Despite an increasing number of studies documenting the adverse effects of cyberbullying victimization on adolescents’ health and mental health, few studies have examined the health and mental health problems associated with cyberbullying victimization among adolescents in China. Thus, it is unclear whether the health and mental health problems associated with cyberbullying victimization among adolescents in Western countries are similar to—or distinct from—those manifested by adolescents in China.
Parent–Child Attachment and Cyberbullying Victimization
Research has identified that positive parent–child relationships, or attachment, may effectively reduce cyberbullying involvement (Fanti, Demetriou, & Hawa, 2012; Larrañaga, Yubero, Ovejero, & Navarro, 2016) and attenuate the negative effects of cyberbullying victimization on adolescents’ health and mental health (Elgar et al., 2014; Özdemir, 2014). According to attachment theory, parent–child attachment has profound influences on individuals’ patterns of perceiving, understanding, and coping with interpersonal relationships (Bowlby, Ainsworth, & Fry, 1965). Larrañaga and colleagues (2016) surveyed 813 Spanish adolescents and found that adolescents with more child–parent communication problems were more likely to experience cyberbullying victimization. Adolescents with a secure parent–child attachment are more likely to develop positive understandings and skills that will facilitate positive interpersonal interactions, including interactions via the Internet, thereby reducing the risk of cyberbullying involvement (Larrañaga et al., 2016).
Furthermore, a secure parent–child attachment can foster resilience, including enhancing emotional regulation and developing positive coping for stress and trauma from interpersonal relationships, thereby reducing the risk of developing mental health and behavioral problems due to cyberbullying involvement. A number of studies have shown the link between the quality of children’s relationships with their parents to their own emotional difficulties and problem behaviors (Garber, Robinson, & Valentiner, 1997; Nikiforou, Georgiou, & Stavrinides, 2013). In addition, adolescents with more positive relationships with their parents may have more resources and supports to cope with cyberbullying victimization. Adolescents who receive support from their parents in the form of emotional comfort and problem-solving are less likely to experience the negative effects associated with cyberbullying victimization. One large survey study with adolescents (aged 12-18 years) in the United States found that family contact and communication significantly moderated the relations between cyberbullying and the rates of internalizing and externalizing problems and substance misuse among these adolescents (Elgar et al., 2014). If fostering positive parent–child relationships is useful to mitigating the effects of cyberbullying victimization, it might be an important area of focus for future cyberbullying prevention and intervention efforts among adolescents in China.
The Current Study
In sum, the investigation of cyberbullying victimization is still in its nascent stages in China, and limited research has examined the associations between cyberbullying victimization and specific health and mental health outcomes. Building upon the extant literature of cyberbullying victimization, the current study used a large, representative sample of adolescents in China to investigate the associations between cyberbullying victimization and a number of health and mental health problems. Furthermore, informed by attachment theory, this study aimed to examine the moderation effects of parent–child attachment in the associations between cyberbullying victimization and adolescents’ health and mental health problems.
Method
Sampling and Data Collection Procedures
Cross-sectional data were collected from adolescents of 15 to 17 years of age in Xi’an (a large, highly populated city in Western China) using a self-administered questionnaire between September 2009 and June 2010. To obtain a representative sample of Chinese high school students, we used a three-stage stratified random sampling method. Power analysis was conducted before sampling. Results yielding a sample size of 3,000 adolescents were needed to guarantee an adequate power. The sampling frame was the total population of high school students in Xi’an. First, we randomly selected three administrative districts (two developed urban districts and one rural district) from all administrative units in Xi’an. The administrative units were stratified by geographic and administrative areas based on the records provided by the Bureau of Education. Then, we randomly selected six schools (including secondary schools, high schools, and technical high schools) from all schools in each of the three selected administrative districts. The lists of high schools in these three administrative districts were obtained from local education departments. Ultimately, we randomly selected students from all students in the 18 selected high schools. A list of students in each school was obtained from school administrative personnel. A total of 3,365 students were randomly selected from the student lists.
All of the 3,365 students were invited to participate in the survey. Informed consent was obtained in advance from all parents/legal guardians of participants, and assent was obtained from all participants. The paper–pencil surveys were administered to participants in classrooms during school time by graduate research assistants. Participants were sufficiently separated from each other to ensure that they could not view each other’s responses. Participants were not provided with an incentive to complete the survey. The survey questionnaire took approximately 30 to 40 min to complete. The first author and graduate research assistants were present during survey administration to answer participants’ questions. A total of 3,232 students successfully returned the survey, suggesting a satisfactory response rate of 96.0%. All procedures were approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority of Hong Kong West Cluster. A card containing information about social services for violence prevention in Xi’an was provided to participants during the survey administration in case a need for help arose.
