
Abstract
Intimate partner violence (IPV) is a major public health concern. The prevalence of IPV in women in Kenya is in the range of 41% to 45% but has also been reported in 20% of men. The most widely used instrument for the screening and diagnosis of IPV is the World Health Organization–Intimate Partner Violence (WHO-IPV). However, it is lengthy for routine large-scale screening and is administered by a trained person, thus limiting the number it can reach for screening. There is therefore a need for a shorter screening version that can be self-administered to reach critical masses. Those who screen positive can then be subjected to the longer version. In addition, the short version should be culturally sensitive, can be used by either gender, can be used in busy clinical settings as the patients wait to be attended to, and can be used for large-scale community populations to raise awareness and promote help-seeking behavior. It should be applicable in similar cultural settings and is aligned to the longer version of the WHO-IPV instrument. This study aimed to develop such a tool. We administered the WHO-IPV to two groups: firstly, postnatal mothers attending postnatal clinics and secondly, men and women attending general clinics to which they had been referred. These referrals were by traditional healers (TH), faith healers (FH), and community health workers (CHW) who had been trained to screen for mental disorders using the Mental Health Gap Action Programme–Intervention Guide (mhGAP-IG) master checklist. Using factor analysis of the scores, we came up with questions that had the highest predictive value for different types of IPV diagnosis and which could therefore be used for self-screening purposes. We call the tool the Intimate Partner Violence–Brief Self-Screener (IPV-BSS; Adapted by the Africa Mental Health Research and Training Foundation from the WHO-IPV).
Introduction
Intimate partner violence (IPV) is defined as actual or threatened physical, sexual, and psychological abuse which includes controlling behavior by a current or former intimate partner (Centers for Disease Control and Prevention, 2012; World Health Organization [WHO], 2014). IPV is a major global health problem that is associated with the development of physical health problems such as respiratory, chronic pain, gynecological disorders, and also adverse pregnancy outcomes (Campbell, 2002; Humphreys, Cooper, & Miaskowski, 2011; Iverson et al., 2013). Furthermore, IPV, whether sexual, physical, or psychological, can lead to various long-term psychological consequences for victims such as anxiety, depression, symptoms of posttraumatic stress disorder, low self-esteem, suicidal behavior, emotional detachment, antisocial behavior and fear of intimacy (Mechanic, Weaver, & Resick, 2008; Overstreet, Willie, Hellmuth, & Sullivan, 2015; Pico-Alfonso et al., 2006; Semiatin, Torres, LaMotte, Portnoy, & Murphy, 2017). All the above consequences of IPV underscore the need for early screening, diagnosis, help-seeking, and intervention for victims of IPV.
Two systematic reviews on IPV have shown that Africa, specifically sub-Saharan Africa, has the highest burden of IPV (Shamu, Abrahams, Temmerman, Musekiwa, & Zarowsky, 2011; WHO, 2013). The Kenya Demographic Health Survey of 2014 showed the following: 45% of women aged 15 to 49 years experience either physical or sexual violence; more than 41% of Kenyan women experience sexual and/or physical violence by intimate partners in their lifetime; approximately 20% of Kenyan males experience episodes of violence before age of 18 years; and 31% of women experienced IPV in the previous 12 months with 90% of the perpetrators being males (Kenya National Bureau of Statistics, 2014).
Because of the huge burden and the associated negative health implications of IPV, there is the need to screen as many as possible of those at risk of IPV followed by a diagnostic procedure for those who screen positive. IPV screening tools currently in use are long, complex, or have not been tested in diverse nonclinical populations (Rabin, Jennings, Campbell, & Bair-Merritt, 2009). They also require a clinical specialist to administer them (Bair-Merritt et al., 2014; Rabin et al., 2009; Wenzel, Monson, & Johnson, 2004). Furthermore, most of the existing tools are appropriate to specific cultures and contexts and therefore not widely applicable because of the cultural and contextual differences of IPV (White & Satyen, 2015). Of the existing screening tools, Partner Violence Screen (PVS) is the shortest with three items and the Women Abuse Screening Tool (WAST) is the longest with eight items (Bair-Merritt et al., 2014; Rabin et al., 2009).
