
Abstract
Child sexual abuse (CSA) remains a major public health concern worldwide. In Africa, particularly, Nigeria, CSA is a silent, but lethal public health menace with prevalence reaching as high as 56% for different child sexual violence. Understanding the vulnerability factors of CSA promotes the creation of strategies toward prevention of CSA. Due to social stigmatization of victims and their families in Nigeria, it is difficult for researchers and policymakers to have access to firsthand information about predisposing factors to CSA, which negatively impacts efforts toward prevention of CSA. Health care professionals are sources of experience-based, anonymous information about various public health issues. This study aims to understand qualitatively health care professionals’ perception of vulnerability factors of CSA. The study presents a thematic content analysis of a semi-structured interview of 14 health care professionals working with sexually abused children in Nigeria, on their perception of vulnerability factors of CSA, while aligning the factors with known models of violence. Participants in the study reported several interrelated vulnerability factors involving the individual, sexual abuse perpetrator, family, environment, socioeconomic situations, and the lack or nonimplementation of policies against CSA. The study concludes that identifying these factors can assist health care professionals, parents, and family to better respond to child sexual violence cases and policymakers to create new strategies of preventing CSA, thereby improving the health and safety of children in Nigeria.
Introduction
Child sexual abuse (CSA) remains a major concern worldwide and has been designated as an epidemic and public health crisis by the World Health Organization (WHO, 2004). It has been identified as a human and sociocultural problem that negatively impacts the lives of victims and the society (Guma & Henda, 2004). Globally, more than half of all children (estimated as 1 billion children) have been reported to have experienced sexual violence in a review of 112 research works from 96 countries (Hillis et al., 2016). In the United States, one out of four girls and one in six boys were estimated statistically to possibly experience sexual abuse before they turn 18 years (Townsend & Rheingold, 2013). In addition, about 12.3% of women had their first sexual experience before age 10, whereas about 30% of women had their first sexual experience between ages 11 and 17 (Black et al., 2011). Children and adolescents have been reported to have a high tendency of being vulnerable to sexual violence because of their characteristics of low discernment of abusive situation and poor decision-making skills which may be associated with their low level of maturity, and certain cultural and societal factors including the culture of respect and obedience to elders (Krug et al., 2002; Nadan et al., 2015).
In Africa, particularly Nigeria, CSA is a silent, but lethal public health problem which has continued to ravage children and adolescents. Reports and data of sexual violence in the literature and from nongovernmental organizations identified children as the major sexual violence victims attended to in Nigerian hospitals, with the prevalence rate being as high as 56% for diverse forms of childhood sexual violence (Abdulkadir et al., 2011; Ige & Fawole, 2012). For children in sub-Saharan Africa, in addition to the physical and sociopsychological consequences of CSA, there is the added troubling situation of possible infection of these innocent children with sexually transmitted diseases including HIV/AIDS (Bugaje et al., 2012), suggesting the need for urgent strategies that can reduce or eradicate this menace.
Although some current efforts by governmental and nongovernmental organizations in Nigeria are being directed toward helping survivors of CSA, it is understood that the best practices in response to CSA in many countries, in addition to rehabilitating survivors and punishing offenders, involve creating preventive strategies and policies that are derived through understanding of the vulnerability factors that predispose children to CSA (Ward & Sorbello, 2003). Recognizing these factors will be a positive step to effectively and efficiently prevent and advocate against CSA within the society. One way to understand CSA vulnerability factors that may expose a child to CSA is through accounts by victims and their families; however, in Nigeria, due to social stigmatization of victims and their families, it is mostly difficult for researchers and policymakers to have access to such children or their family, making little or no information available on vulnerability factors of CSA (Hassan et al., 2016; Tillman et al., 2010). In addition, history has shown that some sexual abuse offenders are family members or close relations, and with cultural norms in Nigeria tilting toward nondisclosures to prevent generational family feuds, most victims and their families cover up the situation (Boakye, 2009; Daru et al., 2011), making it further difficult to access real information about predisposing factors to CSA, thus prompting the need for an alternative information source on CSA vulnerability factors.
Health care professionals are a good source of professional, experience-based and anonymous information about diverse public health concerns, particularly topics related to CSA (Levenson et al., 2010). Currently, no study has reported health care practitioners’ perception of CSA vulnerability factors in Nigeria. Thus, this study aims to qualitatively understand and elucidate vulnerability factors predisposing Nigerian children to CSA through an experience-based perception of health care practitioners that have had contact with CSA victims. Qualitative analysis deploys descriptive and exploratory research strategies to provide detailed information about a subject of interest through a subjective assessment of human conduct, emotion, opinions, and personality characteristics and guided by the perspectives of respondents to a research question of interest, which may not be matched by a quantitative approach (Minayo, 2010; Richard, 2013). It often creates a trusting and interactive relationship between researchers and respondents, making way for collection of firsthand valid data, describing new findings which may lead to new theories or modification and expansion of known ones (Carr, 1994; Kothari, 2004). It is hoped that information gathered through this study will provide insights into CSA vulnerability factors and assist policymakers in designing adequate prevention policies that fit the current-day CSA situations and promoting awareness about this menace.
Models of Violence
Models and theories have been used to explain violence and characterize vulnerability factors of violence. The ecological model was initially used to understand violence against children (Garbarino & Crouter, 1978), but has also been applied to explain the sources of exposure to youth and intimate partner violence (Garbarino, 1985). The model emphasized that no single factor can explain why some people are more vulnerable to violence than others, but that vulnerability to violence is an interaction between diverse factors such as biological, social, cultural, economic, and political, operating at four ecological levels of individual, community, relationship, and societal as depicted in Figure 1.
