
Abstract
Screening rates for intimate partner violence (IPV) among most health care providers are low; yet, positive interactions with providers can benefit people who experience IPV, with respect to increased safety, support, and self-efficacy. Missing is a broad assessment and comparison of knowledge, attitudes, and behavior across the range of providers who are likely to be involved in a response to IPV disclosure. The purpose of our study was to assess health care providers’ IPV preparation, knowledge, opinions, and practices and examine differences across three types of health care providers (medical providers, nursing staff, and social/behavioral health providers). We used an anonymous online survey to gather self-reported information on preparation, knowledge, opinions, and practices around IPV. A random sample of 402 providers was drawn from 13 clinics in a large multispecialty outpatient practice setting. The respondents (N = 204) consisted of medical providers (n = 70), nursing staff (n = 107), and social/behavioral health providers (n = 27). Data analyses consisted of univariate, bivariate, and multivariate analyses. Social/behavioral health providers reported more preparation, knowledge, victim understanding, and less job-related constraints, yet they reported lower screening rates than medical providers and nursing staff. Overall, no provider group seemed well-equipped to work with patients who disclose IPV. Our findings identify unmet needs within our health system to better train health care providers and restructure care models to support IPV identification and response. A focus on interprofessional training and care collaboration would bolster competency and reduce constraints felt by the health care workforce.
Introduction and Background
Approximately, one in four females and one in 10 males in the United States have experienced physical violence, sexual violence, or stalking by an intimate partner (Breiding, 2014). Intimate partner violence (IPV) victimization is associated with substantial mental and physical health consequences (Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012; Dillon, Hussain, Loxton, & Rahman, 2013; McLaughlin, O’Carroll, & O’Connor, 2012; Stewart, Vigod, & Riazantseva, 2016), high medical care costs, and high rates of health service utilization (Bonomi, Anderson, Rivara, & Thompson, 2009; Rivara et al., 2007).
The U.S. Preventive Services Task Force (Moyer, 2013), the Institute of Medicine (2011; now the National Academy of Medicine), and most major nursing and medical organizations recommend screening for IPV in health care settings, especially for females of childbearing age. Yet, screening rates among health care providers are low (Klap, Tang, Wells, Starks, & Rodriguez, 2007), with an estimated 2% to 50% of medical professionals performing routine screening for female patients (Alvarez, Fedock, Grace, & Campbell, 2017). Some researchers have cited discomfort asking about IPV, knowledge deficits, system problems, and negative attitudes and beliefs about IPV as barriers to providers’ screening efforts (Alvarez et al., 2017; Furniss, McCaffrey, Parnell, & Rovi, 2007; Morse, Lafleur, Fogarty, Mittal, & Cerulli, 2012; Sprague et al., 2013; Todahl & Walters, 2011; Yonaka, Yoder, Darrow, & Sherck, 2007). A lack of provider knowledge and preparation may lead to ineffective responses to IPV disclosure or ineffective referrals for services and may prevent people who experience violence from obtaining the support and assistance they need.
Although there is evidence that some health care providers do not believe that addressing IPV is part of their role (Furniss et al., 2007), providers who screen for IPV and counsel patients can actually help reduce subsequent victimization and positively affect a patient’s health (McCloskey et al., 2006). Females with and without a history of IPV believe it is appropriate for health care providers to ask about violence (Plichta, 2007). In a convenience sample of 1,268 females seeking care in emergency departments or primary care clinics, 86% stated they would disclose the abuse when asked directly, respectfully, and confidentially (Kramer, Lorenzon, & Mueller, 2004). Rhodes et al. (2009) found that of 712 males who were in a relationship and presented to the emergency department and agreed to be screened for IPV, 20% (n = 144) disclosed victimization only and 11% (n = 77) disclosed bidirectional IPV. Females have reported that interactions with a health care provider who expresses support and concern resulted in their recognition that they deserved and could obtain safety and a better situation (Chang et al., 2010). For health care providers to hold meaningful and supportive discussions with patients who experience violence and to truly improve patient safety and well-being, it is essential to first assess providers’ readiness to accurately identify and appropriately respond to IPV.
The Physician Readiness to Manage Intimate Partner Violence Survey (PREMIS; Short, Alpert, Harris, & Surprenant, 2006) was created as a comprehensive measure of physician preparedness to manage IPV among their patients. This instrument has been used to measure IPV knowledge, attitudes, and behaviors among primary care physicians and nurses (Bender, 2016; Ramsay et al., 2012), medical students (Connor, Nouer, Mackey, Banet, & Tipton, 2012), nursing students (Connor, Nouer, Speck, Mackey, & Tipton, 2013), dental students (McAndrew, Pierre, & Kojanis, 2014), and pharmacists (Barnard, West-Strum, Yang, & Holmes, 2018) in the United States and the United Kingdom. Overall, the authors of these studies found that providers and students did not perceive themselves to be knowledgeable about IPV or sufficiently prepared to ask patients about IPV and/or to make appropriate referrals; however, those who received IPV training did show higher scores on Knowledge, Preparation, and/or Attitudes scales. Additional recommendations from authors of these studies include increasing training and IPV education incorporated into medical, nursing, and dentistry school curricula (Connor et al., 2012; Connor et al., 2013; McAndrew et al., 2014); more training for pharmacists and primary care clinicians on assessment, intervention, and local resources (Barnard et al., 2018; Ramsay et al., 2012); and establishing universal implements of IPV screening and protocols in health care, especially in rural areas (Bender, 2016).
Reports regarding the correlates of IPV knowledge, preparation, and screening practices are largely limited to physicians and nurses, despite the multidisciplinary nature of health care settings and responses to violence. We found one study where the sample incorporated a broad range of provider types (e.g., nurse, physician, doctor of osteopathy, physician assistant, social worker, psychologist, or psychiatrist) and measured health care providers’ knowledge, attitudes, beliefs, and self-reported behaviors about IPV using 31 items from a survey developed by Maiuro et al. (2000), along with 10 items from the PREMIS (Roush & Kurth, 2016). However, the knowledge, attitudes, and beliefs among the sample of 93 providers were reported as a whole and not delineated by provider type.
