
Abstract
In 2019, Sierra Leone declared national emergency over rape and other forms of sexual violence (SV), hence diverting resources from other issues to tackle SV. However, little is known about nationwide risk/protective factors for SV, and this has been a source of critique for the new policy. To fill this gap in knowledge, we investigated the factors for SV toward women using a nationally representative sample. We analyzed the 2013 Demographic and Health Survey (DHS) data, including 16,658 women, aged 15–49 years. The outcome was current SV, defined as being physically forced to have sexual intercourse within the last 12 months. We examined respondent’s background, sexual activities, and experience of domestic violence (DV). Logistic regression analyses were performed using STATA/SE v.15.1, accounting for survey design and sample weights. Values of p less than .05 were considered statistically significant. ArcMap was used to demonstrate geographic distribution of SV cases. We found that about 258 (6.3%) women reported SV. In adjusted analysis, women in the north (than south; 2.88, 95% CI = [1.44, 5.75]) and women circumcised between the ages of 1 and 14 (1.67, 95% CI = [1.10, 2.54]) reported higher risk of SV, respectively. Women who had sex more than 25 times per year were 6.9 times more likely to report SV, compared with those with 1 to 24 times (6.91, 95% CI = [1.48, 32.19]). The odds of SV were 6 times higher among women who reported experiencing recent physical violence (5.86, 95% CI = [2.49, 13.80]) or history of SV (6.34, 95% CI = [2.57, 15.65]). In conclusion, this study adds to the literature by providing information on major factors associated with SV toward women in Sierra Leone using a nationally representative sample. Women in the north (Tonkolili), circumcised between the ages of 1 and 14, had sex more than 25 times per year, reported physical violence (12 months before the survey) and SV (ever forced to have sex) reported higher risk for current SV. While more research is needed, these findings will help inform the current emergency operations against SV in Sierra Leone.
Introduction
The term “sexual violence” consists of “any sexual act, attempt to obtain a sexual act, unwanted sexual comments or advances, . . . directed, against a person’s sexuality using coercion, by any person regardless of their relationship to the victim, in any setting . . . ” (World Health Organization [WHO], 2011). Sexual violence is a serious global health problem that is associated with several risk factors, such as other forms of violence (physical and psychological aggression), and serious health and economic consequences (Smith et al., 2015). It affects mental health due to the consequences of prolonged stress and post-traumatic stress disorder (PTSD) (Chisholm et al., 2017).
Sexual violence is a major contributor to the global burden of disease, especially in low- and middle-income countries (LMICs). While limited data exist to address sexual violence in most countries, available evidence suggests that the lifetime prevalence of sexual violence among all ever-partnered women in the African region is 37%, an estimate that is significantly higher than that of the global estimates (30%) (WHO, 2014).
Among LMICs that are significantly affected by sexual violence is Sierra Leone (Garcia-Moreno & Stöckl, 2016; Statistics Sierra Leone and ICF International, 2014). The lifetime prevalence of sexual violence among all ever-partnered Sierra Leonean women is 49%, a rate higher than the reported estimates at the regional and global levels (Statistics Sierra Leone, 2013). The incidence of sexual violence affects women in all demographic facets in Sierra Leone, and some groups are more affected than others. According to the Sierra Leone Ministry of Health, spousal violence cases were prevalent in the Tonkolili district, with 63% of ever-married women reporting sexual violence by their partner. Women who are separated, divorced, or widowed have increased odds of experiencing spousal violence compared with those who are married or living together (Statistics Sierra Leone and ICF International, 2014).
To address this concern, in 2019, the Government of Sierra Leone (GoSL) declared a national emergency over rape and other forms of sexual violence due to the high prevalence of recorded cases, hence diverting resources from other national issues to tackle sexual violence (BBC World Service, 2019). However, little is known about factors influencing sexual violence in Sierra Leone, and this has been a source of critique for the new policy. Considering concerns other countries face in addressing sexual violence, we hypothesized that the potential challenges that may face the Sierra Leone health system in addressing sexual violence include the lack of early intimate partner violence (IPV) screening, inadequate access to health centers in rural communities, male partner exclusion (male perpetrators are often left out of the discussion), and difficulty in evaluating the impacts of existing programs (Kramer et al., 2012; Murray et al., 2014; National Child Traumatic Stress Network, 2017).
