
Abstract
There is a dearth of information about the association of victim-related and assailant-related characteristics and posttraumatic stress disorder (PTSD) among sexually assaulted women. Recently, Statistics Canada included items measuring the possible presence of PTSD symptoms in their 2014 nationally representative General Social Survey on Victimization (GSS-V), for the purpose of improving the understanding of mental health impacts associated with sexual victimization. The present study used the GSS-V to examine the association of sociodemographic, health, and assailant characteristics and prior traumatic experiences in the form of physical or sexual dating violence, physical assault, stalking, childhood abuse, and witnessing of violence between parents with PTSD symptomology among sexually assaulted women. Among 319 women who reported experiencing at least one incident of sexual assault in the 12 months prior to the survey, 68.6% had experienced at least one negative emotional impact as a result, among whom, 43.6% reported past-month PTSD symptoms. Logistic regression modeling revealed that prior traumatic events in the form of physical or sexual dating violence, stalking, and having witnessed violence between parents were associated with higher odds of experiencing PTSD symptoms, as was having been sexually assaulted by a known assailant. In contrast, the odds of experiencing PTSD symptoms was lower for Aboriginal or visible minority women. The results suggest that PTSD symptoms in the near aftermath of sexual victimization are common, and there are a range of factors that contribute to the likelihood of developing these symptoms. Implications for future research are discussed.
Violence against women is a human rights violation and a signficant public health problem across the globe (Basile & Smith, 2011). In the last quarter century, sexual violence has been found to be a particularly pernicious and prevalent form of gender-based violence (Basile & Smith, 2011). For example, Canada’s 2014 General Social Survey on Victimization (GSS-V) estimated a sexual assault rate of 37 incidents per 1,000 women aged 15 years and older in a single year (Perreault, 2015). Not counted in this estimate were an additional 7% of spousal violence victims who had been sexually assaulted within the past 5 years (Burczycka, 2016) and 5% of women who had experienced childhood sexual abuse before the age of 15 years (Perreault, 2015).
Sexual assault has myriad negative short-term and long-term physical and psychological consequences, some even fatal (Basile & Smith, 2011; Campbell, Dworkin, & Cabral, 2009). Commonly cited psychological sequelae of sexual assault include shame, anxiety, depression, suicidal ideation, and attempted suicide (Basile & Smith, 2011; Campbell et al., 2009; Dworkin, Menon, Bystrynski, & Allen, 2017a). One psychological outcome of interest is posttraumatic stress disorder (PTSD), first listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM) in 1980 and then considered groundbreaking for uncovering the additional longer term impacts of sexualized violence (Campbell & Wasco, 2005).
Broadly defined, symptoms of PTSD include nightmares or flashbacks of a traumatic experience, avoidance of places or people that remind an individual of the traumatic experience, exaggerated startle response or hypervigilence, and numbness or detachment from others (American Psychiatric Association [APA], 2013; Prins et al., 2003). Research has shown that clinically diagnosed PTSD (Cook, Pilver, Dinnen, Schnurr, & Hoff, 2013; Lipsky, Kernic, Qiu, & Hasin, 2016) or the presence of symptoms indicative of PTSD (Dworkin, Mota, Schumacher, Vinci, & Coffey, 2017b; Elklit & Christiansen, 2013; Möller, Bäckström, Söndergaard, & Helström, 2014; Ullman, Filipas, Townsend, & Starzynski, 2006) is common among those who have experienced sexual assault. Campbell and colleagues (2009) reviewed the effects of sexual assault on women’s mental health and noted that prior estimates of PTSD among victims of sexual assault ranged from 17% to 65%, a difference that can be attributed to varying methodologies. Scott and colleagues (2018) examined data collected from 11 countries for the World Health Organization’s (WHO’s) World Mental Health (WHM) survey and found that 20.2% of women who had experienced sexual assault in their lifetime met the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for PTSD.
Much of the nationally representative research on the association between sexual assault and PTSD comes from population-based surveys conducted in the United States. The 2004-2005 National Epidemiological Survey on Alcohol and Related Conditions (NESARC), a survey of Americans aged 18 years and older with a focus on substance use and disorders and related risk factors, found that sexually assaulted women were three times more likely to have PTSD compared with women who had experienced other traumas such as serious illness, accidents, natural disasters, and military combat (Cook et al., 2013). Lipsky and colleagues’ (2016) analysis of the 2001-2002 and 2004-2005 NESARC further revealed that sexually assaulted women were almost six times more likely to have PTSD in their lifetime compared with women who had experienced other traumas such as parental violence, intimate partner violence, war, accidents, natural disasters, or witnessed a death.
