
Abstract
Transgender and nonbinary (TNB) individuals experience high rates of myriad types of victimization, including in health care settings. Many TNB people avoid medical visits for fear of mistreatment and, when they do visit a provider, report negative experiences (e.g., denial of services, misgendering, verbal abuse). These negative experiences are heightened for TNB individuals who have an intersecting marginalized identity (e.g., low socioeconomic status, disability). Using data from the 2015 United States Transgender Survey, the largest survey of TNB individuals in the United States to date, the present study examines differential experiences of victimization in health care settings by TNB identity and other demographics (i.e., race, age, class, educational level, disability). A series of multivariate logistic regressions were run to determine adjusted odds ratios (AORs) for TNB individuals recently (i.e., in the past year) experiencing four forms of victimization: (a) doctor/health care provider used harsh or abusive language; (b) doctor/health care provider was physically rough or abusive; (c) patient was verbally harassed in health care setting; and (d) patient experienced unwanted sexual contact in health care setting. Frequency of victimization varied by gender identity and type of victimization; the most prevalent form was verbal harassment by a doctor/provider (5.84%) and the least prevalent was unwanted sexual contact in a health care setting (1.20%). Although findings varied by form of violence, generally, regression models demonstrated elevated odds of experiencing some form of health care victimization for those who were transgender compared with genderqueer, biracial/multiracial compared with White, low income compared with higher income, and disabled compared to non-disabled. In addition, odds ratios for victimization increased with age and, for some forms, increased with low educational attainment. We discuss the need for increased mandatory trainings for providers to reduce discriminatory and violent behavior toward TNB patients, as well as intersectional research to better ascertain the extent and nuance of victimization within TNB health care.
Transgender and nonbinary (TNB) individuals experience high rates of discrimination, violence, and victimization across a variety of contexts (Grant et al., 2011; James et al., 2016), including with law enforcement personnel (Carpenter & Marshall, 2017; Operario & Nemoto, 2017), in social service settings (Calton et al., 2016; Kattari, Walls, Whitfield, & Langenderfer Magruder, 2017), in housing and employment (Kattari, Whitfield, Walls, Langenderfer-Magruder, & Ramos, 2016), and in educational spaces (Stolzenberg & Hughes, 2017). While studies have examined discriminatory experiences in medical and health settings, few have delved into specific types of victimization, harassment, and violence experienced by TNB people when trying to access health care.
TNB Identities and Definitions
Transgender and trans are both terms used to describe a range of individuals who do not feel that the sex and/or gender assignments made for them at birth were correct (Devor & Thomas, 2019). The term nonbinary (NB) refers to one’s identity rather than to one’s physical characteristics at birth. Those who identify as NB might identify as a single fixed gender (other than male or female), gender fluid, two-spirit (an indigenous identity), or agender (Richards et al., 2017). Some NB people identify as belonging to the trans community while others do not. It is important to understand a person’s gender identity on an individual level is unique to the individual; it is not linear or “one size fits all.” It should also be noted that medical intervention (or the desire for it) is not required for someone to be trans or NB.
TNB Victimization Experiences in Health care
According to data from the 2015 United States Transgender Survey (USTS; N = 27,715), most TNB persons have seen a health care provider in the past year, though nearly one-third reported that none of their providers knew they were transgender (James et al., 2016). Additional national data suggest that when a provider does know a patient is transgender, the patient’s risk of discrimination increases (Grant et al., 2010). Indeed, one-third of USTS respondents reported having at least one negative experience with a health care provider in the last year related to being transgender, such as verbal harassment, refusal of treatment, or having to educate the health care provider about transgender people to receive appropriate care (James et al., 2016). At the policy level, USTS data show that 14% of transgender individuals are uninsured (compared to 11% of the general adult population) and that one-quarter report negative insurance experiences related to their gender identity, such as coverage denials (James et al., 2016). Given these discrimination and victimization experiences, it is perhaps unsurprising that 23% of USTS respondents said they had avoided seeing a doctor when needed due to the fear of transgender-related mistreatment. A Colorado-based study found that, in addition to cost and inability to locate a provider, fear of discrimination was one reason cited for TNB persons’ avoidance of care (One Colorado Education Fund, 2014).
Prior research indicates that these health care discrimination experiences hold true for multiple genders within the TNB spectrum. Data from the National Transgender Discrimination Survey (NTDS) show that one-fifth of trans-identified individuals report being refused treatment, with similar prevalence among male-to-female (22%) and female-to-male (19%) persons (Grant et al., 2010), and the prevalence of mistreatment was even higher. In Shires and Jaffee’s (2015) study of female-to-male transgender participants in the NTDS (N = 1,711), over 40% reported experiencing health care discrimination (i.e., verbal harassment, denial of equal treatment, physical assault in a doctor’s office or hospital). Similarly, Hughto et al. (2018) found that among 150 transmasculine individuals, 68% had experienced some form of mistreatment in health care settings, while 43% had avoided health care in the past 12 months. Another study found that both transgender men and transgender women were approximately four times more likely to avoid medical care if they had to teach their provider about transgender people (Jaffee et al., 2016).