Previous studies (Marks, 2013, 2014; Ten Bensel & Sample, 2017; Williams & Opdam, 2017) in Sierra Leone have focused on the incidence and systematic use of rape during the years of the decade-long civil war in Sierra Leone, committed by rebel forces and forces loyal to the government, including health consequences and the call for international criminal justice for sexual violence victims through the International Criminal Court (Durbach & Geddes, 2017; Sellers, 2008). While studies have reported the incidence, prevalence, and systematic use of rape as a weapon of war during the Sierra Leone civil war (Jefferson, 2004; Teale, 2010), studies have not focused on the nationwide risk factors for sexual violence in post-war Sierra Leone.
To fill these gaps in knowledge, this article aims to investigate the risk factors for sexual violence among women using a nationally representative sample from the 2013 Sierra Leone Demographic and Health Survey (SLDHS). A deeper understanding of these factors will help inform the current emergency operations against sexual violence in Sierra Leone and sexual violence prevention strategies worldwide. This study includes women in Sierra Leone from a diverse socioeconomic status, ethnicity, language, religion, geography, age, and culture.
Method
Data and Population
We analyzed data from the 2013 SLDHS (Statistics Sierra Leone, 2013), including a weighted sample of 16,658 women, between the ages of 15 and 49 years. The 2013 SLDHS data were the most recent of datasets that were available at the time of this analysis. The Individual Woman’s Questionnaire of the 2013 SLDHS was used to investigate the risk and protective factors of sexual violence toward women in Sierra Leone.
The survey fieldwork took place between June and September 2013 (Statistics Sierra Leone and ICF International, 2014). The survey was funded by the GoSL and various government organizations including the United Nations Population Fund (UNFPA), the United Nations Development Programme (UNDP), WHO, the U.K. Department for International Development (DfID), the World Bank, the World Food Programme (WFP), the Food and Agricultural Organization (FAO), KfW Development Bank, and the United Nations Children’s Fund (UNICEF). According to the Statistics Sierra Leone and the DHS codebook, all data collection took place between June and September 2013, using in-person survey interviews of all selected households at the national level, urban–rural areas, regional level, and the 14 administrative districts. The data require approval from the DHS program of the U.S. Agency for International Development. The weighted sample represents all Sierra Leonean women, between the ages of 15 and 49 years. About 1,052 (20.3%) of respondents were missing for the sexual violence variable (outcomes). According to DHS, this is either because the question was not asked (due to interviewer error) or the respondent did not want to answer. Missing values are coded as “inconsistent,” “don’t know,” and “blank” (or “not applicable.”). DHS recommends that “missing,” “inconsistent,” “don’t know,” and “blank” codes should be excluded when calculating summary and inferential statistics. Hence, all missing values/observations were excluded from this analysis.
The 2013 SLDHS provides data for monitoring the health status of the population of Sierra Leone, with estimates at the national level, urban–rural areas, for each of the four regions/provinces and 14 districts. The 2013 SLDHS data provide contemporary information on various health issues including marriage, the status of women and children, awareness and health attitudes, domestic violence, and prevalence of HIV, malaria, and anemia. These data assist policymakers and local practitioners in the evaluation and design of strategies for improving population health.
Outcome Measure (Current Sexual Violence)
The primary outcome was sexual violence (rape). This variable was defined as being physically forced to have sexual intercourse within the last 12 months before the 2013 SLDHS. Sexual violence was categorized as a binary (no/yes).