Although research is limited, a prominent sociodemographic predictor of PTSD among sexually assaulted women is age, specifically younger age (Campbell et al., 2009). However, there are inconsistent findings with respect to other predictors of PTSD, such as race or ethnicity. For example, Lipsky and colleagues’ (2016) study using the NESARC found that white women were more likely to develop PTSD than visible minority women, whereas Ullman and colleagues (2006) found no association between race and PTSD with their convenience sample of sexual assault survivors in a large Midwestern metropolitan area. However, at the bivariate level, Statistics Canada’s GSS-V, a national population survey, has shown that Aboriginal women are sexually assaulted at a rate three times higher than other Canadian women and experience more severe forms of PTSD following sexual assault (Boyce, 2016).
Limited research also has explored associations between health-related and assailant-related characteristics and PTSD among sexually assaulted women. Comorbid depression (Möller et al., 2014), and in particular Major Depressive Disorder (Lipsky et al., 2016), has been found to be associated with PTSD among sexually assaulted women. Relationship between the assailant(s) and the victim as a predictor of PTSD appears inconsistent. For example, Campbell and colleagues (2009) reviewed empirical literature on adult sexual assault and noted that some studies reported higher rates of PTSD among women who had been sexually assaulted by someone known to them, whereas other studies reported the opposite, with higher rates of PTSD among women sexually assaulted by strangers (Ullman & Filipas, 2001; Ullman et al., 2006). In contrast, Ullman, Filipas, Townsend, and Starzynski (2007) found the relationship of the assailant to the victim was not significant in predicting post sexual assault PTSD, in the presence of a lack of social supports and negative reactions to disclosures. Chivers-Wilson (2006) have argued that negative reactions to sexual assault, usually grounded in rape myths, promote perceptions of sexually assaulted women that often result in blaming the victim, reducing social support, and increasing the risk of PTSD.
Another prominent factor previously found to be associated with PTSD among sexually assaulted women is prior traumatic experiences. The majority of U.S. based studies and reviews, as well as a study conducted in Sweden, revealed that having witnessed family violence (Scott et al., 2018) or experienced abuse in childhood (Basile & Smith, 2011; Bassett, Buchwald, & Manson, 2014; Möller et al., 2014; Ullman & Brecklin, 2002; Ullman et al., 2007; Walsh et al., 2012) were linked to PTSD among women who have been sexually assaulted. Furthermore, sexual revictimization is associated with increased odds of PTSD (Walsh et al., 2012). Using the 2005 National Survey of Adolescents–Replication and the 2006 National Women’s Study–Replication, Walsh and colleagues (2012) found there to be higher odds of PTSD within two timeframes (past 6 months and lifetime) among adolescent, postsecondary, and adult women who had experienced a sexual revictimization compared with those who experienced a single instance of sexual assault.
Although there is a breadth of research conducted in the U.S. focused on sexual assault and PTSD, external validity is a potential concern as similar studies have not been carried out in Canada. This study builds on American research and aims to identify the effects of a broad range of sociodemographic (e.g., homelessness), health (e.g., physical and mental disabilities), and assailant characteristics and the cumulative effects of other types of victimization (e.g., dating violence, experiencing childhood physical and sexual abuse, and witnessing family violence) on the development of PTSD symptomology among sexually assaulted women in Canada. Knowledge from this study could aid in better addressing the mental health needs of diverse sexually assaulted women within a Canadian context and in further enhancing the measurement of these concepts.
Method
Participants and Procedure
This study utilized data drawn from Statistics Canada’s 2014 GSS-V Public Use Microdata File (PUMF). The GSS-V is a population-based survey carried out every 5 years, which measures perceptions of crime and the criminal justice system and experiences of victimization among Canadians aged 15 years and older who live in Canada’s 10 provinces and speak either English or French (Statistics Canada, 2015). Data from residents of Canada’s three territories are collected separately and are not included in the PUMF (see Perreault & Simpson, 2016). Eligible respondents were selected using a disproportionate stratified random sampling method in which the population is divided into strata, and samples selected from these strata are disproportionate to the population size (Statistics Canada, 2015). This helps to ensure that estimates are available for geographic areas with differing populations. Census Metropolitan Areas (CMAs) and non-CMAs made up separate strata within each province with the exception of the smallest province, Prince Edward Island, which is a separate stratum, for a total of 27 strata (Statistics Canada, 2015). In addition, immigrants were oversampled in the three largest CMAs of Toronto, Montreal, and Vancouver, and youths (aged 15-24 years) were oversampled in Toronto, Montreal, Vancouver, Halifax, Ottawa, Winnipeg, Calgary, and Edmonton. The participants were selected using random-digit dialing methodology that includes both landline and cellular phones. Computer-assisted telephone interviewing was used to administer the survey (Statistics Canada, 2015).
