
Abstract
Women’s experiences of intimate partner violence (IPV) from their male partners can include psychological, physical, and sexual control and abuse. The psychological effects of abuse (PEA) include terror, shame, and loss of power and control in relationships. While women’s experiences of IPV are associated with decreased condom use, limited research has examined the impact of PEA on women’s condom use. Intoxicated (breath alcohol content [BrAC] = .10%) versus sober women were evaluated to test the hypothesis that PEA would interact with intoxication and scenario-context partner pressure to forgo condom use and be associated with intentions to engage in condomless sex. After beverage administration, community women (N = 405) projected themselves into a computerized scenario depicting a male partner exerting high or low pressure for condomless sex. In-the-moment condom negotiation self-efficacy and condom-decision abdication—letting the man decide on condom use—were assessed. Path analysis examined the direct and indirect effects of PEA, alcohol, and partner pressure conditions on condomless sex intentions. PEA increased condomless sex intentions indirectly through decreased condom negotiation self-efficacy. Intoxication increased condomless sex intentions indirectly through decreased condom negotiation self-efficacy and increased condom-decision abdication. Intoxicated women in the low pressure condition were more likely to abdicate the condom decision than women in the high pressure condition. Women who have experienced greater PEA may benefit from interventions focusing on how condom negotiation self-efficacy, condom-decision abdication, and intoxication influence sexual decision-making.
Intimate partner violence (IPV) is a significant public health problem with lifetime prevalence rates ranging from 20% to 55% for women in the United States (Breiding, Black, & Ryan, 2008; Coker, Smith, McKeown, & King, 2000). These estimates vary significantly due to the different types of IPV assessed, including physical and psychological abuse, sexual assault, and reproductive coercion, which involves a partner’s attempts to promote pregnancy through verbal pressure and threats, interference with contraception including control of condom use, and control of pregnancy outcomes (e.g., continuation or termination of pregnancy; Miller & Silverman, 2010). Types of IPV can be measured individually or in combination, and are usually measured by assessing specific behavioral acts inflicted by one intimate partner on another (Rogers & Follingstad, 2014). IPV can also include the use of control, monitoring, isolation, threats, jealousy, manipulation, treating one as an inferior, or creating a hostile environment (Follingstad, 2011). Prior research suggests that this process of intimidation, coercion, and control is “not synonymous with experiencing violent attacks” (Ferraro & Johnson, 1983). Operationalizing IPV only by the frequency of specific behavioral acts of physical, psychological, and/or sexual and reproductive abuse (Rogers & Follingstad, 2014) may not capture the context of continuous intimidation and coercion that women experience in violent relationships. Psychological effects of abuse (PEA) refers to the perceived loss of power and control in relationships, perceived experience of coercive and controlling behavior that accompanies IPV, and perceived vulnerability to danger. More research is needed to examine how this ongoing vulnerability to coercion and control is associated with sexual risk decisions.
Although scant research has investigated the association between PEA and sexual risk behavior, women with IPV histories exhibit greater sexual risk behaviors, including a greater likelihood of having a sexually transmitted infection (STI) and less condom use compared with women without IPV histories (Wingood & DiClemente, 1997). Even when women want to use condoms, those endorsing more severe PEA may be more likely to engage in sexual risk-taking, especially if their male partners use pressure to obtain condomless sex. Women who have experienced more severe PEA may feel less efficacious at negotiating for condom use and may be more likely to abdicate the condom decision to their partners. Alcohol intoxication is also associated with increased sexual risk behaviors, including condomless sex, for women with sexual violence histories (Masters et al., 2014). However, the role of alcohol in sexual decision making has not taken PEA into account. Thus, the goal of our study was to examine the association among women’s PEA, condom negotiation self-efficacy, and decisions regarding condom use with a male partner in the context of acute intoxication and partner pressure.
Partner Pressure, Condom Negotiation Self-Efficacy, and Condom-Decision Abdication
Research on the effect of partner pressure has predominately focused on pressure for sex more generally (e.g., Jones, 2006; Teitelman, Ratcliffe, & Cederbaum, 2008) and not specifically pressure for condomless sex. Pressure to engage in condomless sex is inherently different because it is possible for a woman to consent to sex with a condom but not to sex without a condom. Verbally pressuring women to having condomless sex is also perceived as normative by some men (Davis et al., 2014b; Davis et al., 2014c). Pressure to engage in condomless sex can increase a woman’s likelihood of ceding decisional agency through sexual abdication (letting the male decide generally how far to go sexually) or condom-decision abdication (letting the male decide specifically whether or not to use a condom; George et al., 2016). Experimental research has demonstrated that abdicating the decision about condom use is associated with greater condomless sex intentions (Masters et al., 2014). Because condom-decision abdication is related to a greater likelihood of sexual risk-taking, several studies have investigated potential risk factors that may increase its occurrence.
One possible risk factor for condom-decision abdication is low self-efficacy for condom negotiation. Self-efficacy refers to the belief that one can successfully execute a desired behavior and is a powerful predictor of health behaviors, including condom use (Bandura, 1990; Xu, Chen, Yu, Joseph, & Stanton, 2017). Condom negotiation self-efficacy, or the belief that one can successfully negotiate condom use with a partner, has been associated with condom use when it has been examined as both a background characteristic and as an in-the-moment process (Crosby et al., 2013; Stappenbeck et al., 2016).