Covariates: Potential Risk and Protective Factors
Covariates were respondent’s social and demographic characteristics, residential location, sexual activities, and experience of domestic violence. Covariates included the region of residence, categorized as southern, eastern, and northern provinces and the western area. The type of place of residence included urban and rural. Respondent age was classified as 15–25, 26–35, and 36–49 years. Education was categorized as no formal education and formal education. Ethnicity includes the Mende, Temne, and other all ethnic groups. Age at circumcision or female genital mutilation (FGM) was categorized as less than 1 year (infancy), 1–14 years, and 15 years and above. Current relationship/marital status included women who are married and not married. The frequency of sexual intercourse in the last 12 months was coded as 1–24 times per year, 25–49 times, and 50 times and above. Current experience with physical violence, having a history of sexual violence by the previous partner, and partner drinking alcohol were all categorized as no/yes.
Recent physical and historic sexual violence (no/yes) was defined using the Revised Conflict Tactics Scale (ElKady et al., 2005; Schumm & Bagarozzi, 1989). Recent physical violence was defined as whether the respondent was slapped, burnt on purpose, kicked, choked, bitten, pushed, punched, and assaulted using a knife or other weapons by their husband/partner in the past year. However, historic sexual violence was defined as whether any previous husband/partner ever physically forced the respondent to have intercourse or perform any other sexual acts, including being forced to have sex, and humiliating sexual acts or intercourse out of fear.
Analysis
First, we estimated sexual violence prevalence for each district and mapped these estimates for the country. We then calculated weighted frequencies to describe the population sample variables such as respondent’s background, FGM or sexual activities, and experience of DV. Second, we used logistic regression to perform unadjusted analyses to examine the bivariate association between population sample variables and sexual violence. Third, an adjusted logistic regression analysis was performed using a series of models (1–3) to assess whether identified factors were associated with a woman’s recent experience of sexual violence, adjusting for potential confounding factors. The first model examined the respondents’ background or demographic factors. The second included FGM or marital or sexual characteristics or factors. The third included all factors. We present the study findings in the form of percentages, odds ratios, and confidence intervals. All statistical analyses were performed using STATA/SE v.15.1 (StataCorp, 2017). Values of p less than .05 were considered to be statistically significant. Our study’s p-value was set apriori at .05 because this was the amount of Type I error we choose to allow given that we had a reasonably large sample size greater than 30 (n = 258). However, we did not modify our p-value from the set .05 because, from design, no effect modification or multiple comparisons were conducted in the analysis. In addition, ArcMap was used to demonstrate the geographic distribution of sexual violence cases in Sierra Leone.
Findings
A total of 258 (6.3%) women reported they were physically forced into unwanted sex by their husbands/partners (Table 1). In the unadjusted analysis (Table 2), the region of residence was significantly associated with sexual violence (p < .01). As demonstrated in the map showing geographic distribution and estimates of sexual violence cases (Figure 1), the rate of sexual violence was highest in the northern province, mainly in Tonkolili district (ranges from 7.9% to 17.2%), followed by Kionadugu, Bombali, Kambia, Port Loko, Kailahun districts (East), and Western Area Rural (4.4%–9.9%), compared with Bo district in the south (3.0%–4.4%). Ethnicity (p < .01), age at circumcision (FGM) (p < .01), current exposure to physical violence (p < .01), frequency of sexual intercourse (p < .01), having a history of reported sexual violence (p < .01), and alcohol drinking by partner (p < .02) were significantly associated with sexual violence.
Population Description (N = 16,658).

Note. FGM = female genital mutilation.
Logistic Analysis (Outcome = Sexual Violence).
