
Abstract
Retained bullets are common after firearm injuries, yet their management remains poorly defined. Surgeon members of the Eastern Association for the Surgery of Trauma (N = 427) were surveyed using an anonymous, web-based questionnaire during Spring 2016. Indications for bullet removal and practice patterns surrounding this theme were queried. Also, habits around screening and diagnosing psychological illness in victims of firearm injury were asked. Most respondents were male (76.5%, n = 327) and practiced at urban (84.3%, n = 360), academic (88.3%, n = 377), Level 1 trauma centers (72.8%, n = 311). Only 14.5% (n = 62) of surgeons had institutional policies for bullet removal and 5.6% (n = 24) were likely to remove bullets. Half of the surgeons (52.0%, n = 222) preferred to remove bullets after the index hospitalization and pain (88.1%, n = 376) and a palpable bullet (71.2%, n = 304) were the most frequent indications for removal. Having the opportunity to follow-up with patients to discuss bullet removal was significantly predictive of removal (odds ratio (OR) = 2.25, 95% confidence interval (CI) = [1.05, 4.85], p = .04). Furthermore, routinely asking about retained bullets during outpatient follow-up was predictive of new psychological illness screening (OR = 1.94, 95% CI [1.19, 3.16], p = .01) and diagnosis (OR = 1.86, 95% CI = [1.12, 3.09], p = .02) in victims of firearm injury. Thus, surgeons should be encouraged to allot time for patients concerning retained bullet management so that a shared decision can be reached.
Firearm trauma has remained a major cause of injury related deaths in the United States, with more than 39,000 firearm fatalities estimated in 2017 (Centers for Disease Control and Prevention, 2018). In addition, for the annual 95,000 patients who survive a firearm injury (Centers for Disease Control and Prevention, 2018), recovery is often complex and can require medical, legal, and psychological intervention (Greenspan & Kellermann, 2002). A wealth of data exists on managing firearm trauma, but less focus has been given to the bullet itself.
Most research on retained bullets entails associated adverse medical conditions like infection, pain, and lead intoxication (Apte et al., 2019; Jakoi et al., 2015; Najibi et al., 2006). Other small series have concluded that removal is indicated only when the projectile rests in close proximity to neurovascular structures, intra-articular spaces, or weight-bearing regions (Eylon et al., 2005; McQuirter et al., 2001; Riehl et al., 2013, 2015). Due to such variation in practice, many surgeons may interpret removing a bullet, that is, bulletectomy, as unnecessary because these circumstances are uncommon. Although a retained bullet may not physiologically harm a patient, it may still precipitate adverse psychological conditions such as anxiety, depression, and posttraumatic stress disorder (PTSD; Greenspan & Kellermann, 2002; Montgomerie et al., 2015; Powers et al., 2014; Smith et al., 2018).
No consensus exists on the optimal treatment of retained bullets. Therefore, we seek to obtain the perspective of contemporary trauma surgeons to understand management schemes for retained bullets. We also wish to examine if a relationship exists between retained bullet practice patterns and new psychological illness screening and diagnosis. We hypothesize that (a) most surgeons do not routinely remove retained bullets, (b) surgeons do not consider psychological conditions as indications for bullet retrieval, and (c) bullet removal practices are not associated with psychological illness screening or diagnosis.
Method
Participants
In Spring of 2016, an anonymous online survey was created and distributed to current Eastern Association for the Surgery of Trauma (EAST) members via email. EAST was selected for this investigation because it is a diverse assembly of more than 2,000 national surgeon practitioners dedicated to the progressive care of the trauma patient. The University of Pennsylvania institutional review board approved this study. Completion and return of the questionnaire (appendix) indicated that informed consent was given. There were 34 questions and the survey was available for 28 days. The responses were anonymous with respect to individual names and locations of practice.