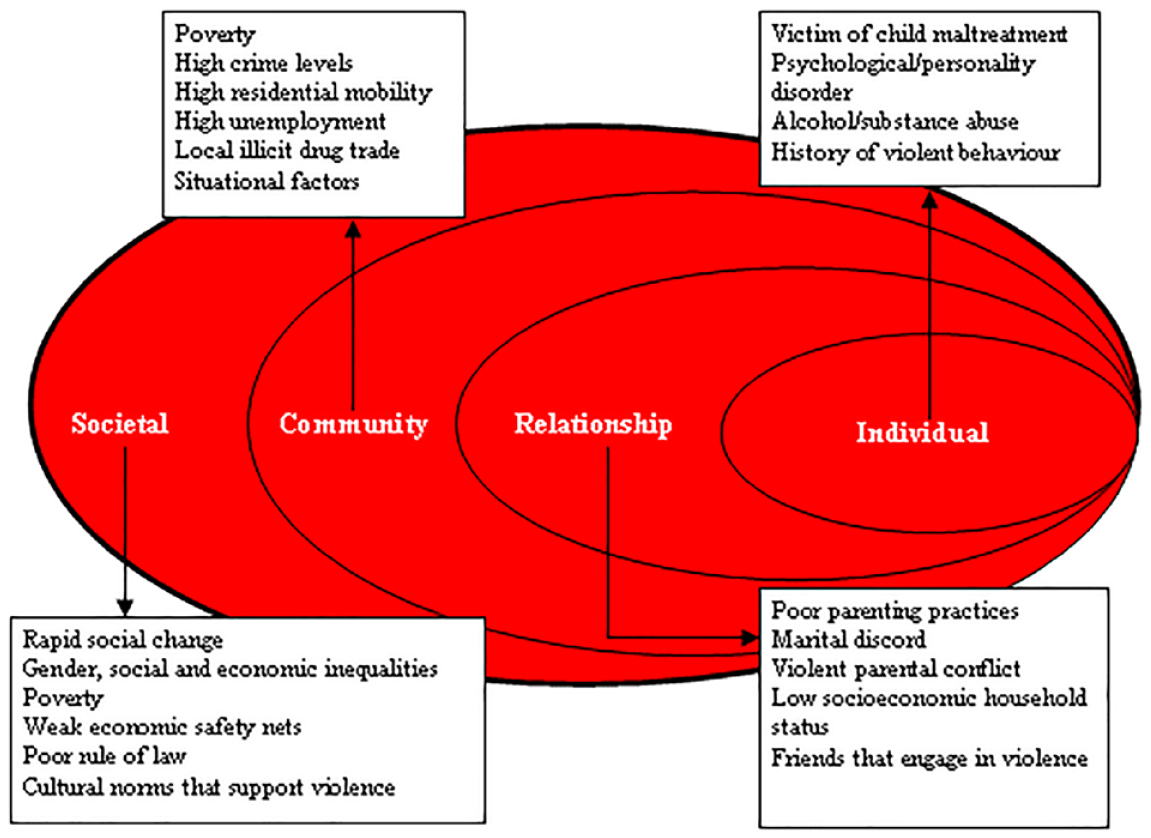
Ecological framework showing examples of risk factors.
The vulnerability theory explains new strategies deployed in reducing risk of violence in the environment. It was used in 1993 to explain individual and collective vulnerability among HIV/AIDS populace (Mann et al., 1996), but has also been applied to different aspects of health challenges (Ayres, 2016). The vulnerability theory is hinged on three dimensions of vulnerability identified as individual, social, and programmatic vulnerability (Ayres, 2016).
These theories were chosen because their fundamental structure is based on evidence that no single factor may explain exposure to interpersonal violence, but that interactions between different factors often explain the elements of interpersonal violence. The theories explain the individual and social dimensions that often make children and adolescents vulnerable to sexual abuse in an environment. The individual level in both theories explains the personal characteristics of both the victim and the violence perpetrator. The community, relationship, and societal levels described under the ecological model explain similar concepts of social and programmatic vulnerability dimensions described under the vulnerability theory. The two theories support and reinforce the information gathered through the health care professionals’ experience-based perception of vulnerability factors of CSA.
Method
Study Design
A qualitative approach, which was adopted in this study systematically identified and analyzed perceptions and opinions attached to CSA vulnerability factors in Nigeria by professional health care providers, and the information gathered could be useful in formulating CSA prevention and intervention programs. The design was guided by two theoretical frameworks—ecological model and vulnerability theory—the conceptual basis of which provided the foundation that was used to critically analyze CSA vulnerability factors in this study.
Data Collection
Data were collected in 2018 through a face-to-face semi-structured interview of health care professionals who have experience with CSA victims at the family health unit of the Lagos State University Teaching Hospital (LASUTH), Ikeja, Lagos, Nigeria. This health institution was chosen because it is located within the heart of the largest economy, commercial and most urban-populated state in Nigeria, Lagos, and has the highest number of health care professionals with experience in CSA. These health care professionals voluntarily work with CSA victims at private establishments and nongovernmental organizations that support CSA victims. Interviews with participants were prescheduled to avoid unnecessary interferences during the interview sessions. Interview sessions conducted with respondents lasted between 12 and 51 min, with an average of 25.6 min. The amount of time was considered adequate after participants ran out of information and the information provided met the goals of the research questions. The interview script included two important open guided questions of “what does child sexual abuse mean” and “what factors make victims vulnerable to child sexual abuse.” In addition, other questions such as “how do victims disclose the occurrence of the abuse” prompted by a participant’s response were asked to clarify or understand the context of such participant’s response. Before each interview session, the interviewer discussed the ethical aspects of the study with the participants and consent forms were signed. All interviews were conducted by the same person in participants’ personal offices where there were no interruptions.
