
Abstract
Inequitable gender norms, including the acceptance of violence in intimate relationships, have been found to be associated with the occurrence of intimate partner violence (IPV) perpetration and victimization. Despite these findings, few studies have considered whether inequitable gender norms are related to IPV severity. This study uses baseline data from a psychotherapeutic intervention targeting heterosexual couples (n = 247) in Lusaka, Zambia, who reported moderate to severe male-perpetrated IPV and male hazardous alcohol use to consider: (a) prevailing gender norms, including those related to IPV; (b) the relationship between IPV acceptance and IPV severity; and (c) the relationship between inequitable gender norms and IPV severity. Multiple linear regression analyses were used to model the relationships between IPV acceptance and inequitable gender norms, and female-reported IPV severity (including threats of violence, physical violence, sexual violence, and total violence), separately among male and female participants. In general, men and women were similar in their patterns of agreement with gender norms, with both highly endorsing items related to household roles. More than three-quarters of men (78.1%) and women (78.5%) indicated overall acceptance of violence in intimate relationships, with no significant differences between men and women in their endorsement of any IPV-related gender norms. Among men, IPV acceptance was associated with a statistically significant increase in IPV perpetration severity in terms of threatening violence (B = 5.86, 95% confidence interval [CI] = [1.84, 9.89]), physical violence (B = 4.54, 95% CI = [0.10, 8.98]), and total violence (B = 11.65, 95% CI = [3.14, 20.16]). There was no association between IPV acceptance and IPV victimization severity among women. Unlike IPV acceptance, there was no evidence for a relationship between inequitable gender norms and IPV severity for either men or women. These findings have implications for the appropriateness of gender transformative interventions in targeting men and women in relationships in which there is ongoing IPV.
Keywords
Introduction
Intimate partner violence (IPV) is a serious human rights and public health issue, with profound short- and long-term repercussions for individuals, families, and communities. IPV has been defined as “any behavior within an intimate relationship that causes physical, psychological, or sexual harm to those in the relationship” (World Health Organization, 2017). It is the most common form of violence experienced by women worldwide, with a lifetime prevalence of around 30% among women over the age of 15 (Devries et al., 2013). This prevalence can vary widely by setting, with estimates ranging from 15% to 71% across countries (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). These findings are particularly concerning due to the severe physical, reproductive, and mental health consequences associated with IPV victimization, including elevated rates of chronic pain, gastrointestinal problems, gynecological disorders, HIV infection, depression, post-traumatic stress disorder, and suicidality (Campbell, 2002; Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008; Trevillion, Oram, Feder, & Howard, 2012).
A growing number of studies have documented the most salient risk factors for IPV perpetration and victimization across diverse cross-national settings. These include low socioeconomic status, young age, early marriage, low levels of education, childhood maltreatment, and harmful alcohol use (Abramsky et al., 2011; Capaldi, Knoble, Shortt, & Kim, 2012; Hindin, Kishor, & Ansara, 2008). In addition, attitudes regarding the use of IPV have been found to play a substantial role in both IPV perpetration and victimization. A robust body of literature focused on men’s use of violence in heterosexual contexts has established that across settings, men who believe that IPV is acceptable are more likely to perpetrate violence, and women who believe that IPV is acceptable are more likely to experience violence (Abramsky et al., 2011; Capaldi et al., 2012; Fulu, Jewkes, Roselli, & Garcia-Moreno, 2013; Hindin et al., 2008). A number of mechanisms may explain this relationship. There is considerable evidence demonstrating intergenerational transmission of violence, possibly via violence attitudes. For example, children who witness IPV in their homes are predisposed to the belief that such violence is appropriate and justifiable and may therefore be more likely to experience or perpetrate IPV as adults (Abramsky et al., 2011; Capaldi et al., 2012; Fulu et al., 2013; Heise, 1998). In addition, women who believe that IPV is acceptable may be less likely to report the problem to family members or civil authorities (Flood & Pease, 2009; Sudha & Morrison, 2011), thereby increasing the likelihood that they will remain in a relationship in which there is ongoing IPV.