Variables and Measurements
Cyberbullying victimization
The Relational Aggression Scale was modified to assess children’s perceived cyberbullying victimization (Crick & Grotpeter, 1995; Keith & Martin, 2005), given that cyberbullying shares similar constructs of the relational form of traditional bullying (Zhu & Chan, 2015). The adapted cyberbullying victimization scale consisted of seven items that ask participants whether they had experienced any forms of cyberbullying repeatedly in the past year and before the past year, such as rumor spreading (e.g., “Did anyone spread rumors about you on the Internet?”), social exclusion (e.g., “Did anyone exclude you from being in their group of friends on the Internet?”), and being threatened to do what others say (“Did anyone threaten to stop liking you or being your friend unless you do what they say on the Internet?”). In the current study, participants were coded as having experienced preceding-year cyberbullying victimization if they endorsed any of the seven items assessing cyberbullying victimization in the past year. Similarly, a separate variable was created to assess cyberbullying victimization over participants’ lifetime. Participants who endorsed any of the seven items assessing cyberbullying victimization in the past year or before the past year were identified as having experienced cyberbullying over their lifetime. The adapted cyberbullying victimization scale was translated and back-translated to Chinese by the research team. The Chinese version of the scale had an internal consistency reliability of α = .84 in the current sample.
Parent–child attachment
Adolescents’ parental attachment was measured using the Adolescent Attachment Questionnaire (AAQ; West, Rose, Spreng, Sheldon-Keller, & Adam, 1998). The AAQ consists of nine items that assess adolescents’ perceptions of anger and distress in their relationships with their parents (e.g., “My parent only seems to notice me when I am angry”), the availability of their parents (e.g., “I am confident that my parent will listen to me”), and the need for/feelings toward their parents (e.g., “It makes me feel good to be able to do things for my parents”). Each item is rated on a 4-point Likert-type scale, with responses ranging from 1 (strongly disagree) to 4 (strongly agree). Higher composite scores indicate greater levels of parent–child attachment. The AAQ has been previously translated to Chinese, and the AAQ-Chinese version demonstrated an internal consistency reliability of .81, a test–retest reliability of .71, and high convergent validity among Chinese adolescents (Yang, 2007). In this study, the Chinese version of the AAQ had an internal consistency reliability of α = .78.
Health
Adolescent’s overall health was measured using the 12-item Short-Form Health Survey (SF-12 Health Survey; Ware, Kosinski, & Keller, 1996). The SF-12 Health Survey assesses participants’ perceptions on their general health (e.g., “In general, would you say your health is excellent, very good, good, fair, or poor”), physical functioning (e.g., “Did you have a lot of energy?”), and role limitations due to physical health and/or emotional problems (e.g., “How much of the time has your physical health interfered with your social activities?”). Higher composite scores indicate better overall health. The SF-12 Health Survey has been previously translated to Chinese. One study with a sample of Chinese adolescents concluded that the Chinese version of the SF-12 Health Survey had high criterion validity (Lam, Tse, & Gandek, 2005). The Chinese version of SF-12 had an internal consistency reliability of α = .77 in the current sample.
Depressive symptoms
Adolescent’s severity of depressive symptoms was assessed using the Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996). The BDI-II consists of 21 items related to depressive symptomology (e.g., “I feel sad”) that are rated using a 4-point Likert-type scale, with responses ranging from 0 (symptoms not present) to 3 (symptoms strongly present). Higher composite scores indicate more severe depressive symptoms. The BDI-II has been previously translated to Chinese and widely used in studies with Chinese population. Previous studies showed that the Chinese version of the BDI-II had internal consistency reliabilities greater than .85 and good criterion validity (Byrne, Stewart, & Lee, 2004; Yang, Wu, & Peng, 2012). In this study, the Chinese version of the BDI-II had an internal consistency reliability of α = .90.
