
Abstract
Experiences of intimate partner violence (IPV) victimization have well-established associations with poor mental health. There is also burgeoning evidence regarding the association between IPV perpetration and mental health in a small number of countries. However, there is a paucity of data about the gendered differences for these IPV experiences within sub-Saharan African. This study examines the association between IPV victimization, perpetration, and mental health outcomes for male and female adolescents and young adults in Uganda. Data on IPV perpetration were available for a nationally representative sample of 1,373 males and 2,022 females in Uganda. Observations were weighted to be representative of 13- to 24-year-olds in Uganda. Study procedures used multivariate logistic regression models to examine associations between ever-perpetration of IPV and four self-reported mental health variables: severe sadness, feelings of worthlessness, suicide ideation, and alcohol abuse. Models controlled for age, marital status, schooling, and past exposure to violence. Models were sex-disaggregated to examine sex-specific associations. Standard errors were adjusted for sampling stratification and clustering. Data analysis showed that males were more than twice as likely as females to perpetrate IPV (14% vs. 6%, respectively; p < .001), while odds of perpetration for both sexes were higher for those ever experiencing IPV (adjusted odds ratio [aOR] = 12.12 for males; aOR=4.73 for females). Male perpetrators had 2.93 greater odds of experiencing suicidal ideation (95% confidence interval [CI]: [1.78, 4.82], p < .001) and increased drinking behaviors (2.21, 95% CI: [1.39, 3.50], p < .001) when compared with non-perpetrating males. In addition, female perpetrators had 2.59 times greater odds of suicidal ideation (95% CI: [1.34,4.99], p < .01), as compared with non-perpetrating females. Our findings among youth and adolescents demonstrated associated but different experiences for males and females. Findings indicate the importance of understanding the relationship between IPV victimization and perpetration, and addressing these correlates with a gender-sensitive perspective to inform policy and programming.
Keywords
Introduction
Intimate partner violence (IPV), defined as physical, sexual, or emotional abuse that occurs in a relationship with a partner or spouse (Centers for Disease Control and Prevention [CDC], 2019), contributes to a myriad of poor health and mental health outcomes globally (Abramsky et al., 2011; Devries et al., 2013). Males are the most common perpetrators of IPV, whereas women are usually victimized (CDC, 2019). IPV victimization adversely affects personal physical, mental, sexual, and reproductive health. Women who experience IPV are more at risk of complicated pregnancies, low-weight babies, unsupervised abortions, depression, alcohol abuse, HIV infection, and suicide (Durevall & Lindskog, 2015; Johnson et al., 2014; World Health Organization [WHO], 2015). In addition, the larger scale impacts of IPV include impediments to economic and social development (WHO, 2015).
IPV victimization is often dynamically associated with IPV perpetration, wherein both partners are at risk of physical and emotional health consequences (Richards et al., 2016). However, less is known about the impacts of IPV perpetration, particularly specific associations between perpetration and mental health (Gibbs et al., 2018). From the limited literature that does exist, studies have found substance abuse, economic insecurity, risky sexual behaviors, and childhood trauma to be associated with men’s IPV perpetration (Krug et al., 2002; Machisa & Shamu, 2018; Spencer & Stith, 2018). Regarding mental health correlates, depression, anxiety, post-traumatic stress disorder (PTSD), antisocial personality disorder, and borderline personality disorder have been shown to be associated both with IPV perpetration and victimization among men. For women, borderline personality disorder has been shown to be a stronger correlate with IPV perpetration than victimization, whereas PTSD has been shown to be a stronger correlate with victimization than perpetration (Stark et al., 2020).
The majority of studies regarding IPV victim–offender dynamics have been conducted in high-income countries, yet multi-country studies have revealed higher IPV incidence in low- and middle-income countries (LMICs). In some LMIC, 62% of women reported experiencing at least one form of IPV, with the highest prevalence in the African region (WHO, 2012). In Uganda, more than half of married women report IPV victimization, whereas 40% of married men report perpetration (Speizer, 2009). These high rates of IPV experiences provide a unique opportunity to study sex-specific experiences and their mental health correlates.