More broadly, societal gender inequities and patriarchal family structures may facilitate a social environment in which IPV is permissible (Gracia & Herrero, 2006; Herrero, Rodríguez, & Torres, 2016; Jewkes, 2002). Indeed, the endorsement of inequitable gender norms has been found to be highly correlated with accepting attitudes toward violence in intimate relationships (Flood & Pease, 2009). For instance, a recent study conducted in 51 countries found that both men and women with sexist attitudes (as measured by hostility toward women in politics and business) are generally more accepting of IPV (Herrero et al., 2016). Other investigations have found that subscribing to a patriarchal ideology, including masculine sex-role stereotypes, negative attitudes toward women, and unequal marital role expectations, has a strong relationship with IPV acceptance (Haj-Yahia, 2003; G. A. Marshall & Furr, 2010; Yoshihama, Blazevski, & Bybee, 2014). These findings suggest that an individual’s gender norms more broadly—and not solely their attitudes regarding violence in intimate relationships—may play an important role in IPV perpetration and victimization. Gender theorists have attributed this link to the concept of hegemonic masculinity, which proposes that male dominance and control over women is a central component of masculinity in many settings, with violence serving as one means of maintaining this power (Connell, 1987; Jewkes, Morrell, et al., 2015). This theory has been borne out in recent studies that establish a direct link between inequitable gender norms and IPV risk (Messersmith et al., 2021; Ozaki & Otis, 2017; Rahman, Nakamura, Seino, & Kizuki, 2013).
Despite the established relationships of both IPV acceptance and inequitable gender norms with IPV, the vast majority of studies that consider these factors have measured IPV as a dichotomous variable (i.e., no violence vs. any violence), rather than unpacking their relationships with IPV severity. This represents a significant gap in the literature, as more severe IPV has been found to correspond to higher rates of revictimization, more serious or lethal injuries, and poorer mental health outcomes (Campbell, 2002; Chandra, Satyanarayana, & Carey, 2009; Garcia-Moreno et al., 2006; Wathen et al., 2016). The limited number of studies that have examined predictors of IPV severity have documented many of the same risk factors as have been found for any occurrence of IPV, including young age, low education, low socioeconomic status, exposure to IPV during childhood, and harmful alcohol use (Dim & Elabor-Idemudia, 2021; Sabri, Renner, Stockman, Mittal, & Decker, 2014; Valdez-Santiago, Híjar, Martínez, Burgos, & Monreal, 2013). There is inadequate evidence, however, as to whether similar patterns hold true for IPV acceptance and inequitable gender norms. While we might expect that these factors would relate to IPV severity, the presence and strength of this relationship have meaningful implications for IPV prevention efforts targeting gender norms.
Such issues may be particularly relevant in Zambia, the site of the current study. The lifetime prevalence of physical, sexual, and/or emotional IPV in Zambia has been found to be 47% among women between the ages of 15 and 49 years, with 31% reporting violence occurring in the past 12 months (Central Statistical Office, Ministry of Health, & ICF International, 2014). Studies have found that in the Zambian context, women who believe that wife beating is justified are more likely to experience physical or sexual IPV (Hindin et al., 2008; Klomegah, 2008), and that around 47% of women and 32% of men believe that IPV is acceptable under at least one circumstance (i.e., if a wife goes out without telling her husband, if she neglects her children, if she argues with her husband, if she refuses to have sex with her husband, or if she burns the food) (Central Statistical Office, Ministry of Health, & ICF International, 2014). Notably, structural disempowerment among women in Zambia, including a lack of access to information (e.g., exposure to television, radio, and print media) and a lack of autonomy in household decision-making, has been found to be associated with IPV acceptance (Lawoko, 2006). This suggests the potential importance of gender inequity to IPV in this context; to our knowledge, however, no studies have directly investigated the relationship between inequitable gender norms and IPV in Zambia. Furthermore, as with most of the literature, all of the above-mentioned studies have assessed IPV as a dichotomous any versus none variable, rather than considering the spectrum of IPV severity.
This article will aim to address these important gaps in the evidence by considering the following research questions: (a) What are the prevailing gender norms, including those related to IPV, among heterosexual couples living in Lusaka, Zambia, and how do these differ between men and women? (b) What is the relationship between (1) IPV acceptance and (2) inequitable gender norms and female-reported IPV victimization severity (including threats of violence, physical violence, and sexual violence) among male and female partners in relationships with ongoing male-perpetrated IPV?