PTSD
The frequency of adolescents’ presence of PTSD symptoms was measured using the University of California, Los Angeles (UCLA) PTSD reaction index (RI) for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; Pynoos, Rodriguez, Steinberg, Stuber, & Frederick, 1998). This measure is a 22-item self-report questionnaire that assesses different PTSD symptoms including intrusion (e.g., “I am afraid that bad things will happen again”), avoidance (e.g., “I have trouble remembering important parts of what happened”), and arousal (e.g., “I have upsetting thoughts, picture, or sounds of what happened come into my mind when I do not want them to”). Responses are rated on a 5-point Likert-type scale, ranging from 0 (none of the time) to 4 (most of all the time). Higher composite scores indicate more severe PTSD symptoms. The UCLA PTSD-RI has been previously translated to Chinese and demonstrated internal consistency reliabilities greater than .85 in previous studies (Shen, 2009; Wang, 2002). In the present study, the Chinese version of the UCLA PTSD-RI had an internal consistency reliability of α = .95.
Substance misuse and gambling behavior
Adolescents’ self-reported problem drinking, cigarette smoking, and gambling engagement were assessed using questions specifically developed for this study (i.e., “I often get drunk”). Responses for questions that assess substance misuse and gambling engagement were coded as 1 = yes and 0 = no.
Sociodemographic information
Adolescents’ sociodemographic characteristics were collected including age, gender, their parents’ marital status, parents’ employment, parents’ education background, number of siblings, whether the participants’ family were recipients of social welfare, and family income. These variables were controlled for in the subsequent multivariate analyses.
Data Analyses
Descriptive statistics were conducted to describe prevalence rates of cyberbullying victimization, participants’ sociodemographic characteristics, engagement in substance misuse and gambling, and responses to the standardized measures that assess their health and mental health problems. Bivariate tests (i.e., chi-square tests and independent t tests) were performed to examine differences in adolescents’ sociodemographics, parent–child attachment, as well as health and mental health problems between cyberbullying victims and nonvictims.
Multiple regression analyses were performed to examine the associations between cyberbullying victimization and various health and mental health problems, as well as the moderating effects of parent–child attachment on the associations between cyberbullying victimization and various health and mental health problems. First, three ordinary least squares (OLS) regression models were estimated to examine the effects of cyberbullying victimization on adolescents’ overall health, depressive symptoms, and PTSD after controlling for parent–child attachment and sociodemographic factors (e.g., age, gender, parents’ marital status, education background, and employment status, and family economic status). Subsequently, three binary logistic regression models were estimated to predict the effects of cyberbullying victimization on cigarette smoking, problem drinking, and gambling engagement after controlling for the same sociodemographic variables and parent–child attachment. Finally, we examined the joint effects of parent–child attachment and cyberbullying victimization on various health and mental health problems. We generated an interactive term, parent–child attachment × cyberbullying victimization, which was entered into all regression models to estimate the moderation effects.
Missing data were handled using multiple imputations. We imputed the missing values of both dependent and independent variables using 10 iterations of multivariate imputation by chain equations. Relative efficiency values indicate that 10 imputations produced point estimates that were more than 95% as efficient as infinite numbers of imputations (Allison, 2012). Regression analyses were performed using the imputed data set. All models were evaluated using two-tailed tests. Statistical significance was determined using p values (5% level) and 95% confidence intervals (CIs). Analyses were performed using Stata 15.
Results
Participants’ Characteristics
Table 1 presents descriptive statistics for the entire sample, including cyberbullying victims and nonvictims, respectively. The average age of the sample was 15.8 years (SD = 0.9). Slightly more than half of the sample (52.3%) were female. One third of participants (33.3%) reported they were from single-child households. The majority of participants (92.2%) reported that their parents had been married or cohabitating at the time of the survey, and 5.5% of the sample reported that their parents had been separated, divorced, or widowed. Slightly more than 10% of the parents had an education level of college and above. A greater proportion of fathers (13.3%) were unemployed at the time of the survey compared with the proportion of mothers who were unemployed (8.3%). Participants also reported their family financial condition. Slightly more than 30% of participants (30.6%) reported that their family had low income (i.e., <1,000 RMB/month), and approximately 10% of the families were recipients of social welfare. A total of 6.3% of the sample reported having experienced cyberbullying victimization in the past year, and 22.2% reported cyberbullying victimization over their lifetime. Finally, more than 10% of participants reported having ever engaged in problem drinking (16.0%), cigarette smoking (14.0%), and/or gambling (10.3%).