Measures
Survey questions examined respondent sex, work experience, and clinical setting (trauma center designation, academic affiliation, and hospital location). We also queried the respondent’s institution’s rate of penetrating trauma. We inquired if there was a formal hospital policy for retained bullet management, and if so, what did the policy entail. We also asked about the number of retained bullets removed by the respondent in the past year, the setting, and timing in which they were removed, as well as the body location from where they were removed. Using a Likert-type scale (never, rarely, sometimes, almost always, always), specific surgeon practice patterns were queried regarding proclivity to (a) arrange outpatient follow-up to discuss bullet removal, (b) ask about retained bullets during an office visit, and (c) allow a patient to influence his or her decision to remove a bullet.
Outcomes
We had three study outcomes, which included a surgeon’s likelihood to remove a retained bullet from a patient, screen for a new psychological illness in a patient with a retained bullet, and diagnose a new psychological illness in a patient with a retained bullet. Bullet removal frequency was asked using a Likert-type scale. To determine bullet removal likelihood, a survey response of almost always or always was considered “likely” while sometimes, rarely, and never were considered “unlikely” responses. A surgeon was also considered “likely” to remove a bullet if he or she removed ≥25% retained bullets in the past year, estimated by dividing the total annual number of retained bullets removed by the total number of nonfatal firearm injury patients treated. After categorizing responses into likely or unlikely, we performed multivariable logistic regression analysis to determine which surgeon practice patterns were associated with bullet retrieval. We similarly investigated each respondent’s habits in screening for and diagnosing new psychological illness in the outpatient setting at time of follow-up (2 weeks to 30 days) in patients who were injured by a firearm. We also performed a multivariable logistic regression to determine which practice patterns were associated with psychological illness conducts.
Data Analysis