Method
Participants and Procedures
This study uses data from the Violence and Alcohol Treatment Study, a randomized control trial (RCT) in Zambia assessing the effectiveness of a psychotherapeutic treatment in reducing both IPV and hazardous alcohol use among heterosexual couples. Ethical approval for the trial was given by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board and the University of Zambia Biomedical Research Ethics Committee.
Detailed procedures for the RCT have been published elsewhere (Kane et al., 2017). In brief, the study evaluated the effectiveness of an evidence-based transdiagnostic cognitive behavioral therapy-based intervention—the Common Elements Treatment Approach (CETA; Murray et al., 2014)—among 248 family “units,” consisting of an adult woman, her male partner, and one youth aged 8 to 17 years (if applicable). The study was carried out in three high-density, low-resource neighborhoods in Lusaka, Zambia. Study recruitment was completed by trained lay mental health counselors, who went door-to-door in the selected neighborhoods and used a script to explain the purpose of the study to potentially eligible families. Inclusion criteria were as follows: (a) the family was living permanently in one of the three study neighborhoods; (b) all family members spoke at least one of the study languages (English, Bemba, or Nyanja); (c) the man and woman were in an intimate relationship (i.e., married or dating); (d) all family members provided consent, and if a child was participating, the woman provided permission; (e) the woman reported recent experiences of moderate or severe IPV perpetrated by the man, as indicated by a score ≥38 on the physical and sexual violence combined subscale of the Severity of Violence Against Women Scale (SVAWS) (L. L. Marshall, 1992; Peltzer & Pengpid, 2013); and (f) the man and/or the woman reported that the man had engaged in recent hazardous alcohol use, as indicated by a score ≥8 on the Alcohol Use Disorders Identification Test (AUDIT) (Saunders, Aasland, Babor, De la Fuente, & Grant, 1993). Exclusion criteria were as follows: (a) any family member on an unstable psychiatric drug regimen; (b) any family member with past-month suicidal behavior including both suicidal ideation and self-harm attempts; or (c) any family member currently diagnosed with a psychotic or developmental disorder.
Given the sensitivity of study topics, eligibility screeners were administered using laptop-based Audio Computer Assisted Self-Interviewing (ACASI), which has been found to be both acceptable and feasible among this study population (Kane et al., 2016; Langhaug, Sherr, & Cowan, 2010). For families that were found to be eligible, a study assessor immediately administered the full baseline assessment battery separately to each participant using ACASI. Eligible families were then randomized to either CETA or an enhanced control condition (treatment-as-usual plus safety checks; Kane et al., 2017). The current analysis focuses solely on baseline data from adult participants who consented to the full study and includes no additional exclusion criteria.
Measures
Men’s and women’s gender norms, including their attitudes toward the use of violence in intimate relationships, were measured using the Gender Equitable Men Scale (GEMS) (Pulerwitz & Barker, 2008). This 24-item measure assesses the degree to which participants agree with statements related to violence, sexual relationships, reproductive health, and household roles. Each item includes three response options: agree, partially agree, and do not agree. Gender norms were measured using the full GEMS, with a participant’s total score created by summing scores from the 24 individual items and higher scores representing more gender-inequitable attitudes. In this sample, the internal consistency of the GEMS was high for both men (α = 0.88) and women (α = 0.86). IPV acceptance was measured using a subset of three GEMS items related to the use of physical violence in intimate relationships: there are times when a woman deserves to be beaten, it is alright for a man to beat his wife is she is unfaithful, and a man can hit his wife if she won’t have sex with him. Participants were coded as accepting of violence if they agreed or partially agreed with any of these three items. This methodology is consistent with a number of other studies that have considered IPV acceptance using either the GEMS or similarly worded items in the Demographic and Health Surveys (DHS) (Fleming et al., 2015; Hindin et al., 2008; Uthman, Lawoko, & Moradi, 2009). To note, while these three items contributed to an individual’s overall inequitable gender norms score, we also assessed them independently from the broader scale to examine the unique associations of IPV acceptance with IPV severity.
IPV severity was measured using the SVAWS administered to the female partner in the couple (L. L. Marshall, 1992). This 46-item measure asked women to report on how often they have experienced several types of IPV perpetrated by their partner enrolled in the study over the past 12 months. Each item includes four response categories: never, once, a few times, or many times. Subscales capture three separate violence domains: threats of violence (e.g., shook a fist at you, threatened you with a weapon); physical violence (e.g., pushed or shoved you, kicked you, beat you up); and sexual violence (e.g., physically forced you to have sex, made you have oral sex against your will). A total sum score was generated to capture overall IPV severity, and domain-specific sum scores were generated to capture threats of violence (19 items), physical violence (21 items), and sexual violence (six items). In this sample, the internal consistency was high for the full SVAWS (α = 0.95), as well as for the threats of violence subscale (α = 0.90), physical violence subscale (α = 0.91), and sexual violence subscale (α = 0.80).