Sample Characteristics Among 3,232 Chinese Adolescents.
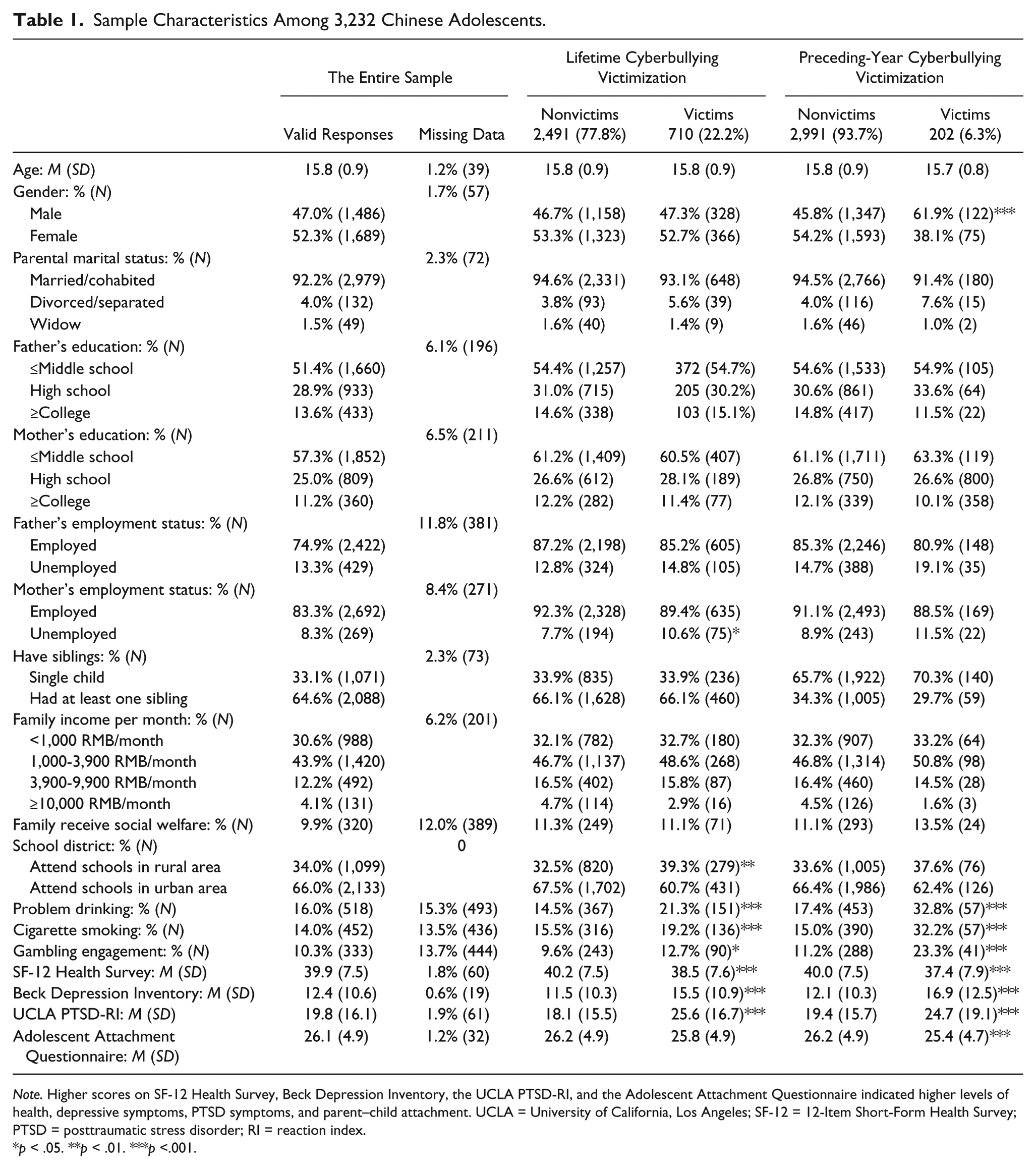
Note. Higher scores on SF-12 Health Survey, Beck Depression Inventory, the UCLA PTSD-RI, and the Adolescent Attachment Questionnaire indicated higher levels of health, depressive symptoms, PTSD symptoms, and parent–child attachment. UCLA = University of California, Los Angeles; SF-12 = 12-Item Short-Form Health Survey; PTSD = posttraumatic stress disorder; RI = reaction index.
p < .05. **p < .01. ***p <.001.
