
Abstract
Intimate partner violence (IPV) among married women of childbearing age can significantly enhance their risk of adverse health outcomes such as injury and disability, depression and anxiety, unwanted pregnancies, premature labor, complications with delivery, and perinatal and neonatal mortality. The objective of this study was to examine the prevalence and individual and societal factors associated with IPV among Egyptian women. Cross-sectional data on 12,205 ever-married women between the ages of 15 to 49 years were collected from the Egypt Demographic and Health Survey (EDHS). Data from the 2005 and 2014 EDHS were pooled and analyzed. Self-reported responses on violence by husbands were classified into physical, sexual, and emotional violence. The factors of association were quantified using logistic regression methods. The prevalence of experiencing any form of violence among ever-married women in Egypt was 29.4%. Overall, women reported experiencing physical, emotional, and sexual violence at 26.7%, 17.8%, and 4.6%, respectively. Women in the age group of 25 to 29 years had the highest odds (odds ratio [OR] = 1.539, 95% confidence interval [CI] = [1.327, 1.785]) of suffering from any form of IPV. Women residing in urban areas (OR = 1.149, 95% CI = [1.046, 1.262]), having only a primary-level education (OR = 1.756, 95% CI = [1.543, 1.999]), being followers of Islam (OR = 1.713, 95% CI = [1.379, 2.126]), and having husbands with no education (OR = 1.422, 95% CI = [1.263, 1.601]) reported having higher odds of experiencing any form of IPV. Nearly one third of married women of childbearing age are exposed to IPV of any form in Egypt. IPV intervention programs should pay special attention to the socioeconomically vulnerable segments of the population and promote educational status among men and women to curb the occurrence of IPV.
Keywords
Background
Intimate partner violence (IPV) includes emotional, physical, and sexual coercion or assault by an adult partner or spouse (Holden, 2003). IPV is a global public health concern as women are widely targeted for abuse by their intimate partners, causing serious consequences to their personal health and well-being, as well as incurring costs at a societal level. In many cases, IPV is correlated with higher rates of morbidity and mortality among women in every country (Diop-Sidibé, Campbell, & Becker, 2006). IPV can result in acute medical conditions such as multiple injuries to the head and body, which can then be a cause for acquiring chronic conditions such as headaches, abdominal and pelvic pain, and sexual dysfunction (Campbell, 2002; Diop-Sidibé et al., 2006). IPV against women can also cause serious reproductive health and child delivery issues. Some of these issues include the inability to use contraception, unwanted pregnancies, an increased risk of sexually transmitted infections including HIV/AIDS, as well as premature labor, complications with delivery, and suffering through perinatal and neonatal mortality (Vyas, 2017; Vyas & Watts, n.d.). IPV is also associated with mental health issues including lowered self-esteem, depression, and anxiety (Abdelhai & Mosleh, 2015). Studies have found that children who observe IPV in their family households are more likely to be victims of abuse and become abusive themselves, in addition to suffering from feelings of helplessness, shame, guilt, and anger (Diop-Sidibé et al., 2006; Ellsberg et al., 2000). It is evident that IPV bears significant risks not only to the female victim in several ways, but also to her offspring (Diop-Sidibé et al., 2006; Ellsberg et al., 2000; Kishor & Johnson, 2004).
At a societal level, the cost of IPV is high and affects Egyptian communities as a whole. For instance, IPV can sustain the false belief that men are superior to women, and women deserve to be abused—snowballing the intergenerational cycle of IPV. Second, it is plausible that everyone’s quality of life suffers when the participation and productivity of abused women in social and economic activities are lessened. Third, the monetary estimates for direct service-related costs related to IPV are high in developing regions such as Egypt (United Nations International Children’s Emergency Fund [UNICEF], 2000). Overall, IPV against women ultimately affects their social, economic, and even political participation in society, which is undoubtedly costly to society as a whole (Day, 1995; Diop-Sidibé et al., 2006; Murshid & Murshid, 2018).