Despite some information on IPV awareness and behaviors among select disciplines of health care providers, what is missing is a broad assessment and comparison of preparation, knowledge, opinions, and practices across the range of providers who are most likely to be involved in a coordinated response to IPV. The purpose of our study was to fill this gap by assessing IPV knowledge, preparation, opinions, and practices among medical providers, nursing staff, and social/behavioral health providers in an outpatient multispecialty clinic setting. Our research questions were as follows:
In addition, we explored whether prior IPV training influenced providers’ preparation, knowledge, and opinions.
Method
Data Source and Sample
Data were collected through an anonymous online survey in the fall of 2016. Given the funder’s focus on women’s health, clinics were selected for the sample based on the total number of female clients they served. The top 10 nonprocedural clinics that attended to a large number of female patients based on a rank ordering of clinics by female patient count for the month of March 2015 were identified. One procedural clinic that predominantly served women was also included, regardless of female patient volume, for a total sample of 13 clinics due to the presence of separate subclinics in one clinical area. These clinics included cardiovascular medicine, dermatology, endocrinology, neurology, oncology, Breast Center, orthopedics, otolaryngology, primary care, pulmonology, and rheumatology. The number of clinics chosen for the subsample represented over one third of all practice site clinics in a large, single clinic and surgery center. A random sample of 402 providers was drawn from these 13 clinics. The distribution of the sample across clinics was accomplished using proportional stratified sampling based on the total number of providers in each clinic, not including residents, students, or staff whose duties did not involve patient care. Selection of the sample was done using simple random sampling, using the random number function in Excel. Staff members for each clinic were ordered from highest to lowest random number and the required number from each clinic was selected starting from the top of the ordered list. The 402 providers were invited to participate in an anonymous online survey focused on all patients served in the clinic as the content was not exclusive to IPV among female patients. The survey was open for 8 weeks and a maximum of 10 reminders were sent via email. Respondents who completed the survey received US$10 in “food bucks”—a certificate that was redeemable at the clinic café. Approval for the study was granted by the University of Minnesota Institutional Review Board.
A total of 219 responses were received, for a response rate of 54.48%. Respondents with missing data on key variables were excluded from the current analyses. The final sample consisted of 204 health care providers, including medical providers (n = 70, 44.9% female), nursing staff (n = 107, 93.5% female), and social/behavioral health providers (n = 27, 85.2% female). Table 1 presents sociodemographic information for the sample.
Demographic Characteristics for the Full Sample (N = 204).
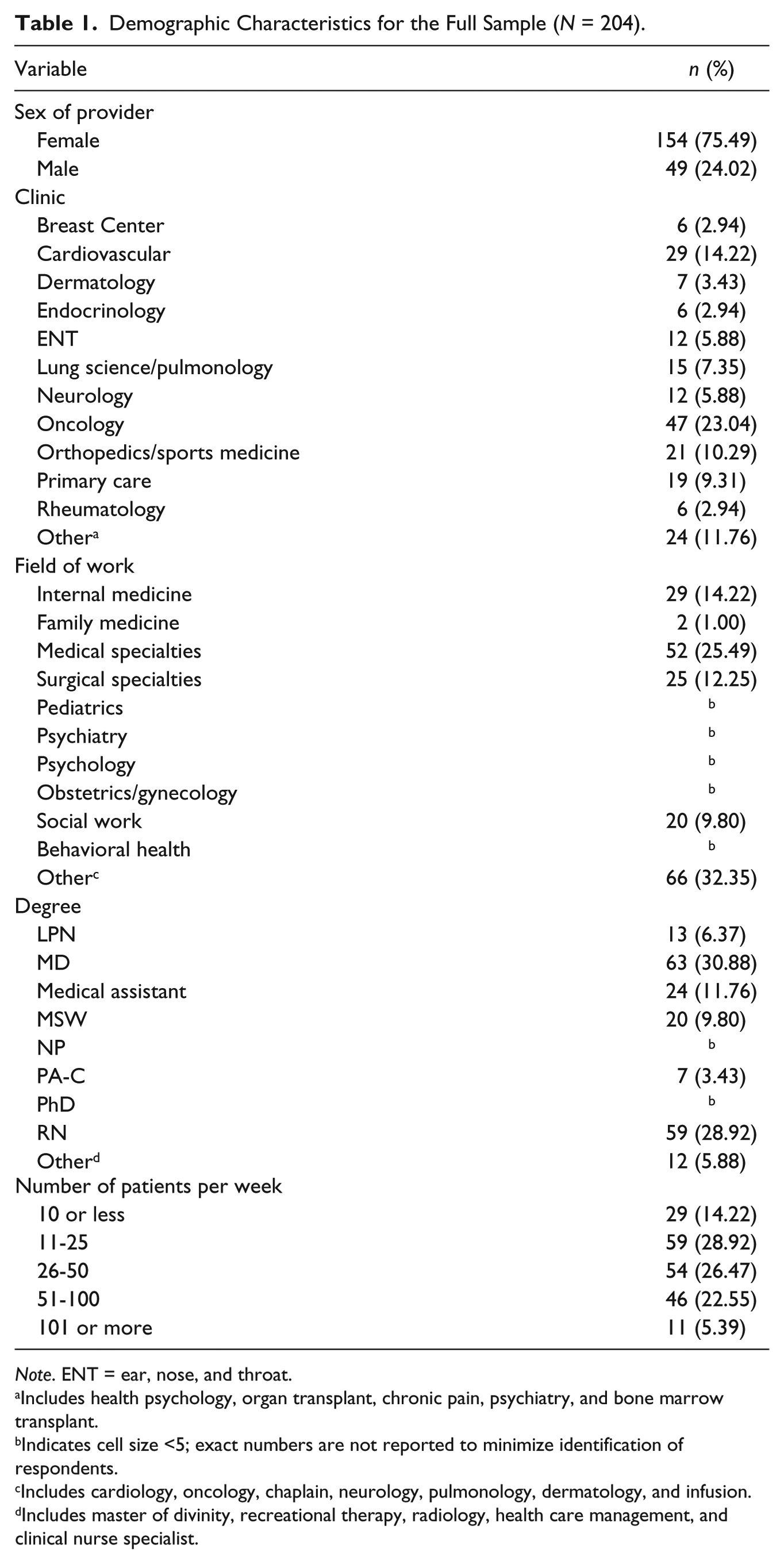
Note. ENT = ear, nose, and throat.