Bivariate tests revealed that adolescent males were significantly more likely to report cyberbullying victimization in the preceding year than their female counterparts, χ2(1) = 19.25, p < .001. Furthermore, adolescents who reported lifetime and preceding-year cyberbullying victimization, respectively, were significantly more likely to engage in problem drinking, χ2 lifetime (1) = 18.57, p < .001; χ2 past-year (1) = 25.89, p < .001); cigarette smoking, χ2 lifetime (1) = 20.22, p < .001; χ2 past-year (1) = 35.99, p < .001); and gambling, χ2 lifetime (1) = 5.54, p < .05; χ2 past-year (1) = 23.14, p < .001 compared with their nonvictimized peers. In addition, adolescents who reported lifetime and preceding-year cyberbullying victimization, respectively, reported significantly lower levels of overall health, tlifetime(3,131) = 4.91, p < .001; tpast-year(3,145) = 4.78, p < .001, and higher levels of depressive symptoms, tlifetime(3,166) = −8.87, p < .001; tpast-year(3,183) = −6.23, p < .001, and PTSD symptoms, tlifetime(3,130) = −11.12, p < .001; tpast-year(3,147) = −4.45, p < .001, compared with their nonvictimized peers. The significant difference in parent–child attachment was only observed between cyberbullying victims and nonvictims in the preceding year, with victims reporting significantly lower levels of parent–child attachment compared with their nonvictimized peers, t(3,160) = 2.26, p < .05.
Associations Between Cyberbullying Victimization and Health and Mental Health Problems
Table 2 presents the results of the OLS and binary logistic regressions that examine the effects of lifetime cyberbullying victimization on adolescents’ health and mental health problems after controlling for sociodemographic factors and parent–child attachment. The OLS regressions revealed that lifetime cyberbullying victimization was significantly negatively associated with participants’ scores on the SF-12 Health Survey (β = −1.58, p < .001) and positively associated with participants’ scores on the BDI (β = 3.74, p < .001) and the UCLA PTSD-RI (β = 7.16, p < .001). Binary logistic regressions revealed that lifetime cyberbullying victimization was significantly related to higher odds of problem drinking (odds ratio [OR] = 1.64, 95% CI = [1.31, 2.06]), cigarette smoking (OR = 1.69, 95% CI = [1.33, 2.16]), and gambling engagement (OR = 1.34, 95% CI = [1.02, 1.76]).
Effects of Lifetime Cyberbullying Victimization on Health and Mental Health Problems (N = 3,232).

Note. PTSD = posttraumatic stress disorder.
p < .05. **p < .01. ***p < .001.
Table 3 presents the results of the OLS and binary logistic regressions that examine the effects of preceding-year cyberbullying victimization on adolescents’ health and mental health problems after controlling for sociodemographic factors and parent–child attachment. The OLS regressions revealed that experiencing cyberbullying victimization in the past year was significantly negatively associated with participants’ scores on the SF-12 Health Survey (β = −2.22, p < .001), and positively related to participants’ scores on the BDI (β = 4.48, p < .001) and the UCLA PTSD-RI (β = 4.77, p < .001). Binary logistic regressions revealed that preceding-year cyberbullying victimization was significantly associated with higher odds of problem drinking (OR = 1.84, 95% CI = [1.30, 2.61]), cigarette smoking (OR = 2.21, 95% CI = [1.55, 3.16]), and gambling engagement (OR = 1.97, 95% CI = [1.34, 2.90]).
Effects of Preceding-Year Cyberbullying Victimization on Health and Mental Health Problems (N = 3,232).