Discrepancies exist when comparing IPV in North American and European countries to those in Africa, Asia, Latin America, and the Middle East (Yount & Li, 2010). Research in this field indicates that women who live in poorer, more gender-stratified settings often experience more physical violence than men (Langhinrichsen-Rohling, 2010). In higher income countries, however, IPV is distributed rather equally between both sexes (Swan, Gambone, Caldwell, Sullivan, & Snow, 2008; Yount & Li, 2010). A major concern specifically in North Africa and the Middle East are the attitudes and perceptions of violence against women by both men and women (Boy & Kulczycki, 2008). Research indicates that women in these regions are conditioned to believe that violence toward them is justified and that they are partially responsible for the abuse that they suffer (Boy & Kulczycki, 2008; Yount et al., 2014). In Egypt, the most populous country in the Middle East, 86% of women believe that IPV against them is justified, with the highest specified reason being refusal of sexual intercourse (Boy & Kulczycki, 2008). This belief is also held by men and contributes to the significant gender inequitable attitudes that exist in the country (Haj-Yahia, 2002a). Furthermore, patriarchal structures, sexism and gender roles, and interpretations of the Islamic Sharia law have been found to contribute to these attitudes and beliefs that justify IPV against women in Arab societies (Haj-Yahia, 2002b; Yount, 2011).
The United Nations (UN) has identified gender equality to be one of the 17 Sustainable Development Goals (SDGs) developed to tackle social and economic inequities that exist worldwide. A UN report (2017) focusing on gender inequality (SDG 5) found that just over 52% of women between the ages of 15 and 49 years who are married or in union make their own decisions about consensual sexual relations, the use of contraceptives, and health services (UN, 2017). A high burden of this inequality with an emphasis on IPV exists in Middle Eastern countries, and much of this data is underestimated as a result of the political uprising that swept the Arab regions in 2011 (Vyas, 2017). During times of crises and conflict, women encounter a heightened risk of IPV as they face barriers to accessing legal, social, and economic protection (Heidari & Moreno, 2016; Vyas, 2017). Factors associated with IPV as a result of the high burden of gender inequality and the 2011 political uprising in Egypt are largely unknown. In this study, we compare the prevalence and predictors of IPV before and after the Arab uprising (i.e., in 2005 and 2014 respectively) and also examine pooled results from cross-sectional surveys that took place during these years.
Gender inequality, especially IPV against women, is a significant social and global public health issue requiring strategic intervention. It was therefore necessary to conduct this study to assess the prevalence and factors associated with IPV against women in Egypt. We anticipate that this study will lead to a clearer understanding of IPV among married women in Egypt and will help to identify the types of individual and community-based interventions that are needed to curb this public health issue.
Method
Data Source
Data for this study were collected from the Egypt Demographic and Health Survey (EDHS) conducted in 2005 and 2014. These are nationally representative population and health surveys conducted by El-Zanaty and Associates (Egypt) under the auspices of the Ministry of Health and Population (Egypt) (MOHP). The Demographic and Health Surveys (DHS) program and Inner City Fund (ICF) provided technical support to deliver the survey.
The sampling process for both the 2005 and 2014 surveys included three key stages. The first stage involved the selection of a primary sampling frame for urban and rural areas (MOHP, El-Zanaty and Associates, The DHS Program, & ICF International, 2015). The Central Agency for Public Mobilization and Statistics (CAPMAS) updated the lists that made up these frames to reflect the current populations during both EDHS.
Next, the primary sampling units (PSUs) were divided into parts of roughly equal size, with the number of parts determined by dividing the population in the villages by 5,000. A quick count was carried out as a quality control measure to estimate how many households were included in each part of each PSU. One to three parts were then systematically selected from each PSU, depending on the size of the villages.
The third stage involved selecting the household sample for each EDHS, respectively. A household listing was then obtained for each segment. Using the household lists for each segment, a systematic random sample of households was selected for both EDHS (El-Zanaty & Way, 2006; MOHP, El-Zanaty and Associates, The DHS Program, & ICF International, 2015). During the surveys, usual household members and visitors who were present in the household during the night before the survey visit were identified and listed in the household questionnaire. All ever-married women between the ages of 15 and 49 who were included in the list were eligible to participate in the individual survey interview. In the 2014 EDHS, a total of 21,903 women were identified as eligible of whom 21,762 were successfully interviewed, representing a response rate of 99.4%. Similarly, 22,807 households were selected for the 2005 EDHS, of which 22,211 were found and 21,972 successfully participated; again demonstrating a response rate of 99%.