The total sample size for the 2014 GSS-V was 33,127, with a response rate of 53%, which was calculated by dividing usable responses (33,127) by the estimated number of households in the sample scope (62,674). Women made up 54% (n = 17,955) of the sample. The data examined in this study are based on a subsample of women who reported being sexually assaulted at least once by an assailant other than a spouse in the 12 months prior to the survey (n = 319). Data about physical and sexual assaults by previous and current spouses are collected separately in the survey and are suppressed on the PUMF due to confidentiality concerns.
Measures
Sexual assault
Statistics Canada uses a derived variable to measure sexual assault that captures the number of incidents (not persons) perpetrated by assailants other than spouses or common-law partners in the 12 month period prior to the survey, which includes “forced unwanted sexual activity,” “sexual activity to which respondent was unable to consent,” and “unwanted sexual touching, grabbing, kissing, or fondling.” Although there are no efforts to date to empirically validate and test the reliability of these items that make up the sexual assault derived variable, they are consistent with the Criminal Code of Canada.
Independent variables
The selection of independent variables for analysis was based on (a) perceived theoretical and clinical importance to PTSD found within the research literature (Campbell et al., 2009; Cook et al., 2013; Gilbert et al., 2009; Lipsky et al., 2016; Möller et al., 2014; Ozer, Best, Lipsey, & Weiss, 2003; Ullman & Filipas, 2001) and (b) availability in the PUMF. Sociodemographic characteristics of respondents included age, marital status, education, main activity (e.g., working at a paid job, going to school, caring for children), country of birth, Aboriginal status (First Nations, Status and Non-Status; Métis; and Inuk/Inuit), visible minority status (as per Census definition used in the GSS-V: South Asian, Chinese, Black, Filipino, Latin American, Arab, Southeast Asian, West Asian, Japanese, Korean, and other visible minority groups, such as Pacific Islanders; see Statistics Canada, 2017), and homelessness or precarious housing (lived in a shelter, on the street or abandoned building; temporarily lived with family or friends, in a car, or anywhere else because they had nowhere to live). Given the small sample counts for Aboriginal status and visible minority status, we created a derived variable that grouped Aboriginal and visible minorities with the response categories as 1 = Aboriginal or visible minority and 0 = white. The respondent’s mental/psychological disability status (daily activities limited as a result of an emotional, psychological, or mental health condition) and physical disability status (difficulty carrying out daily physical activities that limit mobility) were examined using Statistics Canada’s broad derived variables. A respondent’s history of prior traumatic experiences in the form of physical or sexual dating violence in the past 5 years, physical assault in the past 12 months (excludes violence by previous and current spouses), childhood physical abuse, childhood sexual abuse, and witnessing violence between parents before the age of 15 years were also examined. In addition, stalking in the past 5 years was examined by using Statistics Canada’s derived variable, which was recoded as 1 = yes and 0 = no, and included 12 items measuring various forms of stalking (e.g., unwanted messages through e-mail, text, Facebook, or any other social media; anyone waited outside of their home and persistently asked for a date and refused to take no for an answer; for full list, see Statistics Canada, 2015). The relationship of the assailant to the victim was recoded to 1 = known and 0 = stranger. In instances of multiple offenders, the code refers to the offender with the closest relationship to the victim.