Includes health psychology, organ transplant, chronic pain, psychiatry, and bone marrow transplant.
Indicates cell size <5; exact numbers are not reported to minimize identification of respondents.
Includes cardiology, oncology, chaplain, neurology, pulmonology, dermatology, and infusion.
Includes master of divinity, recreational therapy, radiology, health care management, and clinical nurse specialist.
Measures
Preparation, knowledge, opinions, and practices around IPV
Data on preparation, knowledge, opinions, and practices around IPV were assessed using a modified version of the PREMIS (Short et al., 2006). The PREMIS was originally tested with physicians from the United States (N = 166, 76% male with a mean age of 50.4 years) with Cronbach’s α ≥ .65 for the 10 final scales. An adapted version of the PREMIS has been utilized with a group of medicine, nursing, social work, and dentistry students (N = 286, 57% female, and an average sample age of 27.4 years; Connor, Nouer, Mackey, Tipton, & Lloyd, 2011). In this adapted instrument, six of the eight scales described in the original PREMIS study were identified, with four scales demonstrating acceptable reliability (Cronbach’s α ≥ .70).
We also created a modified version of the original PREMIS, reducing the length of the original survey and removing some overlap in content. This was done based on feedback received during pilot testing. When scoring our modified PREMIS scales, we adhered to instructions in the original survey despite having fewer items per scale. We created summary scales to assess preparation, knowledge, opinions, and practice issues. A respondent needed to provide data for at least 80% of the items in the scale to have a scale score calculated. Thus, there are differences in the number of respondents represented in the scale scores compared with the number who provided data on individual scale items.
A score of perceived preparation (e.g., appropriately respond to disclosures of abuse, conduct safety assessment, and make appropriate referrals) was represented by the mean of 12 items assessing how well respondents believed they are prepared to work with survivors of IPV. Each item was assessed on a 7-point scale ranging from 1 (not prepared) to 7 (quite well prepared). Items were averaged and the scale ranged from 1 to 7. Cronbach’s alpha was .97, which indicated a high level of internal consistency for this scale with this sample. As another measure of preparation, participants were asked whether they had the necessary skills to discuss IPV with a patient who identified as female, male, a sexual or gender minority, and a racial/ethnic minority. The original PREMIS assessed providers’ agreement, using a 7-point scale, about whether they had skills to discuss abuse with IPV victims who were female, male, or from a different cultural/ethnic background. In our study, participants provided a “yes” or “no” response to these four items.
Knowledge (e.g., warning signs of IPV and appropriate ways to ask about IPV) was assessed by 28 items that measured actual knowledge using multiple choice and true/false questions. The scale ranged from 0 to 28, with the score indicating the number of correct responses. Cronbach’s alpha for this scale was at an acceptable level of .64.
Several scales were used to assess each provider’s global opinions about preparation 1 (“opinion-preparation,” one item focused on the respondent’s opinion on whether health care providers are generally prepared to respond to IPV), victim understanding (six items focused on why a person does/does not disclose IPV or leave the relationship, perceptions about screening for IPV in health care settings), victim autonomy (three items focused on a person who experiences IPV and their ability to make decisions about interventions, whether to remain or stay in a relationship), and constraints (two items focused on job-related time constraints in addressing IPV). Response options for the opinion items followed a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree), with some items reverse coded when scoring. Responses were averaged so that each scale score ranged from 1 to 7. Cronbach’s alpha was calculated for each of the Opinion scales with more than one item. Values were .63 for the Victim Understanding and the Constraints scales and .43 for the Victim Autonomy scale.
Practice issues (e.g., situations in which provider screens for IPV, actions taken following screening, whether clinic has adequate space to screen for IPV, and whether clinic provides staff with adequate time to respond to IPV) were measured by 11 items focused on the current screening practices and the clinic environment. The scale ranged from 0 to 26, with higher scores indicating more environmental support for IPV screening and greater engagement in screening one’s patients. Several respondents had significant missing data on items focused on their own individual screening practices or they indicated they were not in clinical practice and these items did not apply. Thus, the number of survey respondents captured in the composite practice issues scale (n = 78; 20 medical providers, 44 nursing staff, and 14 social/behavioral health providers) is significantly less than the number that provided individual item data about their clinic environment or worksite or their individual practice efforts.
Sociodemographic characteristics
Survey respondents provided information on their age, sex, highest education level, clinic where currently employed, and hours of prior IPV training. Respondents also reported their year of graduation from professional school/program and what degree or certificate they received. Based on this latter response, three groups of providers were created: (a) medical providers, including doctor of medicine, doctor of osteopathic medicine, and physician assistant; (b) nursing staff, including nurse practitioner, registered nurse, licensed practical nurse, and certified medical assistant; and (c) social/behavioral health providers, including master of social work, master of divinity, and doctorates in psychology or psychiatry.
Data Analysis
Univariate statistics were calculated and presented by provider type, using means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Preparation, knowledge, opinion, and practice issues—both summary scales and individual items—were compared among medical providers, nursing staff, and social/behavioral health providers using one-way ANOVAs for continuous variables and chi-square tests or Fisher’s exact tests for categorical variables. Associations between provider type and IPV preparation, knowledge, and opinion scores, and skills to discuss abuse with patients were further examined using multivariate linear or logistic regression models, depending on the nature of the outcome of interest. The associations between prior IPV training and knowledge, preparation, and opinions scores were also examined using multivariate linear regression models, adjusting for provider type, sex, and number of years since graduation. With 204 subjects, we had 80% power to detect a difference of 0.7 SD as statistically significant between any two of the three provider type groups at the 0.05 level. The assumptions of linear regression and ANOVA were met. The outcome variable was continuous in the linear regression (see Tables 7 and 9) and was binary in the logistic regression (see Table 8). Analyses were performed using SAS 9.3 (SAS Institute Inc., Cary, NC) and SPSS Version 25 (IBM Corp., 2017) software. A p value ≤ .05 was considered statistically significant.