All survey data were collected and entered into a secure web-based application (Research Electronic Data Capture, that is, REDCap™), which met Health Insurance Portability and Accountability Act (HIPAA) compliance standards. Likert-type scales were utilized for many of the responses because these questions pertained to attitudes, opinions, or practices, which are not intuitively grouped into binary responses. Multivariable logistic regression was used to determine which surgeon practice patterns predicted bullet removal after adjusting for institutional penetrating trauma rates, a policy for bullet removal, trauma center designation, surgeon sex, specific surgeon practice patterns, and years in practice. Multivariable logistic regression was also performed to evaluate which surgeon practice patterns were associated with screening for and diagnosing psychological illness after adjusting for the same aforementioned variables and bullet removal. Analyses were performed with JMP® Pro software, Version 14.2 of the SAS® System for Windows® (Copyright © 2018 SAS Institute Inc., SAS Campus Drive, Cary, USA).
Results
Participants
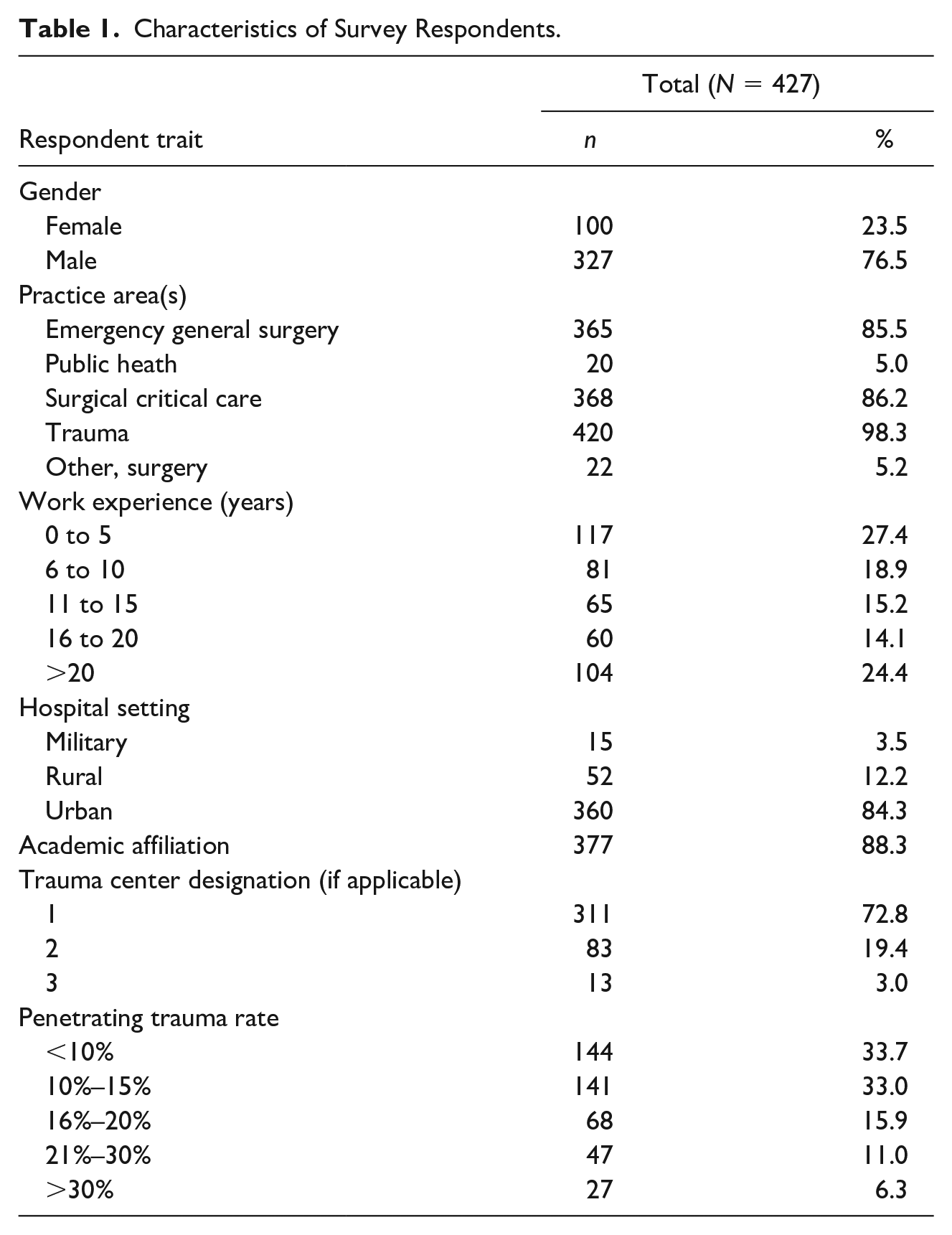
A total of 472 surgeons of 1,710 surveyed participated (27.6% response rate). We excluded 45 returned surveys due to incompleteness, which yielded 427 surveys for analysis. The majority of respondents were male (76.6%, n = 327) and specialized in trauma surgery (98.3%, n = 420; Table 1). Years of work experience varied, with the greatest response from surgeons with 0 to 5 years (27.4%, n = 117) and more than 20 years (24.4%, n = 104). Most respondents practiced in urban (84.3%, n = 360), academic (88.3%, n = 377), and Level 1 trauma centers (72.8%, n = 311). The most frequent rates of penetrating trauma were <10% (33.7%, n = 144; Table 1).
Characteristics of Survey Respondents.
Surgeon Bullet Removal Practices
Retained bullets were preferably removed in the operating room (78.5%, n = 335) and after the index hospitalization (52.0%, n = 222; Table 2). Only 14.5% of the cohort (n = 62) had an institutional policy for bullet removal, which typically provided specific indications for retrieval (37.1%, n = 23) or recommended against removal (24.2%, n = 15; Table 2). For all respondents, the most frequently provided indications for bullet removal were pain (88.1%, n = 376), a palpable bullet (71.2%, n = 304), and infection (40%, n = 170; Figure 1). Less common reasons for bullet retrieval were patient anxiety (12.9%, n = 55) and PTSD (4%, n = 17; Figure 1). When querying the ratio of retained bullets removed in the past year, most surgeons responded with 1% to 5% (32.1%, n = 137), whereas only 6.3% (n = 27) of respondents answered ≥ 25% (Table 2). Bullets were retrieved most often from a patient’s lower extremities (41.5%, n = 177), torso (32.1%, n = 137), and upper extremities (30.7%, n = 131).