Dependent variable
PTSD symptomology was measured by Statistics Canada with items from Prins and colleagues (2003) Primary Care PTSD Screen (PC-PTSD) used to detect, not clinically diagnose, symptoms of the disorder (Perreault, 2015). PTSD symptomology was considered to be present if a respondent experienced any of the following in the month prior to the survey interview: (a) nightmares about the incident or thinking about it when they did not want to; (b) trying to not think about the incident or going out of their way to avoid situations that reminded them of it; (c) feeling constantly on guard, watchful, or easily startled; and/or (d) feeling numb or detached from others, activities, or their surroundings. Prins and colleagues (2003) have noted that the retest reliability for this screening tool is .83 among primary care patients (n = 188) recruited from Veterans Affairs Medical Center in California. In the GSS-V, respondents were asked PTSD symptomology questions only if they reported that they had experienced at least one negative emotional impact as a result of being victimized (e.g., angry, upset, shock/disbelief, hurt/disappointed). PTSD symptomology items were combined to create a composite index that has a Cronbach’s alpha of .801. However, due to the small cell sizes and a positive skew of 1.114 for this variable, parametric statistics could not be applied. Therefore, we created a derived dichotomized variable with the response categories of 1 = yes, experienced PTSD symptomology and 0 = no, did not experience PTSD symptomology.
Data Analyses
Data within response categories of “valid skip,” “don’t know,” “not stated,” or “refusal” were set to missing and excluded from the analyses. Chi-square tests were performed to examine zero-order associations between PTSD symptomology and the independent variables, with a cut-off value for inclusion in the multivariate model of p < .05. Linear regression analysis was used to assess multicollinearity in the model, with the largest variance inflation factor (VIF) value of 2.47 indicating that multicollinearity was not biasing the model. Binary logistic regression analysis using the Statistical Package for the Social Sciences (version 21) was used to identify factors associated with PTSD symptomology among women who had experienced at least one sexual assault. Variables significant at p < .05 were age, martial status, race/ethnicity, homeless/precariously housed, mental/psychological disability, physical disability, stalking, physical/sexual dating violence, childhood physical abuse, witnessed violence between parents, and relationship of assailant to victim and entered into a multivariate logistic regression model. Items that lost significance at p < .05 in the multivariate logistic regression model, including age, marital status, homeless/precariously housed, physical disability, and childhood physical abuse were not included in the most parsimonious logistic regression model presented.
Statistics Canada provides weights to improve the representativeness of the survey sample due to non-response factors, for example, refusal to participate in survey or to answer specific questions. However, weights that inflate the sample size to the adult population of Canada (over 29 million) inflate the coefficients and may be inappropriate for multivariate analyses. To avoid this problem and to reduce sample bias, an adjusted sample weight was calculated by dividing each weight by the average weight (Thomas, Heck, & Bauer, 2005). With this formula, respondents in underrepresented groups are assigned a weight larger than 1, those in overrepresented groups receive a weight smaller than 1, and the original sample size is retained.
Results
Among the 319 women who reported experiencing sexual assault by a nonspouse in the past 12 months, 219 (68.6%) had experienced at least one negative emotional impact as a result of being sexually assaulted and were, therefore, asked the PTSD symptomology questions. Of this group, 96 (43.6%) reported past-month PTSD symptomology (see Table 1). The most common symptom reported was trying not to think about the assault or avoiding situations that reminded them of it (32.2%), followed by feeling constantly on guard, watchful, or easily startled (26.5%); having nightmares or recurring thoughts about the assault (25.5%); and feeling numb or detached from other people, activities, or surroundings (15.4%).
PTSD Symptomology in Past Month Among Women Who Experienced a Negative Emotional Impact as a Result of Sexual Assault in Past 12 Months.