The data collection procedure was approved by the Board of Examiners, Department of Public Health, School of Nursing, University of Sao Paulo in Ribeirao Preto, Brazil and the National Health Research Ethics Committee, Nigeria (NHREC) before interviews were conducted. The data collection procedure also involved a familiarization meeting with prospective participants at the family health unit of LASUTH. Familiarization with participants in qualitative studies often enable better understanding of an organization, establishing relationships of trust, which could assist in gathering credible data from research participants (Shenton, 2004).
Study Participants
Participants for this study were selected based on three selection criteria: The participant (a) must be a health care professional; (b) must have worked in the health unit for at least 6 months; and (c) must have worked with at least three victims of CSA. In addition, the participant must be willing to participate in the study.
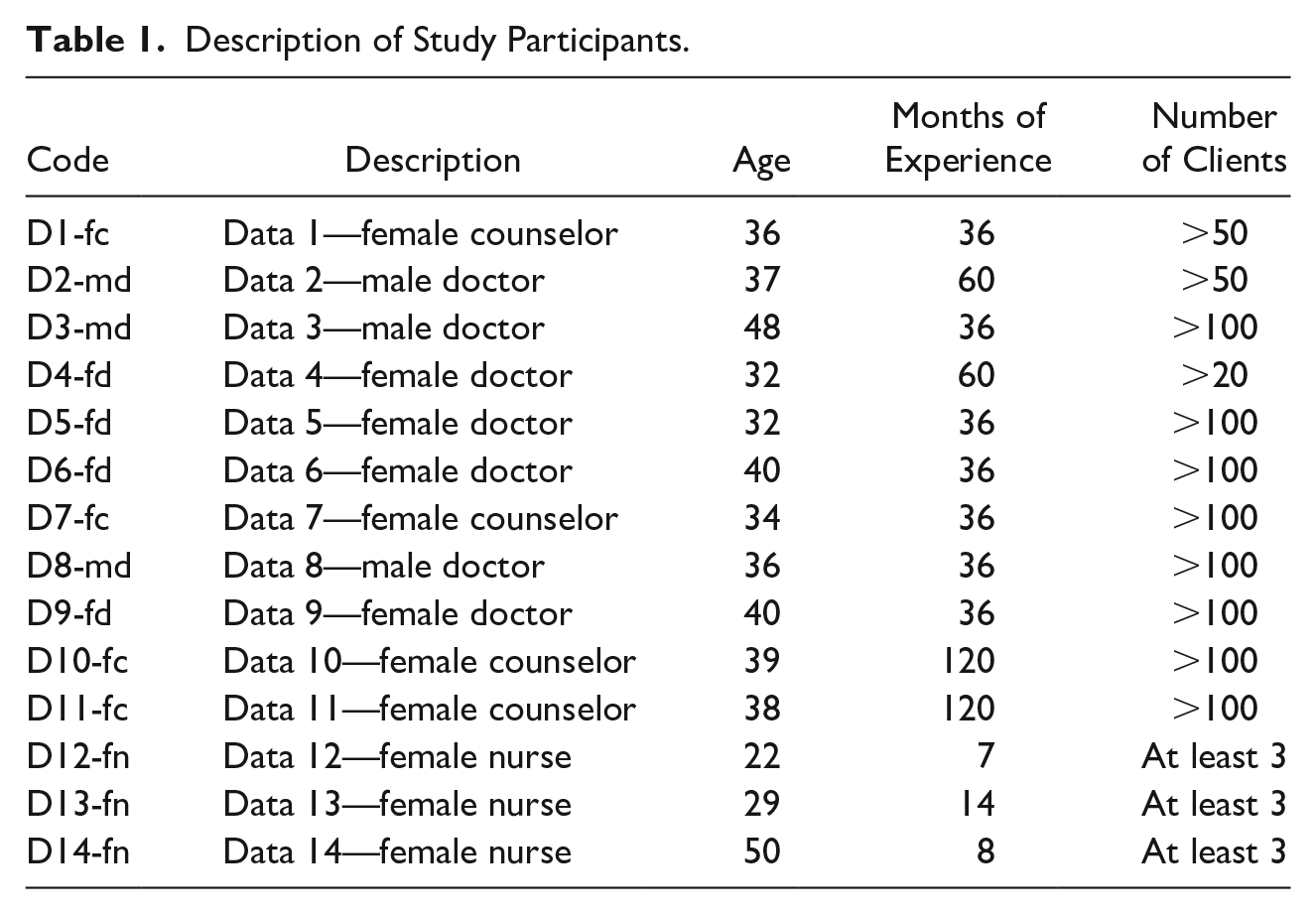
A total of 55 medical and administrative staff were employed in the health care unit, whereas only 14 participants met the selection criteria and agreed to participate in the study. Nine health care professionals who met the selection criteria but did not participate did so because some have tight schedules which prevented scheduling an interview, and two were not comfortable giving information about CSA due to confidentiality and other personal reasons. The participants were composed of seven medical doctors, three nurses, and four psychologists/counselors, which included three males and 11 females from different cultural and religious backgrounds. The participants were well educated with the least level of education being a bachelor’s degree, whereas eight (57%) participants had a postgraduate education in their respective profession. The average age of participants was 36.6 years with age ranging between 22 and 50 years. The average participants’ experience with sexually abused children was 45.8 months (approximately 4 years) with experience ranging between 8 and 120 months and their contacts with victims were two or three times a month depending on occurrence and nature of abuse. The least number of clients attended to by each participant was 3, whereas the most was more than 100. Table 1 provides the summarized description and codes of the health care professionals interviewed in this study.