More evidence is required to understand the ways in which sex, IPV perpetration and victimization, and mental health outcomes are associated in the African context. To fill this gap in the literature, a recently published study from Nigeria assessed sex-disaggregated associations between IPV perpetration, IPV victimization, and mental health outcomes among adolescents and young adults using data from the Violence Against Children Survey (VACS; Stark et al., 2020). The study found that males’ perpetration of IPV was significantly associated with feelings of worthlessness and alcohol use. In contrast, IPV perpetration from females was significantly associated with severe sadness and suicidal ideation. These findings allude to striking differences between the ways females and males might internalize IPV victimization and perpetration (Aluko, 2005). However, these findings are specific to conditions in Nigeria, the most populous country with the largest economy in Africa (Nwabunike & Tenkorang, 2017).
This article presents data from the Uganda VACS, examining the relationship between IPV victimization, perpetration and mental health outcomes among 13- to 24-year-old males and females. Associations were explored with four mental health variables—severe sadness, feelings of worthlessness, suicide ideation, and alcohol use. This article is one of the first to assess the gendered mental health correlates of IPV victimization and perpetration in Uganda. Evidence about IPV perpetration, particularly among adolescents and young adults in LMICs, is vital to provide a more tailored approach to targeting policy, interventions, and social norms that perpetuate IPV.
Method
Setting
Uganda is classified as a low-income country, with a gross domestic product (GDP) per capita of US$1,700 (Demyttenaere et al., 2004), and 87.8% of the population currently living below the international poverty line (The World Bank, 2020). Gender inequities, due in part to Uganda’s patriarchal norms, are most evident in educational attainment, child marriage, employment, and intimate partner relations (Koenig et al., 2003). In addition, from 1996 to 2006, Northern Uganda experienced a civil war that displaced 1.8 million people and saw the abduction of 66,000 children and youth as soldiers, sex slaves, or porters for the Lords’ Resistance Army (LRA). Histories of conflict and the recent influx of refugees have exhausted community resources and further perpetuated inequities (Durevall & Lindskog, 2015; Ugandan Bureau of Statistics [UBOS] & ICF, 2018). Witnessing violence, economic strain, and limited years of education due to protracted crisis are associated with higher rates of IPV (Abramsky et al., 2011; Kapungu et al., 2018; United Nations Children’s Fund [UNICEF], 2018). Current laws such as the Penal Code (Amendment) Act of 2007, the Domestic Violence Act of 2010, the Sexual Offences Bill, and the Marriage Bill do not address key aspects of violence against women (VAW). None of these laws criminalize marital rape or rape within cohabiting relationships (The World Bank, 2016).
Data
The Uganda VACS is a nationally representative data set collected in 2015 as part of a collaboration with the U.S. CDC (CDC); AfriChild; ChildFund; President’s Emergency Plan for AIDS Relief (PEPFAR); Transcultural Psychosocial Organization (TPO) Uganda; UBOS; United States Agency for International Development (USAID); and the UNICEF, the Ugandan government, and other local, bilateral, and multilateral partners. The VACS, which have been implemented in 11 countries as of 2019, collect detailed information on young people’s experiences of sexual, physical, and emotional violence. In Uganda, a total of 5,804 children ages 13 to 24 years were surveyed.
The original sampling frame for the Uganda VACS was compiled by UBOS for the 2014 Census. The primary sampling units were the enumeration areas (EA) previously used in the census. A three-stage cluster sample survey design was utilized. In the first stage, 368 female EAs and 400 male EAs were selected out of 78,093 EAs. This split sample approach was designed to protect the confidentiality of respondents and eliminate the chance that a perpetrator of sexual violence and victim of violence in the same community would both be interviewed. EAs were randomly selected with a probability proportional to the size of the EAs (the number of households). In the second stage, data collection teams conducted mapping and listing of all households in each selected EA. Twenty-five households in each EA were randomly selected by equal probability systematic sampling. In cases in which the total number of households exceeded 250, the survey teams segmented the EA into segments of approximately 100 households each. After segmenting the EA, segments were randomly selected (UNICEF, 2018).