The World Health Organization–Intimate Partner Violence (WHO-IPV) screening and diagnostic instrument is an attractive instrument with the merit that it is a WHO tool designed to be applicable to wider cultural contexts (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). It is also likely to be embraced by WHO member states. However, it has the limitation that it is lengthy, despite its good psychometric properties (Chandra-Mouli, 2012; Jewkes, Fulu, Roselli, & Garcia-Moreno, 2013; Pallitto et al., 2013). There is a need for a shorter version screener, based on the WHO-IPV tool, based on the need for screening tools that are simple and culture appropriate (Bair-Merritt et al., 2014; Shamu et al., 2011).
Availability of such a version, that is brief, user friendly, gender sensitive, and culturally appropriate, can be easily self-administered, with inbuilt recommendation on when, depending on the scores, to seek for confirmatory diagnosis and possible management has the potential to reach critical masses in both clinical and community settings. This study primarily aimed to develop such an instrument based on the WHO-IPV long version tool.
Method
Study Design and Site
This was a cross-sectional descriptive study. The study was conducted in Makueni County in Kenya. It is one of the 47 counties in Kenya. It is located about 200 kilometers South East of Nairobi, the capital and largest city in Kenya. It lies astride the highway between Nairobi and Mombasa (the biggest port in East Africa). It is sparsely populated with about 1 million residents (51% females, 49% males), a population density of 124.9 people per km2, and a total of 186,478 households with an economy that is largely representative of other rural counties in Kenya (Government of Makueni County, 2018). At the time of the study, it had neither a psychiatrist nor a clinical psychologist. We chose Makueni County for two main reasons: first, it is among the majorly rural counties in Kenya and second, it embraced mental health and allowed testing a model for community mental health implementation strategy, with the full participation and support of the various stakeholders including policy makers (Mutiso, Gitonga, et al., 2018; University of Aberdeen, 2017) with potential for replication to similar social-cultural settings.
Recruitment of Participants
The participants from this study were recruited from two populations, identified from two previous research studies. Group 1 consisted of mothers visiting designated postnatal clinics with an infant aged less than 1 year, spoke the local dialect, Kamba, and were residents of the study site catchment communities within Makueni County (n = 544). Mothers visiting the postnatal clinics were systematically sampled such that every second mother on the queue was approached to participate in the study. This interval was computed by dividing the approximate population of postnatal mothers in the select health facilities by the required sample. This was done until the required sample was achieved. This first group was part of the study to determine the levels of depression in mothers attending mother–child clinics.
Group 2 included both women and men from the same county who had been referred for care at the study sites for suspected mental illness(es), on the basis of the Mental Health Gap Action Programme—Intervention Guide (mhGAP-IG) based screener (WHO, 2010); men (n = 2,862) and women (n = 5,448). Participants were screened by community health workers (CHW), faith healers (FH), traditional healers (TH), family, and friends, as well as clinicians for suspected mental health conditions and referred to a health facility for confirmatory diagnosis (Mutiso, Gitonga, et al., 2018; Mutiso, Musyimi, et al., 2018). This group included all the participants whether or not they met the M.I.N.I. Plus (van Vliet & de Beurs, 2007) criteria for a Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994)/International Classification of Diseases–10th Revision (ICD 10) diagnosis. This second group was part of a bigger community-based study on feasibility of implementation of mhGAP-IG (Mutiso, Gitonga, et al., 2018). Both groups were approached to participate in the study. In both groups, trained research assistants administered the measures to the participants in the language they were comfortable with.
Measures
These were administered by trained and supervised research assistants.