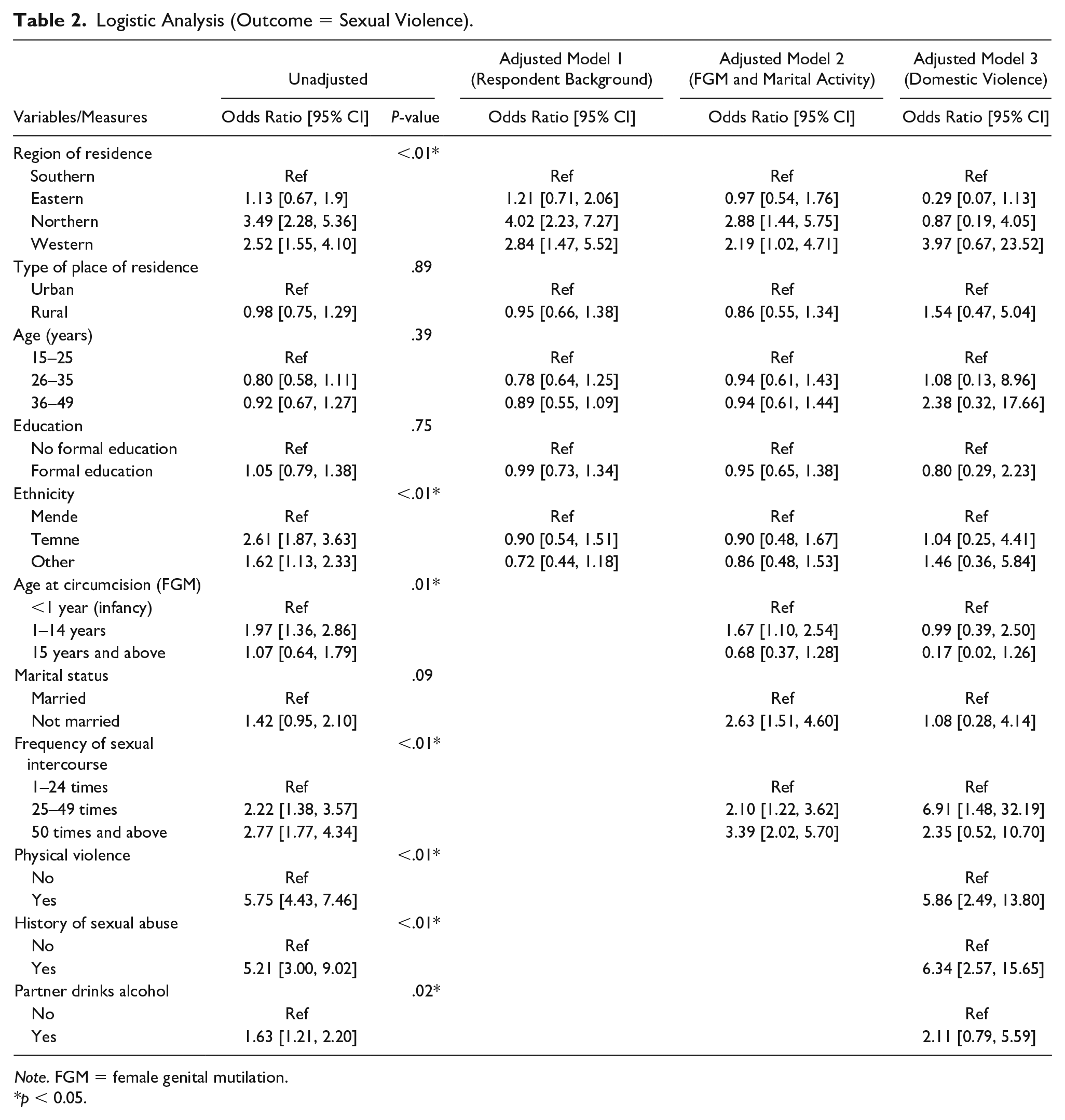
Note. FGM = female genital mutilation.
p < 0.05.