For respondents 13 to 17 years of age, caregiver consent was obtained verbally and respondents provided assent to participate in the study. Consent for respondents 18 and over was obtained directly. Surveys were administered in seven languages: English, Iteso-Karamajong, Luganda, Lugbara, Luo, Swahili, Runyankole-Rukiga, and Runyoro-Rutooro. The interviews were only conducted in spaces where privacy could be ensured, as indicated by respondents and trained interviewers. Data were collected electronically using Electronic Data Capture (EDC) in CSPro and, to the extent possible. The protocol for the Uganda VACS was reviewed by the MakSPH ethics review committee, the Uganda National Council for Science and Technology, and the CDC Institutional Review Board (UNICEF, 2018).
Variables of Interest
This study utilized a sex-disaggregation method employed in a previous study (Stark et al., 2020) that used VACS data from Nigeria to assess the associations between perpetration of IPV and mental health outcomes for male and female adolescents and young adults while also controlling for exposure to violence, age, and education. Table 1 provides the operationalization of IPV perpetration and forms of violence exposure. Demographic variables of interest included age, partnership status, and if the respondent ever attended school.
Operationalization of Key Terms.
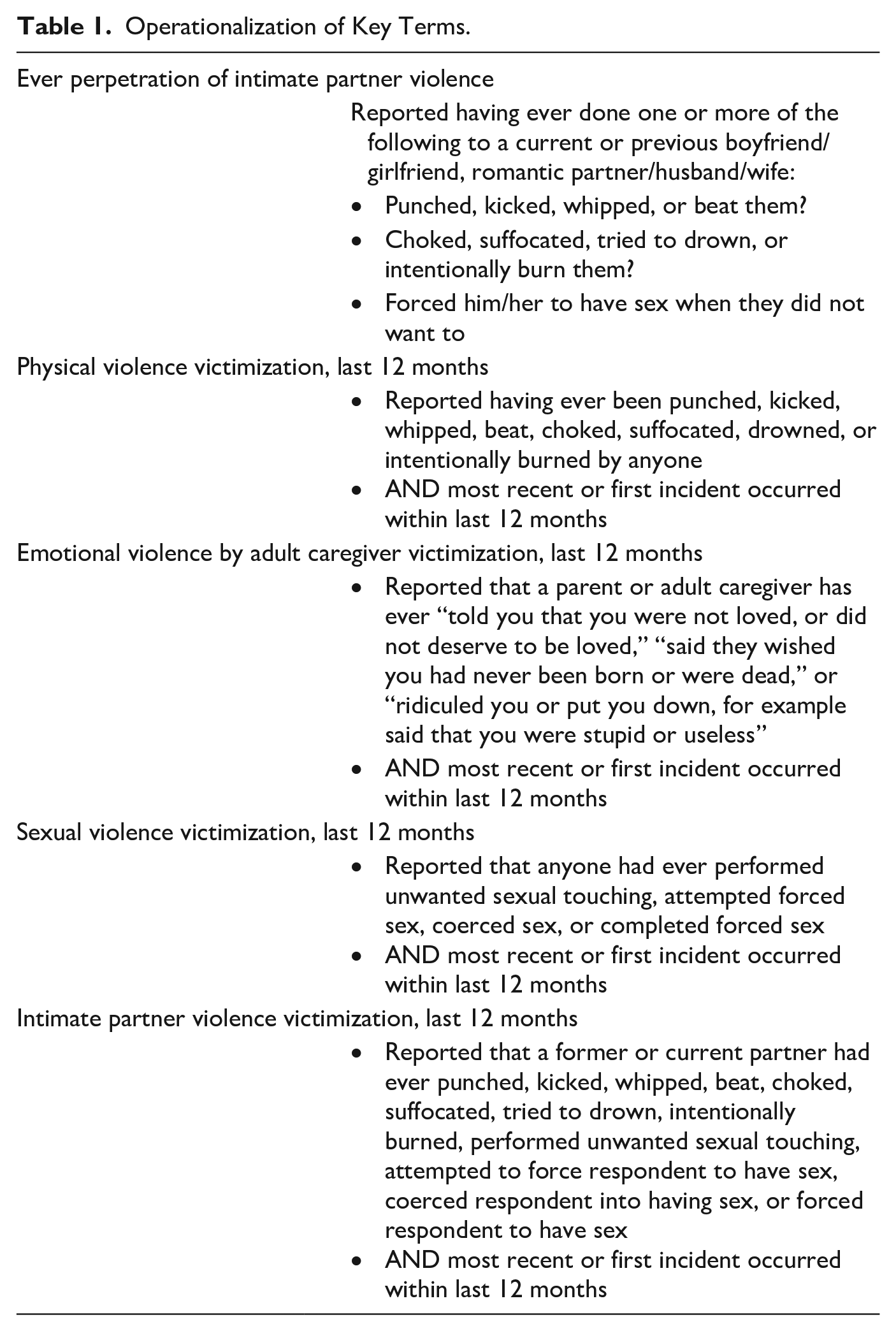
Four outcomes related to mental health were analyzed, each of which was operationalized using VACS survey questions. Two variables capture symptoms of depression: severe sadness and feelings of worthlessness. Respondents were considered to have severe sadness if they answered “all the time” or “most of the time” to the question: During the past 30 days, how often did you feel so sad that nothing could cheer you up? Respondents were considered to exhibit feelings of worthlessness if they selected one of the same two responses for the question: During the past 30 days, how often did you feel worthless? Respondents who selected “some of the time,” “a little of the time,” or “none of the time,” for either of these questions were considered defined as not exhibiting the respective symptom. Suicide ideation was operationalized in the binary using the question: Have you ever thought about killing yourself? Finally, a measure of alcohol use was developed from the survey question: In the past 30 days, on how many days did you drink alcohol to the point that you became drunk? This measure could take a value from 0 to 30.
Statistical Analysis