Description of Study Participants.
Data Analysis
Data collected from participants were organized and analyzed using ATLAS.ti (version 8), a qualitative data analysis and research software. A thematic content analysis (Bardin, 2011) was performed and the data were aligned with the concepts of the ecological model and vulnerability theory discussed previously.
The thematic content analysis was composed of three phases, namely, preanalysis, material exploration and treatment of the results, and inference and interpretation. The preanalysis phase involved data transcription into written form, classification and organization of data, formulation of objectives, and elaboration of final interpretation indicators, with all memos and comments well articulated in the ATLAS.ti software.
The second phase (exploration and treatment of data) involved attentive reading of material to establish deep understanding and identify central points of the text relevant to CSA vulnerability factors. At this stage, quotations from the text were selected and attached to codes that best capture perceived vulnerability factors of CSA before grouping them into categories. To further refine coding categories, line-by-line coding of a randomly selected sample of cases was carried out by the first author, whereas the principal investigator, an established qualitative researcher, finalized the coding categorization by conducting a line-by-line coding of randomly selected samples (Creswell & Creswell, 2017). The coding and categorization processes were finalized after the first author and principal investigator reached an intercoder reliability of >.90 (Lombard et al., 2005).
The third phase (inference and interpretation) allowed the establishment of meaningful and valid understanding of analyzed results by associating relationships among quotations, codes, and memos. It involved the interpretation, critical evaluation, and presentation of results by creating an interface between the main findings by the researcher and the theoretical content of the study. The categorization of quotations and the construction of thematic nucleus for analysis in this study are described in Table 2.
Construction of Thematic Nucleus.

Source. Authors (2018).
Note. CSA = child sexual abuse.
Results
This study specifically presents interview themes that are related to factors influencing sexual abuse among Nigeria children as perceived by health care professionals through their day-to-day activities with their CSA victims. Through narrations by the health care professionals, four thematic nuclei that focus on the study interest were developed and this study is discussed within the purview of these four thematic nuclei.
Vulnerability of Victims to CSA
The health care professionals interviewed identified the child victim’s identity as one of the most important factors in understanding and dealing with CSA. This identity varies from one child to another and includes age factor, which was identified by all the participants in addition to other biologically related factors such as personality and early development of a child. Moreover, individual vulnerability was characterized by innocence, trust, and lack of information on the part of child victims.
Participants identified that the majority of their clients who reported at the medical unit were young children with ages far below 18. They perceived that the high rate of sexual abuse among children is due to the ability of perpetrators to take advantage of a child’s incapacity and inability to adequately discern or judge a sexual abuse situation. In a similar manner, poor understanding of sexual abuse caused low/no disclosure of the abuse by child victims. For instance, Participant D4-fd noted that abusers take advantage of poor children who cannot defend themselves: ((Erm)) it’s just has to do with the fact that . . . ok, this people are small, they can’t probably defend themselves and ehm . . . somebody just took advantage of that . . .
Participant D4-fd has a good understanding of the abilities of young victims of CSA and how these abilities are being targeted by perpetrators to satisfy their sexual needs. Similarly, Participant D8-md opined that poor discernment of sexual abuse by victims is also a vulnerability factor: that they are less likely to report . . . ehm to report the perpetrator, the fact that children don’t really understand what is going on, the fact that they are being sexually assaulted.
Vulnerability to CSA not only is due to a victim’s poor understanding of sexual abuse, but is also associated with a child victim’s innocence, which is embedded within trust as reported by some of the participants. Victims were generally characterized with an unconscious ability to easily relate with people, but with no ability to differentiate good behaviors from bad ones within the society. A child’s ability to trust bothers around people’s reliability, show of affection, and generosity in terms of gifts, making them easily put their faith and trust in people. The innocence characterized by this group of people was narrated by Participant D11-fc: They are innocent, (innocent in what sense?) if you look at their age range, they feel free with anybody, you won’t believe that “Uncle Tunji” that I have been playing with can do this, Uncle Tunji that is my brother’s friend, out of their innocence, feel free to Uncle Tunji’s room, sit down and do whatever they want to do and even when Uncle Tunji starts, they might not know where Uncle Tunji is going. Most of them don’t know, they don’t even think around that area . . .
This innocent behavior of CSA victims was characterized by immature sexual nature, sexual naivety, poor decision-making skills, and sexual consent incapability.
The absence of valuable information that can improve a child’s decision making in an abusive situation could also be a risk factor. Participants emphasized the conservative nature of most Nigerian homes and cultural beliefs that tend to treat sexual education and sexual abuse information as sensitive information, so they often keep children out of such discussions. Although Participant D6-fd highlights this as a risk factor, she excluded children below age 3 as they are often believed not to be cognitively developed to process such sensitive information. In addition, lack of an age-appropriate method of communication about CSA may predispose a child to an abusive sexual situation.
Of course, ehm . . . especially for children usually, let me say from age 3 and above. I believe that if they have a better knowledge about sex education, probably it will help and erm . . . but or a child 3month, 1 year . . . It doesn’t really make any difference. In fact, for those children, we’ve seen some that they grew up to become perpetrators themselves because they never knew it was wrong, it was probably those that live in their house and has been doing that since they were 6month and it continues since the child was 3 or 4, and he didn’t even know this thing was wrong until maybe he started practicing on other children . . . (D6-fd)
In addition to the individual vulnerability of victims, health care professionals described personality and early development of some children as a contributing factor to CSA within the society. Participant D2-md noted that perpetrators tend to often approach children whose personalities are mostly characterized as “extreme,” describing them as either the very extroverted children who are generally outspoken and energetic or very introverted children who are generally quiet and keep secrets.