Types of Health care Mistreatment
Based on the responses of 152 transgender survey participants, 71% of whom experienced at least one form of mistreatment in health care, Kosenko et al. (2013) identified six distinct forms of health care mistreatment: (a) gender insensitivity (e.g., using incorrect pronouns, commenting on a patient’s degree of “passing”); (b) displays of discomfort (i.e., patient perceives “awkward” behaviors, such as fidgeting, staring, or avoiding eye contact, as stigmatizing and discriminatory); (c) denial of services; (d) receipt of substandard care (e.g., rough exams); (e) verbal abuse (e.g., being mocked, belittled, or abused); and (f) forced care (e.g., being forced to undergo procedures). Baldwin et al.’s (2018) study of negative patient–provider experiences similarly identified misgendering, transphobia, and provider lack of information/experience as major negative elements of patient–provider interactions. Notably, the mistreatment of TNB people in health care settings has been associated with increased risk of depression, suicide, and HIV (Poteat et al., 2013).
At a systemic level, Hatzenbuehler et al. (2013) have theorized stigma as a fundamental cause of population-level health disparities when it is conceptualized as “labeling, stereotyping, separation, status loss, and discrimination in a context in which power is exercised” (p. 813). The authors argue that despite changes to the problem (e.g., risk factors, interventions), social factors, like stigma, will continue to perpetuate health inequities, such as by inducing stress and creating a lack of availability of resources (Hatzenbuehler et al., 2013). Derived from interviews with transgender individuals (n = 55) and medical providers (n = 12), Poteat et al. (2013) developed a grounded theory to describe interpersonal stigma in the provider–transgender patient dynamic. Systemic stigma against TNB individuals results in their care being excluded from medical training, which leads to providers who are ill prepared and left with uncertainty or ambivalence in how to best meet the needs of TNB persons. Concurrently, TNB individuals anticipate providers will not be able to meet their needs. Power in the relationship is subsequently upset by this uncertainty, as providers retain interpersonal stigma against their TNB patients as a way to combat their uncertainty and maintain authority in the relationship (Poteat et al., 2013). Notably, Herek (2016) argues terms like “homophobia” and “transphobia” are too broad when discussing sexual and gender minority health, as they lose the nuance of the experience (e.g., discrimination, prejudice, violence, internalized attitudes). Instead, Herek (2016) posits that stigma-based language (e.g., “gender minority stigma”) is more appropriate as it reinforces the notion that health disparities are in large part due to societal definitions or perceptions of a particular characteristic, as opposed to the characteristic itself.
Intersecting Identities and Health Care Mistreatment
That we find TNB patients to be at greater risk of health care victimization when they have an intersecting marginalized identity is aligned with minority stress theory, which has been previously applied to victimization research with this population (e.g., Atteberry-Ash, Walls, Kattari, Peitzmeier, Kattari, & Langenderfer-Magruder, 2019; Whitfield, Kattari, Langenderfer-Magruder, Walls, & Ramos, 2019; Seelman et al., 2017). Minority stress theory has captured the health effects of oppression on marginalized individuals and groups, including lesbian, gay, bisexual, transgender, and queer populations (Balsam et al., 2011; Kelleher, 2009). More recently, it has been adapted to be more specific for the TNB population, to demonstrate the individual and interpersonal impacts of transgender-related discrimination and internalized stigma (Gamarel et al., 2014; Hendricks & Testa, 2012). In his original theorization of minority stress among lesbian, gay, and bisexual persons, Meyer (1995) outlined three primary stressors: (a) observable environmental or external stressors (e.g., objective experiences of discrimination); (b) anticipation of external stressors (e.g., harm, rejection); and (c) internalization of negativity (e.g., internalized homophobia). Hendricks and Testa (2012) note specific parallels to Meyer’s (1995) theory for TNB persons, the most obvious being the documented elevated prevalence of various forms of violence against TNB individuals (i.e., observable violence) and its association with poor health and mental health outcomes. Although less research has been conducted directly linking these negative, external experiences to internal processes, as Hendricks and Testa (2012) note, previous research with TNB samples indicates intentional concealment of identity (Beemyn & Rankin, 2011). Feeling or perceiving stigma, as Herek (2016) notes, can lead TNB persons to avoid disclosure of gender identity–related concerns to their health care providers. This speaks to Hatzenbuehler et al.’s (2013) conceptualization that stigma works, in part, to both increase stress and reduce access to services, resulting in continued health disparities. These theories are useful in helping us understand the important effects of oppressive stressors across marginalized identities.