Research indicates that women’s IPV victimization is associated with both decreased condom negotiation self-efficacy and a higher likelihood of abdicating condom use decisions to their male partners (e.g., Swan & O’Connell, 2012). Masters and colleagues (2014) found that having a history of sexual victimization may in part increase abdication likelihood through an increased anticipation that the partner will react negatively to the woman’s request to use a condom. However, this particular study did not include a partner asserting pressure to avoid condom use. Qualitative investigations with HIV-positive communities have found both physical and psychological IPV histories were associated with less ability to negotiate safe sex practices including condom use (Lichtenstein, 2005). In a study of adolescent and young adult women recruited from family planning clinics, reproductive coercion was associated with decreased condom negotiation self-efficacy (Jones et al., 2016), and other studies have found associations among IPV victimization and condom use self-efficacy (Quina, Harlow, Morokoff, Burkholder, & Deiter, 2000). Together, these studies suggest that victimized women’s perceptions of their ability to negotiate for and use condoms may be related to their condom-decision abdication.
Alcohol and Condomless Sex
Alcohol intoxication has also been demonstrated as a risk factor for condom negotiation self-efficacy and women’s condom-decision abdication. Extant literature suggests that alcohol intoxication is associated with decreased self-efficacy to use condoms (for review, see Abbey, Parkhill, Buck, & Saenz, 2007). Individuals with low characteristic self-efficacy to use condoms are less likely to engage in condom negotiation when they have consumed alcohol prior to sex (Davis et al., 2014a). Alcohol intoxication has also been demonstrated as a risk factor for women’s condom-decision abdication. Acute intoxication can directly increase women’s intentions to abdicate condom use decisions to their partners (Masters et al., 2014), as well as moderate the effects of relationship factors and individual characteristics on women’s abdication intentions (Zawacki et al., 2009). George and colleagues conducted an experiment to examine the effects of alcohol intoxication and partner pressure on condomless sex intentions in a hypothetical sexual scenario (George et al., 2016). In the sober condition, sexual assault severity was positively associated with likelihood of condom-decision abdication intentions when pressure to engage in condomless sex was exerted. Yet, it is unknown whether a similar pattern exists for women who have experienced coercive or controlling behaviors within an intimate relationship or whether this pattern is related to PEA.
Study Overview and Hypotheses
The present study utilized a 2 (alcohol condition: no alcohol vs. target peak BrAC of .10%) × 2 (partner pressure condition: low vs. high) experimental design (i.e., no alcohol/low pressure, no alcohol/high pressure, alcohol/low pressure, alcohol/high pressure) to examine the effects of PEA, alcohol intoxication, and pressure from a male partner on a woman’s intentions to engage in condomless sex with a hypothetical male partner in response to an eroticized hypothetical sexual scenario. In addition, we examined whether condom negotiation self-efficacy and condom-decision abdication mediated the association between PEA and condomless sex intentions. Given the public health priority to reduce the prevalence of STIs and unwanted pregnancies (World Health Organization, 2016), the present study included women identified as at risk of STIs and/or HIV. Employing a path analysis framework, the hypothesized model (see Figure 1) proposes that PEA will be positively, directly associated with intentions to engage in condomless sex (Hypothesis 1). We anticipate PEA will also indirectly increase condomless sex intentions through decreased condom negotiation self-efficacy and increased condom-decision abdication (Hypothesis 2). We predict intoxicated women will report greater condomless sex intentions (Hypothesis 3a) and that alcohol will have an indirect effect on condomless sex intentions through condom negotiation self-efficacy and condom-decision abdication, such that intoxicated women will report less condom negotiation self-efficacy and this will in turn be associated with higher condom-decision abdication relative to sober women (Hypothesis 3b). To examine the moderating effects of alcohol intoxication on the relationship between PEA and condom use, we explored the interactive effects of alcohol and PEA on the dependent measures. Finally, we predict that women in the high pressure condition will report greater condomless sex intentions, lower condom negotiation self-efficacy, and greater condom-decision abdication intentions than women in the low pressure condition (Hypothesis 4). We also explored the interactive effects of partner pressure and PEA on the dependent measures, as well as the interaction of alcohol and partner pressure on dependent measures.
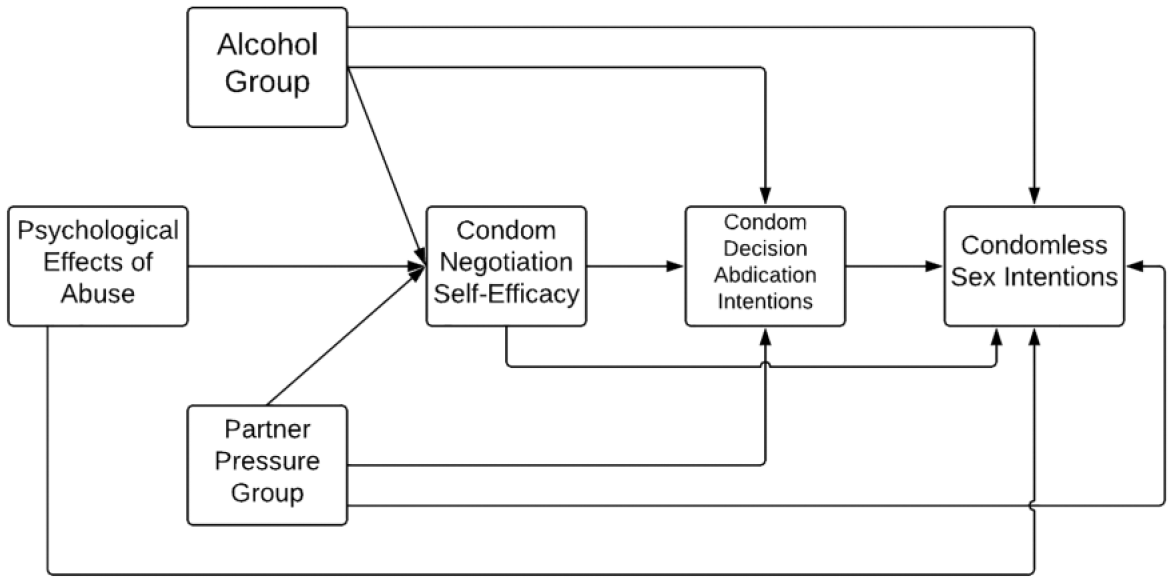
Hypothesized model.