The baseline assessment battery also collected basic sociodemographic information including age (categorized for the purposes of this analysis as 18-25, 26-35, 36-45, and 46+ years old), educational attainment (categorized as either having completed primary school or higher, or not having completed primary school), employment status (categorized as either full or part-time employed, or unemployed), monthly income (categorized as <100 Zambian Kwacha [ZMW], 101-299 ZMW, 300-499 ZMW, or 500+ ZMW), and relationship to partner in the study (categorized as either married or unmarried).
Data Analysis
We first calculated univariate descriptive statistics to separately examine the prevailing gender norms among this population, with chi-square tests used to evaluate whether there were statistically significant differences between male and female participants. Then, multiple linear regression analyses were used to model the relationships between (a) IPV acceptance and (b) inequitable gender norms and IPV severity, separately among male and female participants. Separate models considered IPV severity in terms of threats of violence, physical violence, sexual violence, and total violence. Although all models relied on the female partner’s reporting of IPV severity, it is important to note that this outcome variable simultaneously captured IPV perpetration for the male partner and IPV victimization for the female partner, as women were asked to report about IPV experienced specifically in relation to their partner enrolled in the study. All models controlled for age, education, employment status, monthly income, and relationship to partner as potential confounders. In order to reduce the effects of extreme data values, resistant multiple linear regression models were fit using iteratively reweighted least squares (Hamilton, 2013). As there were very low levels of missingness across all included variables (<5%), listwise deletion was used to deal with missing data. All analyses were undertaken using Stata 14.2 (StataCorp, 2015). Statistical significance was established at the 0.05 alpha level.
Results
Sociodemographic Characteristics
The sociodemographic characteristics of participants are presented in Table 1. Although a total of 248 couples enrolled in the study, 247 couples were included in the current analysis as one couple was missing gender norms data for both the man and woman. A plurality of both men (38.1%) and women (40.1%) were between the ages of 26 and 35 years. Slightly over half of the men (51.4%) had completed primary school or higher, whereas the majority of women (66.0%) had not completed primary school. Likewise, while over half of the men (55.5%) reported full- or part-time employment, most of the women (58.7%) were unemployed. For men, the most commonly reported average monthly income was greater than 500 ZMW (41.7%); for women, it was less than 100 ZMW (38.1%). There was a lack of concordance between men and women in terms of their reported relationship status: according to men, 26.7% of the couples were married, whereas according to women, 37.3% of the couples were married.
Baseline Sociodemographic Characteristics for Men and Women (N = 247 Couples).

Note. ZMW = Zambian Kwacha.
Relationship status according to either man or woman within couples.
Gender Norms Among Men and Women
Prevailing gender norms among men and women, including those related to IPV, are presented in Table 2. In general, men and women were similar in their gender norms, with particularly high endorsement of items related to roles within the household. For instance, 93.5% of men and 94.7% of women agreed or partially agreed that a women’s role is taking care of her home and family, and 81.4% of men and 83.4% of women agreed or partially agreed that the husband should decide to buy the major household items. In addition, 88.3% of men and 88.7% of women agreed or partially agreed that a woman should obey her husband in all things. A majority of both men (78.1%) and women (78.5%) indicated their overall acceptance of violence in intimate relationships through their agreement or partial agreement with one or more of the following items: there are times when a woman deserves to be beaten (men 59.9%, women 57.9%), it is alright for a man to beat his wife if she is unfaithful (men 55.5%, women 52.2%), and a man can hit his wife if she won’t have sex with him (men 40.9%, women 48.6%). There were no significant differences between men and women in their endorsement of any of the items related to IPV acceptance.
Gender Norms Using the Gender Equitable Men Scale for Men and Women (N = 247 Couples).

Note. Bolded items represent those that are statistically significantly different at p < .05.
Pearson’s chi-square test for difference in prevalence.