Data on IPV perpetration was available for 1,373 males and 2,022 females regardless of current partnerships status. Data about IPV perpetration were missing for 48% of males and 36% of females. Descriptive statistics for all correlates and outcomes of interest were first estimated for males and females, separately; differences between genders were assessed using adjusted Wald tests. There were 0.65% missing from feelings of sadness, 0.78% from feelings of worthlessness, 0.05% from suicidal ideation, and 0.12% from drinking behaviors. Due to the low rate of missing observations for outcomes of interest, a case-wise deletion method was used.
Logistic regressions were used to estimate the relationships between the correlates of interest and each of the mental health outcomes. Poisson regressions were used to estimate the relationship between the correlates of interest and the measure of alcohol use due to the nature of the variable. Model 1 estimated the relationship between ever-perpetration of IPV and the corresponding mental health outcome, while controlling for age, being married or in a domestic partnership, and having ever been to school. Model 2 included the same covariates from Model 1, in addition to four covariates representing past-year victimization. These included exposure to the four types of violence outlined in Table 1. All regressions were estimated separately for males and females to understand how these relationships may be gendered. Observations were weighted to be representative of the population of 13- to 24-year-olds in Uganda and standard errors were adjusted for the complex sampling design. All analysis was conducted using Stata V.14 (StataCorp LP, College Station, TX, USA).
Results
Key demographic characteristics and variables of interest across males and females are summarized in Table 2. Compared with males, females were more likely to have ever been partnered (33% vs. 13%; p < .001). Male and female adolescents and young adults faced different exposures to violence victimization as well. Past-year physical violence exposure among males was higher than among females (41% vs. 32%; p ≤ .001) and sexual violence victimization was higher among females (26% among females vs. 13% among males; p < .001). Females were significantly more likely to have experienced IPV in the last 12 months as compared with males (22% vs. 8%; p < .001), and less likely to perpetrate IPV (6% vs. 13%; p < .001). Finally, self-reported feelings of severe sadness and worthlessness in the last 30 days and ever considering suicide were more than twice as common among females (13%, 6%, and 12% among females vs. 7%, 3%, and 6% among males; p < .001).