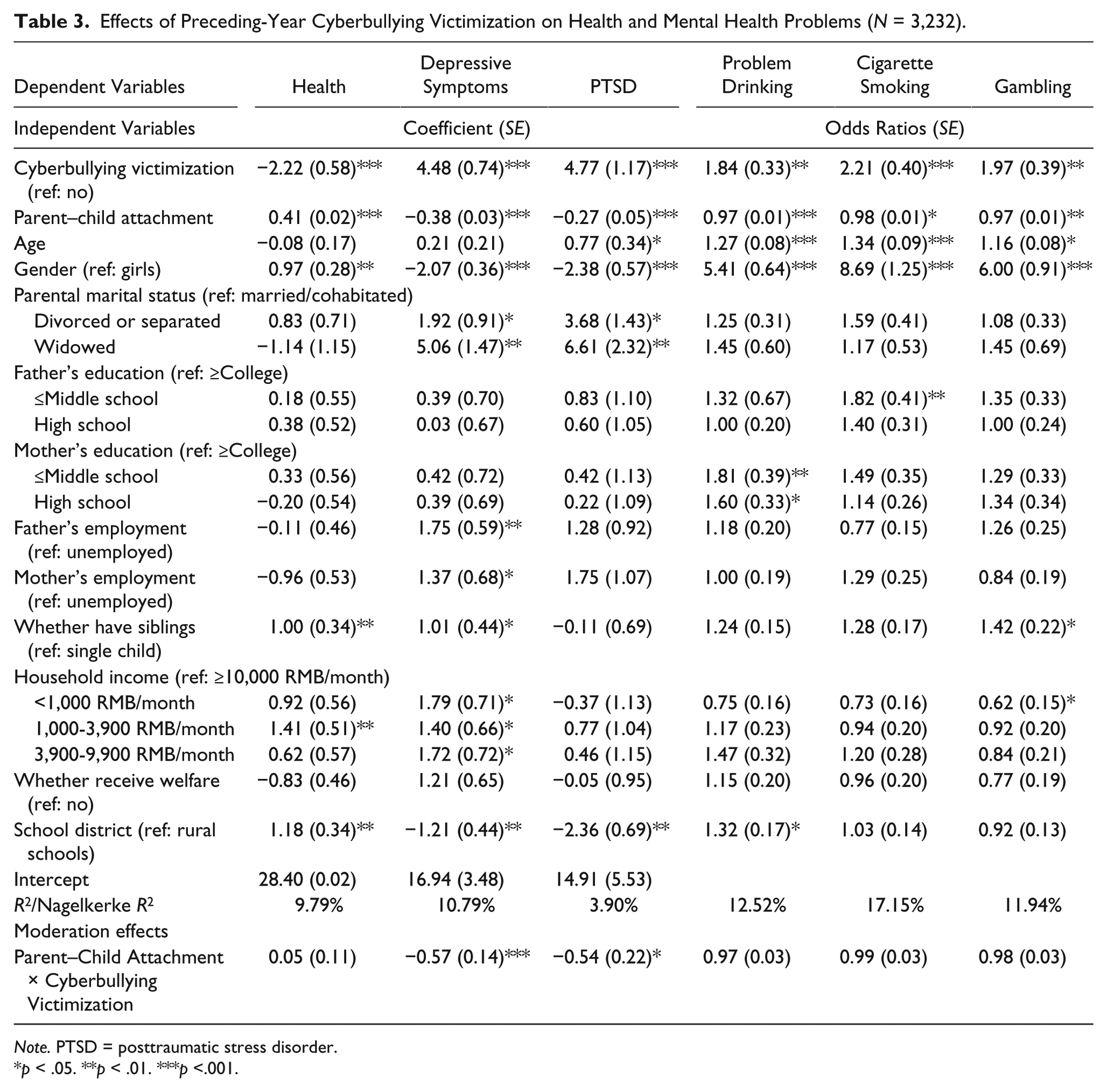
Note. PTSD = posttraumatic stress disorder.
p < .05. **p < .01. ***p <.001.
Moderation Effects of Parent–Child Attachment
Results revealed that parent–child attachment significantly moderated the effects of cyberbullying victimization on adolescents’ depressive symptoms and PTSD symptoms. Specifically, for those who had greater levels of parent–child attachment, the lifetime and preceding-year cyberbullying victimization, respectively, had significantly less effects on adolescents’ depressive symptoms (β lifetime = −.33, p < .001; β past-year = −.57, p < .001) and PTSD (β lifetime = −.40, p < .01; β past-year = −.54, p < .05) compared with those who had lower attachment scores. Significant moderation effect of parent–child attachment was not observed on the associations of cyberbullying victimization and adolescent’s overall health or addictive behaviors (p > .05) (Figure 1).

Parent–child attachment moderates the effects of lifetime cyberbullying victimization (figures on the left) and preceding-year cyberbullying victimization (figures on the right) on adolescents’ depressive and PTSD symptoms.