Based on positive endorsement of any of the following items: there are times when a woman deserves to be beaten; it is alright for a man to beat his wife if she is unfaithful; and a man can hit his wife if she won’t have sex with him.
Most of the gender norms that demonstrated significant differential endorsement by men and women were related to sexual relationships. Women were significantly more likely to agree that men need more sex than women do (men 70.5%, women 83.4%, p = .001) and that a man needs other women even if things with his wife are fine (men 60.3%, women 70.0%, p = .02). Conversely, men were significantly more likely to agree that a woman who has sex before she marries does not deserve respect (men 52.6%, women 43.1%, p = .03) and that women who carry condoms on them are easy (men 70.5%, women 61.5%, p = .04). Furthermore, there were significant gender differences in endorsement of two items related to roles within the household: changing diapers, giving a bath, and feeding kids is the mother’s responsibility (men 76.9%, women 87.9%, p = .001) and a man should have the final word about decisions in his home (men 85.4%, women 78.5%, p = .047).
IPV Acceptance and IPV Severity
The multiple linear regression analyses of the association of female- and male-reported IPV acceptance with female-reported IPV severity were divided into four gender-specific models by primary outcome: threatening violence, physical violence, sexual violence, and total violence (Table 3). Each of these models adjusted for age, education, employment status, monthly income, and self-reported relationship to partner. Among men, IPV acceptance was associated with a statistically significant increase in IPV perpetration severity in the couple in terms of threatening violence (B = 5.86, 95% confidence interval [CI] = [1.84, 9.89], p = .005), physical violence (B = 4.54, 95% CI = [0.10, 8.98], p = .045), and total violence (B = 11.65, 95% CI = [3.14, 20.16], p = .008). There was only marginal evidence, however, for a relationship between IPV acceptance and sexual violence perpetration severity among men (B = 1.41, 95% CI = [−0.15, 2.98], p = .076). By contrast, there was no association between IPV acceptance and IPV victimization severity among women in the couple. This held true for total violence, as well as for each of the violence subdomains. Among both men and women, there were few associations between IPV severity and any of the control variables. The exceptions were significant increases in threatening violence and total violence severity among older men (≥46 years old), as well as significant increases in threatening violence and sexual violence severity among older women (≥46 years old).
Multiple Linear Regression Analyses of the Relationships Between IPV Acceptance, Inequitable Gender Norms, and IPV Severity for Men and Women (N = 247 Couples).
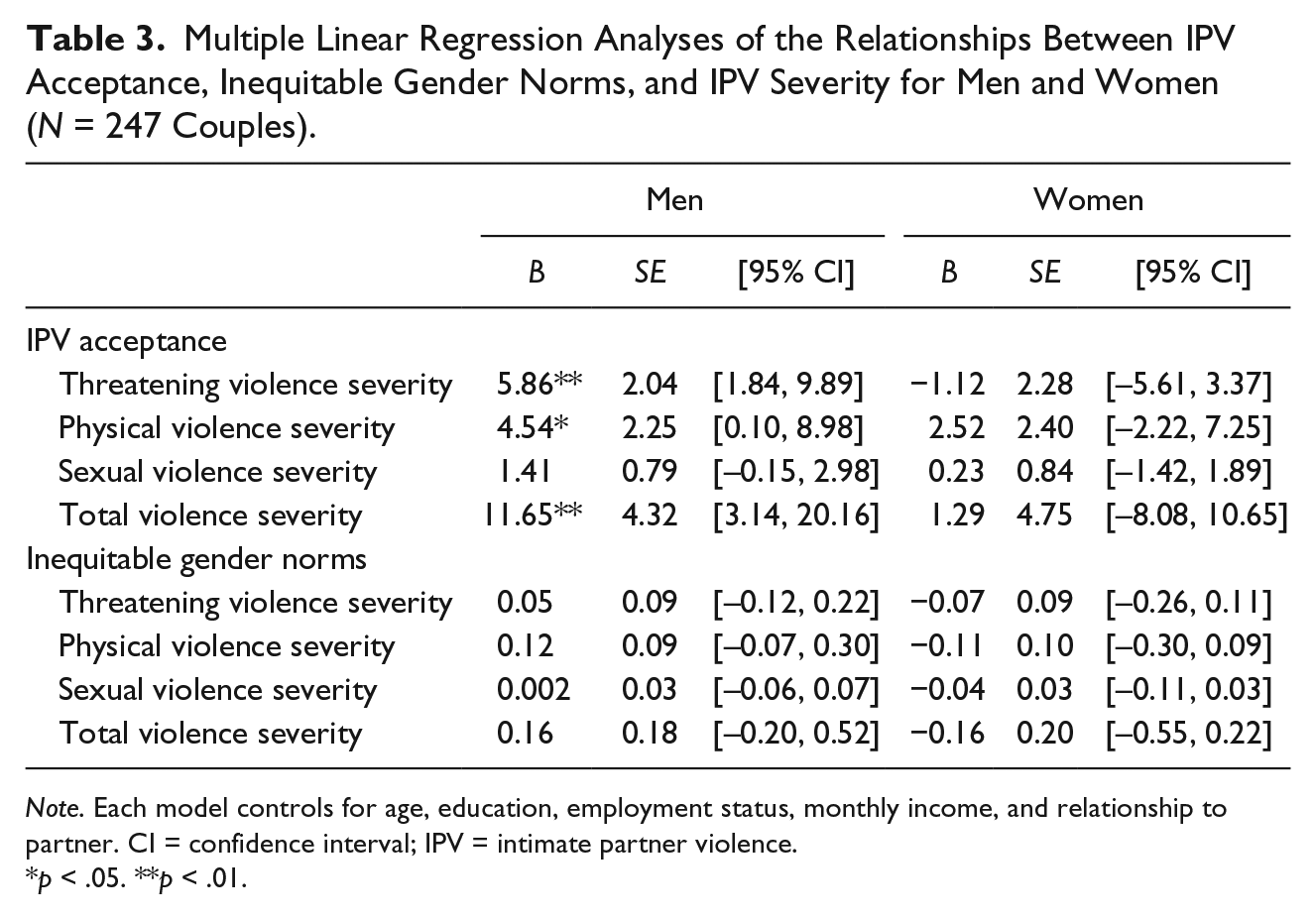
Note. Each model controls for age, education, employment status, monthly income, and relationship to partner. CI = confidence interval; IPV = intimate partner violence.
p < .05. **p < .01.
Inequitable Gender Norms and IPV Severity