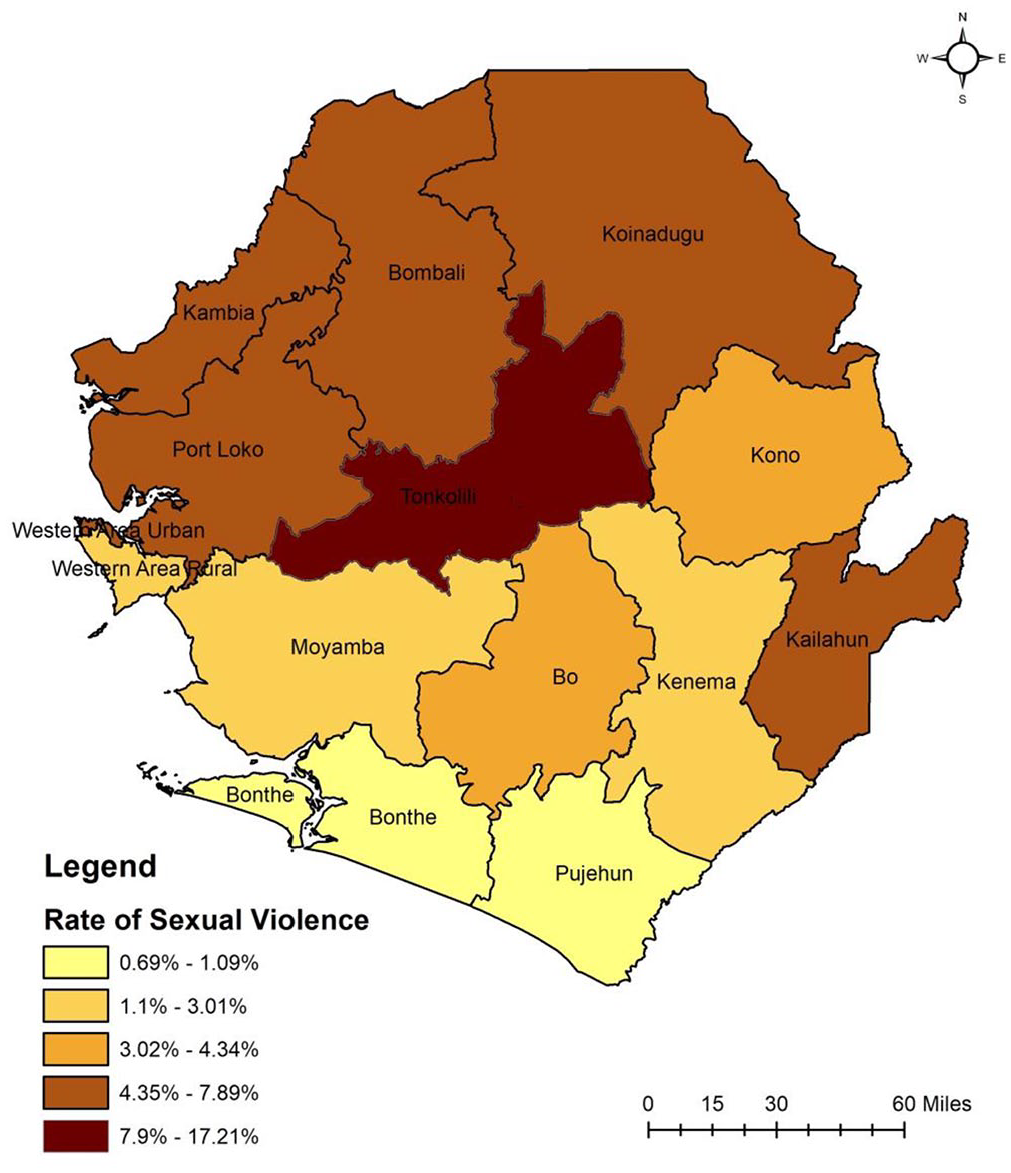
Geographic distribution of sexual violence cases in Sierra Leone.
After adjusting for respondents’ background and FGM or marital/sexual activities (Model 2), women in the northern and western regions were almost 3 times (2.88, 95% CI = [1.44, 5.75]) and 2 times (2.19, 95% CI = [1.02, 4.71]) more likely to report experiencing sexual violence compared with the south, respectively. Women who reported experiencing FGM below the age of 14 (1.67, 95% CI = [1.10, 2.54]) were unmarried (2.63, 95% CI = [1.51, 4.60]), and reported having sexual intercourse more than 25 times a year (3.39, 95% CI = [2.02, 5.70]) had higher odds of reporting experiencing sexual violence. After adjusting for respondents’ background, FGM or marital activities, and domestic violence variables (Model 3), women who reported having sexual intercourse more than 25 times a year were 6.9 times more likely to report experiencing sexual violence, compared with those who had less number of sexual intercourse between 1 and 24 times (6.91, 95% CI = [1.48, 32.19]). The likelihood of sexual violence was 2 times higher for women whose partners drink alcohol (2.11, 95% CI = [0.79, 5.59]) and 6 times higher among women who recently reported experiencing physical violence (5.86, 95% CI = [2.49, 13.80]) or reported historic sexual violence (6.34, 95% CI = [2.57, 15.65]).