People of color are more likely to experience discrimination in health care settings than their White counterparts (LaVeist et al., 2003). Even after accounting for individual and system-level factors, race is a strong determinant of perceived health care discrimination, especially for those who identify as African American and Native American (Abramson et al., 2015). Prior research has found that transgender people of color are more likely to experience discrimination in health care settings than their White transgender counterparts (Kattari, Walls, Whitfield, & Langenderfer-Magruder, 2015). Moreover, transgender men and transgender women who are multiracial, and transgender men who are Native American, are more likely to delay medical care due to discrimination (Jaffee et al., 2016).
Like people of color, those of lower socioeconomic status also experience negative interactions in health care settings. These individuals face challenges in navigating health care systems for a variety of reasons, including lack of knowledge, lower likelihood of having health insurance, fewer financial resources to devote to health care, and a variety of additional health concerns that are often compounded by class (Schroeder, 2016). They may also notice higher rates of discrimination from their health care providers (Tajeu et al., 2015). Studies have found lower socioeconomic status to be associated with perceived health care discrimination (Bratter & Gorman, 2011), including among lesbian, gay, bisexual, transgender, and queer (LGBTQ)-identified samples (Gamarel et al., 2012). Specific to transgender samples, lower socioeconomic status is correlated with health care discrimination among transgender men (Shires & Jaffee, 2015), and for transgender women, increased income is a protective factor against health care discrimination (Jaffee et al., 2016).
Negative Health Care Experiences and Disability Status
Disabled people are one of the largest marginalized populations in the United States. The United States Census Bureau (Brault, 2012) reported that in the 2010 census, 21.3% of people aged 15 years and older had a disability or impairment. People with disabilities are significantly more likely to experience violence and victimization in many settings (Admire & Ramirez, 2017; Chan et al., 2018; Lund et al., 2017) and are also at higher risk of experiencing discrimination in health care settings (Kelly et al., 2015; Rogers et al., 2015). Although little research exists on the intersection of disability and gender identity, particularly in health care settings, a recent study found that disabled TNB individuals experienced higher rates of discrimination in mental health settings. In this study, while people with all types of disability and impairment experienced elevated rates of discrimination over non-disabled TNB people, those with multiple disabilities and impairments were over four times more likely to have experienced discrimination than their non-disabled peers (Kattari, Walls, & Speer, 2017).
Negative Health Care Experiences and Education Level
When examining different marginalized communities’ experiences in health care settings, one area that is difficult to assess is the intersection of negative health care experiences with providers’ and a patient’s level of education. There is not a lot of research on the intersection of education level and health care experiences. In a 2015 study, having a graduate degree was connected to increased reports of discrimination experiences in health care settings (Shires & Jaffee, 2015). This study focused exclusively on the experiences of transgender men and concluded that power and stigma play a role in health care encounters and that this finding could help to elucidate the relationship between perceived discrimination and higher levels of education. Jaffee et al. (2016) also found that education level plays a role in the choice to delay health care due to fear of discrimination.
Negative Health Care Experiences and Age
Ageism and negative health care experiences may go hand in hand due to the biases and assumptions of providers, and both age and disability can be predictors of discrimination in health care settings (Rogers et al., 2015). Adults aged 40 years and older are more likely to experience sexual victimization at the hands of physicians than their younger counterparts (DuBois et al., 2017). Experiences of health care discrimination, harassment, and victimization occur across all age groups of TNB individuals, and participants in older age groups have reported fewer experiences of discrimination and harassment but higher rates of victimization (Kattari & Hasche, 2016).
Research Questions
Quality health care is lacking for individuals who possess multiple marginalized identities. This study assesses the hypothesis that TNB individuals with more marginalized identities are more likely to experience victimization in health care settings. Because when examining negative experiences of marginalized people in health care, it is impossible to ask individuals to separate their experiences from their various identities, this study attempts to answer the following questions:
Method
Study Design
The 2015 USTS is the largest survey of TNB individuals in the United States to date. Respondents were invited to provide information on life experiences across a breadth of areas, including health, work, family, and their communities. To recruit respondents, the USTS utilized convenience sampling online and through several hundred organizational partners. The survey was offered online in both English and Spanish, and only those who self-identified as transgender, NB, and aged 18 years or older were invited to complete the survey. The total sample size was 27,715 individuals across all 50 states, Washington D.C., and several U.S. territories (James et al., 2016). The current study utilized the USTS for secondary data analysis and was therefore exempt from Institutional Review Board (IRB) human subject research approval.