Similar to the prior set of analyses, the multiple linear regression analyses of the relationship between overall gender-inequitable attitudes and IPV severity were divided into four models for both men and women, with separate models capturing total violence as well as each of the violence subdomains (Table 3). These models adjusted for the same covariates as listed above. Unlike IPV acceptance, however, there was no evidence for a relationship between men’s or women’s inequitable gender norms and female-reported IPV severity.
IPV Acceptance and Inequitable Gender Norms
In order to expand upon these initial results, we subsequently explored the relationship between IPV acceptance and nonviolence-related inequitable gender norms. We first created a new subscale consisting of the 21 GEMS items that do not relate to the acceptance of violence in intimate relationships. As before, a participant’s total score was created by summing scores from the 21 individual items, with higher scores representing more gender-inequitable attitudes. Then, we performed independent sample t tests on the mean subscale score for men and women who endorsed IPV acceptance compared with those who did not. Finally, we included nonviolence-related inequitable gender norms alongside IPV acceptance in the set of regression analyses outlined in the “IPV Acceptance and IPV Severity” section.
Non-violence-related inequitable gender norms were significantly larger among those who accepted violence in intimate relationships for both men (mean difference = 7.75, p < .001) and women (mean difference = 8.64, p < .001). The inclusion of nonviolence-related inequitable gender norms alongside IPV acceptance in the regression analyses had a negligible impact on the results detailed above for both men and women. This suggests that among men, IPV acceptance is associated with IPV severity independent of nonviolence-related inequitable gender norms.
Discussion
The results of this study indicate that acceptance of violence in intimate relationships is highly normative among IPV-affected men and women in Lusaka, Zambia. Among 247 couples, the vast majority of individuals agreed or partially agreed that there are times when a woman deserves to be beaten, that it is alright for a man to beat his wife if she is unfaithful, and/or that a man can hit his wife if she refuses to have sex with him. Across these items, there were no significant differences in endorsement between men and women. This is different from prior studies conducted in sub-Saharan Africa. In their analysis of DHS data in 17 sub-Saharan African countries, Uthman et al. (2009) found that women were consistently more likely to justify IPV than men, with the exception of Lesotho, Swaziland, and Kenya. Although this analysis did not include Zambia, the most recent DHS data from Zambia indicated a similarly discrepant pattern in IPV acceptance between men and women (Central Statistical Office, Ministry of Health, & ICF International, 2014). In addition, the DHS reported a much lower overall endorsement of IPV acceptance than was observed in our study, with only 32% of men and 47% of women agreeing that IPV was justifiable in one or more circumstances. Notably, although DHS data are representative of the general population, the current study was limited to couples with recent reports of moderate or severe male-perpetrated IPV. It is likely that this explains the higher prevalence of IPV acceptance.