Discussion
This article investigated the risk and protective factors for sexual violence against women in Sierra Leone using a nationally weighted sample, to help inform the current emergency operations against sexual violence by the GoSL and anti-sexual violence strategies worldwide. We found that region of residence (north), FGM (circumcision <14 years), sexual activity (>25 times per year), alcohol drinking by the partner, and experiencing recent physical violence and historic sexual violence are significantly associated with current sexual violence. While we did not find evidence of significant protective factors, these findings will help inform where and what factors to target in the current emergency operations against sexual violence in Sierra Leone. This analysis addresses limitations in the existing literature (Cohen, 2018; Marks, 2013, 2014; Pankhurst, 2012; Ten Bensel & Sample, 2017) that did not address factors associated with sexual violence, and to help inform the current emergency operations against sexual violence interventions by the GoSL.
Our findings are consistent with previous studies (Heaton, 2015; Meinck et al., 2015) on sexual violence in other countries, which further validates our findings. Our findings that a history of exposure to sexual violence and current exposure to physical violence were significantly associated with sexual violence align with the evidence provided by a recent systematic review that discovered in varying samples of children and adults in Africa (Meinck et al., 2015). Sierra Leone’s situation is similar to that of the Democratic Republic of Congo, concerning sexual violence and neglected needs of sexual violence victims and unintended health consequences (Heaton, 2015). A study (Chu & Akinsulure-Smith, 2016) of West African immigrant women from high-prevalence countries in New York City found similar results.
The risk factors for sexual violence that are identified in this study can be further explained by household-level factors (poverty, household violence, extended-family, family functioning, parenting, and substance abuse) and community-level factors (exposure to bullying, and rural/urban location, gender inequalities) (Garcia-Moreno & Stöckl, 2016; Meinck et al., 2015). Other risk factors include FGM and forced or child marriage (Bunting, 2012; Ellsberg et al., 2015). A systematic review that published empirical studies on sexual violence identified two domains to be significantly associated with sexual violence victimization and perpetration: (a) the presence and acceptance of violence and (b) unhealthy sexual behaviors, experiences, or attitudes (Tharp et al., 2013). Another study conducted in Swaziland among females aged 13 to 24 years concluded that inadequate guidance and unstable environment place girls at risk of sexual violence, and strengthen educational opportunities and mother–daughter relationships were protective against sexual violence (Breiding et al., 2011). While these studies are essential in identifying the risk and protective factors for sexual violence in other countries, none of these studies focused on Sierra Leone or included certain covariates (ethnicity, age at circumcision) that were utilized in this study.
The findings of this study should be interpreted in light of Sierra Leone’s social and economic contexts. Our finding that region (north) and FGM between ages 1 and 14 years were at increased risk for sexual violence as compared with the south should be interpreted in light of the socioeconomic concerns facing women in the northern province, whose populations are the poorest with less education in the nation compared with the south, as studies show (Statistics Sierra Leone, 2013). While our findings suggest that higher rates of sexual activity are associated with sexual violence, it is likely because they are having sex against their will. Sierra Leone has one of the highest rates of FGM (removal of the clitoris) observed in West Africa, with about 9 in 10 women circumcised (Statistics Sierra Leone, 2013). According to the Ministry of Health, FGM is most common among the least educated women and those from the poorest households in the northern province such as Kambia and Tonkolili (97% each). FGM is a cultural practice carried out by women and many women do support it. However, this is a practice that is carried out for men, with severe and detrimental health impacts for women as our findings show. FGM is commonly understood to ensure virginity before marriage, faithfulness to a partner, and to increase their partners’ sexual pleasure (Johansen, 2017).