All data were collected by female interviewers who were trained in basic interviewing techniques and on filling out the EDHS questionnaires. They also received lectures on specific EDHS topics such as fertility, maternal, and child health (El-Zanaty & Way, 2006; MOHP, El-Zanaty and Associates, The DHS Program, & ICF International, 2015).
Variables Selection and Measurement
The outcome variable of IPV includes several questions that focused on specific aspects of domestic and interpersonal violence, extracted to measure this outcome among married women in Egypt. The following questions addressed women’s experience of interpersonal violence, including acts of sexual, physical, and emotional violence:
a. Ever been pushed/shaken/thrown something by husband/partner: Never; Often; Sometimes; Yes, but not in the last 12 months.
b. Ever been slapped by husband/partner: Never; Often; Sometimes; Yes, but not in the last 12 months.
c. Ever had arm twisted by husband/partner: Never; Often; Sometimes; Yes, but not in the last 12 months.
d. Ever been punched with something harmful by husband/partner: Never; Often; Sometimes; Yes, but not in the last 12 months.
e. Ever been kicked by husband/partner: Never; Often; Sometimes; Yes, but not in the last 12 months.
f. Ever been humiliated by husband/partner: Never; Often; Sometimes; Yes, but not in the last 12 months.
g. Ever been threatened with harm by husband/partner: Never; Often; Sometimes; Yes, but not in the last 12 months.
h. Ever been physically forced to engage in unwanted sex by husband/partner: Never; Often; Sometimes; Yes, but not in the last 12 months.
i. Ever been forced into other unwanted sexual acts by husband/partner: Never; Often; Sometimes; Yes, but not in the last 12 months.
Scoring Procedure
IPV-related questions were computed in dichotomous forms—where “never” was recoded in negative = 0, but “often,” “sometimes,” and “Yes, but not in the last 12 months” were categorized for women’s lifetime experience of IPV (Yes = 1). Furthermore, these items were classified as sexual, emotional, and physical violence.
The Explanatory Variables
The explanatory variables that were assessed to be associated with the IPV outcome variables include the following:
Year: 2005 and 2014;
Age (years): 20-24, 25-29, 30-34, 35-39, 40-44, and 45-49;
Type of place of residence: urban vs. rural;
Religion: Christianity and Islam;
Education: no education, primary, and secondary;
Gender of household respondent: male vs. female;
currently working: no vs. yes;
Husband’s education: no education, primary, and secondary.
For the calculation household wealth index, the volume of durable goods (e.g., bicycle, TV, radio) possessed by the household as well as housing quality (e.g., type of building, floor, wall, and roof) was considered. Each item is assigned a factor score generated through principal component analysis which are then summed and standardized for the households. These standardized scores place the households in a continuous scale based on relative wealth scores. The scores thus obtained from a continuous scale and subsequently categorized into quintiles were used to rank the household as poorest/poorer/middle/richer/richest. Furthermore, poorest and poorer categories were merged making the “poor” group, and middle, richer, and richest were merged to make the “non-poor” group.
Ethical Considerations
All participants provided informed consent prior to taking part in the survey. Ethical procedures were the responsibility of the institutions that commissioned, funded, or managed the surveys. All DHS are approved by ICF international as well as an institutional review board (IRB) in respective countries to ensure that the protocols are in compliance with the U.S. Department of Health and Human Services regulations for the protection of human subjects. Therefore, this study required no other ethical approval.
Data Analysis
To adjust for data representation, we used complex survey module for all analyses to account for clustering, stratification, and sample weight. For multicollinearity diagnostics, a correlation value of .7 was used to examine interdependence of explanatory variables. The correlation matrix values fell below the cut-off confirming lack of multicollinearity to raise concerns of removing interdependent variables from the model. Therefore, all explanatory variables were added in the model. The sociodemographic characteristics of the participants were presented as percentages. In addition, the prevalence of IPV was calculated for the years 2005 and 2014. Variables that showed association with a p-value <.05 in the bivariate tests were retained for the multivariable analysis. In the final step, multivariable binary logistic regression model was used to estimate the odds ratios (ORs) and 95% confidence interval (CI) of the associations between intimate partner’s violence including physical, emotional, sexual, and any IPV and the explanatory variables. Data were analyzed using STATA version 14 (StataCorp, College Station, TX).