Our results also demonstrate an overall endorsement of inequitable gender norms among IPV-affected men and women in Zambia, with particularly high levels of gender-inequitable attitudes related to roles within the household. Furthermore, these inequitable gender norms are related to IPV acceptance, with men and women who accept violence in intimate relationships holding greater gender-inequitable attitudes on topics unrelated to IPV. Notably, although men and women generally held similar gender norms, men were more likely to agree with inequitable statements related to women’s sexual behaviors (i.e., women should not have premarital sex or carry condoms) and women were more likely to agree with inequitable statements related to men’s sexual needs (i.e., men need more sex and women outside their marriage). Several prior comparative studies that have examined gender norms among both men and women have found that on the whole, women are more likely to agree with gender-inequitable statements than their male counterparts (Krishnan et al., 2012; Messersmith et al., 2021; Scott et al., 2013). For instance, in their recent study among 450 couples in Tanzania, Messersmith et al. (2021) found that women were more likely to endorse inequitable attitudes related to gender roles, contraceptive use, and tolerance of violence, reflecting high levels of internalized sexism. Although our study did not find similar imbalances between men and women, the widespread acceptance of inequitable gender norms among this IPV-affected population merits further qualitative exploration to unpack the individual factors that shape such attitudes and beliefs.
Among men in our study, there was a significant association between IPV acceptance and IPV severity across multiple violence domains (threatening violence, physical violence, and total violence). This suggests that not only are men who accept violence in intimate relationships more likely to perpetrate IPV, as has been well established in the literature (Fleming et al., 2015; Fulu et al., 2013; Hindin et al., 2008), but they are also more likely to perpetrate more severe forms of IPV (i.e., more frequent violence and/or more types of violence). This is a novel finding, as to our knowledge no existing studies have examined the relationship between IPV acceptance and IPV severity across multiple violence domains. It emphasizes the potential for men’s IPV acceptance to be a point of intervention for those who are already engaged in moderate or severe IPV. Notably, the relationship between women’s IPV acceptance and IPV severity did not hold true in our study. This suggests that within relationships in which there is ongoing IPV, men’s acceptance of violence overshadows women’s in driving continued severe perpetration.
We found no evidence for a relationship between men’s or women’s overall gender-inequitable attitudes and IPV severity. Despite the theoretical basis for the association between inequitable gender norms and IPV (Connell, 1987; Jewkes, Morrell, et al., 2015), we are not alone in our finding that they may not always be related at the individual level. Indeed, a recent systematic review of studies examining the relationship between gender norms and IPV perpetration found that across 18 included studies, about 50% found no evidence for a relationship between the endorsement of gender-inequitable attitudes and IPV perpetration (McCarthy, Mehta, & Haberland, 2018). The authors hypothesized that if gender inequities are in fact salient to IPV perpetration, as gender theory would suggest, these mixed findings may be due to underlying measurement issues, as most included studies did not validate context-specific gender norms measures. The lack of validation of the GEM scale in our study is problematic and could potentially explain its observed absence of relationship with IPV severity. Future qualitative work should focus explicitly on local conceptualizations of gender norms, views, practices, and relations, as well as a more in-depth exploration of gender equitability in this setting. This would serve to inform the adaptation and validation of the GEM scale, or the construction of an alternative instrument that may be more appropriate for measuring inequitable gender norms in the Zambian context.