Sociodemographic characteristics
We used a self-administered sociodemographic questionnaire to capture respondent’s profiles and characteristics. These included gender, age, marital status, and level of education—divided into four categories: no formal education (i.e., never went to school), primary education (1-8 years of formal education), secondary education (1-4 years postprimary education), and tertiary/university education.
Employment status included those who had no jobs, were either self-employed or working for somebody else or organization.
IPV
The WHO Women and Life Questionnaire has been tested and found to have good properties in collecting data on experience of IPV across various cultural settings (Garcia-Moreno et al., 2006). This instrument has four dimensions: physical, sexual, emotional, and controlling behavior. Furthermore, it has a number of statements that link exposure to each form of violence: five for physical violence, three for sexual violence, four for emotional violence, and six for controlling behavior. Each of the statements had three answer options: (a) “no” for no lifetime exposure, (b) “yes” for experience, and (c) “not applicable” for participants who had never had an intimate partner.
Statistical Analysis
Data reduction techniques summarized the observed IPV variables into a few dimensions using principal component analysis (PCA). Component internal consistency and the reliability for the overall screen for each domain were used for selecting IPV variables, by calculating Cronbach’s alpha.
Before performing a factor analysis, the correlation matrix was inspected to check for the strength of correlation. Then factorability was tested using the explanatory factor analysis (Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity. Factor analysis using PCA with varimax rotation was carried out to determine the dimensional structure IPV experience using the following criteria: (a) eigenvalue > 1 (Kaiser, 1960), (b) variables should load >0.50 on only one factor and on other factors <0.40, (c) the interpretation of the factor structure should be meaningful, and (d) screen plot is accurate in the case that the means of communalities are above 0.60 (Hakstian, Rogers, & Cattell, 1982). Computations were based on covariance matrix as all variables were receiving values from the same measurement scale (Morrison, 2005). A Bartlett’s test of sphericity with p < .05 and a KMO measure of sampling adequacy of 0.6 were used in performing this factor analysis. A factor was considered as important if its eigenvalue exceeded 1.0 (Kaiser, 1960). Pairwise associations between the items corresponding to 2 × 2 contingency tables for all possible pairs were computed. Factor scores were then generated for each item. Items with the highest loadings were considered to the most important factor as they explained most of the observed variance (Thompson, 2004). The process used to identify items for the brief scale was iterative, with the reliability of the final set of items tested using Cronbach’s alpha. All the data analysis was done using the Statistical Package for Social Sciences (SPSS) version 23.
Results
Sociodemographic Characteristics
Table 1 summarizes the sociodemographic characteristics of postpartum mothers. The mean age was 26.8 years, and the range was from 18 to 44 years. More than three quarters (77.9%) were married. Nearly 40.8% had a primary and below level of education, whereas 43.6% had a secondary level of education, and the remaining15.6% had a tertiary level of education.
Sociodemographic Characteristics of Postpartum Women in Rural Kenya (Group 1; n = 544).