Data Analysis
Descriptive results were generated for all variables. Bivariate chi-square tests were conducted to assess the relationship between gender identity and each dependent variable. Subsequently, multivariate logistic regression analysis was conducted to assess the odds of TNB people experiencing four forms of victimization in a health care setting across several demographic variables.
In the USTS, the four binary dependent variables, which were ascertained of only those respondents who previously indicated that they had seen a doctor or health care provider in the previous year, included (a) “provider used harsh or abusive language when treating me”; (b) “provider was physically rough or abusive when treating me”; (c) “I was verbally harassed in a health care setting (such as a hospital, office, clinic)”; and (d) “I experienced unwanted sexual contact (such as fondling, sexual assault or rape) in a health care setting” (James et al., 2016). Respondents answered if each experience did or did not happen to them over the course of the previous year (0 = no; 1 = yes).
Demographic independent variables include gender identity, income, race, age, disability, and educational attainment. Age was a continuous variable. Disability was a binary variable that captured if a person self-identified as disabled. Educational attainment, income, and race were categorical variables. For gender, both a USTS-generated five-category variable, used in bivariate analysis, and binary gender variable, used in multivariate analysis, were employed. The five-category variable was constructed by USTS investigators by cross-tabulating questions on biological sex and gender identity. This created five gender categories: (a) trans women; (b) trans men; (c) assigned female at birth genderqueer/nonbinary (AFAB GQ/NB); (d) assigned male at birth genderqueer/nonbinary (AMAB GQ/NB); and (e) crossdresser. The final category of crossdresser, which respondents could select as their gender identity, was dropped from the current analysis as we were concerned with individuals who identified as transgender or NB. For multivariate logistic analysis, the AFAB GQ/NB and AMAB GQ/NB categories were collapsed together to attain sufficient sample size across models. Furthermore, trans women and trans men were collapsed together to compare TNB experiences of victimization.
Specification tests were conducted for each regression. First, variables were tested for sufficient data. The Native American (n = 141) and Middle Eastern (n = 77) race categories were dropped due to low sample size. Second, the age variable was assessed for polynomial properties in each regression by including a quadratic age term. The quadratic term was included in the final model if a post hoc F-test showed its inclusion strengthened the model. Finally, as suggested by USTS investigators due to their oversampling of White individuals and those 18 years old, standard survey weights for age and race were utilized in each model (James et al., 2016). The final analytical sample for each regression differed slightly due to non-response for some of the dependent variable research questions.
Descriptive results (Table 1) are shown for all respondents who responded to any of the survey questions on the four forms of victimization. They show that approximately two-thirds of the weighted sample identified as transgender and one-third identified as genderqueer. Just under half of the individuals sampled (48.80%) had an associate degree or higher, while 36.76% had an annual income of less than US$25,000. The mean age was 31.3 years and 63.5% identified their race as White. A total of 28.45% of the sample identified as disabled. These weighted subsample descriptive results are mostly comparable to those found in the full weighted USTS sample. The only exceptions are income, where 55% of the full USTS sample earn less than US$25,000 annually, and disability, where 39% of the full USTS sample identify as disabled (James et al., 2016).
Descriptive Results.