Discussion
Previous literature suggests that cyberbullying is prevalent among adolescents, and cyberbullying victimization may be associated with many negative psychosocial consequences among adolescents (Kim, Colwell, Kata, Boyle, & Georgiades, 2018; Tsitsika et al., 2015). Results of this study using a representative sample of adolescents in a major city in China demonstrated that cyberbullying victimization had significant negative effects on Chinese adolescents’ overall health, depressive symptoms, PTSD, substance misuse, and gambling behavior. Results of the current study also revealed that parent–child attachment might have attenuated the effects of cyberbullying victimization on certain outcomes among Chinese adolescents, including depressive and PTSD symptoms.
First, findings showed that cyberbullying victimization had negative effects on adolescents’ health and mental health. Cyberbullying victims reported significantly lower levels of overall health and higher levels of depressive symptoms and PTSD symptoms compared with their nonvictimized peers. These results suggest that adolescents in China who experience cyberbullying victimization might demonstrate similar health and mental health problems as adolescents in Western countries (Arslan, Savaser, Hallett, & Balci, 2012; Didden et al., 2009; Gámez-Guadix et al., 2013; Ranney et al., 2016). The current study assessed only cross-sectional relationships between cyberbullying victimization and mental health problems, including depressive symptoms and PTSD. These mental distress symptoms may, in turn, contribute to life stress among adolescents, including (re)victimization (Gámez-Guadix et al., 2013). Adolescents with depression and PTSD may lack adaptive coping, positive interpersonal skills, and supportive peer relationships, which may increase their problem Internet use and risk for experiencing cyberbullying (re)victimization (Gámez-Guadix et al., 2013; Li, Garland, & Howard, 2014). Future research using longitudinal data is needed to elucidate the bi-directional relationships of cyberbullying victimization and these mental health problems.
We also found that cyberbullying victimization was associated with adolescents’ addictive behaviors, specifically, substance misuse and gambling engagement. Adolescents who had experienced cyberbullying victimization in the current study were 70% more likely to engage in problem alcohol use, 65% more likely to engage in cigarette smoking, and 35% more likely to engage in gambling compared with their nonvictimized peers. Childhood victimization, including bullying victimization, has been found to be a significant etiological factor in the development of substance misuse and problem gambling (Blaszczynski & Nower, 2002; Kilpatrick et al., 2003). Adolescents who do not have adequate support and skills to cope with victimization may turn to substance use to escape from interpersonal stress and traumatic experiences (Mitchell et al., 2007). Also, adolescents who engage in deviant social behaviors, such as substance misuse, may experience more peer isolation and interpersonal conflict, which, in turn, intensifies cyberbullying involvement (Gámez-Guadix et al., 2013). Different from substance misuse, gambling is not often used as an avoidant or escapist coping mechanism (Blaszczynski & Nower, 2002). It is plausible that victims use gambling as a way to establish dominance. However, data in the current study could not assess the mechanisms underlying the association of cyberbullying victimization and gambling behavior. Future research is needed to better understand why some victims develop substance misuse, but others engage in different problem behaviors, such as gambling.
Informed by attachment theory (Bowlby et al., 1965), we found that parent–child attachment moderated the effects of cyberbullying victimization on adolescents’ depressive symptoms and PTSD. Cyberbullying victims with greater attachment to their parents had less severe depressive symptoms and PTSD compared with victims with lower levels of parent–child attachment. This finding contributes to the literature of cyberbullying by identifying an important protective mechanism of initial victimization, given that cyberbullying victims and nonvictims did not evidence different levels of parent–child attachment over the lifetime in this study. Positive parent–child attachment might have protected adolescents against initial victimization and reduced the negative effects of victimization (Claes, Luyckx, Baetens, Van de Ven, & Witteman, 2015; Lereya, Samara, & Wolke, 2013). Accordingly, adolescents with greater parent–child attachment might have been more likely to disclose their Internet use to their parents, and communicate with their parents when negative experiences (such as cyberbullying victimization) occurred. It follows that parents who were aware such victimization was occurring might have been more likely to provide timely interventions. These adolescents may have also been more likely to seek and obtain emotional support and/or problem-solving from parents directly after and/or during their experience of cyberbullying victimization. It is well-established that the effects of trauma naturally fade over time (Creamer, Burgess, & Pattison, 1992). Thus, it is likely that the parent–child attachment is not significantly different between lifetime cyberbullying victims and nonvictims not because it is not an important component of children’s lives, but because the symptomology of the trauma is reduced as a natural function of time.