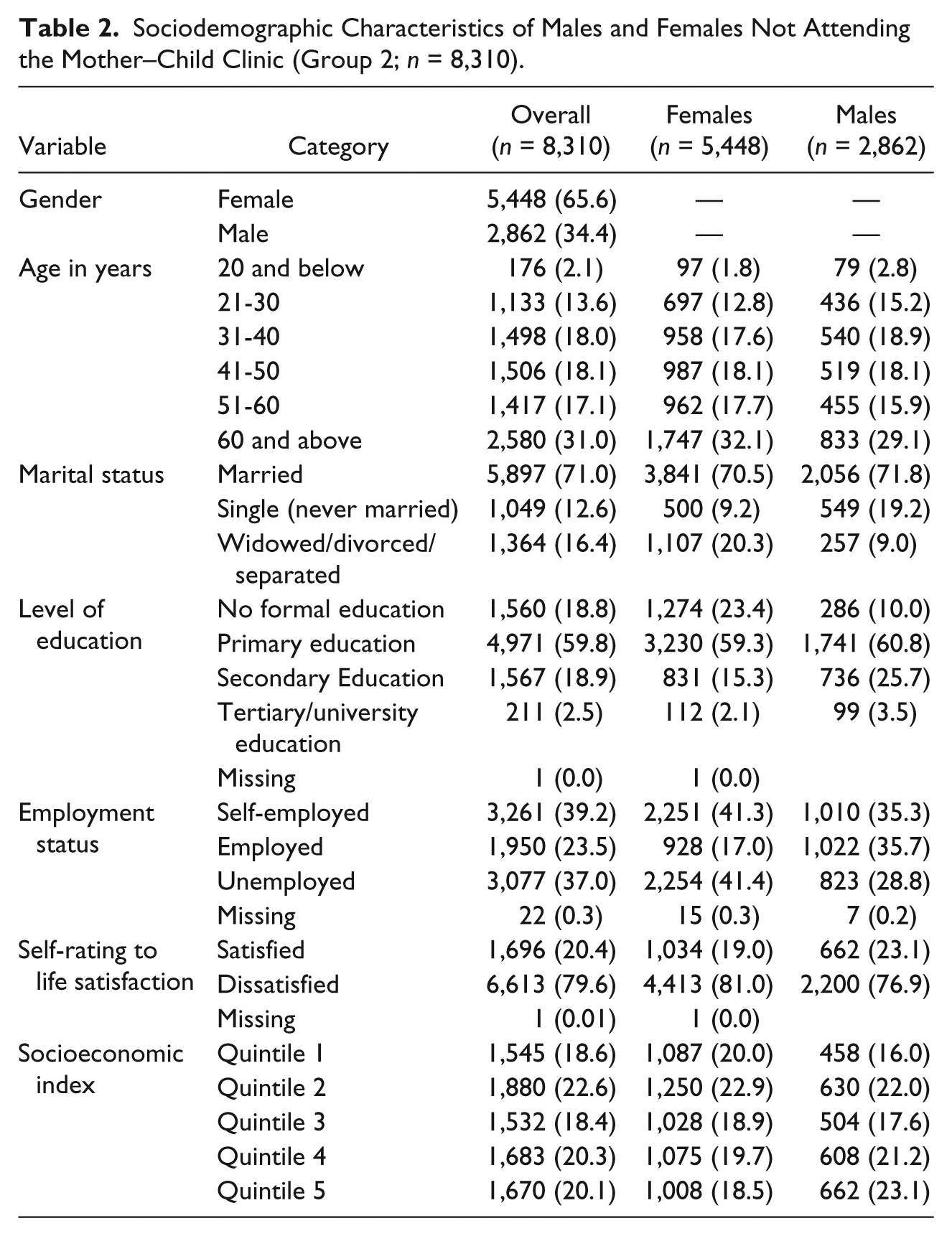
The sociodemographic characteristics of the males and females not attending the mother–child clinics are summarized in Table 2. Two thirds of these were females. Nearly one third (31%) of all the participants were aged 60 years and above. More than three quarters had primary or less level of education. More females than males were self-employed and vice-versa for the employed. Females were more dissatisfied with life than males, and both genders were more dissatisfied than satisfied with life. Males had higher level of economic status than females.
Sociodemographic Characteristics of Males and Females Not Attending the Mother–Child Clinic (Group 2; n = 8,310).
Factor Analysis
After performing factor analysis using PCA on all items, controlling behaviors items loaded heavily on Factor 1. This explained most of the variance in all the subset population of men, women, and postnatal mothers. The eigenvalues for all Factor 1 for postnatal mothers, women, and men were greater than 5.6. Therefore, contributing to a total variance of around 31% of the entire subset population. The reliability (Cronbach’s α) of this scale was .85 in all the subset population.