Results
Provider IPV Preparation, Knowledge, Opinions, and Practice
Table 2 presents means and standard deviations for the providers’ age, number of years since graduating, and amount of prior IPV training, in addition to PREMIS scale scores. Results of the one-way ANOVAs show that mean scores on Perceived Preparation (4.98 compared with 2.59 and 2.90, p < .001), Knowledge (23.26 compared with 21.36 and 20.74, p < .001), and Practice scales (10.08 compared with 8.39 and 8.61, p = .50) were higher among social/behavioral health providers compared with medical providers and nursing staff, respectively. Social/behavioral health providers also had higher mean scores on the four opinion subscales compared with medical providers and nursing staff (all p < .001).
Means and Standard Deviations Sample Characteristics and PREMIS Scale Scores by Provider Type.
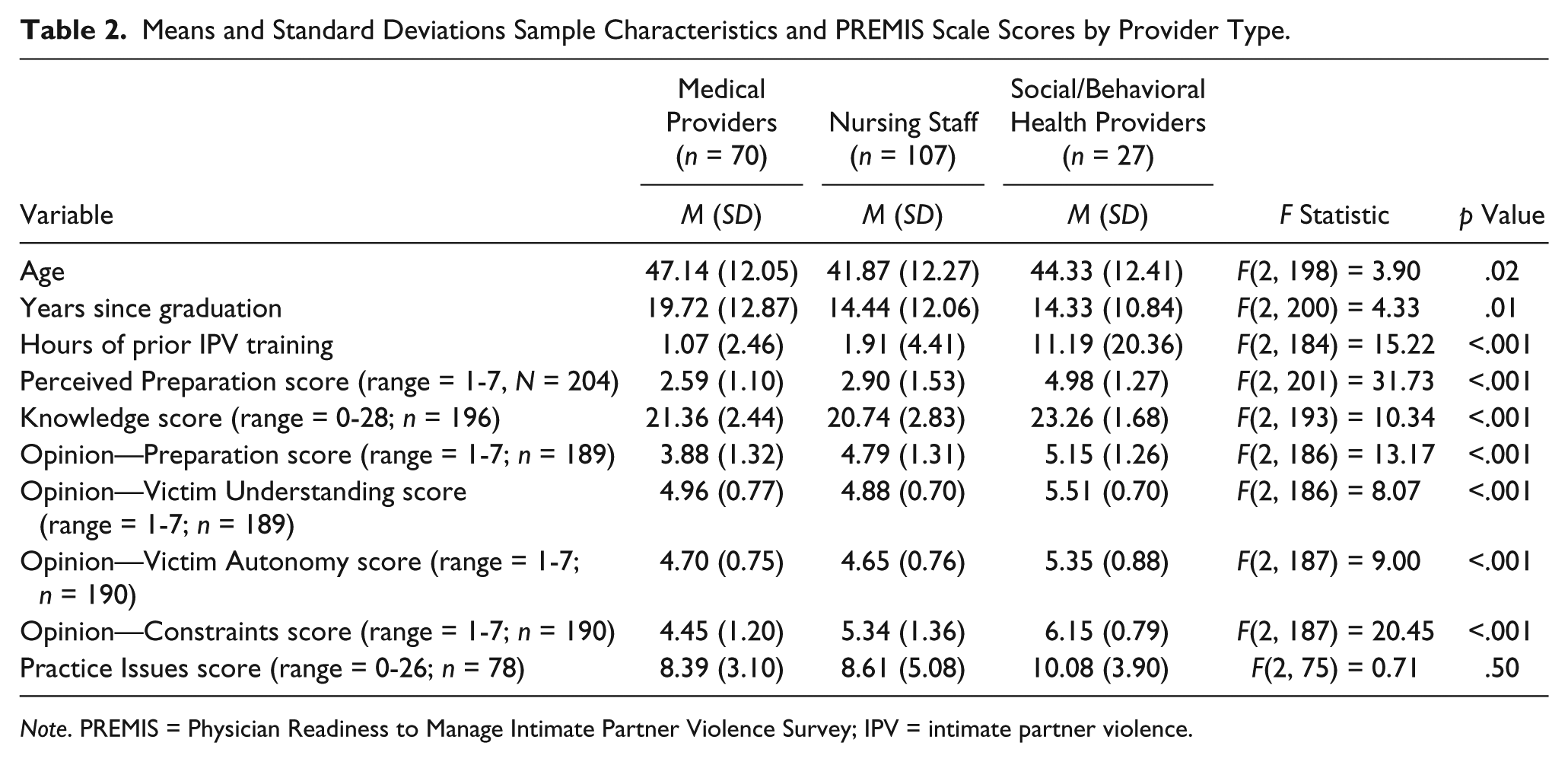
Note. PREMIS = Physician Readiness to Manage Intimate Partner Violence Survey; IPV = intimate partner violence.
Tables 3 to 6 present individual items from the Perceived Preparation, the various Opinions, and Practice scales along with mean scores and percentages across the three provider groups in addition to results of one-way ANOVAs, chi-square tests, and Fisher’s exact tests. All provider types agreed that it was within their scope of work to screen for IPV, with social/behavioral health providers reporting stronger agreement than nursing staff and medical providers. Medical providers were more likely than nursing staff and social/behavioral health providers to agree that health care professionals do not have the knowledge to assist patients in addressing IPV. Over half of the providers (n = 113, 55.39%) did not know whether their clinic had a protocol for responding to disclosures of IPV among adults. Nearly 40% of providers (n = 81, 39.71%) reported that their clinic encouraged them to respond to IPV although only 31.37% (n = 64) reported that their clinic allows adequate time to respond to patients who disclose IPV. Less than one quarter of social/behavioral health providers and approximately half of nurses and medical providers reported that they do not currently screen for IPV.