Method
Participants
Participants were recruited from an urban community with online and print advertisements soliciting single female drinkers aged 21 to 30 to participate in a research study focused on women’s sexual victimization experiences and social drinking. The age-related inclusion criterion was used due to the increased incidence and prevalence of STIs within young adult compared with older adult populations (Centers for Disease Control, 2018). To recruit a sample at higher risk of STIs, advertisements were placed in STI clinics. To facilitate recruitment of a racially and ethnically diverse sample, advertisements were placed in publications typically marketed to racial and ethnic minority communities. Consistent with the National Institute on Alcohol Abuse and Alcoholism’s (NIAAA) guidelines on the ethical administration of alcohol (NIAAA, 2004a), eligible women had consumed at least five drinks per week and had at least one occasion of heavy episodic drinking (four or more drinks in a 2-hr time period; NIAAA, 2004b) in the past year. Consistent with the goal of examining a sample at risk of STIs, eligible women had at least one instance of condomless sex in the past year while concurrently having at least one additional STI/HIV risk factor (see George et al., 2016). Women were excluded from participating if they had contraindicated medical conditions or prescription medication use, negative reactions to alcohol, or a history of problem drinking assessed by the Brief Michigan Alcohol Screening Test (BMAST; Pokorny, Miller, & Kaplan, 1972). Participants were paid US$15 per hour and compensation ranged from US$45 to US$150. The final data set included 405 women (M = 24.7 years, SD = 2.79). Descriptive statistics for the sample are found in Table 1. It should be noted that not all 405 included participants completed all demographic measures.
Sample (N = 405) Descriptive Statistics.

Procedures
The University Human Subjects Division approved all study methods. Interested women responded to print and online advertisements by calling in to be screened for eligibility by a trained female research assistant and, if eligible, were scheduled for an appointment. Upon arrival at the laboratory, a trained female research assistant confirmed the participant’s BrAC was .00% with a handheld breathalyzer (Alco-Sensor IV; Intoximeters, Inc.), confirmed each participant was not pregnant via a self-administered urine test, and obtained informed consent. The informed consent document included examples of some of the most sensitive and potentially distressing questions assessing past victimization history. Although this did not occur throughout the duration of data collection, in the event that a participant became distressed by the questions or procedure, a licensed clinical psychologist was supervising and available. Participants were weighed to determine their alcohol dose (see below). Participants then completed background questionnaires about their demographics, sexual experiences, drinking habits, PEA, and history of sexual victimization in a private room on a computer. This portion took approximately 1 hr to complete. Participants were randomized into one of four conditions of alcohol consumption (no alcohol/alcohol) and pressure by the male character to have sex without a condom (low/high). The study employed a double blind design to participants’ story condition such that neither participant nor research assistant knew to which pressure condition the participant was assigned. Participants were informed at multiple points throughout the protocol that they were free to withdraw from the study at any time and without penalty.
All drinks were prepared and administered by trained female research assistants. Participants in the alcohol condition consumed beverages consisting of five parts cranberry juice and one part 190-proof grain alcohol, dosed at 1.0 ml per kg of body weight. Participants in the control condition consumed cranberry juice only, but the volume of liquid that they consumed was equivalent to that consumed by participants in the alcohol condition. The beverages were divided into three equivalent portions that were each consumed over a 4-min period, followed by a breathalyzer test every 4 min until a criterion BrAC level (alcohol group = .07%) was attained, assuring that the participant read the scenario and completed measures on the ascending limb of the alcohol biphasic curve. There are individual differences in speed of alcohol absorption (Schacht, Stoner, George, & Norris, 2010). To control for these differences, each control participant was yoked to an alcohol participant and received the same number of breath samples over the same number of minutes as the alcohol participant (Schacht et al., 2010). Once alcohol participants reached the criterion BrAC or control participants completed the yoked number of breathalyzer tests, they read an eroticized hypothetical sexual scenario.