Results
Demographic Information of Married Women in Egypt
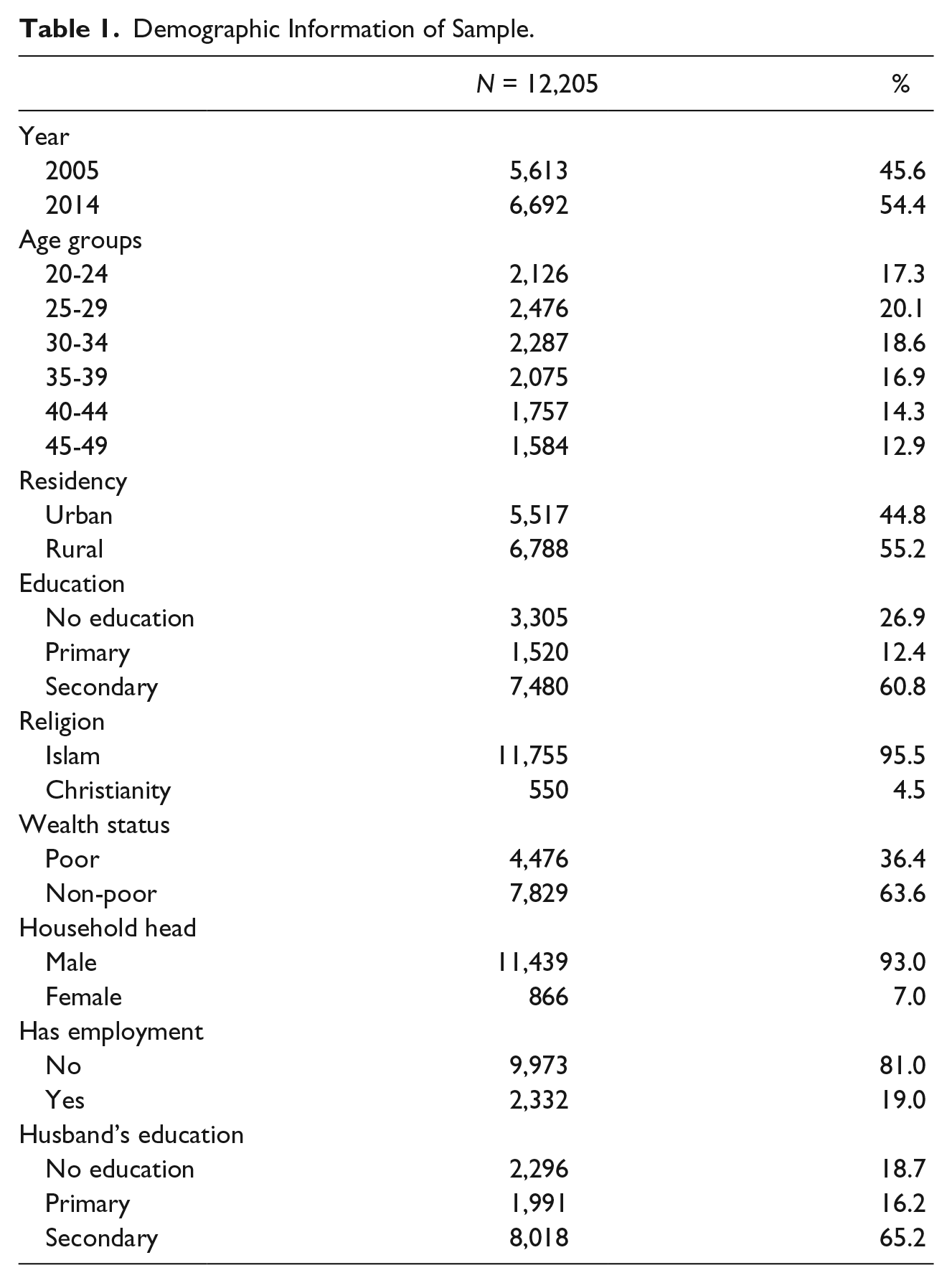
Table 1 numerically displays the characteristics of married women who participated in the 2005 and 2015 EDHS. A total of 12,205 married Egyptian women participated in the 2005 and 2014 EDHS. Approximately, one fifth of the women who were interviewed ranged in age from 25 to 29 years, and over half (55.2%) of them resided in rural regions within the country. Over half of the married women and their husbands who were surveyed had secondary-level education, with more men having this level of education than women, at 65.2% and 60.8% respectively. As shown below, the level of education among the women varied considerably. Over a quarter had never attended school, while significantly over half (60.8%) completed at least secondary-level education. Furthermore, over 95% of the women came from an Islamic religious background, and a majority of them were unemployed. Male breadwinners headed a majority of the family households, and this may potentially be another reason for the stark power imbalance in Egyptian married couples, possibly contributing to different aspects of IPV.