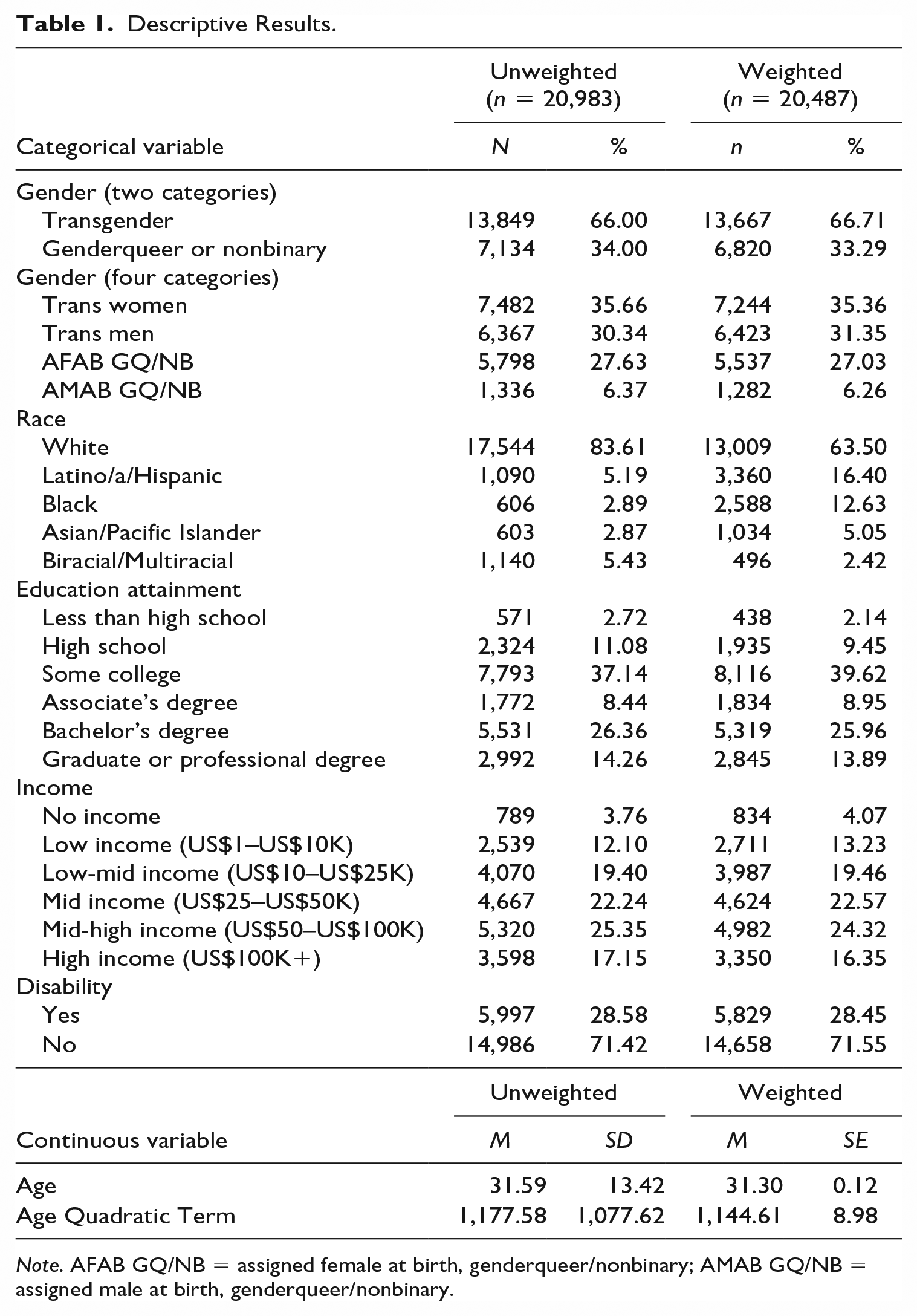
Note. AFAB GQ/NB = assigned female at birth, genderqueer/nonbinary; AMAB GQ/NB = assigned male at birth, genderqueer/nonbinary.
Results
Bivariate results (Table 2) show that there is a statistically significant relationship between all forms of victimization and gender identity, save for a doctor or health care provider using harsh or abusive language. The most prevalent form of victimization was being verbally harassed in a health care setting (5.84%), followed by a doctor or health care provider using harsh or abusive language (5.05%). The least prevalent form of victimization was experiencing unwanted sexual contact in a health care setting (1.20%).
Victimization in Health care Settings: Chi-Squared Results for Gender Identity.
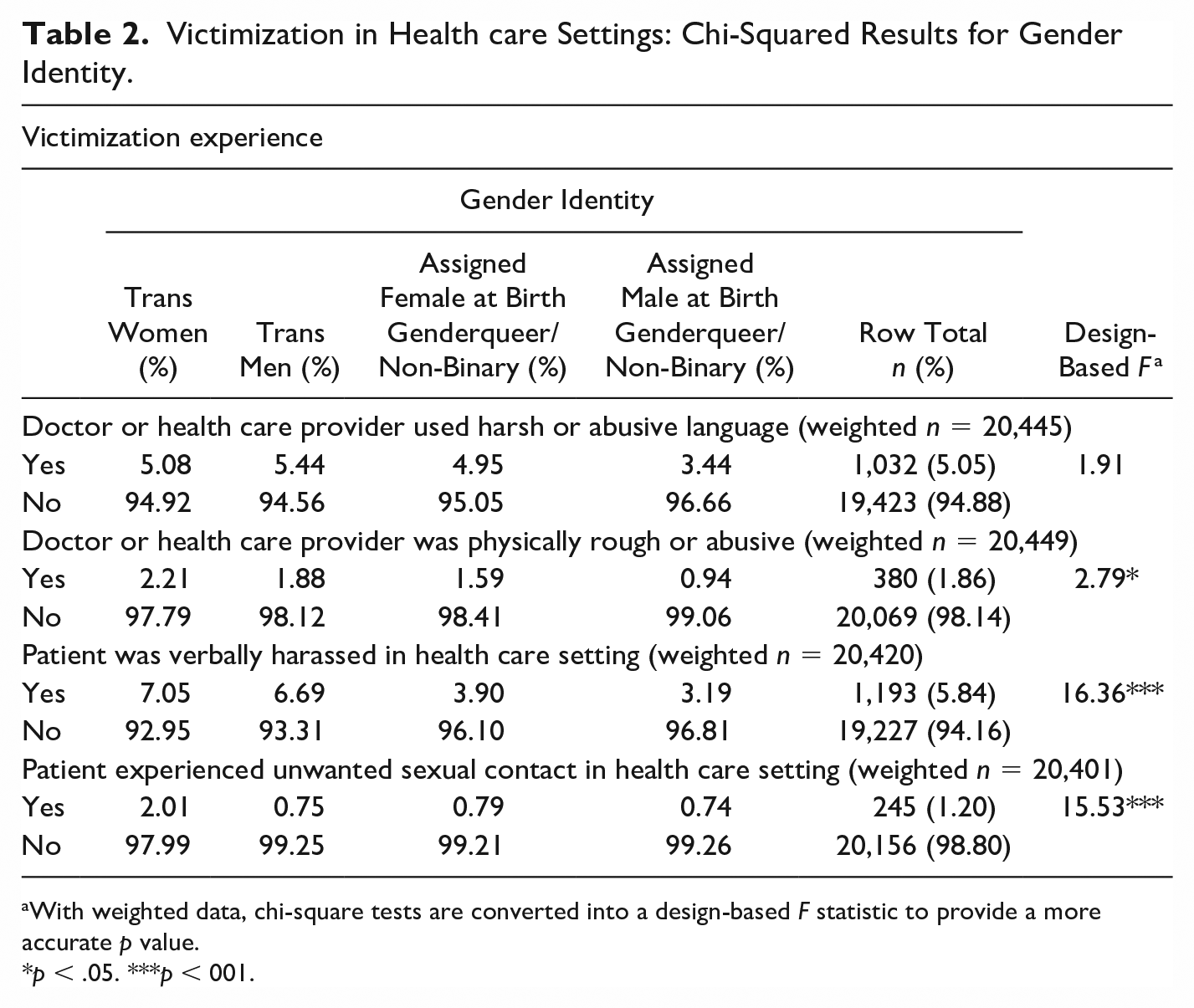
With weighted data, chi-square tests are converted into a design-based F statistic to provide a more accurate p value.
p < .05. ***p < 001.
Multivariate logistic regression was conducted for all four forms of victimization using the weighted sample (Table 3). All four models show overall statistical significance (p < .001) and Hosmer–Lemeshow Goodness of Fit tests were all insignificant (p > .05), which indicated good model fit. However, with such a large sample size, predictor effect sizes are emphasized for meaningful interpretation of results. Results are presented for demographic variables as AOR, holding all other variables constant, and demonstrate mostly weak to weakly moderate effect sizes (Chen et al., 2010). Across three models, including providers who used harsh and abusive language (AOR = 1.41; confidence interval [CI]: [1.16, 1.70]; p < .001), patients being verbally