Retained Bullet Practices.

Note. ED = emergency department; ICU = intensive care unit; OR = operating room.

Indications for bullet removal (N = 427).
Only a third of surgeons (33.5%, n =143) were likely to follow-up with patients after acute injury to discuss bullet removal (Table 2). Less than a third of surgeons (27.6%, n =118) were likely to ask about retained bullets on outpatient follow-up. Approximately, a third of surgeons (30.8%, n = 131) responded that a patient’s request influences his or her decision to remove a retained bullet. Interestingly, only 8.7% (n = 37) of surgeons were likely to remove a bullet (Table 2). On multivariable logistic regression (Table 3), arranging outpatient follow-up for discussion of removal (odds ratio (OR) = 2.25, 95% confidence interval (CI) = [1.05, 4.85], p = .04) was significantly associated with bullet removal.
Multivariable Logistic Regression Predicting Bullet Removal (N = 427).

Note. OR = odds ratio; CI = confidence interval.
p < .05.
Surgeon Practice With Psychological Screening and Diagnosis in Patients Following Firearm Injury
A portion of surgeons (32.8%, n = 140) were likely to screen for psychiatric illness in patients who sustained gunshot wounds. A smaller percentage of surgeons (27.9%, n = 119) routinely diagnosed psychiatric illness in these patients. On multivariable logistic regression (Table 4), surgeons working at a Level 1 trauma center (OR = 1.92, 95% CI = [1.11, 3.32], p = .02) and surgeons who asked about retained bullets during follow-up (OR = 1.94, 95% CI = [1.19, 3.16], p = .01) had a greater odds of being likely to screen for new psychological illness (Table 4). On multivariable logistic regression predicting diagnosis of new psychological illness, the same variables were significantly associated as having an institutional policy for bullet removal (OR = 1.84, 95% CI = [1.01, 3.30], p = .04; Table 5).
Multivariable Logistic Regression Predicting New Psychological Illness Screening by a Surgeon (N = 427).

Note. OR = odds ratio; CI = confidence interval.
p < .05.
Multivariable Logistic Regression Predicting New Psychological Illness Diagnosis by a Surgeon (N = 427).

Note. OR = odds ratio; CI = confidence interval.
p < .05.
Discussion
In this study, we determined that 8.7% of surgeons are likely to remove a retained bullet, whereas the remainder of surgeons never, rarely, or sometimes remove a bullet. Common reasons for removal were pain and a palpable bullet, which are indications supported by several series. Researchers contend that there are specific indications for bullet retrieval such as ballistics in joints, ones impinging a nerve or causing pain; bullets causing lead poisoning; or palpable bullets (Dienstknecht et al., 2012; Hafertepen et al., 2015; Richards et al., 1990). PTSD and anxiety were infrequently cited as indications for bulletectomy. Although the literature does not detail the optimal timing of removal, we found that most surgeons prefer to remove a bullet after the index hospitalization. We also discovered that a third of the surgeons were likely to arrange follow-up to discuss bullet removal and this practice was a significant and independent predictor of bullet removal. Although it is likely that the group of surgeons arranging follow-up for removal discussion were already biased toward removal, it is also possible that facilitating a more in-depth and less rushed patient experience facilitated bullet removal.