The sexual scenario depicted a sexual encounter between a female protagonist (the participant) and a hypothetical male partner, “Michael,” with whom the participant was in a dating relationship and whom she had previously had sex with while using a condom. The scenario was written in the second person and participants were instructed to project themselves into the story (e.g., “Imagine that you are the person being described in the scenario and try to put yourself in the situation”; [for a detailed description of instructions, see George et al., 2016]. The story indicated that the participant was on oral contraceptives, and progressed from a date with Michael to consensual sexual activity. Descriptions and dialogue were eroticized to elevate the participants’ sexual arousal. Participants were randomized to a scenario manipulation in which Michael applied either high or low pressure to have condomless sex when a condom was readily available. In the low-pressure condition, Michael indicated a preference to have condomless sex but stated that the participant/protagonist could make the decision. In the high-pressure condition, Michael indicated that if the protagonist wanted to continue the relationship, they should have condomless sex. These scenario characteristics were based on similar experiments reported on in the past George et al., 2016; however, the pressure manipulation in the present study is novel to this experiment. The scenario was developed using data from focus groups on young women’s casual sexual relationships and condom use, and it was pilot tested to ensure realism. Participants completed two realism questions regarding how likely they were to behave as described in the story (M = 5.29, SD = 1.51; 1 = not at all likely to 7 = extremely likely) and how realistic they perceived the situation in the story (M = 5.86, SD = 1.33; 1 = not at all realistic to 7 = extremely realistic).
Measures
PEA
Women’s lifetime PEA by a male intimate partner was assessed utilizing the Women’s Experiences with Battering Questionnaire, a 10-item measure evaluating perceptions of male partners’ coercive and controlling behaviors (Smith, Earp, & DeVellis, 1995). To capture the range of PEA that participants may have encountered with different partners, participants were instructed to rate how much they agreed or disagreed with 10 statements about any past or current relationships, using response scales (1 = agree strongly to 6 = disagree strongly) which were then reverse-scored such that a low score (10) indicates low levels of PEA and a high score (60) indicates high levels of PEA. Rather than specify the type of abuse that one has experienced (e.g., physical, psychological, or sexual), items assess the psychological impacts of abuse, such as vulnerability to danger and loss of power and control in the relationship. Example items include “My partner made me feel unsafe even in my own home,” “My partner could scare me without laying a hand on me,” and “My partner made me feel like I had no control over my life, no power, no protection.” These items demonstrated excellent reliability (α = .95) and were added to compute a sum score.
In-the-moment condom negotiation self-efficacy
To measure participants’ self-efficacy to negotiate using a condom in-the-moment, participants were asked three questions as to how confident (1 = not at all to 7 = extremely) they felt they could insist upon condom use (e.g., “How confident do you feel that you could insist Michael to use a condom?”). Condom negotiation self-efficacy was computed as the mean of these three items and possessed excellent reliability (α = .92). These items were modified from the Condom Influence Strategy Questionnaire (Noar, Morokoff, & Harlow, 2002).
In-the-moment condom-decision abdication intentions
The woman’s intentions to abdicate the condom use decision to her male partner were evaluated with two items. Participants indicated their likelihood (1 = not at all likely to 7 = extremely likely) of “letting Michael decide whether or not to use a condom” and “going along with what Michael wants about not using a condom” (α = .90). Abdication intention was computed as the mean of these two items. These items were modified from research examining general sexual abdication (Masters et al., 2014).
In-the-moment condomless sex intentions
Women’s intentions to engage in condomless sex with the man in the scenario were assessed through three items measuring the likelihood (1 = not at all likely to 7 = extremely likely) of having condomless vaginal–penile contact with Michael. We computed the average condomless sex intentions score through a mean of these items, which had good reliability (α = .87). These questions have been used in prior research to assess women’s condomless sex intentions in similar hypothetical scenarios (e.g., George et al., 2009; Masters et al., 2014). Prior research suggests that sexual risk-taking behavioral intentions correspond to real-world sexual risk-taking (Kajumulo, Davis, & George, 2009; Norris, Kiekel, Purdie, & Abdallah, 2010).
Data Analytic Approach
Path analysis with Mplus statistical modeling software (Muthén & Muthén, 1998 [2017]) was utilized to examine the hypothesized model depicted in Figure 1. Working within a model generating framework (Byrne, 2011; Jöreskog, 1993), we began with the most parsimonious model consisting of main effects. We expanded to a more complex model in which the two-way and three-way interactions were included to test the interaction effects of the alcohol condition, partner pressure condition, and PEA. PEA was centered. Using the preliminary analyses and extant literature (Davis et al., 2014a; Woolf-King & Maisto, 2015) as guidelines, the interactions were regressed on condomless sex intentions, condom-decision abdication intentions, and condom negotiation self-efficacy. Per the model generation framework, we then fixed all nonsignificant paths to zero and reran the model. Goodness of model fit was indicated by a nonsignificant chi-square test, root mean square error of approximation (RMSEA) values less than .05, comparative fit index (CFI) values greater than .95, and standardized root mean square residual (SRMR) values less than .06 (Kline, 2005). We utilized maximum likelihood estimation with bias-corrected confidence intervals (CIs; Hayes, 2013). Statistical significance was determined by 95% bias-corrected bootstrapped CIs that do not contain zero (du Prel, Hommel, Röhrig, & Blettner, 2009).