Key Characteristics, by Gender.

Note. Based on questionnaire construction, sexual intimate partner violence (IPV) is counted in both sexual violence and IPV. Standard errors are adjusted for complex sampling design. All observations are weighted to be representative of the population. Statistical significance of differences between groups are assessed using adjusted Wald tests and differences are significant at *p < .05. **p < .01. ***p < .001.
When further examining the relationships between IPV perpetration and mental health outcomes within the past 30 days, there were a few significant findings presented in Table 3. Males who reported perpetrating IPV had 2.93 times higher odds of experiencing suicidal ideation than males who did not report ever perpetrating IPV, 95% confidence interval (CI): [1.78, 4.82], p < .001, even when controlling for demographic variables. Women who perpetrated IPV also had 2.59 times higher odds of experiencing suicidal ideation (95% CI: [1.34, 4.99], p = .01). Men who perpetrated IPV reported increased alcohol use by a factor of 2.21 (95% CI: [1.39, 3.50], p = .001). In contrast, women who perpetrated IPV did not have a statistically significant increased risk of alcohol use.
Perpetration of IPV, Mental Health Symptoms, and Alcohol Use in Uganda, Adjusted Odds Ratios.
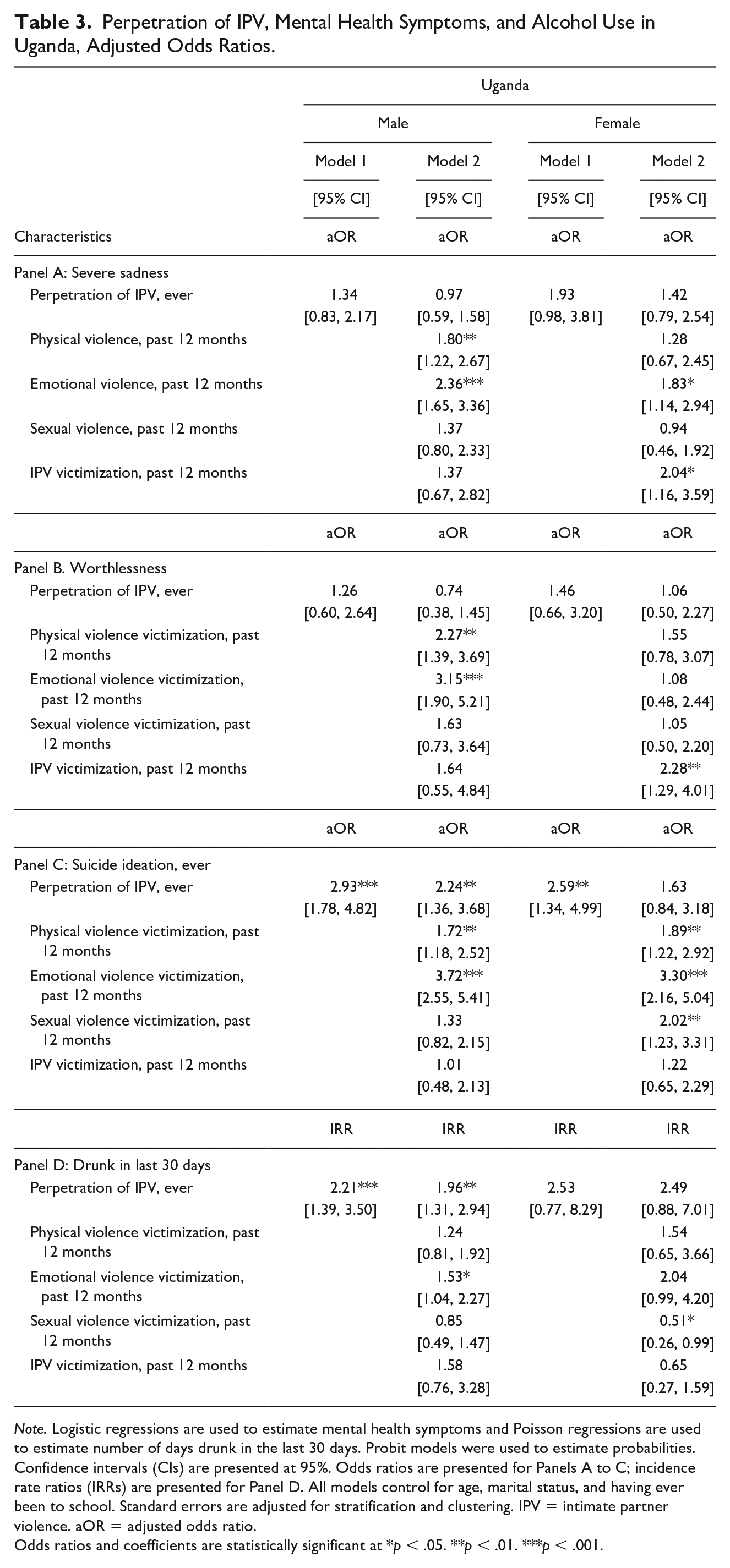
Note. Logistic regressions are used to estimate mental health symptoms and Poisson regressions are used to estimate number of days drunk in the last 30 days. Probit models were used to estimate probabilities. Confidence intervals (CIs) are presented at 95%. Odds ratios are presented for Panels A to C; incidence rate ratios (IRRs) are presented for Panel D. All models control for age, marital status, and having ever been to school. Standard errors are adjusted for stratification and clustering. IPV = intimate partner violence. aOR = adjusted odds ratio.
Odds ratios and coefficients are statistically significant at *p < .05. **p < .01. ***p < .001.