Means and Standard Deviations for Perceived Preparation Scale Items by Provider Type.

Note. 1 = not prepared to 7 = quite well prepared. IPV = intimate partner violence.
p < .05. **p < .01. ***p < .001.
Means and Standard Deviations for Opinion Scale Items by Provider Type.

Note. 1 = strongly disagree to 7 = strongly agree. IPV = intimate partner violence.
Indicates the item is reverse coded (1 = strongly agree to 7 = strongly disagree).
p < .05. **p < .01. ***p < .001.
Frequencies and Percentages for Practice Issues Scale Items Focused on the Clinic Environment by Provider Type.
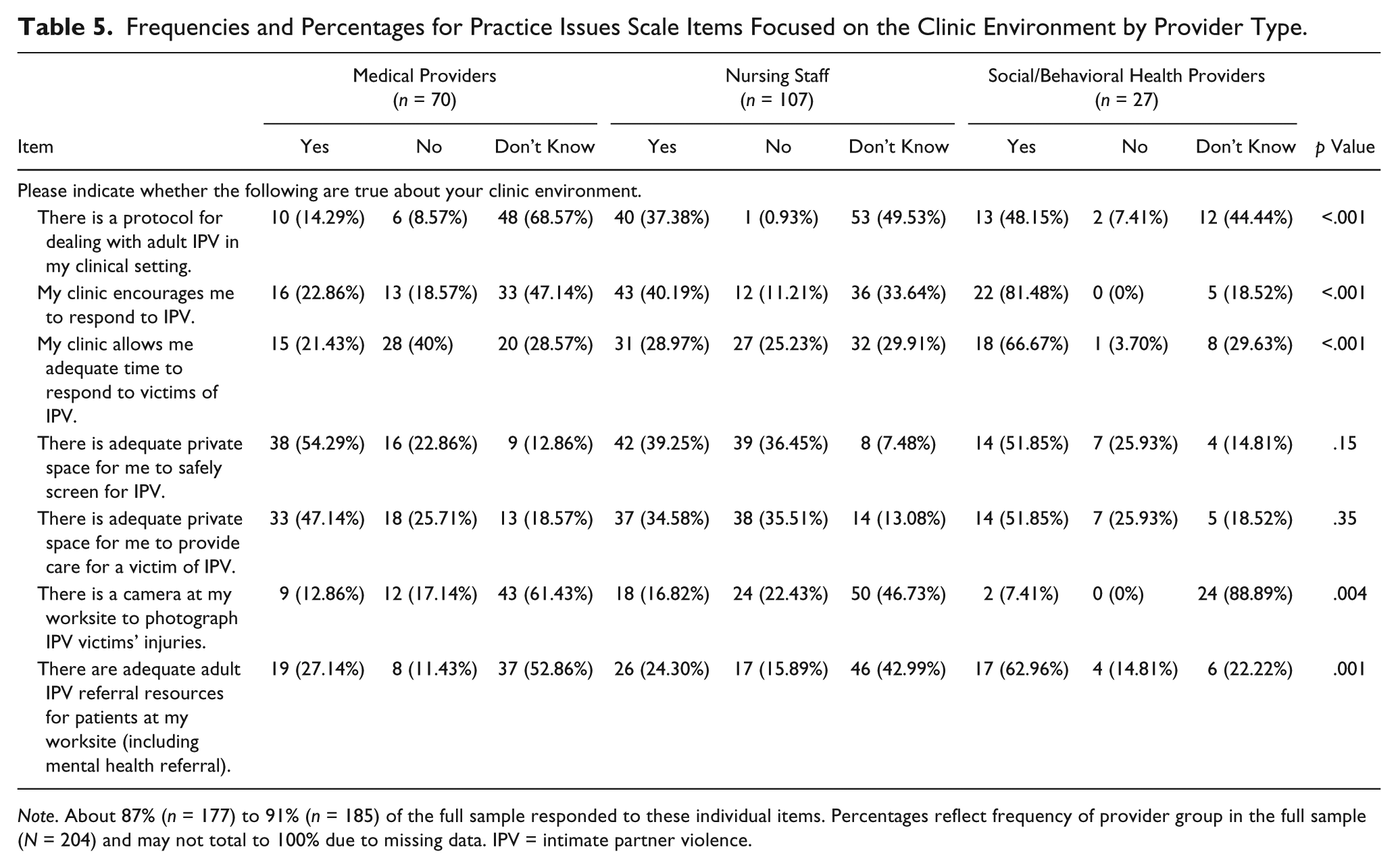
Note. About 87% (n = 177) to 91% (n = 185) of the full sample responded to these individual items. Percentages reflect frequency of provider group in the full sample (N = 204) and may not total to 100% due to missing data. IPV = intimate partner violence.
Frequencies and Percentages for Practice Issues Scale Items Focused on Individual Screening Efforts by Provider Type.