While FGM is a significant cultural practice, it constitutes a human rights violation, especially when minors are subjected to FGM without their informed consent, but only with parental or family consent. While further research on how FGM increases the risk for sexual violence is required, at a minimum, the GoSL should ensure a minimum age requirement relating minors undergoing FGM, at least 18 years and above. The 1991 Constitution of Sierra Leone (GoSL, 1991) prohibits violence and harmful practices against women and girls. Article 20(1) of the 1991 Constitution is the only section of importance, maintaining that “No person shall be subject to any form of torture or any punishment or other treatment which is inhuman or degrading.” Currently, penalties for causing harm, in general, are set out under other national laws such as the Child Rights Act of 2007 (GoSL, 2007) and the Domestic Violence Act of 2007 (Ahmed Tijan Kabbah, 2007). Offenses under the Child Rights Act is set out in Sections 33 and 35 which include harm caused to a child by any cultural practice, but not FGM and a fine of up to 30,000,000 Leones ($3,046) or imprisonment for up to 2 years, or both. Domestic violence offenses in the Domestic Violence Act is punishable under Section 2(3) by a fine of up to 5,000,000 Leones ($507.7) or imprisonment for up to 2 years, or both. Anyone who contravenes a protection order is punishable under Article 19(1) by a fine up to 5,000,000 Leones ($507.7) or imprisonment for up to 3 years, or both.
The above laws prohibit harmful practices against women and girls; however, there is currently no evidence of national legislation that provides punitive measures for the practice of FGM (Thomson Reuters Foundation, 2018). At the local level, however, some chiefdoms (including in the districts of Pujehun, Bo, Port Loko, Western Area Rural, and Western Area Urban), paramount chiefs, and local practitioners (soweis) have signed “Memoranda of Understanding” (MOUs) to ban FGM for girls below the age of 18 and require the consent of women above the age of 18 (Thomson Reuters Foundation, 2018). While these MOUs are positive steps in the right direction for community dialogue, they are entirely voluntary and have no legal standing (Amnesty International, 2014). Although our findings cannot establish this fact, a national law that provides criminal penalties on the participation and performance of local and medical professionals in acts of FGM may help to reduce sexual violence against women and girls.
Sierra Leonean women who reported experiencing recent physical violence or had a history of sexual violence were at significant risk for current sexual violence. This finding could be associated with the systematic use of rape during the civil war, and cultural beliefs and attitudes about wife-beating and FGM (Statistics Sierra Leone and ICF International, 2014). According to the Ministry of Health and Sanitation, more than 6 in 10 women (and one-third of men) approve that a husband is justified in beating his wife if she refuses to have sex, argues or goes out without telling her husband or partner, burns the food, or neglects the children.
The findings of this study should be interpreted in light of its limitations. While DHS data use a nationally representative weighted sample and a uniform survey instrument that allows for detailed international comparisons of health status and health indicators, it comes with limitations. The limitations include omissions and reporting and recall bias, particularly for age or other retrospective data relying on memory of a past event (Boerma & Sommerfelt, 1993), such as the prior experience of sexual violence in this study. In addition, the sample is small relative to the total N. This is because of the fewer number of women who responded to the sexual violence question, hence, underreporting and/or reluctance to report and cultural acceptance of violence, as suggested earlier, may have played a role. We acknowledge that given the high-prevalence figures for the country, our sample size is small. We used secondary data analysis, and most variables (such as age and frequency of sexual intercourse) were categorical rather than just a continuous, and investigators had limited choice of variables for protective factors. The factors identified are association and not causal. Future studies on this subject should take these limitations into account. Future research should consider including clearer and valid indicators of the types of sexual violence in multiple item questions as opposed to the single items included in this survey. In Sierra Leone, less is known about what protects youth from perpetration and victimization, or how protective factors change over time. Hence, we recommend a quantitative inquiry about protective factors of sexual violence. Future studies should examine the risk and protective factors of FGM and sexual violence among women of reproductive age in Sierra Leone.