Men, women, and mothers had different highest scores for items regarding their partners: (a) “Is often suspicious that you are unfaithful” item ranked highest among men, (b) “Got angry if you speak with another man/woman” ranked highest for women, and (c) “Tried to keep you from seeing your friends” ranked highest for mothers as summarized in Table 3.
Individual Factor Loading on Items of WHO-IPV Tool.

Note. WHO-IPV = World Health Organization–Intimate Partner Violence.
To determine the most important factors, we conducted further factor analysis of the individual subscales shown in Table 2. We found,
These findings are summarized in Table 4.
Individual Factor Loading on Items of Subsets of Domains of WHO-IPV Tool.

Note. WHO-IPV = World Health Organization–Intimate Partner Violence.
To develop a brief screening test, we picked social demographic characteristics that emphasized a history of intimate relationship, and for females, we picked obstetric history.
We picked the IPV questions that accounted for the highest variance for each of the study groups for controlling behavior and sexual physical and emotional abuse. The proposed screening tool is presented as Appendix.
Discussion
We present a study that has led to the first screening test of IPV (i.e., IPV-BSS) in Kenya and the region. It has the potential for mass screening of IPV in clinical and community settings. It has inbuilt recommendation on when to go for further diagnosis and management. It is socioculturally context appropriate and may find use in other similar social-cultural contexts. We paid attention to adequate statistical analysis to justify the selection and inclusion of minimum items from the longer WHO-IPV screening and diagnostic tool to constitute the IPV-BSS.
When all the items in the WHO-IPV instrument were included in the analysis, we found that the items assessing controlling behavior in a partner accounted for the most variance. Further studies are required in the Kenyan context to determine the directionality of controlling behavior. However, several studies have reported similar findings to ours to the effect that people who reported controlling behaviors were more likely to experience psychological and physical violence and that controlling behaviors were a precursor to other forms of violence (Aizpurua, Copp, Ricarte, & Vázquez, 2021; Antai, 2011). The same was noted by the developers of the WHO-IPV that controlling behavior should be considered as a starting point in screening for IPV (Garcia-Moreno et al., 2006).
Other screening tools recorded an average of 4.2 items (Coker, Pope, Smith, Sanderson, & Hussey, 2001; Wenzel et al., 2004), whereas the WHO-IPV screener has eight items with a total of 22 questions (Garcia-Moreno et al., 2006) and the WAST has eight items (Bair-Merritt et al., 2014; Rabin et al., 2009). PVS with three items compares favorably with our WHO-IPV based IPV-BSS which has four items namely (a) controlling behavior for all groups, (b) unwilling sexual intercourse, (c) physical abuse, and (d) emotional abuse. However, there are variations within these items depending on whether male, female, or mothers. It has already been reported that single items perform inconsistently in their ability to identify IPV victims (Peralta & Fleming, 2003; Wasson et al., 2000). In our study, we did not find a single item that could be applied across the board.
Despite different sociodemographics and mental health profiles both within and across the cohorts, there were similarities and overlaps in the responses to questions on (a) physical and emotional abuse for all mothers attending mother–child clinic, (b) sexual violence for all female cohort not attending mother and child health clinic (MCH) and the male cohort (Study Group 2), and (c) sexual abuse in all mothers and the other cohorts. Some of the females in the Group 2, though not recruited from MCH, might have been attending antenatal or postnatal clinics. Thus, we have a good mix of study participants but similar results across the cohorts. Therefore, our design to use three categories of patients—postpartum mothers, males, and nonpostpartum females—had two main advantages: (a) it served to identify commonalities across the groups and categories and (ii) it broadened the scope for the application of IPV-BSS. This design was therefore a strength rather than weakness or flaw in our study. The implication of this is that the IPV-BSS can be applied as a self-screener for both males and females.