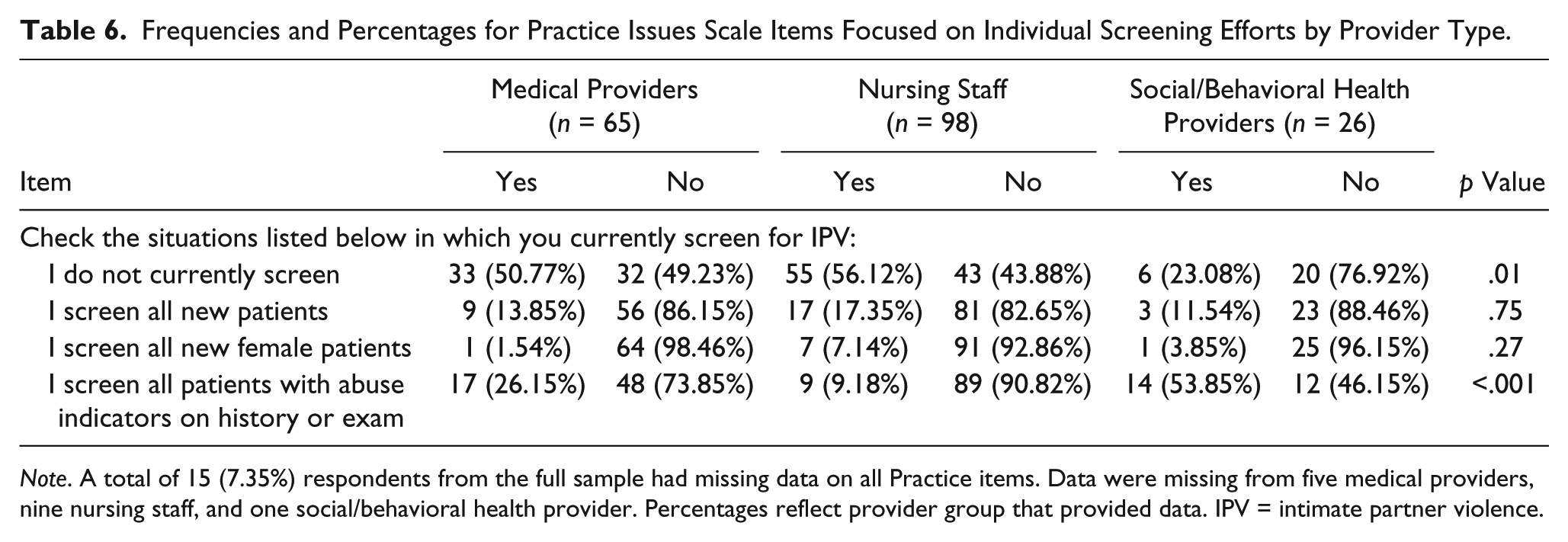
Note. A total of 15 (7.35%) respondents from the full sample had missing data on all Practice items. Data were missing from five medical providers, nine nursing staff, and one social/behavioral health provider. Percentages reflect provider group that provided data. IPV = intimate partner violence.
Separate multiple linear regressions were calculated to predict each PREMIS scale score, based on provider type and controlling for sex and number of years since graduating (Table 7). Compared with medical providers, social/behavioral health providers had significantly higher Perceived Preparation scores (B = 2.30, p < .001), higher Knowledge scores (B = 1.79, p < .01), higher Opinion—Preparation scores (B = 1.22, p < .001), greater Victim Understanding (B = 0.57, p < .01), greater acknowledgment of Victim Autonomy (B = 0.66, p < .001), and greater disagreement that time constraints of the job should affect care of patients who experience IPV (B = 1.68, p < .001). Nursing staff had significantly higher Opinion—Preparation and Opinion—Constraints scores than medical providers (p < .001), but otherwise did not differ from medical providers on any other scales. Providers with fewer numbers of years since graduation also reported higher Opinion—Preparation scores (p < .01). The three provider types were not statistically significantly different from one another in their Practice scores.
Associations Between Provider Type and IPV Preparation, Knowledge, and Opinion Scores.

Note. IPV = intimate partner violence. ns = not significant at .05.
Social/behavioral health providers were more likely to report having the necessary skills to discuss IPV with patients who identified as female, male, of a sexual and/or gender minority, and from a racial/ethnic minority (Table 8). In addition, providers with greater numbers of years since graduation were less likely to report having the necessary skills to discuss IPV with patients who identified as female, male, and sexual/gender minorities.
Associations Between Provider Type and Skills to Discuss Abuse With Diverse Patients.
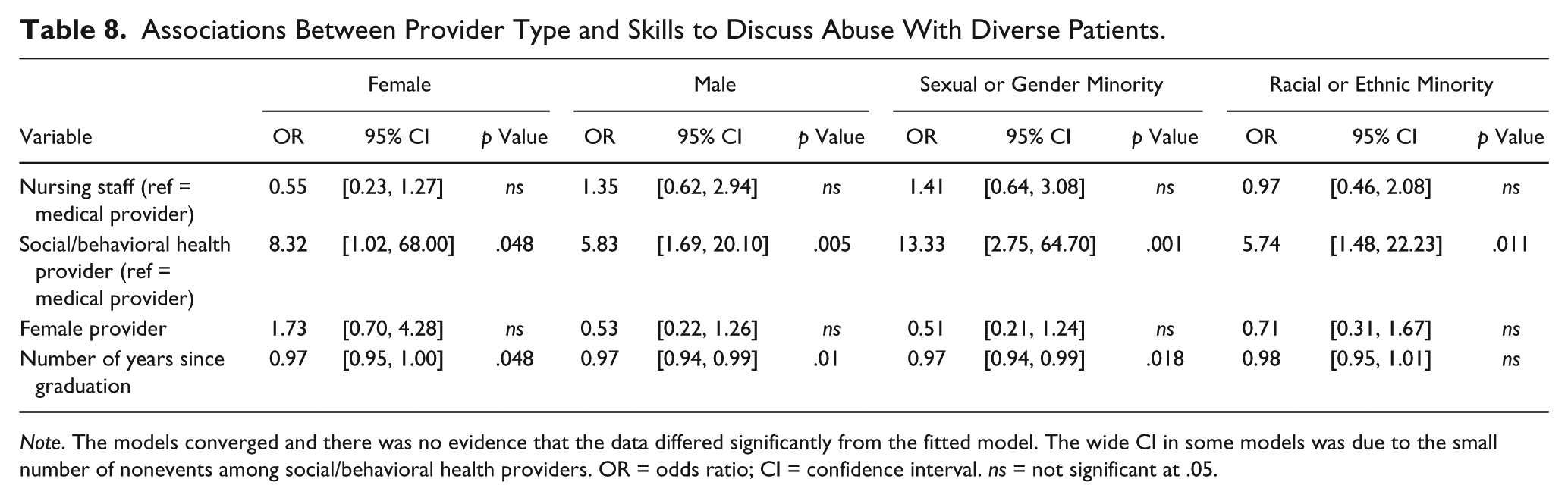
Note. The models converged and there was no evidence that the data differed significantly from the fitted model. The wide CI in some models was due to the small number of nonevents among social/behavioral health providers. OR = odds ratio; CI = confidence interval. ns = not significant at .05.