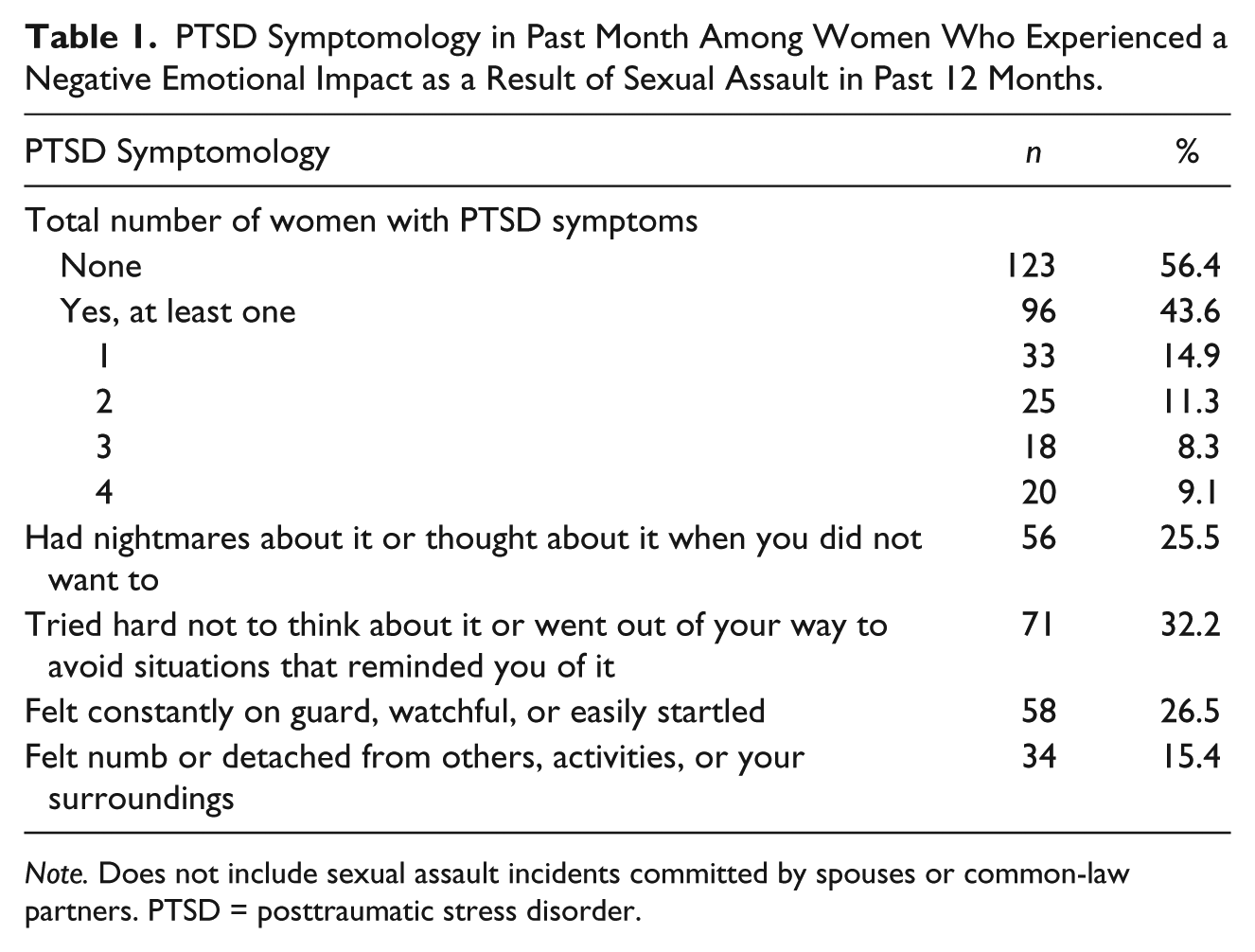
Note. Does not include sexual assault incidents committed by spouses or common-law partners. PTSD = posttraumatic stress disorder.
Table 2 shows the association between independent variables and PTSD symptomology among women who had experienced sexual assault. Chi-square tests demonstrated significant associations between PTSD symptomology and age (χ2 = 8.64, p < .05), marital status (χ2 = 9.65, p < .01), race/ethnicity (χ2 = 7.30, p < .01), homelessness/precarious housing (χ2 = 3.88, p < .05), mental/psychological disability, physical disability (χ2 = 12.83, p < .01), the relationship of the assailant to the victim and prior traumatic experiences in the form of stalking (χ2 = 28.62, p < .01), physical/sexual dating violence (χ2 = 20.94, p < .01), childhood physical abuse (χ2 = 11.97, p < .01), and witnessing of violence between parents (χ2 = 22.80, p < .01).
PTSD Symptomology in Past Month by Sociodemographic, Health, Prior Traumatic Events, and Assailant Characteristics Among Women Who Experienced a Negative Emotional Impact as a Result of Sexual Assault in Past 12 Months.

Note. Does not include sexual assault incidents committed by spouses or common-law partners. PTSD = posttraumatic stress disorder.
High sampling variability; estimate unreliable and should be interpreted with caution.
Includes looking for paid work, caring for children, household work, retired, maternity/paternity leave or parental leave, long-term illness, volunteering or care-giving other than for children, other.
Does not include physical assault incidents committed by spouses or common-law partners.
Includes parents, step-parents, or guardians hit each other or another adult.
Includes incidents involving multiple assailants in which closest relationship was coded.
p < .05. **p < .01.