Demographic Information of Sample.
Prevalence of IPV Among Married Women in 2005 and 2014
Table 2 presents the prevalence of all types of IPV against married women in Egypt based on the 2005 and 2014 EDHS data and a pooled analysis of data from both years. Overall, 29.4% of married women included in this study reported having experienced some form of violence from their husbands. Physical violence is observed to be the most common form of IPV against married women in this study, with slapping being the most prevalent form of this violence (22.7%); followed by being pushed, shaken, or having something thrown at them (19.6%); and arm twisting (18.1%). Emotional violence was the second most prevalent form of IPV and included being humiliated (13.6%) or threatened with harm (5.2%). Interestingly, sexual violence was the least prevalent, with 4.5% of married women reporting being physically forced to engage in sexual intercourse, and 3.1% reporting that they were forced to perform other sexual acts.
Prevalence of IPV.

Based on the EDHS data from both 2005 and 2014, it is clear that there has been a reduction in almost all types of IPV in Egypt since 2005. However, despite a reduction in both physical and sexual violence, there is a slight increase in reported emotional violence experienced by married women. Physical violence, the most prevalent form of IPV in Egypt, decreased the most between 2005 and 2014, with a 6.4% reduction in the 9 years between both national EDHS. A 1.9% reduction is observed in the prevalence of sexual violence, while an increase by 1.5% in the prevalence of emotional violence from 2005 to 2014 has also been observed. Overall, there is a 1.5% reduction in any form of violence observed within this time frame (Table 2).
Factors Associated With IPV Among Married Women in Egypt
Table 3 presents a multivariate analysis of the factors associated with IPV against married women in Egypt. Married women aged 44 and below had higher odds of experiencing IPV compared with married women aged 45 to 49 years old. Furthermore, the odds of experiencing IPV (sexual violence) in women with an Islamic religious background were 2.19 times higher (95% CI = [1.228, 3.922]) as compared with women who were