To compare models, we utilized Akaike information criterion (AIC), Bayesian information criterion (BIC), and theoretical rationale. Smaller AIC and BIC scores indicate an improved model fit (Kass & Raftery, 1995). Both AIC and BIC favor more parsimonious models and introduce penalty terms as the number of parameters in the model increase (Burnham & Anderson, 2002; Kass & Raftery, 1995). Significant interactions were probed to ascertain whether the simple slopes were significantly different from zero (Hayes, 2013). Based upon empirical findings that condom negotiation self-efficacy is associated with condomless sex intentions (Stappenbeck et al., 2016) and preliminary bivariate analyses, the final model also included a direct path from condom negotiation self-efficacy to condomless sex intentions. This also allowed us to test multiple indirect pathways from PEA and condomless sex intentions. To calculate the indirect effects, we utilized 10,000 bootstrapping resamples (Hayes, 2013).
Results
Preliminary Analyses
Sixty-five percent (n = 264) of our sample reported lifetime PEA as greater than 10, with no significant differences in PEA between groups in either experimental manipulation (ts < –1.0, ps > .3). Means, standard deviations, and correlations of the model variables appear in Table 2. PEA was positively associated with condom-decision abdication intentions and condomless sex intentions and negatively associated with condom negotiation self-efficacy.
Means, Standard Deviations, and Zero-Order Correlations.
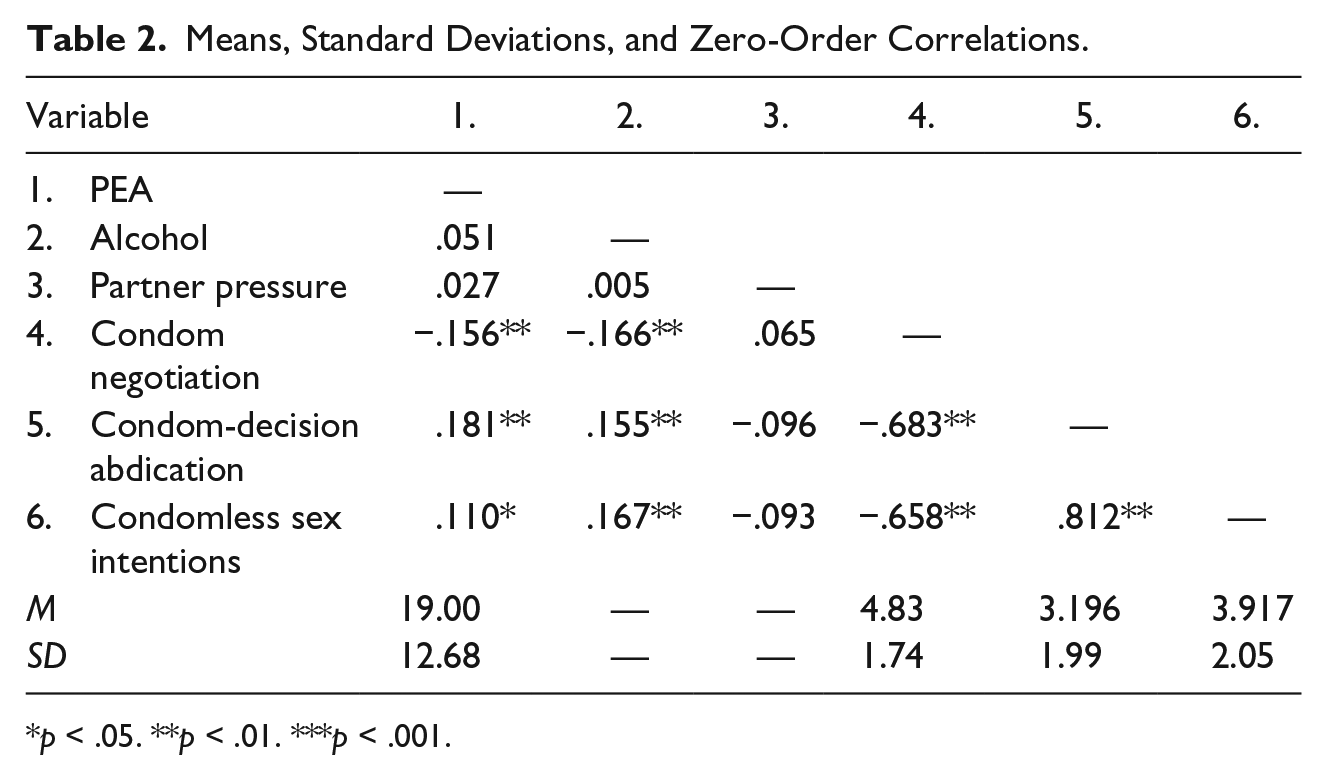
p < .05. **p < .01. ***p < .001.
Model Fitting
Figure 1 shows the hypothesized model. This model was not a good fit for the data, χ2(2) = 26.73, p < .01, RMSEA = .179, 95% CI = [.120, .236], CFI = .97, Tucker–Lewis index (TLI) = .80, SRMR = .02. The final model included only one significant interaction path (Alcohol × Partner Pressure; see Figure 2) and was a good fit for the data, χ2(2) = 2.40, p = .30, RMSEA = .02, 95% CI = [.0, .10], CFI = .99, TLI = .99, SRMR = .004. Examination of AIC and BIC indicated that the final model possessed superior fit over models containing nonsignificant interactions. The final model was compared with a model with no interactions. The final model possessed superior AIC fit (AICfinal = 4,318.61 vs. AICnointeractions = 4,320.80). However, the final model possessed a BIC indicating small evidence (BICdifference > 2) of a poorer fit compared with the model without interactions (BICfinal = 4,394.61 vs. BICnointeractions = 4,392.80). Given the superior model fit of AIC and the theoretical rationale that partner pressure and alcohol have moderating effects on women’s sexual risk-taking decisions, we selected the model with the one significant interaction.