Table 3 shows findings from the logistic regression analysis. The strongest predictor of PTSD symptomology among sexually assaulted women was physical/sexual dating violence. The odds of experiencing PTSD symptoms among women with a history of dating violence was more than nine times higher than among those who did not have a history of dating violence (adjusted odds ratio [AOR] = 9.03, 95% confidence interval [CI] = [2.04, 39.85]). The odds of experiencing PTSD symptoms was three times higher among those who had experienced stalking compared with those who had not (AOR = 3.33, 95% CI = [1.05, 10.56]). The odds of experiencing PTSD symptoms was almost four times higher among sexually assaulted women who had witnessed violence between parents compared to those who had not (AOR = 3.96, 95% CI = [1.38, 11.39]). Similarly, the odds of experiencing PTSD symptoms among women who knew the assailant was over three times higher than for women who were sexually assaulted by a stranger (AOR = 3.41, 95% CI = [1.33, 8.73]). Aboriginal or visible minority women were at a much lower odds of experiencing PTSD symptoms compared with white women (AOR = 0.18, 95% CI = [0.06, 0.58]).
Factors Associated With Past Month PTSD Symptomology Among Women Who Experienced a Negative Emotional Impact as a Result of Sexual Assault in Past 12 Months.

Note. Does not include sexual assault incidents committed by spouses or common-law partners.–2 log likelihood = 136.517 and Nagelkerke R2 = .483. PTSD = posttraumatic stress disorder; AOR = adjusted odds ratio; CI = confidence interval.
Includes parents, step-parents, or guardians hit each other or another adult.
Includes incidents involving multiple assailants in which closest relationship was coded.
p < .05.
Discussion
To our knowledge, this is the first Canadian study to use population-based data to assess factors associated with PTSD symptomology as a result of non-spousal sexual assault experiences within the past 12 months. A substantial proportion (43.6%) of women who were sexually assaulted reported PTSD symptoms in the month prior to the survey interview, a finding consistent with earlier research (Campbell et al., 2009; Dworkin, Menon, Bystrynski, & Allen, 2017a; Walsh et al., 2012; Zinzow et al., 2012). Certain important sociodemographic, health-related, and assailant-related characteristics and prior traumatic experiences were associated with PTSD symptomology.
Sexually assaulted women who reported a history of physical/sexual dating violence or stalking had much higher odds of reporting PTSD symptoms. This association between prior history of victimization and PTSD symptoms confirms findings from earlier research (Basile & Smith, 2011; Möller et al., 2014; Ullman & Brecklin, 2002; Ullman et al., 2007; Walsh et al., 2012). Similarly, women who had witnessed violence between their parents had increased odds of reporting PTSD symptoms following sexual assault, which is consistent with previous research which has found that negative psychological effects, including PTSD, are associated with witnessing violence in childhood (Randall & Haskell, 2013; Scott et al., 2018; Zinzow et al., 2012). Najdowski and Ullman (2009) have noted that it is important to consider the impacts of cumulative traumatic experiences over the lifetime among women who experience sexual assault in adulthood as it is associated with poorer recovery; for example, these women are more likely to engage in maladaptive coping strategies.
The presence of PTSD symptomology was considerably higher among those women sexually assaulted by a known assailant versus a stranger. Campbell and colleagues (2009) also have noted that some studies found higher rates of PTSD among women who know their assailant. Ullman and colleagues (2007) have argued that this association may be mediated by other psychosocial factors and that relationship of the assailant to the victim is often no longer significant once the effects of social supports and reactions by others after disclosure are controlled. Negative reactions by others and a lack of social supports, which are more prominent in instances in which a victim’s experience does not align with the “real rape” script of having been attacked by a stranger (Du Mont, Miller, & Myhr, 2003; Suarez & Gadalla, 2010), can adversely affect recovery and increase the odds of experiencing PTSD. Increased efforts to raise awareness of the realities of sexual assault will contribute to dispelling incorrect assumptions within rape scripts on who is considered a “legitimate victim” (Du Mont et al., 2003), while simultaneously improving health and social supports by reducing blame toward victims—a strategy that holds the potential to positively affect victim recovery post trauma.