Christians. Women whose husbands had no education were 1.51 times (95% CI = [1.179, 1.923]) as likely to experience sexual abuse compared with women whose husbands had attained the secondary level of education. The odds of women with only a primary-level education experiencing physical violence were 1.83 times (95% CI = [1.607, 2.093]) higher compared with women who had attained secondary-level education.
Factors Associated With IPV in Egypt (Multivariate Analysis).
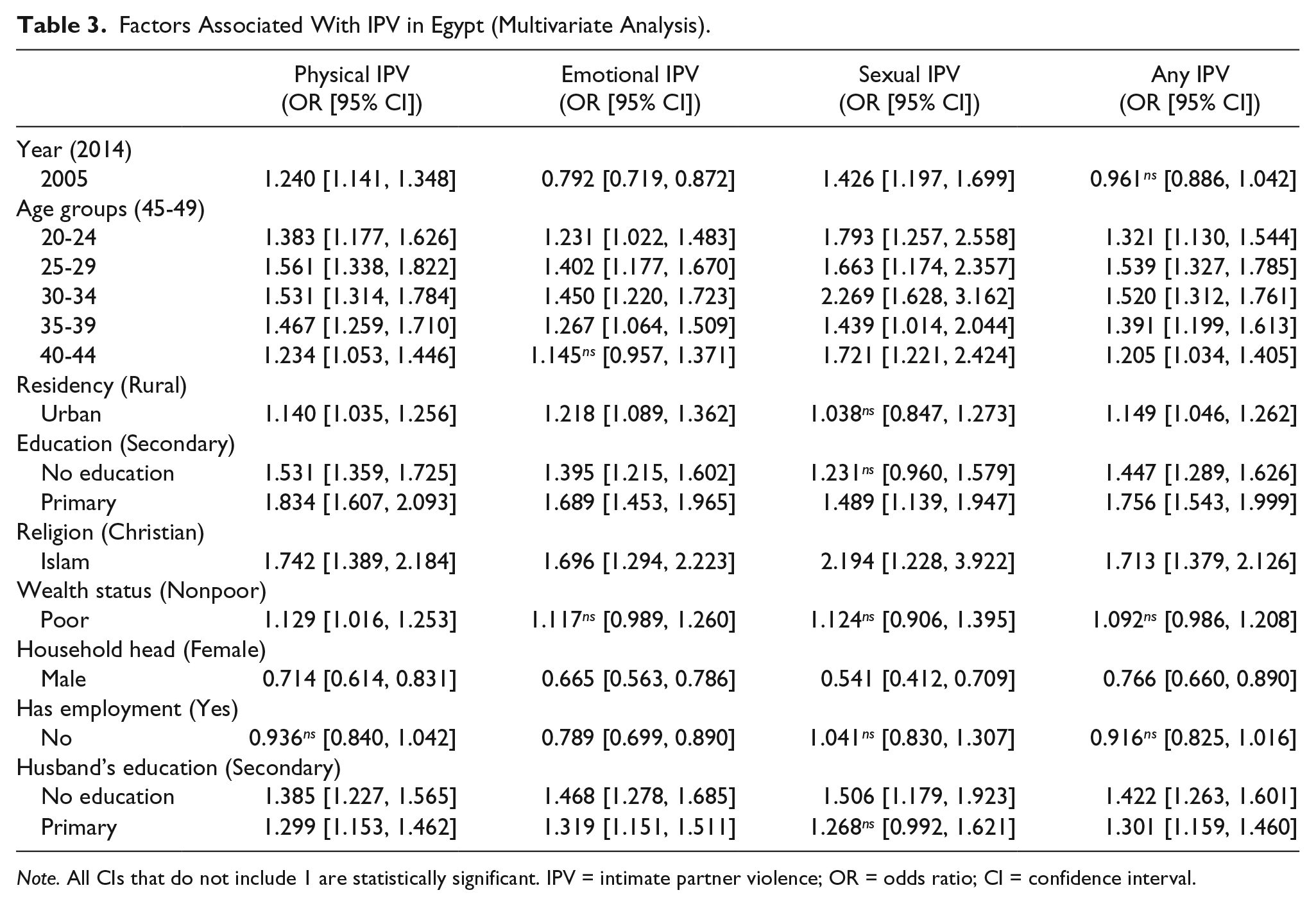
Note. All CIs that do not include 1 are statistically significant. IPV = intimate partner violence; OR = odds ratio; CI = confidence interval.
Also, results showed that women who resided in urban areas were 1.22 times (95% CI = [1.089, 1.362]) as likely to experience emotional violence compared with women who resided in rural areas. Poorer women reported higher odds of experiencing physical violence from their husbands (OR = 1.129, 95% CI = [1.016, 1.253]) compared to women with nonpoor wealth status. Women’s employment status was not statistically associated with experiencing physical or sexual violence; however, women who were unemployed had a decreased odd of experiencing emotional violence (OR = 0.789, 95% CI = [0.699, 0.890]) in comparison to those who were employed. Furthermore, women were less likely to be emotionally abused but were more likely to be sexually abused by their husbands in 2005 in comparison to the EDHS data collected in 2014.
Discussion
This study examined the prevalence of IPV among married women and also investigated the factors associated with IPV among Egyptian women using data from the EDHS conducted in 2005 and 2014. The results showed that nearly one third of women of childbearing age have experienced some form of IPV in Egypt. The common types of IPV experienced by Egyptian women include physical violence, emotional violence, and sexual violence. In the multivariate logistic regression analysis, the results revealed that the factors that had a statistically significant association with woman experiencing IPV included being between the ages of 25 and 29 years, residing in urban areas, having only primary-level education, being a follower of Islam, and having a husband with no education.