Regarding victimization, males who experienced emotional violence had 2.36 greater odds of feelings of severe sadness (95% CI: [1.65, 3.36], p < .001), 3.15 higher odds of feelings of worthlessness (95% CI: [1.90, 3.5.21], p < .001), and 3.72 higher odds of suicidal ideation (95% CI: [2.55, 5.41], p < .001). Females who experienced emotional violence victimization in the past 12 months had 3.30 higher odds of suicidal ideation (95% CI: [2.16, 5.04], p < .001), In addition, men who experienced physical violence victimization in the past 12 months had 1.80 higher odds of experiencing feelings of severe sadness, 2.27 higher odds of experiencing feelings of worthlessness, and 1.72 higher odds of suicidal ideation (95% CI: [1.22, 2.67], p < .01; [1.39, 3.69], p < .001; and [1.18, 2.52], p < .01). Interestingly, these associations were not found to be significant with females. Females who experienced IPV victimization in the past 12 months had 2.04 higher odds of reporting feelings of severe sadness, and 2.28 higher odds of reporting feelings of worthlessness (95% CI: [1.16, 3.59], p < .05; [1.29, 4.01], p < .01). Finally, all findings are robust to the sensitivity analysis, in which the same models were estimated based on a subsample of individuals who had never experienced IPV.
Discussion
This study aimed to expand upon the existing evidence related to adolescents’ and young adults’ experiences of violence and their subsequent mental health outcomes. Male and female adolescents in our sample who experienced IPV victimization or perpetration had a higher likelihood of experiencing negative mental health outcomes; however, these mental health correlates differed by sex. Males who perpetrated IPV were significantly at risk of feelings of suicide ideation and worthlessness. Although female adolescent perpetrators were also shown to be at risk of suicide ideation, this association was moderated by experiences of victimization.