. . . you know we have these kids who are very outspoken, who does, who are very energetic . . . who are just all over, they can jump, they can do everything, sometimes you see these perpetrators see them as people who wants to be touched, have seen a lady told me that “the way I play everything, some people thought I want sex” . . . (D2-md)
Participant D2-md described that early growth and development in children could be an influencing factor that may attract sexual abuse perpetrators to children. He emphasized physical body features of CSA victims as a risk factor based on the accounts of child victims he has managed: oh, yeah, sometimes you know the children that are on the big side tends to be more abused, in short, most of my survivors who are on the big side told me, in fact one of them was telling me that I have always been big from childhood, so every man, every person that comes around easily sees her and you see the small ones who are tiny, people don’t reckon with them so you see a 9, 6, 7 year old who is already big, some of them are already having little burden of breast tend to be more sexually abused, so I won’t call it pre-causal puberty, they just tend to grow, nutritional value, grow faster, so the bigger ones even though their age . . . they are still young, but they are tending to be more abused . . .
In summary, the first thematic nucleus of vulnerability as described by participants suggested that the victim’s identity such as the chronological age factor of a child characterized by innocence and trust, physical body features or body changes due to development, individual’s personality and sexuality information are important factors identified as vulnerability factors of CSA. Understanding these factors will help in creating strategies to mitigate CSA menace within the society and help in managing CSA cases.
Perpetrator’s Characteristics as an Element of CSA
This theme discussion points at the perpetrator’s characteristics as a risk factor by taking the blame off the child victim based on the view that child victims are mostly naïve, trying to form their identity and getting to know who they really are. The health care professionals associated the occurrence of CSA to perpetrators’ past experiences and socioeconomic factors which include unemployment, peer group pressure, and perpetrators’ need for cheap workforce. These factors were described to often affect perpetrators psychologically to an extent of pushing them to abuse children sexually. The participants described perpetrators of CSA as an older person or a younger child, but mostly known faces to the victims, and can be of either sex. They perceived that some perpetrators were reported to have experienced sexual abuse in the past but did not get rehabilitated medically and psychologically, and, most importantly, did not get justice for being abused. Participant D1-fc emphasized low acceptance of psychological rehabilitation services in managing CSA victims as a problem within the society. This often makes such victims grow up to have a perception that such bad experience is normal within the society and makes them continue to perpetrate CSA on others within the society: in our society, . . . well, I will just say most of the time psychologically, most perpetrators have been abused at a time . . . because they have been abused so in expense it’s like a fore-running, so these are people that have been abused while they were growing and there was no psycho-social support of any kind because in the environment, people are still trying to accept the benefit of psychological effort of counselors, they feel “we are excellent, we can deal with it,” so now not even addressing those issues repressing them, they come out as to express themselves in this kind of abusing a vulnerable children. (D1-fc)
Here, Participant D1-fc described the psychological implication of human experiences and how learning takes place within the society. The participant reported how bad activities grow subconsciously in previous sexual abuse victims’ mind when necessary medical and psychological interventions are not available. Thus, the effect of past sexual abuse experienced by perpetrators coupled with economic and societal factors influences the risk of CSA. As explained by Participant D9-fd, the economic status of perpetrators could make them abuse children sexually as some perpetrators see young children as a source of sexual service that does not require financial commitments: personally, I don’t see it that way. I just see that man does not . . . I see it has the man feels that if I use this girl I won’t pay her unlike any other adult that if I have to use I will give something. So, he could see it has opportunity that this one will not cost me anything. That is the way I see it . . .
In addition, D3-md identified that a high rate of unemployment or idleness within the society often encourages perpetrators to take advantage of young children that were put under their care while their parents were not around: apart from their appearances, most of them . . . when you have overcrowded . . . all this joblessness among the people they are living with, they are . . . that is another factor that can make them to be . . . I mean, unemployed youth for example . . .
In relation to economic factors, social influencing factors like peer group influences, social networking among friends, and their social lifestyles were suggested to have a serious impact on a perpetrator’s predisposition to sexually abuse children. These factors encourage learning of sexual acts among peers and rapidly incentivizing future sexual abuse perpetrations. For instance, Participant D1-fc noted, Now obviously in the media, the way sex has been over-amped, the label that has been placed on sex and sexual immorality has been over-amped which can also have effect on perpetrators, things they watch in groups up to the music they are being played . . .
The peculiarities of perpetrators’ identity as a risk factor for CSA suggest that they are individuals that were previously abused sexually but have difficulties in parting ways with the abuse trauma due to either lack of rehabilitation or the perception of the abuse as a normal occurrence, making them inclined to continuously sexually abuse other children.