The prevalence of IPV revealed in our study reflects results reported by the World Health Organization (WHO) in 2013, which state that 1 in 3 women globally experience physical and/or sexual violence by a partner or sexual violence by a non-partner (WHO, 2013). The IPV prevalence reported in this study is also closely similar to the 30.5% prevalence of any violence against women reported in Nigeria (Bamiwuye & Odimegwu, 2014). However, the IPV prevalence in this study is far lower than the 52.83% and 54% IPV prevalence reported in other sub-Saharan African studies (Beyene, Chojenta, Roba, Melka, & Loxton, 2019; Karamagi, Tumwine, Tylleskar, & Heggenhougen, 2006). Globally, the Eastern Mediterranean region has the second highest IPV prevalence rate, following South-East Asia (WHO, 2013). The results indicated an improvement in the situation between 2005 and 2014, with a clear reduction in almost all types of IPV (except for emotional). This is however not representative of the general population as we studied the married women only where interpersonal violence is more likely to occur. Physical violence, being the most prevalent form of IPV in Egypt, was the one that showed reduction by largest percentage point among all three forms of IPV—6.4% reduction between 2005 and 2014, compared against the 1.5% reduction in any form of IPV.
With regard to the factors associated with IPV, our study revealed that a woman’s place of residence and educational level are associated with her exposure to some form of IPV. This finding is consistent with the results of other studies that have also reported place of residence and level of education to be significantly related with IPV (Beyene et al., 2019; Karamagi et al., 2006). Nevertheless, this study also revealed women’s age (25-29), Islamic religious beliefs, and husband’s education to be significantly associated with IPV. These findings are inconsistent with the results of other studies that have found women’s household wealth status, marital status, and substance abuse to be associated with IPV (Bamiwuye & Odimegwu, 2014; Beyene et al., 2019). Based on the results of this study, there are some clear predictors of various forms of IPV that need to be given special attention by local, national, and international decision-makers. For example, although IPV has generally decreased since 2005, the prevalence of emotional violence experienced by married Egyptian women has increased since then. In the multivariate analysis, the odds of reporting emotional IPV in 2005 was significantly lower compared with 2014. The demographic information listed in Table 1 demonstrates that about three fifths of women in Egypt have at least a secondary level of education, yet a majority of women are unemployed and live in male-headed households. The multivariate analysis in Table 3 indicates that despite receiving even some level of education, women are still exposed to all forms of IPV. Furthermore, most families residing in Egypt are Muslim, which was found to be a factor associated with experiencing all types of IPV with an emphasis on sexual violence, which is surprising given the values that the religion promotes among its believers. Moreover, a majority of the women sampled in the survey reported having a nonpoor wealth status. However, this factor was not significantly associated with women being exposed to emotional or sexual violence by their husbands. These are a few examples of unexpected correlations, which may be explained by the cultural attitudes and beliefs of the population over time.
Evidence suggests that one of the largest issues that challenges the prevention of IPV in the Middle East including Egypt are the cultural attitudes and beliefs of the women who suffer the abuse. Many women justify this abuse and commonly believe they deserve it. Data from five small-scale studies from the Middle East and North Africa that investigated the beliefs of women and IPV demonstrated several reasons why physical abuse was justified (Boy & Kulczycki, 2008). These reasons included infidelity, disobeying the husband, nagging or insulting the husband, dishonoring the family, neglecting the children, burning food, and other kitchen-related problems (Amowitz, Kim, Reis, Asher, & Iacopino, 2004; Haj-Yahia, 1998, 2002b; Khawaja, 2004; Maziak & Asfar, 2003). Furthermore, DHS data from Jordan and Egypt demonstrate different rates of justification from women for physical violence that they experienced from their husbands. In Jordan, 83% of women justified abuse if they betrayed their husband, 60% if they burnt a meal, and 50% if they disobeyed their husband (Government of Jordan & ORC Macro, 2003). Whereas in Egypt, 70% of women justified physical abuse if they refused to have sex with their husbands (Boy & Kulczycki, 2008; El-Zanaty, Hussein, Shawky, Way, & Kishor, 1996). Contrary to the expectation that the less educated women are, the more likely they are to justify this type of abuse, this was not the case based on the results of the multivariate regression conducted for this study.
Further research is required to understand the attitudes and beliefs of men, women, and other informants as they relate to IPV. This research must extend to attitudes and beliefs that go beyond those of physical violence, which seems to be the most prevalent, but is also easier to identify and report. Data from this study suggest that emotional violence is the second most prevalent after physical violence among this target population. However, more research is needed to explore what this violence entails, why it takes place, and how the women themselves address it. Two studies from Israel and Sudan indicated a lack of discussion about IPV among doctors and their women patients, due to various reasons including the following: limited awareness of the issues, perceived inability to assist victims, and cultural and professional pressures to avoid the issue altogether (Ahmed, Abdella, Yousif, & Elmardi, 2003; Boy & Kulczycki, 2008; Kahan et al., 2000). This is one identified barrier preventing women from receiving required and adequate care and support as they suffer the consequences of physical, sexual, and emotional abuse.