To maximize on widespread applicability, reach to critical masses, and utilize IPV-BSS, we recommend the following: (a) IPV-BSS can be uploaded on applications in English or local dialects, so that people can screen themselves in their own privacy; (b) IPV-BSS in both English and local dialects should, on a priority basis, be made freely and widely available to all mothers attending prenatal and postnatal clinics as IPV in mothers can also have harmful effects on their babies; (c) Brochures of IPV-BSS should be freely available in English, Swahili (lingua franca), and local dialects in all adult clinics attending for services at dispensary and health centers where the majority of people seeking medical help in Kenya are seen; (d) To meet the potentially high demand for help, staff managing the health facilities should be trained to handle any referrals for help as a result of (a) to (c) above to confirm diagnosis and initiate management; and (e) FHs and THs should be educated to provide social support as first aid and refer when necessary substantial number of people who are victims of IPV. This is because IPV victims are likely to consult their religious leaders or their traditional practitioners as their first point of care, in health-seeking behavior (Mutiso, Musyimi, et al., 2018).
The full WHO-IPV scale which has well-established psychometric properties can still be used as a fallback for those who need to know the full range of IPV, either for themselves or by the care providers who provide the management. The benefits of full diagnosis include informed management. The benefit of management is amelioration or prevention of the full negative impact of IPV on the victims and, in the case of mothers, the harmful effects on unborn and born babies. The negative and harmful effects have been described in our “Introduction.” Furthermore, management of IPV has the potential to improve emotional relationships within families and, by extension, the children.
We conclude that IPV-BSS is an appropriate tool that has the potential for use in large-scale clinical and community-based screening for IPV, with provision for confirmation and management in a Kenyan setting. It is short, the included questions are direct, simple, and only require a “yes” or “no” answers and can therefore be easily self-administered. It is appropriate for either gender. It has potential to reach critical masses in enhancing awareness, screening, and promoting health-seeking behavior for confirmation of diagnosis and management. We have thus achieved our purpose of developing a culturally appropriate local brief version (IPV-BSS) of the WHO-IPV.
Limitations
There are several limitations in our study. The most important of this is that we did not study the psychometric properties of the proposed IPV-BSS. This is still needed despite the fact that it was derived from the widely used WHO-IPV and also despite the fact any positive screens would still be subjected to the full WHO-IPV instrument. Another limitation is that, the participants drawn from the general facilities and not the female from MCH Clinic included individuals who had screened positive on mhGAP-IG (but not confirmed). Therefore, they do not reflect a random sample of the general population. In mitigation to this limitation, several studies have suggested that majority of IPV victims have depression and other forms of comorbid mental disorders, that is, there is a high comorbidity of IPV and mental health disorders (Jonas et al., 2014; Lagdon, Armour, & Stringer, 2014). Therefore, by extension, IPV-BSS will be used in people with mental illness. Another limitation is that only postnatal mothers with children less than 1 year were sampled. However, as already explained in our discussion, the women from the general facilities cohort could also have been at various stages of pregnancy or postnatal period. Finally, there is a limitation that IPV-BSS may not be applicable in sociocultural contexts that are different from our study site. In mitigation, most rural settings in Kenya and other low and middle income countries (LMICs) have more similarities than differences. Overall and more significantly, our findings are similar to other findings, even from high income countries (HICs) but using instruments other than WHO-IPV.
Footnotes
Appendix
Acknowledgements
The authors acknowledge the Government of Makueni County for their logistical support during the implementation of this study. We are also grateful to Ruth Wambui, Darius Nyamai, Rubie Miseda, and Grace Mutevu of Africa Mental Health Research and Training Foundation (AMHRTF) and Nicole Khauli of Columbia University for their valuable editorial inputs in the course of drafting the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grand Challenges Canada (GCC; grant: 0739-05).
Ethical Approval
Ethical approval for this study was obtained from Maseno University–Ethics Review Committee (MU-ERC). Informed consent was obtained from all individual participants included in the study. Data were coded with no personal identifiers.