The finding that parent–child attachment did not moderate the effects of victimization on health and substance misuse outcomes is complex. Health and substance misuse have a well-established link to mental health; however, the directionality is unclear. For example, it may be that the mental health problem precedes poor health and substance misuse (e.g., Khoury, Tang, Bradley, Cubells, & Ressler, 2010; Scott & Happell, 2011); however, it may also be that the mental health problem is an outcome of poor health and substance misuse (Scott & Happell, 2011). Given these complex and multidirectional relationships, it is not entirely clear what role cyberbullying victimization may take in mediating or moderating the relationships among mental health, health, and substance misuse. Future studies should explore these complex relationships closely, using longitudinal data to ascertain directionality and causation.
In addition to predeveloped research questions, the study found that more than 20% of adolescents in Xi’an had experienced some form of cyberbullying victimization in their lifetime. This finding suggests that there is likely a substantial number of adolescents in China who suffer from this issue. It is worth noting that this survey was conducted in 2009 to 2010 before smartphones and social media (e.g., QQ and WeChat) had become popular among adolescents in China. Therefore, this study might have underestimated the prevalence of cyberbullying victimization at present among adolescents in China. A more recent study found that nearly 45% of adolescents in China reported having experienced cyberbullying victimization in the past 6 months (Rao et al., 2019). Social media use may place adolescents at a greater risk of experiencing interpersonal stress and associated psychological and emotional aggression (Tokunaga, 2010). In addition, certain popular online video games (e.g., PlayerUnknown’s Battlegrounds) may facilitate an aggressive and violent environment that increases the risk of cyberbullying victimization for adolescents (Lam, Cheng, & Liu, 2013). Given the rapid development of technology and social media, the way that adolescents use the Internet and interact with other people on the Internet changes constantly, which may change the characteristics of cyberbullying. Consequently, timely research is needed to ensure research findings accurately reflect the realities of adolescents’ technology and Internet use.
Limitations
We urge readers to consider the results of the current study in the light of its limitations. A major limitation of this study is the adoption of a cross-sectional design, which precluded the temporal order of cyberbullying victimization and health and mental health problems; thus, the causality or directionality between cyberbullying victimization and health/mental health problems can only be speculated. Furthermore, this study used retrospective data that heavily relied on adolescents’ self-report, which may have potentially biased results. Specifically, adolescents may have misremembered past events in favor of social desirability. Third, although this study applied a stratified random sampling method, data were collected from adolescents that could only represent one major city in China (i.e., Xi’an), which might limit the generalizability of the findings. Finally, the dichotomized variables of cyberbullying victimization (adolescents who experienced any form of cyberbullying victimization vs. adolescents who did not experience cyberbullying victimization) marks potential differences in characteristics of victimization and associated problems caused by a variety of forms of cyberbullying. For example, adolescents who experience exclusion by others on the Internet may develop different levels of mental health problems compared with those who experience online sexual harassment. Further studies need to explore the health consequences of cyberbullying victimization by considering different forms of bullying on the Internet.
Implications
Despite these limitations, the findings have important implications for policy and practice. Given the prevalence rates and negative psychosocial consequences of cyberbullying victimization, there is a critical need to develop and implement prevention and early intervention programs that are tailored to address the needs of adolescents in China. Specific interventions that foster social support and address bullying behaviors on the Internet are needed. The current study found that parent–child attachment may be an important protective factor against some of the negative effects of cyberbullying victimization. Thus, parents need to be included in prevention and early intervention efforts. Specifically, educational information regarding parental monitoring of children’s technology use, and potential signs and symptoms of cyberbullying victimization, are needed. Such information can be provided to parents via social media platforms and at school-parent meetings. In addition, prevention and intervention programs need to emphasize the importance of open communication between parents and their children about cyberbullying involvement and other problem behaviors on the Internet. Schools need to provide policies, campaigns, and programs that facilitate positive technology use and supportive peer relationships. Finally, education and awareness campaigns on cyberbullying are needed for families, schools, and health professionals.
Footnotes
Acknowledgements
We are grateful to the Optimus Study which was initiated and funded by the UBS Optimus Foundation. Many thanks also go to Prof Ko Ling Chan from Hong Kong Polytechnic University, who authorized us to access to the original data and provided valuable comments on an earlier version of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by National Social Science Foundation of China (Grant No.:17CSH076).