harassed (AOR = 2.15; CI: [1.77, 2.60]; p < .001), and patients experiencing unwanted sexual contact (AOR = 2.20; CI: [1.48, 3.27]; p < .001), those who were transgender had statistically significant greater odds of experiencing victimization than those who were genderqueer/NB. Lower incomes showed weakly moderate effect sizes and were associated with increased odds of experiencing victimization. For example, those who were low income had 2.74 greater odds (CI: [1.28, 5.90]; p < .01) of experiencing physical abuse from a doctor or health care provider, and 1.97 greater odds (CI: [1.21, 3.19]; p < .01) of being verbally harassed in a health care setting, in comparison with those who were high income. Those who were disabled experienced roughly 2–2.5 greater odds, and those who were biracial/multiracial experienced roughly 1.5–2.5 greater odds, of experiencing all forms of victimization in comparison with those who were not disabled or were White, respectively. Increases in age demonstrated weak effect sizes and were associated with slightly greater odds of experiencing harsh or abusive language (AOR = 1.09; CI: [1.04, 1.14]; p < .01), physical abuse (AOR = 1.14; CI: [1.06, 1.22]; p < .001), and verbal harassment (AOR = 1.10; CI: [1.06, 1.14]; p < .001). Finally, various levels of educational attainment were significantly associated with greater odds of experiencing some forms of victimization. Those with less than a high school education had 2.91 (CI: [1.27, 6.67]; p < .05) greater odds of experiencing unwanted sexual contact and 1.78 (CI: [1.05, 3.04]; p < .05) greater odds of being verbally harassed, in comparison with those whose highest educational level was a bachelor’s degree.