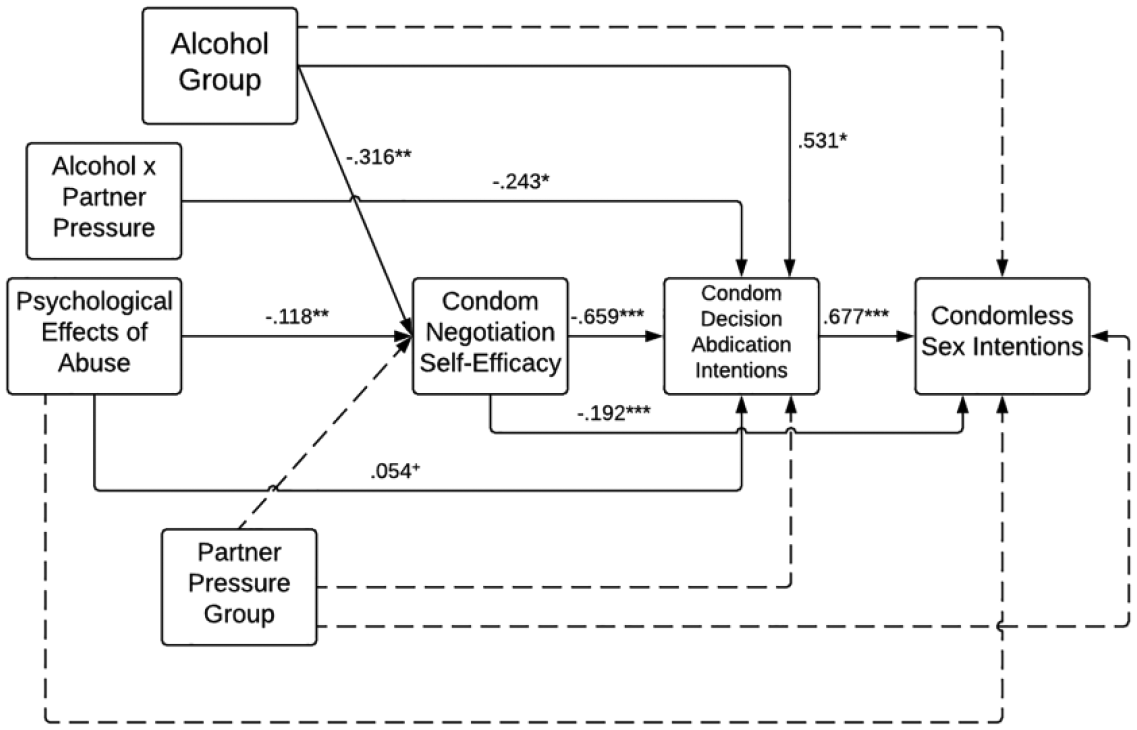
Final model.
Direct and Indirect Effects
Figure 2 depicts the final model with standardized coefficients. The model accounted for 67.7% of the variance associated with condomless sex intentions, 47.7% of condom-decision abdication, and 5.4% of condom negotiation self-efficacy. Standardized coefficients of the indirect paths are found in Table 3. 1 There was no significant direct relationship between PEA and condomless sex intentions; thus, we failed to find support for Hypothesis 1. Consistent with Hypothesis 2, there were two significant indirect pathways from PEA to condomless sex intentions. PEA was indirectly associated with condomless sex intentions via condom negotiation self-efficacy and was indirectly associated with condomless sex intentions via the condom negotiation self-efficacy and condom-decision abdication pathway. Contrary to Hypothesis 3a, alcohol intoxication did not directly influence condomless sex intentions. Supporting Hypothesis 3b, there was a significant indirect association between alcohol and condomless sex intentions through all combinations of condom negotiation self-efficacy and condom-decision abdication intentions. Alcohol was also significantly associated with condom negotiation self-efficacy and condom-decision abdication intentions; women in the intoxicated group reported lower condom negotiation self-efficacy and greater condom-decision abdication intentions than women in the sober group.
Standardized Coefficients of Indirect Effects.

Note. CI = confidence interval.
p < .05. **p < .01. ***p < .001.
The results did not support Hypothesis 4. There was no significant direct or indirect effect of partner pressure on any of the variables. Notably, there was a significant interaction between alcohol condition and partner pressure condition on condom-decision abdication intentions (b = –.24, p < .05; CI = [–.48, –.04]). However, the interaction was opposite of the hypothesized effect. Figure 3 displays this interaction graphically. Simple slope analyses indicated that for women in the alcohol group, low partner pressure was associated with higher intentions to abdicate the decision to use a condom, relative to women in the high pressure condition, t(df = 402) = .52, p < .05.