The Influence of IPV Training on Preparation, Knowledge, and Opinions
Social/behavioral health providers had the most prior training on IPV, averaging 11 hours, compared with below 2 hours for nursing staff and 1 hour for medical providers (Table 2). Using separate adjusted multivariate linear regressions, we examined the association between prior IPV training and knowledge, preparation, and opinion scores. The number of IPV training hours was positively associated with Perceived Preparation (p < .01) but not with IPV Knowledge or any of the Opinion scale scores (Table 9).
Associations Between Training Hours, Provider Type, and IPV Preparation, Knowledge, and Opinion Scores.
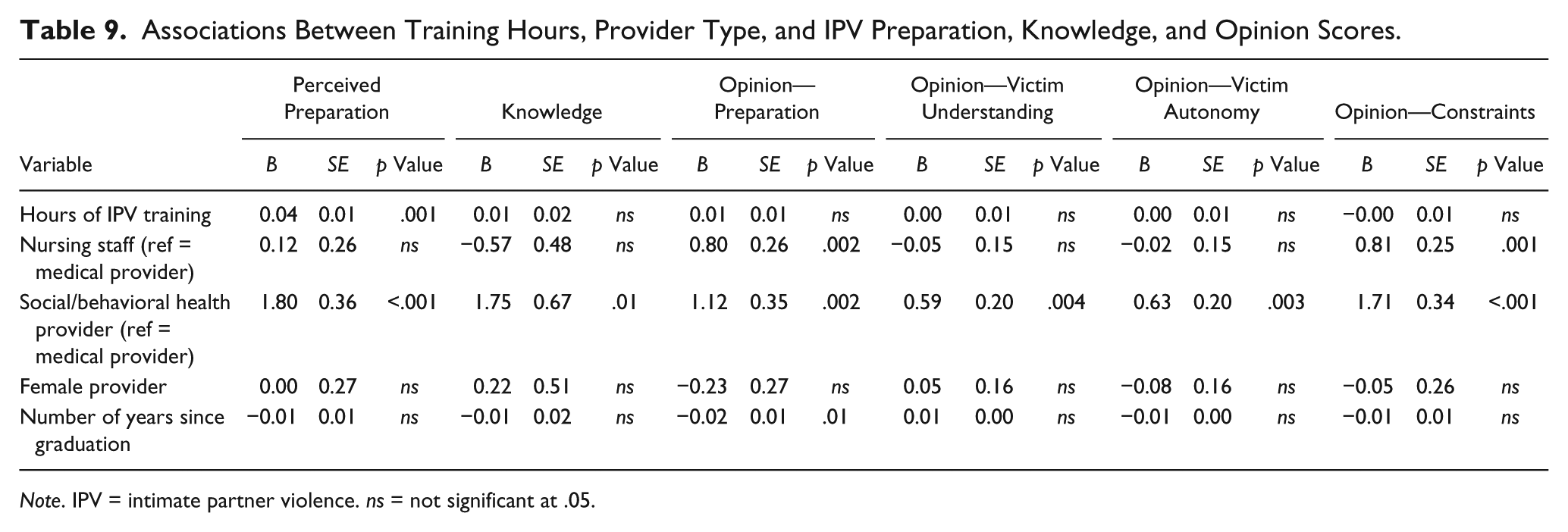
Note. IPV = intimate partner violence. ns = not significant at .05.
Associations of Preparation, Knowledge, and Opinions on Current IPV Screening
Finally, we used separate multivariate logistic regression models to explore whether scores on the Preparation, Knowledge, and Opinion scales were associated with screening practices (results not shown). Affirmative responses to individual practice issues items (e.g., “I screen all new patients,” “I screen all new female patients,” and “I screen all patients with abuse indicators on history or exam”) were modeled as a dichotomous variable that represented providers who currently screen at least some adult patients.
As Perceived Preparation increased, the odds were higher that the respondent screened at least some adult patients (odds ratio [OR] = 2.7, p < .0001). Opinion—Preparation was associated with greater odds of screening for IPV (OR = 1.31, p = .045). Knowledge was not significantly associated with screening patients (OR = 1.04, p = .54). Providers who believed that health care providers should screen for IPV were more likely to report screening. Victim Understanding (OR = 1.06, p = .81) and Victim Autonomy were not associated with providers’ current screening practices (OR = 0.93, p = .74). Finally, the Opinion—Constraints score was associated with screening (OR = 1.38, p = .02). Providers who agreed that job-related time limits did not prevent them from addressing IPV were more likely to screen at least some adult patients.
Discussion
The purpose of this study was to examine IPV knowledge, preparation, opinions, and practices among health care providers in a large multispecialty practice and to test for differences across provider type. It is the first study, to our knowledge, to provide such an assessment across multiple provider types. Despite the widespread recognition by numerous professional organizations of the importance of identifying and responding to violence in the health sector (De Boinville, 2013) and recommendations by the U.S. Preventive Services Task Force and American National Academy of Medicine for screening and counseling in health care settings, our findings revealed that none of the provider types were especially well prepared to screen and respond to IPV, and the degree of IPV knowledge and preparation was lower than anticipated for nurses and often most poor among medical providers. This highlights training needs that appear relevant to all providers as well as some differences in needs by provider type. All provider types scored less than optimally on the Preparation, Knowledge, and Opinion scales, with social/behavioral health providers scoring higher across-the-board than both medical and nursing providers. Disparities with regard to skills in addressing IPV among patients who identified as a sexual/gender or racial/ethnic minority were also found, particularly between social/behavioral health and medical providers. The findings suggest that medical providers may especially benefit from more advanced training and skill-building focused on both general (e.g., assessment of IPV) and specific IPV content (e.g., IPV among diverse populations).