Finally, Aboriginal or visible minority women who experienced sexual assault were at a decreased odds of experiencing PTSD symptomology as compared with white women. Although this finding lends support to some prior research (Lipsky et al., 2016), it should be interpreted with caution due to the small AOR which barely reached significance and small sample counts in our study. Some research with Aboriginal women has attributed lower odds of developing PTSD to the cultural biases within measurements and clinical diagnostic materials, as a history of continuous trauma among this group may result in a normalization of mental health distress (Bellamy & Hardy, 2016). The results of this study may have been different also if the sample size had been large enough to examine Aboriginal women and other racialized women separately. Aboriginal populations are underrepresented in Statistics Canada’s GSS-V and their experiences, therefore, are underestimated. Moreover, other studies have found ethnicity (Ullman & Brecklin, 2002; Ullman et al., 2006, 2007) and Aboriginal status (Bassett et al., 2014; Ehlers, Gizer, Gilder, & Yehuda, 2013) among sexually assaulted women to be a factor associated with increased presence of PTSD. Further exploration is required in this area to fully understand and capture the interplay between sexual assault, ethnicity, colonization, racism, and mental health, including PTSD.
This study has a number of limitations. The GSS-V screens respondents into items that measure symptoms of PTSD only if they have reported negative emotional impacts as a result of the victimization. Furthermore, the survey uses a past-month timeframe for measuring these symptoms, and although this can increase confidence that PTSD symptoms have followed a sexual assault temporally, it may have underestimated the prevalence of PTSD symptomology in our sample, as those whose symptoms had already abated would not have been counted. Future population-based studies, including the GSS-V, should expand their timeframes to better elucidate the trajectories of PTSD among women who have experienced sexual assault.
Reliability concerns regarding Statistics Canada’s measurement of sexual assault could result in an underestimation of the rates (Fisher & Cullen, 2000; Johnson & Dawson, 2011). The GSS-V frames the items as gender-neutral and as crimes; however, experiences that are not considered legally criminal and/or experiences that deviate from a “real rape” scenario (e.g., involve a known assailant; Johnson & Dawson, 2011) may not be disclosed due to shame or embarrassment or confusion about whether to disclose to survey interviewers. In addition, although the 1-year reference period may be useful for estimating current rates of sexual assault, it fails to capture the cumulative long-term effects of sexual assault (Jaquier, Johnson, & Fisher, 2010; Johnson & Dawson, 2011). Finally, the GSS-V measurements for sexual assault are methodologically dated with respect to international best practices, with two of the questions (forced sexual acts and unwanted sexual touching) being modeled after Statistic’s Canada’s 1993 Violence Against Women Survey (European Union Agency for Fundamental Rights [EU FRA], 2014). Inadequate and dated measures can underestimate incidents of sexual assault which, in turn, can compromise the ability to examine long-term effects of sexual assault such as PTSD symptoms.
An additional limitation of this study involves Statistics Canada’s suppression on the PUMF of questions measuring spousal violence and its impacts. Therefore, this study was limited to examining experiences of sexual assault by assailants other than marital and common-law partners. Future research would benefit from making spousal violence data available to researchers using the PUMF and expanding timeframes for experiencing sexual assault from 12 months to lifetime. This would aid in capturing the longer term physical and psychological consequences of of all types of sexual assault to better address the needs of victimized women.
Another limitation of this study is the small counts of Aboriginal women, both due to the small subsample of women examined in this study as well as their underrepresentation in general in the GSS-V, which resulted in the need to group this population with visible minority women. Furthermore, respondents had the choice to be interviewed in English or French only, which may have prevented participation from some immigrants due to language barriers. Research has shown that PTSD among Aboriginal and ethnic populations is often prevalent and complex as a result of additional factors resulting from colonization and systemic racism that disproportionately burden these groups (Bassett et al., 2014; Boyce, 2016; Ullman & Brecklin, 2002; Ullman et al., 2006, 2007). Although the GSS-V has taken some strides in the collection of data in the northern territories (where Aboriginal populations are prevalent) using a separate survey (see Perreault & Simpson, 2016), Aboriginal and non-English and French speaking immigrant populations need to be better represented in these national surveys to more accurately account for their experiences.
This study is the first to use a nationally representative victimization survey in Canada to measure PTSD symptomology items among women who experienced non-spousal sexual assault. Our findings suggest that PTSD symptomology in the immediate aftermath of sexual assault is common and that certain groups of women have higher odds of developing PTSD symptoms. Additional surveys that are more methodologically rigorous and inclusive are warranted to further uncover the prevalence, nature, and extent of PTSD among sexually assaulted women, so as to continue to improve health and social service responses to victimized women.
Footnotes
Acknowledgements
We would like to thank Daisy Kosa for her helpful comments on an earlier draft of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.