Multivariate Logistic Regression of Victimization in Health care Settings.

Note. As is standard practice, the quadratic term is left out if it does not strengthen the model (as determined by a post hoc F test). AOR = adjusted odds ratio; OR = odds ratio; CI = confidence interval; SE = standard error; GED = general educational development.
p < .05. **p < .01. ***p < .001.
Discussion
Corroborating findings from previous research (e.g., Hughto et al., 2018), the present study found that TNB individuals experienced victimization in health care settings, particularly verbal victimization (e.g., verbal harassment, doctor used harsh or abusive language). Notably, reported frequencies of victimization were lower in this study than in prior research, though this is likely due to the time frame of the victimization, as the present study focused on recent (i.e., past year) experiences, whereas previous large sample studies focused on lifetime experiences and, more specifically, on health care discrimination broadly (e.g., Bradford et al., 2013; Hughto et al., 2016). This speaks to Herek’s (2016) argument for capturing nuance in negative health care experiences among sexual and gender minority populations. Importantly, our results suggest that not all TNB people are at equal risk for victimization in health care settings. Hughto et al.’s (2016) examination of transgender lifetime experiences of care refusal by a provider showed that identifying as older, trans feminine, Native American, multiracial, another racial/ethnic minority, or low income was significantly associated with being refused care. The present findings closely mirror those of Hughto et al. (2016) and demonstrate that these risks factors exist not only for refusal of care but also for victimization once under a provider’s care. In alignment with Hatzenbuehler et al.’s (2013) conceptualization of stigma as a primary cause of health inequities, the current study suggests that those holding multiple marginalized identities are at particular risk for lack of access to safe, affirming health care.
Our study showed an increased risk for victimization in health care settings with patients’ increasing age. Hughto et al. (2016) similarly found that increasing age was associated with lifetime experiences of refusal of health care among transgender patients, noting that this is likely due to older patients’ increased opportunities to have experienced refusal over time. However, the present study found the same pattern for recent health care victimization. Building on Hughto and colleagues’ (2016) suggestion, it is possible that, as a function of increasing age, patients require more frequent medical care and the greater risk of past year victimization is due to increased opportunity for such victimization to occur; however, intersecting ageism could certainly be at the root of this finding and requires further study.
Compared with White participants, some biracial and multiracial participants in the present sample had a higher risk of experiencing health care victimization, which is reflective of systemic racism. Marginalized racial and ethnic groups have previously been shown to experience high rates of victimization in various contexts within TNB-specific research (e.g., Bradford et al., 2013; Reisner et al., 2014; Xavier et al., 2005), including health care settings ( Kattari, Walls, Whitfield, & Langenderfer-Magruder, 2015; Hughto et al., 2016). The present findings, as well as those of Hughto et al. (2016), indicate that biracial/multiracial individuals are particularly vulnerable to victimization in health care settings. Jaffee et al. (2016) had these same findings regarding this group being likely to delay needed medical care. Kattari, Walls, Whitfield, & Langenderfer-Magruder (2015) found that biracial/multiracial participants reported significantly greater frequency of discrimination in multiple health care domains compared with White participants: by doctors/hospitals (32.8% vs. 18.5%), in emergency rooms (20.6% vs.10.1%), and when using ambulances/interacting with Emergency Medical Technicians (EMTs; 9.1% vs. 3.0%). While alarming, these findings are unsurprising given that trans people of color have experienced elevated discrimination in other social service contexts, including mental health services, drug treatment programs, domestic violence shelters, and rape crisis centers (Kattari, Walls, Whitfield, & Langenderfer Magruder, 2017).
Past literature indicates that low income is predictive of discrimination in health care settings (LaVeist et al., 2003; Stepanikova & Oates, 2017), including within transgender samples (Hughto et al., 2016). In the present sample, risk of experiencing verbal violence (i.e., provider used harsh or abusive language, patient was verbally harassed) was elevated for nearly all persons earning less than US$100,000 annually. However, only those with no or low income had elevated odds of physical forms of violence (i.e., provider was physically rough/abusive, patient experienced unwanted sexual contact). In their examination of refusal of care, Hughto and colleagues (2016) found that income, even more than insurance coverage, was predictive of care refusal experiences among transgender patients, suggesting that those with financial means could travel to receive appropriate services, thus reducing their risk of victimization.