Past research shows that adolescents and young adults are more at risk of self-harm and suicidal ideation than their adult counterparts due to disturbed interpersonal relationships, poverty, and loneliness (Kinyanda et al., 2004, 2016); however, these findings have not previously been sex-disaggregated. Our findings add to the literature by demonstrating that the relationships between IPV victimization, perpetration, and mental health are highly gendered. Our findings differed from the original study using VAC in Nigeria, underscoring the contextual nature of these relationships. Future studies might further explore the contextual effects of urban and rural status and could include qualitative analysis to assess the role of culture, religion, and social norms related to IPV perpetration, IPV victimization, and acceptable expressions of mental health, and how and why these relationships might differ for males and females across sub-Saharan African contexts.
Interestingly, overall, the variables included in the analysis showed stronger associations for males than for females. One hypothesis is that women have more protective mechanisms, such as social support, that help them cope with their experiences of violence, whereas masculine experiences of violence may be subject to “ethical loneliness,” or routine silencing of their experiences by multiple layers of their ecologies (Schulz, 2018). Men might therefore be limited in their willingness to actively participate in gender transformative programming. In addition, collective detrimental community beliefs about household gender roles, including a promotion of males exercising controlling behaviors, may be normalized within the Ugandan context (Abramsky et al., 2016; Black et al., 2019; Koenig et al., 2003). Providing outlets for males to discuss these social ecologies may play an instrumental role in fighting toxic gender norms.
The life cycle approach posits that risk factors and protective factors for mental disorders are affected through development. Adolescence and young adulthood are critical life stages where social norms are entrenched and hormonal shifts may cause mental health volatility (Sawyer et al., 2018). Research shows that experiences during these formative periods, including exposure to violence, abuse, and neglect, can influence the adult-onset of mental health problems (Kapungu et al., 2018; Kieling et al., 2011). In addition, mental health issues that develop during adolescence and young adulthood can often persist later in life (Kim-Cohen et al., 2003; Patton et al., 2014). There is emerging attention to the serious mental health needs of African adolescents and young adults, many of whom face daily challenges, including extreme poverty (Kigozi et al., 2010; Kleintjes et al., 2010).
Our findings may have important implications for programming and policies within Uganda, the African region, and LMICs. The gendered findings from this study point to a need for more programs that can mitigate the different pathways between violence victimization, perpetration, and mental health. Such responses should be tailored to both female and male young adults, inclusive of their experiences and potential subsequent outcomes. Previous studies have found that integrated community mobilization interventions which engage men and women in dialogue about gender norms and behaviors are successful in decreasing IPV and improving mental health outcomes (Abramsky et al., 2016).
Although the data used in our analysis are comprehensive and nationally representative, there remain certain limitations. The cross-sectional nature of the data does not account for temporality, which limits our ability to confirm causal claims. Another limitation is that the data included a binary gender variable, which does not account for people who identify as gender nonbinary or transgender. This limitation supports claims made in other calls to action that survey data are often established in a way that reinforces existing gender norms, limiting the ability of researchers to collect the data needed to challenge such norms (Weber et al., 2019). Relatedly, although previous research has shown a high correlation between sexual orientation and risk of IPV, our data set did not account for individuals who identify as LGBTQA (lesbian gay bisexual transgender queer/questioning asexual). Men who have sex with men have a significantly high risk of IPV, especially in the African continent (Finneran et al., 2012; Stephenson et al., 2011). In addition, openly LGBTQA Ugandans face stigma, discrimination, harassment, and intimated compounded by legal restrictions (Thapa, 2015). Although this data set measured suicidal ideation, there may be some bias in data collection due to the criminalization of suicide in Uganda (Lubaale, 2017). Finally, the measures for assessing severe sadness, worthlessness, hopelessness, and other indicators of distress were not psychometrically tested measures for mental health. These questions were recoded to be binary from their original Likert-type scale form, which may have provided more detailed information about well-being.
Overall, the study has important implications for IPV policy and programming. The nuances in experiences of IPV victimization, perpetration, and mental health correlates for men and women in Uganda illuminate important components of IPV prevention and recovery interventions. Interventions should account for the duality of IPV victimization and perpetration, in addition to providing additional mental health services, including suicide assessments, for males and females based on the gendered pathways that are illuminated in different contexts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.