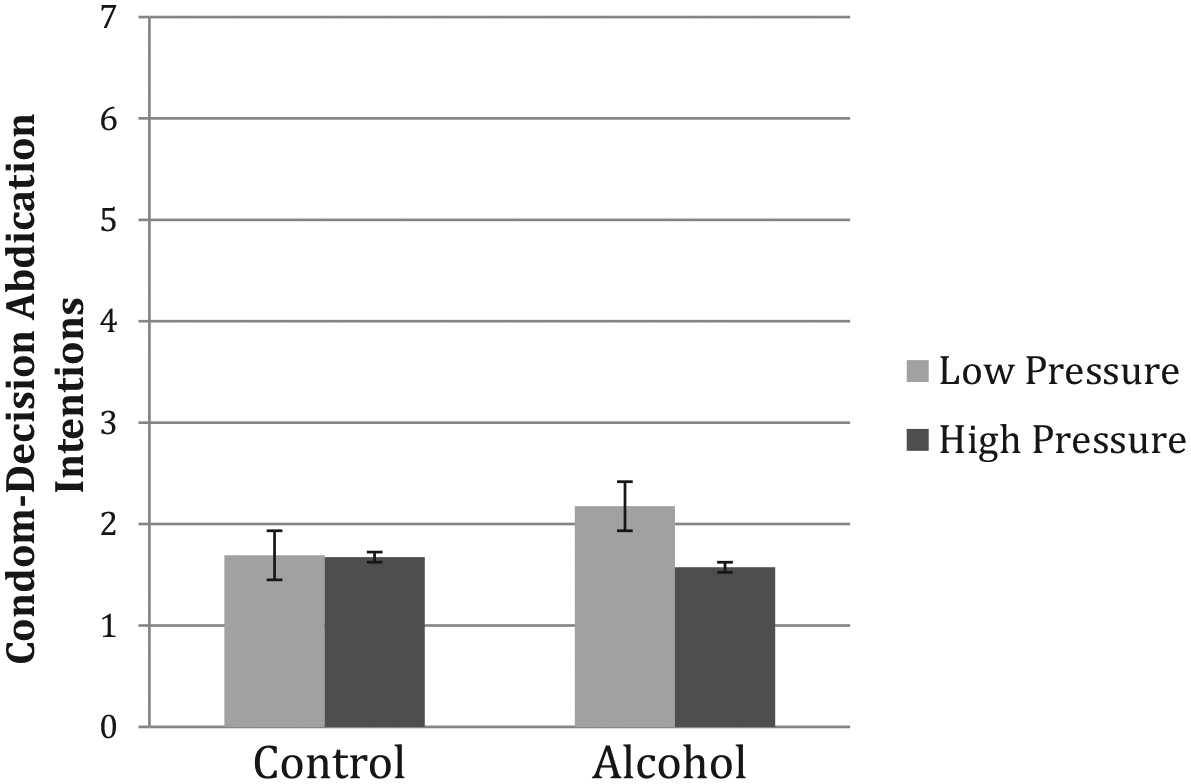
The interaction of alcohol and partner pressure conditions on condom-decision abdication intentions.
Discussion
This study expanded upon prior research on IPV and sexual risk behaviors by focusing on the psychological effects of women’s abusive experiences. We examined associations among PEA, alcohol intoxication, condom negotiation self-efficacy, and condom-decision abdication on condomless sex intentions and our hypotheses were partially supported. We did not find support for a direct positive association between PEA and condomless sex intentions (Hypothesis 1). However, PEA was indirectly associated with condomless sex via condom negotiation self-efficacy and condom-decision abdication intentions. PEA was also indirectly associated with condomless sex intentions via condom negotiation self-efficacy alone. In contrast to expectations, alcohol intoxication did not directly predict condomless sex intentions (Hypothesis 3a). However, we found support for indirect effects of alcohol on condomless sex intentions (Hypothesis 3b). We did not find any interactions between alcohol and PEA, nor did we find direct or indirect effects of partner pressure condition. Interestingly, there was a significant interaction between alcohol condition and partner pressure condition on condom-decision abdication intentions. Intoxicated women in the high pressure condition reported lower condom-decision abdication intentions than did intoxicated women in the low pressure condition.
Condomless sex is a confluence of individual, situational, and interpersonal factors (Cooper, 2010). Ideally, women would feel efficacious in how to use condoms, as well as feel control and confidence in their ability to negotiate condom use with a partner. The results of the current study suggest, however, that women with more severe histories of PEA—marked by the effects of experiencing a partner’s attempts to control, manipulate, and berate them—display less in-the-moment confidence in their ability to negotiate for condom use relative to women with less severe histories, and this is associated with intentions to engage in condomless sex. Women with IPV histories report that such experiences are detrimental to their self-worth and self-efficacy (Matheson et al., 2015). Thus, the impact of PEA on self-worth and control may undermine a woman’s ability to identify and express her sexual desires and needs as important (Matheson et al., 2015). Indeed, women with IPV histories have more negative sexual self-perceptions (i.e., of sex and of themselves as sexual beings) than women without such histories (Offman & Matheson, 2004). Perceived lack of control and more negative views of sex may be detrimental to a woman’s ability to negotiate condom use; thus, a woman may ultimately leave the decision to use a condom up to the partner. Furthermore, women’s IPV victimization has been indirectly associated with sexual risk-taking via posttraumatic stress disorder symptoms (Overstreet, Willie, Hellmuth, & Sullivan, 2015). Controlling behaviors by a partner positively predicted the avoidance symptom cluster severity, which positively predicted sexual risk-taking. Thus, it is possible that women with PEA are avoiding trauma-related thoughts, emotions, or memories during sexual interactions (e.g., potential conflict with a partner) and one outcome of this avoidance is to abdicate the condom decision to a partner.