We found that some survey participants with less than a bachelor’s degree had a significantly elevated risk for verbal harassment and unwanted sexual contact, while those with an associate’s degree had lower risk for experiencing harsh language and unwanted sexual contact. Beyond this, the authors could not find additional discernible patterns in the findings, and analyses confirmed no multicollinearity between education level and income. NB individuals experienced lower rates of victimization than transgender identified individuals; it is possible this is due to them not being as out or able to be out about their identities with providers as their transgender counterparts, and therefore, less susceptible to these negative experiences. NB, genderqueer, agender, and others with similar identities may have very different experiences than their transgender peers (Harrison et al., 2012), and more research is needed to explore this.
Unique to this examination of health care discrimination among TNB individuals was the inclusion of disability status, although a 2017 study found that disabled TNB individuals experienced higher rates of discrimination in accessing mental health services than their nondisabled counterparts (Kattari, Walls, & Speer). Across all forms of violence examined, disabled TNB individuals had significantly elevated odds ratios for victimization, indicating the need to explore the intersection of ableism and transphobia more fully as related to experiences of violence in health care settings.
Limitations
This study involved secondary data analysis of an existing survey, and therefore, it has many of the limitations associated with secondary data, such as not having input on the design of survey questions. It would have been useful to get more information about the types of health care contexts in which victimization occurred, whether the perpetrator was a provider or staff member, whether the context was one of general care or specialty care, and so forth. In addition, this survey was cross-sectional, meaning that the data only provided a one-time snapshot of these instances of health care victimization experienced by TNB individuals. Future survey responses might differ, depending on laws and policies of individual cities, counties, and states; current political climate; and other variables. Because of these challenges, there is a demonstrated need for both cohort and longitudinal studies of the TNB population.
This sample, especially among the dependent variables, contained very small numbers of individuals belonging to certain groups that needed to be dropped from the analytic sample. Regarding future samples, researchers should consider oversampling among marginalized identities to have enough power to run proper statistical analysis. In addition, the USTS sample was based in the United States, and further research is needed to assess whether these findings are similar to findings in other countries.
Finally, these data were collected as part of a purposive sample of TNB individuals living in the United States. As of date of publication, there were no representative data on this population, and therefore, we could not assess how accurately this sample reflects the TNB population in the United States. It is important to consider the community context of participants’ lives. While the USTS data were collected from disparate locations, the present study did not examine the impact of location on the victimization experience. The United States varies in TNB inclusivity by location, and experiences likely co-vary by region or state. For example, after adjusting for individual- and state-level factors, Hughto et al. (2016) found that the strongest state-level predictor of transgender refusal of care was the percent of state residents voting Republican. Given the high rates of victimization, violence, and overall discrimination and disparities faced by this population, it is beyond crucial for representative data on this population to be collected in the future to better inform current and future interventions as well as the direction of future research.
Implications
Despite these limitations, the present study builds on previous TNB health care victimization research by corroborating previous risk factors (e.g., low income) and identifying new ones (e.g., disability status). Regarding health care practice, there is a clearly demonstrated need for increased training for providers to reduce their uncertainty in working with this population and reduce the need to reassert power in the patient–provider relationship through discriminatory, or even violent, behaviors. This education needs to use an intersectional lens that includes the experience of TNB individuals who experience multiple types of marginalization across various identities. There also needs to be systems that support TNB individuals in reporting such instances of victimization that are inclusive around diverse genders and protect patients from penalization or retaliation from providers. Some organizations are already working to better support providers in being inclusive and affirming of trans individuals and can serve as a model for future trainings (Love et al., 2018; Reisner et al., 2015).
Future research needs to conduct more nuanced analyses that take diverse TNB identities into consideration. Using 2005–2013 Behavioral Risk Factor Surveillance System data, Stepanikova and Oates (2017) found that intersecting identities had differential risk patterns for perceived health care discrimination, though a binary concept of gender was applied. Researchers should consider replicating these efforts with TNB samples to determine if similar patterns hold true. There is also the need for research that more specifically distinguishes the perpetrator of victimization (providers, staff, other patients, etc..), as well as that more specifically analyze the type of service, such as mental versus physical health services and routine care versus specialty care.
Conclusion
Research, including findings from this study, demonstrates that TNB people experience victimization in many health care settings. Experiences of violence and victimization of this population in health care settings may result in medical mistrust, decisions not to seek out needed medical care, and the longer term impact of not being able to receive quality health care. These experiences of TNB individuals in health care settings drive the point home that health care professionals need more education, resources, and cultural responsiveness training in working with this population. Without acknowledging this and working toward better quality care and reduced victimization for TNB people, this population will continue to experience mistreatment and violence in health care settings.
Footnotes
Acknowledgments
We would like to acknowledge the National Center for Transgender Equality for their important work on this survey and willingness to share their data and members of the TNB community for their labor in participating.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.