Recent work by Smith and colleagues demonstrates that patients with retained bullets have more severe depression and a poorer quality of life compared with patients without retained bullets. They found that retained bullets are associated with a decreased likelihood of returning to baseline employment (Smith et al., 2018). Social science research corroborates these discoveries; Lee states that over half of the gunshot victims he encountered lived with retained bullets and these bullets were major sources of pain and anxiety (Lee, 2012). Lee also states that many victims protested for bullet removal, but their surgeons refused due to the pretense that removal could cause more harm than good (Lee, 2012). Fortunately, we found that 30.8% of surgeons were likely to allow a patient’s request to influence their decision to remove a bullet. This finding demonstrates that some trauma surgeons incorporate patient wishes into the surgical planning process, which contradicts the theory that surgeons are paternalistic and inconsiderate (Wu et al., 2001). In fact, similar findings have been demonstrated in literature regarding breast cancer treatment. Wu et al. found that patients who were more concerned about losing a breast were less likely to be recommended a mastectomy by their surgeons (OR = 0.39, 95% CI = [0.16, 0.94]), whereas patients who were more concerned with dying from cancer were more likely to be recommended a mastectomy (OR = 4.6, 95% CI = [1.94, 11.59]). The authors concluded that surgeons integrate patient preferences and concerns into treatment recommendations (Wu et al., 2001).
Retained bullets can also be constant reminders of the shooting and may lead to psychological issues (Lee, 2012). A minority of surgeons in our survey screened for and diagnosed PTSD and depression in patients who sustained gunshot. In a similarly powered study of orthopedic surgeons regarding psychological screening and referral practices, approximately 45% of surgeons reported that they were somewhat or very likely to formally screen patients for psychiatric disease. Although the authors did not perform association analyses, on our multivariable logistic regression we found that asking about retained bullets was a significant predictor of psychiatric disease screening and diagnosing—bullet removal was not predictive. We surmise that surgeons who ask patients about retained bullets provide appropriate time for patients to vocalize concerns; these surgeons attentively listen and avoid haste (Braaf et al., 2018). Moreover, Vranceanu et al. believe this empathic communication style is key to screening and discussing psychological issues with trauma patients (Vranceanu et al., 2017). These authors understand that injury and psychological symptoms are highly intertwined. Interestingly, we did identify that working at a Level 1 trauma center increased the odds of both screening for and diagnosing psychological illness. This finding is likely because Level 1 centers are generally staffed by more experienced surgeons, emphasize injury prevention, follow injury recommendations from the American College of Surgeons, and frequently possess more resources than lower-level centers (Cudnik et al., 2009; American College of Surgeons: Committee on Trauma, 2014). Inasmuch, all patients injured by firearms should be approached with empathy to better identify psychological disease and to promote patient satisfaction (Jacoby et al., 2020; Menendez et al., 2015).
Limitations
Our study has inherent limitations. We had a response rate less than 30%, which may have introduced a selection bias. Furthermore, the vast majority of respondents were male surgeons from academic, urban centers, which does not accurately represent all of the diverse practices of EAST. In addition, we were unable to discern where the individuals with institutional policies on bullet removal came from. It is possible and likely that respondents with similar practices work at the same institution, which may confound the analysis. We also used Likert-type scale responses, which, although meant to enable flexibility in response, sometimes and rarely could be interpreted as interchangeable. Therefore, we grouped sometimes, rarely, and never into an “unlikely” category, but doing so may have inadvertently underestimated the number of surgeons who actually removed bullets because sometimes could also be interpreted as often. Another study limitation was that we lacked data on respondent race and ethnicity, which also may have influenced practice patterns.
Conclusion
We found that a minority of surgeons are likely to remove bullets and that psychological conditions are rare indications for bulletectomy. However, we did note that having the opportunity for follow-up was predictive of bullet removal and asking about retained bullets during outpatient follow-up was associated with psychological illness screening and diagnosis. Regardless of the clinical setting, surgeons should be encouraged to allot time for conversations with their patients, particularly concerning retained bullets, so that the management decision can be a shared effort.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
Sean Johnson is also affiliated with Icahn School of Medicine at Mount Sinai, New York, NY, USA.