Conclusion and Interpretation
African countries should be held to task in addressing sexual violence, by ratifying and effectively implementing the United Nations Security Council Resolution 1325 (Beoku-Betts, 2016). Sierra Leone’s National Action Plan (SILNAP) was passed in 2010 to implement UN Resolution 1325. Pillars two and three of SILNAP aim to protect and prevent women and girls from sexual violence, promote gender equality, and reduce institutionalized violence through strengthening women’s legal rights and local peace initiatives such as women’s activists. This plan needs effective implementation and resources (human, technical, and financial). Also, issues around women’s rights should be addressed because the majority of Sierra Leonean women are marginalized from their marital rights of access to land, subordination, and violation of women’s universal human rights (Berhane-Selassie, 2009), as enshrined in the Convention on the Elimination of all Forms of Discrimination Against Women (CEDAW), an international treaty adopted in 1979 by the UN General Assembly.
Practitioners and policymakers can play critical roles in interventions around early screening, research/evaluation, and expanding access to sexual violence prevention services in rural disadvantaged communities. However, given the acceptance of attitudes about wife-beating and FGM, it would be helpful for communities to prevent and reduce sexual violence perpetration using the STOP sexual violence: a technical package to prevent sexual violence (Centers for Disease Control and Prevention, 2016). The strategies highlight evidence-based interventions to promote changes in social norms that protect against violence (bystander approaches and mobilizing men and boys as allies), teach skills to prevent sexual violence (safe dating and intimate relationship skills), and provide economic supports and strengthen leadership opportunities to empower women and girls.
Recommendations for Research, Policy, and Practice
The first and perhaps most important is to identify women as early in life as possible (National Child Traumatic Stress Network, 2017) who may be potential victims for sexual violence. Sexual violence has a lifelong negative consequence on overall health; however, effective interventions exist to mitigate its impact. Promising interventions for women exposed to sexual violence include initiatives that address risk factors, including depression and PTSD. Other services include providing legal guidance and evidence-based screening or treatment in medical settings. IPV extremely affects women, including the nation’s public health and economic well-being. However, policymakers and practitioners can play an important role in responding to the needs of women exposed to sexual violence by supporting the following interventions.
Policymakers and health care providers should be trained (Laelago et al., 2017) to address the mental health effects of sexual violence by emphasizing mental health screening and treatment. This would include integrating the life course perspective (Donovan et al., 2016) and a trauma-informed approach into existing prevention programs to address lifetime stressors among women in high-risk communities. The government should provide women with a centered care approach recommended by the WHO guidelines (Sohal & James-Hanman, 2013). These recommendations are based on the experience of practitioners with survivors of sexual violence. Women who disclose sexual violence should be offered timely support through women’s groups, primary care providers, community-based organizations, and non-governmental organizations. Activities should include ensuring confidential and private consultations, validation and being non-judgmental and supportive, increase safety and support daily needs, conduct screening about the history of violence, and improve access to resources (legal and other services). Male partners should also be included in these intervention processes.
Finally, we need more qualitative enquires in different districts, especially in Kono, Bo, Kenema, and Moyamba, to learn about what they are doing differently to tackle sexual violence that can be replicated in Tonkolili district that have shown the high number of sexual violence cases, compared with other districts.
Footnotes
Acknowledgements
The authors thank the women who participated in the Demographic Health Survey (DHS) and the agencies that provided funding for this survey, such as the Government of Sierra Leone, and various governmental organizations including the United Nations Population Fund (UNFPA), the United Nations Development Programme (UNDP), the World Health Organization (WHO), the U.K. Department for International Development (DfID), the World Bank, the World Food Programme (WFP), the Food and Agricultural Organization (FAO), KfW Development Bank, and the United Nations Children’s Fund (UNICEF). Funding agencies have no role in the analysis and interpretation of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.