In the IPV prevention sphere, there has been a recent drive toward interventions that seek to transform individual and community gender norms in order to prevent IPV perpetration (Bourey, Williams, Bernstein, & Stephenson, 2015; Jewkes, Flood, & Lang, 2015). In particular, there is mounting global evidence regarding the promise of “gender transformative” approaches, which endeavor to engage boys and men in IPV prevention efforts through an explicit focus on increasing gender-equitable attitudes and behaviors (Casey, Carlson, Two Bulls, & Yager, 2018; Dworkin, Treves-Kagan, & Lippman, 2013; Jewkes, Morrell, et al., 2015). For instance, the Male Norms Initiative contributed to a statistically significant increase in gender-equitable norms and reduction in IPV perpetration among young men in Ethiopia through a combination of interactive group reflections on common gender norms, and community mobilization and engagement activities (Pulerwitz, Hui, Arney, & Scott, 2015). Likewise, the Stepping Stones program in South Africa, which involved single-sex discussion groups on gender norms, sexual and reproductive health, and communication skills, led to a significant reduction in male perpetration of violence, although it had no impact on the experience of violence among women (Jewkes et al., 2008). Results from the present study lend support to this focus on men’s engagement in interventions targeting IPV. Specifically, the fact that we found a relationship between IPV acceptance and IPV severity for men but not women suggests that targeting men’s use of violence as an appropriate conflict- and problem-solving strategy in this setting may help to mitigate severe IPV perpetration.
Given the above-mentioned trend toward focusing on gender norms in IPV prevention efforts, our study’s finding regarding the lack of relationship between gender-inequitable attitudes and IPV severity merits further discussion. Although our results do not invalidate the potential of general gender transformative programming to reduce the prevalence of IPV at a community level, they do suggest that a greater impact may be seen through a narrower focus on IPV acceptance, particularly as a tertiary prevention or treatment approach in families where IPV is already occurring. Indeed, although interventions focused on gender norms have been shown to have a robust impact on increasing gender-equitable attitudes, the evidence is much more mixed in terms of their corresponding influence on IPV perpetration (Casey et al., 2018; McCarthy et al., 2018). While the rationale behind trying to shift gender norms seems clear from a pure prevention standpoint, it may be that this kind of broad-based approach has less utility for those who are already engaged in relationships in which there is ongoing moderate or severe IPV, as in the case of the current study.
Several study limitations must be noted. First, as mentioned above, the GEM scale was not specifically adapted for use in the Zambian context. Although the scale demonstrated high internal consistency among both men and women in our study, it may be that it does not fully capture the underlying construct of gender-inequitable attitudes in Zambia. In addition, the cross-sectional nature of these data precludes statements about causality or directionality of influence between IPV acceptance, inequitable gender norms, and IPV severity. Indeed, there is the strong possibility of a bidirectional relationship between IPV acceptance and IPV severity, with those who are in more severe IPV situations for an extended time being more likely to normalize or justify those violence experiences. Unfortunately, the vast majority of existing studies on these issues have been cross-sectional (McCarthy et al., 2018); the literature would benefit greatly from longitudinal investigations that attempt to unpack temporal complexities in the relationship between violence attitudes and behaviors. Furthermore, this study only included couples with recent reports of moderate or severe male-perpetrated IPV, limiting the generalizability of findings. Finally, the measurement of IPV severity in this study was entirely based on the woman’s report. Lack of concordance in IPV reporting between men and women is a common finding, with women generally more likely to report IPV victimization than men to report IPV perpetration (Cunradi, Bersamin, & Ames, 2009; Khawaja, Tewtel-Salem, 2004; Schluter, Paterson, & Feehan, 2007; Yoshikawa, Shakya, Poudel, & Jimba, 2021).
The results of this baseline study among IPV-affected couples in Zambia indicate that although the acceptance of violence in intimate relationships is pervasive among this population, such attitudes may play a much greater role for men than for women in motivating ongoing severe IPV perpetration. Furthermore, despite notable levels of endorsement for a broad set of inequitable gender norms, there does not appear to be a direct relationship between overall gender-inequitable attitudes and IPV severity. Collectively, the findings support the testing of gender transformative interventions that directly target men’s attitudes toward violence in preventing IPV.
Footnotes
Acknowledgements
We would like to acknowledge the research team for their efforts in implementing this study. We are grateful to the UK Department for International Development and the South Africa Medical Research Council for support and funding. We would also like to acknowledge the couples and families that took part in our study and allowed us to learn from them.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the UK Department for International Development and the South Africa Medical Research Council (#52069) as part of the What Works to Prevent Violence against Women and Girls Programme. S.L.F. is supported by the National Institute of Mental Health’s Global Mental Health Training Program (5T32MH10321).