Currently, there are limited interventions to combat IPV against women in the Middle East and North Africa, and this is not surprising given the attitudes and beliefs surrounding the issue. Few countries have enacted laws against IPV let alone implemented them, and social service organization are limited in the assistance they are able to offer for various reasons (Nazir, 2005). Many Arab societies impose restrictions on a woman’s ability to obtain a divorce, as it is perceived negatively in society and according to their interpretations of Islamic law; and as a result, women have to continue to endure the various types of IPVs that they suffer (Haj-Yahia, 2002b). For interventions that focus on changing attitudes and beliefs about individual and community-level health behaviors, psychosocial models such as the health belief model and social learning theory should be considered (Nutbeam, Harris, & Wise, 2010; Yount & Li, 2010). Girls must be socially and economically empowered early on, before marriage, to stand up for their rights, health, and safety—and to do this cooperation, advocacy, and support is required from the government and broader community (Vyas, 2017). Law enforcement authorities must also take this issue more seriously and refer victims to the appropriate social support services that can provide these women with the tools, resources, and support they need (Boy & Kulczycki, 2008). Furthermore, there is a need for more research to explore the attitudes and beliefs of Egyptian men, and different stakeholders such as physicians and social support workers involved in the care and programming associated with IPV. Although IPV is common nationwide, special efforts should be made to address the issue in urban region where odds of experiencing any form of IPV (other than sexual) were found to be higher.
The 2014 EDHS includes new information about husband’s substance use, women’s history of family violence, and the extent to which the husband exhibited jealousy or attempted to control women’s interaction with family or friends. This information was not collected in the 2005 DHS but should be compared in the next EDHS to explore any change as a result of ongoing interventions (Yount & Li, 2010). Finally, the data were cross-sectional and hence no causal relationship can be established from the findings.
Strengths and Limitations
This study was based on nationally representative secondary data. Findings of this study are generalizable to women in Egypt who range from 15 to 49 years of age. As discussed, the sample size for this study is considerably large with 12,205 married women being interviewed from across the country in both the 2005 and 2014 EDHS. EDHS samples were selected in three stages, and geographic stratification was implemented (MOHP, El-Zanaty and Associates, The DHS Program, & ICF International, 2015). One of the main limitations to this study is the self-reported nature of the data. This could have potentially heightened the risks of recall and reporting biases. The nature of the IPV topic may also be underreported as it is a sensitive subject about which women may choose to refrain from speaking because of their discomfort in revealing this information to interviewers with whom they have not had the opportunity to build trust or rapport, and/or fear in disclosing personal information without their husband’s consent. Furthermore, it is important to acknowledge that national data in Egypt focus exclusively on married women, and hence IPV overall may be underreported. This is because cohabitation without marriage is illegal, and therefore unmarried women are not considered for interviews to collect data about IPV as this would be culturally insensitive (El-Zanaty & Way, 2006). As a result, it is possible that DHS statistics for IPV against women underreport physical, sexual, and emotional violence by excluding unmarried women. Furthermore, the outcomes and severity of emotional violence are harder to assess and report. Therefore, it is recommended that more survey questions from the WHO Core Questionnaire be included in the EDHS to truly measure the extent of emotional or psychological violence experienced by women (Yoshihama, Horrocks, & Kamano, 2009).
Conclusion
Almost one third of married women are exposed to IPV of any form in Egypt. Factors that had statistically significant association with women experiencing IPV include being of age 25 to 29, residing in urban areas, having primary level of education, following Islam, and having a husband with no education. Interventions to prevent IPV among this part of the Arab world must target those who are socioeconomically vulnerable by promoting education and employment. Prevention programs should focus on educating families about the negative health outcomes associated with IPV, and influential religious and community practices should come forward to promote this type of teaching to prevent IPV from continuing to be a threat to women and children’s health.
Footnotes
Authors’ Note
Sanni Yaya is also affiliated with The George Institute for Global Health, University of Oxford, Oxford, United Kingdom.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.