Social and Economic Elements of CSA
Social and economic factors may play a range of vital roles in CSA vulnerability. As discussed in previous themes, past experiences of perpetrators relating to their social and economic situations are factors that could push a perpetrator to sexually abuse a child; however, the current theme discusses how both social and economic factors within the family and environment of victims increase the chance of exposure of a child to sexual abuse. It discusses existing intrafamily and interpersonal relationships, the financial status of victims, parents’ level of education, and religious and cultural factors that may predispose a child to sexual abuse. The health care professionals interviewed pointed out some intrafamily lapses like dysfunctional family, intrafamily conflict especially between parents, and neglect due to intrafamilial conflict or busy parents’ schedules. Participants are also aware of poor communication among family members which was related to existing conflicts within the family settings. For instance, Participant D7-fc identified internal problems within the family unit as a principal predisposing factor: The predisposing factors will start from the family unit, dysfunctional family, family whereby the parents are not settled, they are not together . . . It could be an unstable father who might have psychological issues, maybe the mother, the wife is starving the man of affection and then before you know it the man may not be psychologically stable or emotionally stable and will begin to do it with the child or even the housemaid in the house . . .
Participant D7-fc understands the impact of family members in a child’s life, and, based on the participant’s experience on the job, she was able to link internal family problems to CSA predisposing factors. Similarly, Participant D8-md also emphasized problems within the family as a risk factor that could expose a child to sexual abuse.
we’ve seen that there is a problem with the family structure, and we have some numbers where there is a separation between the parents, so the child is actually living with a guardian or some relatives. Of course, we know that the level of care may not be the same as if you have a family . . .
In their accounts, parents’ separation or differences could make a child seek shelter from extended family members who may not care for the child the way his or her biological parents would do, thereby exposing such a child to sexually abusive relationships. This form of family conflict not only is limited to conflicts between both parents but also include parent–child conflicts, particularly in adolescents as expressed by Participant D7-fc, who described irrational developmental changes during adolescence as a source of exposure to sexual violence which is often overlooked by parents and guardians: when they are approaching that adolescent age and then the hormones are being produced, the opposite sex . . . you know . . . are attracted to them and all that. If they are not getting a lot of parental love from home, chances are they fall vulnerable into voice of the opposite sex and want to experiment with them because they think that those ones are their best friends because a lot of parental child conflict during adolescent period . . .
Participant D12-fn also identified lack of care and communication between parents or guardians and their children as a factor because poor communication between parents and children can undermine the child’s ability to disclose sexual abuse, especially when the abuse is accompanied by threats from the perpetrator. Thus, if parents fail to create an enabling environment for easy communication with their young ones, it will be very difficult for a child to disclose a sexual abuse, which may encourage reoccurrence of such abuse: and most times communication is almost very important and most of the Nigeria parents don’t know how to communicate well with their children, so it’s a lot difficult to even find out. Just very few that communicate ethics . . . (D12-fn)
Participant D12-fn described communication as an important factor in disclosing and evicting CSA issues in the society. Lack of communication may be linked to parents’ low educational status, exposure, and/or ignorance (Chen et al., 2007). Although academic qualifications may not determine parents’ educational and exposure status as CSA still occurs in educated families, a high percentage of CSA victims were reported by participants to have a low educational and socioeconomic status. These victims were characterized by low family income, as the majority of the victims are from poor family backgrounds and mostly fell prey of sexual abuse while in the process of seeking financial assistance or shelter from relatives and neighbors: in terms of poverty, you have erm . . . one family that has large number of children, very low socio-economic status, so they have difficulty providing for the children. So that can be a means of opportunity for perpetrators to be able to offer the children things that we might not take as being very significant . . . (D8-md)
Participant D5-fd noted that low financial capability affects people’s living conditions, as environments with high CSA prevalence are places where family and neighbors share almost everything, including toilet, bathroom, kitchen, corridor, and sometimes bedrooms. Some of the child victims were also reported to be violated on the street while hawking with the aim of assisting their family financially.
Then again . . . yes, children that hawks, they are all prone to all these kinds of things because somebody calling them to say . . . “come and I want to buy something,” oh, come inside and they lure them . . . (D5-fd)
The health care professionals emphasized the cultural and religious practices in Nigeria as a factor that may predispose a child to sexual abuse. The patriarchy system, practice of respect, beliefs, and the conservative cultural nature were particularly noted as practices that may increase the risk of CSA. Women and children were often denied their human rights because men are categorized as the heads of the family and they make decisions within the family, just as adults or elderly have more opportunity to make decisions than younger ones. These decisions are often regarded as perfect, adequate, and mostly unquestionable, such that when an elderly approaches a young child for sexual intents, children find it difficult to turn down such offer. Participant D1-fc described this cultural nature of the society as follows: D1because in our society, in our culture we advise respect. exactly, if an elder call and say do this for me, we can’t easily say no, we should respect . . . so I mean, elders or male perpetrators use, take the advantage of that to perpetrate . . .
In addition, the secrecy, denial, or nondisclosure of CSA due to social stigmatization and particularly due to fear of disclosure leading to family feud may be a factor that predisposes a child to sexual abuse within the family as described by Participant D10-fc: . . . one of the Nurses just came to us and said this thing (sexual abuse) we are talking about happened to a woman recently and she linked us with the woman, and the woman just said I don’t want problem, I don’t want problem . . . and the person that abused the child is the uncle, the younger brother to her husband, I don’t want anything that will send me out of my husband’s house. So, you see, do you think that man will not continue doing it and he will even do it to another person . . .
It is obvious that reasons which make it difficult to get firsthand information about CSA vulnerability from CSA victims and their family such as the inability to disclose abuses due to societal stigmatization and concerns about family feud may also contribute to continuous abuse of a victim.
Programmatic Policies as an Element of CSA
This thematic nucleus supports mediating elements between human life and diverse social institutions created with the aim of promoting sanity within the society. Participants identified that inadequate or no implementation of public policies related to health, education, economic, and legal services may promote occurrences of CSA in the society. The nonavailability of systems that punish sexual abuse offenders often create an avenue that encourages other perpetrators to indulge in sexual abuse practices. For instance, Participant D2-md noted that the current poor state of the judicial system in Nigeria has a great impact in encouraging CSA: . . . and again i will say poor judicial or poor ehm ehm . . . i don’t know how to put it now, the system, the government system, the law in the land, we rarely have cases of conviction so people, perpetrators get away if they are rich, they pay their bail, it is only if a daughter of a rich man is being abused is when they get justice . . .