Although not directly assessed in the current study, it is possible that women’s experiences of PEA include condom-specific coercion, such as reproductive coercion and condom use resistance (CUR; Davis et al., 2014a, 2014c). Men who perpetrate abuse are less likely to use condoms with their partners (for review, see Bergmann & Stockman, 2015). Women in the study who have experienced greater PEA may be afraid of the repercussions that condom negotiation tactics may prompt. A woman’s fear of potential violence in response to a condom request may limit her confidence in her ability to negotiate condom use (Crosby et al., 2013; Lichtenstein, 2005; Masters et al., 2014; Wingood & DiClemente, 1997). Future studies should examine the role of PEA in the context of reproductive coercion and CUR on condom-decision abdication.
The influence of alcohol on condom use may be contingent upon other factors, such as condom negotiation self-efficacy. Consistent with prior findings (Davis et al., 2014a), alcohol directly decreased in-the-moment condom negotiation self-efficacy. Alcohol myopia theory posits that acute intoxication prompts deficits in cognitive processing that result in narrowed attention to salient, immediate, and easily understood situational cues (Steele & Josephs, 1990). In the context of acute intoxication, women focused on situational cues that decreased their condom negotiation self-efficacy (for review, see George & Stoner, 2000). Interestingly, we found an interaction between intoxication and partner pressure condition. Intoxicated women in the high-pressure group were less likely to abdicate the condom decision than women in the low-pressure group. It is possible that intoxicated women in the high-pressure condition were more attentive to Michael’s overt condom resistance, found it aversive, and made negative attributions about Michael, whereas women in the low-pressure condition were more attentive to Michael’s less overt resistance, found it considerate, and saw Michael as potentially trustworthy. Intoxicated participants may have focused more on the salient and relevant cues within the environment, including their sexual partner’s condom avoidance style, compared with sober participants. Again, this study did not investigate these mechanisms and thus these interpretations are speculative.
Strengths and Limitations
The current study has several strengths and limitations to consider when interpreting the results. Participants aged 21 to 30 years were recruited from the community and represent women who engage in heavy episodic drinking and sexual risk behaviors. The sample was also predominantly White, and the majority had attained at least some college education. These findings may not generalize to women who do not belong to these groups. For example, participants who identify as racial/ethnic minorities are found to perceive greater risk of contracting HIV and STIs from sex partners than White participants, which may have implications for their condom use decision-making (Mehrotra, Noar, Zimmerman, & Palmgreen, 2009). Furthermore, the sample comprised women who were interested in sexual experiences with men, and analyses did not investigate differences between exclusively heterosexual women and women who may be sexually attracted to multiple genders. Future research examining women who identify as bisexual and/or have sex contact with multiple genders is needed to ascertain similarities and differences in their condom negotiation and decision-making with men.
While behavioral intentions to engage in sexual risk-taking correlate with real-world sexual risk-taking (Kajumulo et al., 2009; Norris et al., 2010), these results may not fully replicate sexual decision-making in the real world. While PEA could occur in the context of sexual violence perpetrated by a partner, it is also noteworthy that this study did not examine past sexual assault by nonpartners and PEA concurrently. Future research should examine the distinct and synergistic effects of both PEA and sexual assault. It is possible that answering questions assessing PEA had a priming effect, such that the questions prompted participants to reflect upon their past experiences of PEA, which may have contributed to participants’ responses. Because this was an alcohol administration experiment, individuals who have negative reactions to alcohol, are alcohol abstainers, or who engage in problem drinking were excluded from the study. Thus, the population is restricted to individuals who consume alcohol but who are not problem drinkers, which again limits the generalization of the results. It is not possible to extricate expectancy and physiological effects of alcohol on these relations. A placebo condition was not utilized as the expectancy set placebo control has more internal validity at low-dose (BrAC < .04%) than high-dose conditions (Martin & Sayette, 1993). Future investigations might examine these constructs in the context of a balanced placebo design to better ascertain the role of alcohol expectancies.
Clinical Implications and Conclusion
Results suggest the importance of tailoring sexual health prevention and intervention programs with specific targets for doing so. Specifically, targeting in-the-moment condom negotiation self-efficacy through skills training and education may decrease sexual risk behaviors, including abdicating the condom decision to a partner. In addition to existing recommendations regarding evidence-based IPV assessment and counseling practices, as part of preventive health care (Miller, McCaw, Humphreys, & Mitchell, 2015), policy makers may consider increasing training and implementation of evidence-based sexuality education for providers who interface with survivors of IPV. With regard to the role of alcohol, these results indicate that alcohol’s effect on condom use occurs through psychological processes and situational factors including condom negotiation self-efficacy and level of partner pressure. For example, providers at family planning clinics may consider including information on the role of alcohol on self-efficacy and perceptions of partner pressure for patients with histories of alcohol use and IPV. Similarly, providers working with women in substance abuse programs may consider including skill-based curricula to increase condom negotiation self-efficacy. Future research should continue to examine these variables in the context of other factors (e.g., drug use, relationship status) to gain a richer understanding of the impact of PEA on sexual risk behaviors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection and manuscript preparation were supported by grants from the National Institute on Alcohol Abuse and Alcoholism (2R01AA016281; Principal Investigators [PIs]: W. H. George and K. C. Davis; 5F31AA024352-03; PI: E. C. Neilson; 5K08AA021745-05; PI: C. A. Stappenbeck) and the National Institute on Drug Abuse (5K23DA042935-02, PI: A. K. Gilmore).