Our study findings linking preparation to actual practice have important implications for adherence to practice guidelines and recommendations. The lack of preparation among medical providers is especially challenging because of the expectation for clinicians to identify survivors. One approach to survivor identification that is being promoted for use in several service lines is universal education, which relies heavily on clinician–patient interaction around healthy relationships, control, abuse, and risk factors (Decker et al., 2017; Miller et al., 2017; Miller, McCaw, Humphreys, & Mitchell, 2015). Although debate remains about the utility of universal screening compared with other forms of identification (e.g., selective screening and universal education), comfort and preparation to identify and support survivors is an essential skill set for health care providers. Furthermore, the lack of preparation, especially among medical providers, to address IPV among racial and sexual minorities is especially problematic as African Americans, Native Americans, and people who identify as sexual and gender minorities have been shown to have higher risk of IPV (Black et al., 2011; Valentine et al., 2017). Therefore, a lack of preparation to address patients from diverse communities serves to reinforce health inequalities by greater missed opportunities to identify and support people who experience violence.
The duration of training was associated with greater preparation and more active identification of survivors in this study, even if improved knowledge was not evident at the time of this study’s assessment. This finding aligns well with prior research linking training to improved identification and referral of IPV survivors within a health setting (Feder et al., 2011). Training the health care and public health workforce to address IPV is a strategic priority of the U.S. Health Resources and Services Administration (Health Resources and Services Administration Office of Women’s Health, 2017) and training on IPV in medical school is recommended by the World Health Organization (WHO; 2013) and the United Kingdom’s National Institute for Health and Care Excellence (Potter & Feder, 2017). However, IPV-focused training, when it is available, is often of limited duration, explaining the constraints reported by physicians in this study and other studies (e.g., Potter & Feder, 2017). Regardless, this finding has implications for the type and content of training opportunities that are needed. Brief, stand-alone trainings on IPV have not been shown to change clinician behavior (Zaher, Keogh, & Ratnapalan, 2014). More substantial training within a system-focused intervention is more effective at increasing referrals for survivors to support services (WHO, 2013; Zaher et al., 2014). A bridge to community resources is also an essential part of a comprehensive system’s response to IPV (Miller et al., 2015), which simultaneously provides opportunities to train the health workforce (Feder et al., 2011).
The identification of disparities in IPV preparation and opinions between social/behavioral health providers and medical providers and nursing staff, and the higher knowledge and skills in addressing IPV among sexual/gender and racial/ethnic minorities among social/behavioral health providers, as compared with medical providers, suggests that interprofessional training and collaboration among these groups may serve as a unique opportunity to bolster IPV knowledge, confidence, and practice for health care professionals. Other researchers who assessed provider knowledge, preparation, and practices using the PREMIS only focused on one medical provider type (e.g., nursing students, dental students, and pharmacists) and did not include social and/or behavioral health providers. Thus, our findings are able to better outline potential areas for knowledge and practice improvements among all providers and also among specific provider types. Because IPV is a multidisciplinary problem, there is evidence to support interprofessional training and response (Lewis et al., 2017). Authors of an early randomized trial among hospital emergency departments found that interprofessional training and cooperation was associated with greater staff knowledge and improved attitudes, organizational culture, and patient satisfaction, but not improved identification of survivors evidenced by medical record documentation (Campbell et al., 2001). A more recent trial centered around a multidisciplinary training and support intervention to improve identification and referral of IPV survivors found markedly greater electronic health record documentation of IPV, health record documentation of referral, and referrals received by community agencies among intervention clinics compared with control clinics (Feder et al., 2011). A Cochrane review of interprofessional education found it to be effective in the management of cases of domestic violence (Reeves, Perrier, Goldman, Freeth, & Zwarenstein, 2013), which is consistent with the complex and inherently interdisciplinary nature of survivors’ health and social needs.
In addition to more robust interprofessional training opportunities among health care providers, there are likely opportunities to enhance organizational infrastructure and support. Of note, although social/behavioral health providers reported more training and confidence around IPV identification and response and fewer job-related constraints to screening, they reported practices that may not reflect this. Only 11.54% of these providers screened all new patients for IPV and only 53.85% screened all patients with abuse indicators compared with 13.85% and 26.15%, respectively, of medical providers. Basic support and infrastructure, such as visible policies and protocols, ample time and private space for working with victims, and readily available resources, would greatly enhance the practice environment. Furthermore, because medical providers are the least prepared to provide IPV-related care, health care systems with imbedded behavioral health teams may form partnerships with social workers and behavioral health clinicians to develop innovative screening and response protocols, thereby capitalizing on the enhanced preparation and knowledge of social/behavioral health providers.
Limitations
Although our study sample was diverse and of a sufficiently powered size, the sample size was insufficient to examine potential effect modification by clinic type (e.g., primary care vs. subspeciality) or by subspeciality type. We did not collect information on the race and/or ethnicity of the health care providers who were the survey respondents, which may limit our ability to understand how these factors affect IPV-related knowledge and practices. We used a modified version of the PREMIS, based on feedback from a pilot study we conducted; however, the modifications only reduced redundant items in the survey. Streamlining the survey questions did not exclude any pertinent content and we do not believe the modifications had any effect on the study findings. Finally, our sample was collected at one practice location within one organization, further limiting variability in environment and practice.
Conclusion
In this study, we sought to understand differences in knowledge, preparation, opinions, and practices surrounding IPV across different health care provider types. Echoing previously published findings, we found health care providers were grossly underprepared to identify and respond to IPV in the medical setting. Frontline medical and nursing staff were among the least prepared, as compared with social/behavioral health providers. Furthermore, clear gaps in practice existed, despite recommendations to screen and counsel patients for IPV. These findings identify unmet needs within our health services sector to better train providers and restructure care models to support social determinants of health. A focus on interprofessional training for all providers, along with efforts to bolster behavioral health responses within health care organizations and building bridges to local community organizations, would serve these needs and develop a more confident, culturally sensitive health care workforce.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This initiative is made possible with funding from the U.S. Department of Health and Human Services, Office on Women’s Health, grant number 1 ASTWH150031-01-00.