Moreover, Participant D2-md related the poor judicial system to a high rate of corruption in which rich perpetrators often buy their way out of justice and go unpunished for sexual offenses. Interestingly, victims from rich family background mostly get justice as they have the financial capability to adequately pursue legal fights against sexual abuse offenders. The participants emphasized that poor victims mostly do not get justice, which is related to the previously discussed thematic nucleus of social and economic elements as a predisposing factor to CSA, as CSA was reported to be more prevalent among those with low socioeconomic status. In addition to inadequacies and biases in the judicial system, legal procedures are time-consuming and often discourage people from seeking legal assistance after experiencing CSA. For example, Participant D11-fc noted, Yes, its just a long process, it takes courage, the faith of our clients will drop down at the middle of it and sometimes, you yourself, you get tired going to court today, going to court tomorrow so those ones need encouragement . . .
Participant D13-fn related lack of policy implementation to CSA prevalence, as there are some good policies against CSA, which are mostly not implemented by the government: There are health and education policies, excellent, beautiful policies. Yes, but the implementation is the problem and implementation need funding . . . for the private sectors and for the public sectors because the public sector, the way Nigerian public sector is meant to function, there will be no place for abuse on its own . . .
The formulation and implementation of sexual violence policies that guide public services, and the commitment of the government to sustaining these policies can promote healthy living and reduce CSA within the society. Likewise, the creation of intersectoral and multisectoral activities that articulate public sexual violence policies with private endeavors may also mitigate CSA within the society.
Discussion
This article provides information on ways of assessing CSA vulnerability factors, particularly in sub-Saharan African countries such as Nigeria, where access to child victims and their family is difficult due to societal stigmatization. It qualitatively assessed the experience-based perception of health care professionals about vulnerability factors that could predispose a child to CSA. The experience of health care professionals working directly with sexually abused children may help recognize the causes of CSA within the society and proffer professional ways of preventing the menace. Health care professionals that participated in this study identified several factors that could substantially predispose a child to CSA and these factors were categorized and discussed under four themes of victims’ individual vulnerability, sexual abuse perpetrators’ personal characteristics, social and economic components, and programmatic determinants that deal with government policies toward CSA. Without understanding these factors contextually, efforts directed at proffering ways to prevent CSA may remain ineffective in African countries. We argue that, to understand this menace, we need to start acknowledging health professional experiences and efforts in treating and rehabilitating CSA victims, particularly in sub-Saharan countries like Nigeria, where access to firsthand information from victims is difficult due to stigmatization and culture. The analysis of interviews with health care professionals who worked with CSA victims showed clearly that CSA is associated with victims’ and perpetrators’ characteristics, in addition to social and economic factors within the society.
Previous studies and theoretical writings have recognized one of the vulnerability factors of CSA to be victims’ characteristics (Boss, 2007; Meinck et al., 2015; Putnam, 2003; Silva Júnior, 2006; Snyder, 2000; Wolak et al., 2010). These factors include age, innocence, trust, lack of information, personality, and early development. The importance of understanding these vulnerability actors among child victims and proffering active solutions by educating children about CSA has been noted to strengthen victims’ capabilities and abilities to identify sexual abusive situation (Ogunjimi et al., 2017). By directly talking to health care professionals who had contact with these victims, we were able to highlight how children fall victim to CSA without having any knowledge of it because of individual nature of immaturity and inexperience. With this information, it is important that efforts and resources must be directed toward educating children, parents, community leaders, heads of religious group, and youth organizations within the society about children’s intrinsic characteristics that can predispose them to CSA.
Our study findings suggested that perpetrators’ characteristics can have a significant influence on the occurrence of CSA in young children. Consistent with other studies, our study suggests that previous sexual abuse experiences of perpetrators may predispose them to commit this act on other children (Finkelhor, 2009; Jewkes et al., 2006; Lewis et al., 2016; Vizard, 2013). Sexual violence perpetrators’ behaviors were found to be an implication of psychological instability caused by lack of rehabilitation programs that may heal victims of their past CSA experiences. Interestingly, Nigeria does not have a one-stop rehabilitation center or program where sexual abuse victims can receive adequate rehabilitation. This includes provision of initial shelter away from the abuse perpetrator, food and clothing, family counseling, and legal advice, in addition to medical and psychological services. The availability of such centers in a country such as Nigeria may improve victims’ access to necessary help and disclosure of sexual abuse. Socioeconomic instability of perpetrators was also identified as impactful and could predispose a perpetrator to commit CSA (Lalor, 2004). Idleness and low financial status of a perpetrator due to a high unemployment rate in Nigeria was suggested as a reason for child sexual exploration by perpetrators in their quest for access to cheap sexual experiences. To further buttress this, a nexus between unemployment and several societal vices has been identified in Nigeria, as an increase in criminality has been directly linked to youth joblessness (Adebayo, 2013). It is understandable that human stability (psychological, medical, financial, societal, etc.) is important for an effective functioning of individuals within a society (Garbarino & Ganzel, 2000) and a lack of this may be detrimental to individuals and can influence relationships with children around them.
Social environmental factors have long been recognized by scholars to contribute to CSA menace in the society (Kellogg & Menard, 2003; Krug et al., 2002; Madu & Peltzer, 2001; Nlewem & Amodu, 2017). The family structure, relationship between spouses and their children, presence of conflict, and neglect have historically been identified to determine sexual violence against children (Boden et al., 2007; Peter, 2009; Petersen et al., 2005). As we have noted, the presence of conflict within family settings discourages communication and care between partners (father and mother), and between parents and their children. The implication is that children suffer most in this situation due to lack of care and communication between children and their parents. For instance, scenarios where some women deny their men of sexual relationship due to disagreements have led to sexual frustration in such men, which prompted them to make sexual advances toward their children or other children to satisfy their sexual urge, and the lack of communication between such children and their parents further prevents reporting of these incidences, leading to a continuous abuse by such men.
The socioeconomic status of children has been well established as a predisposing factor when considering CSA within the social setting (Boden et al., 2007; Peter, 2009). This study buttressed the well-established evidence that low socioeconomic status of children’s family may be an indicator of CSA occurrence (Krug et al., 2002), but CSA occurrences in children from medium- to high-socioeconomic-status homes are also common and may be linked to neglect experienced by children from their parents/guardians. The neglect experienced depends on the socioeconomic status of a child’s family. In Nigeria, children from low-socioeconomic-status homes may be neglected by parents/guardians due to financial constraints, which could make some children explore alternative sources of financial support, thereby exposing them to CSA. Conversely, children from high-socioeconomic-status homes are often overpampered and uncontrolled as parents mostly jettison good parenting for financial commitments. This scenario may expose such children to CSA as they often live in situations where they make crucial decisions without their parents’ consent. In terms of CSA victims’ access to care, participants in this study mostly had contact with victims from low-socioeconomic-status homes, as this facility is public owned and the cost of seeing a health care professional is generally low or completely free. Although rich families mostly get justice against CSA perpetrators in Nigeria, most events following sexual abuse of a child from a rich home are often done in secrecy. These events include seeking treatment in privately owned hospitals and situations where such a child is flown out of Nigeria away from the vicinity of the abuse.
This study also highlighted some cultural and religious practices including patriarchy practices as CSA predisposing factors. These practices are also related to how much value is placed on children and women’s rights in Nigeria. In Africa, particularly Nigeria, children are generally classed to have fewer rights than adults, with expectations to believe, obey, and respect commands, wishes, and interests of parents and other elderly ones even if they are not a family member (Fontes & Plummer, 2010). Likewise, women generally have fewer rights than men which make mothers struggle between family preservation, family loyalty, and anxiety of being alienated, which mostly prevent mothers from taking actions in CSA cases (Lovett, 2004). This cultural belief has emboldened many perpetrators to repeatedly abuse children sexually and getting away without justice. In addition, the belief of solving most family problems, particularly socioeconomic issues, religiously and ascribing an infallible status to religious leaders has also contributed to CSA menace in Nigeria. Some religious leaders have sexually abused children in the name of performing spiritual deliverance, whereas some have proposed doctrines that led religious group members to crave for sexual relationships with children.
An association between the weak judicial system and the occurrence of CSA was also identified in this study. Most of the participants perceived that loopholes in government services and systems that are meant to prepare citizens for right responses to CSA situations are not available, as such a lot of people do not know the right steps to take after the occurrence of sexual abuse (Liebling et al., 2012; Tillman et al., 2010). Weak legislation through delays and bureaucracies in the criminal justice process, intimidation of child victims, and practices of the traditional justice system often lead to nonsupportive and nonencouraging behavior in reporting CSA cases in Nigeria, an idea which has been supported by other studies (Hanna et al., 2010; Krug et al., 2002; Lalor, 2004; Liebling et al., 2012). In addition, traditional justice system practices by community elders often interfere with promoting effective child protection laws within the community because our cultural practices had already limited the right of a child. There may be a need for social discussion in Nigeria on how to align differences in the traditional, cultural, and orthodox justice system in relation to CSA, with a view to protect children from this menace.
Conclusion
In this study, we acknowledged CSA as a social and environmental menace that could negatively impact the well-being of a child and it is important that we identify and understand vulnerability factors that can predispose a child to sexual abuse, particularly in Nigeria where access to firsthand information from CSA victims and their families is rare. It is crucial to thus move beyond seeking information from CSA victims and access alternative sources of information about factors that can predispose children to sexual abuse in Nigeria.
By presenting the qualitative analysis of the perception of health care practitioners who had contact with CSA victims in Nigeria, we have highlighted factors that may make a child vulnerable to sexual abuse. Our qualitative approach provided detailed information about these factors through the experiences, opinions, and perspectives of health care professionals in this study. These factors identified include characteristics of a child victim and a perpetrator, victim’s socioeconomic status, sociocultural ideals, government policies, and the justice system in Nigeria. These new insights should produce significant response to CSA by parents through strengthening child–parent relationships, by the society through engagement in actions that support prevention of violence against children and eradication of cultural biases against children, and by the government through creating new and updating existing policies on CSA and implementing such policies adequately. Generalizability of this study is limited by the small (N = 14) sample size. A study involving a larger sample size of health care professionals in other regions of Nigeria, in addition to comparing responses from a quantitative approach with this qualitative method, may give better insights about vulnerability factors associated with CSA. It will also be interesting to study religious perspectives to CSA and its vulnerability factors.
Footnotes
Author’s Note
Wanderlei Abadio de Oliveira is also affiliated to Pontifical Catholic University of Campinas, Brazil.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Coordenação de Aperfeicoamento de Pessoal de Nível Superior (CAPES) under the Ministry of Education of the Brazilian government.