
Abstract
Intimate partner violence (IPV) has been related to brain alterations in female survivors. Nonetheless, few studies have used an exploratory approach, focusing on brain regions that are traditionally studied in other populations with post-traumatic stress. Traumatic brain injury (TBI), strangulation, and childhood trauma are highly prevalent among this population, and have also been associated with brain alterations and functional deterioration. As such, it is difficult to determine how different brain regions are affected by the complex interplay of these factors in female survivors. The aim of this study is to assess (a) brain alterations in female survivors of IPV as compared to non-victim females and (b) the potential causal mechanisms associated with such alterations. We hypothesized that structural brain differences would be found between female survivors of IPV and non-victims, and that these differences would be related to IPV-related TBI, strangulation, IPV severity, depression, post-traumatic stress, generalized anxiety, and childhood adverse experiences. A total of 27 non-victims and 28 survivors completed structural magnetic resonance imaging and questionnaires to measure the potential causal mechanisms for brain alterations. Structural brain differences were found between groups, principally in volumetric analyses. The brain regions in which between-group differences were found were related to attempted strangulation, IPV-related TBI, severity of IPV, adverse childhood experiences, and post-traumatic stress. These results demonstrate that a wider range of brain regions may be impacted by IPV and that various factors are implicated in the structural brain alterations found in female survivors. This study demonstrates the importance of post-traumatic stress, childhood and adult trauma, and physical violence in assessing brain alterations in IPV survivors. Further, it serves as a critical first step in assessing an extensive list of potential causal mechanisms for structural brain alterations, using a more comprehensive a whole-brain structural analysis of IPV female victims, a largely understudied and vulnerable population.
Keywords
Intimate partner violence (IPV) is a highly prevalent and pervasive problem. While prevalence rates are difficult to decipher due to underreporting, worldwide reports reveal that one in every three women has suffered either physical or sexual violence by her partners throughout her lifetime (Devries et al., 2013; World Health Organization, 2013). IPV is related to a wide array of sequelae, ranging from physical consequences such as autoimmune disorders and traumatic brain injury (TBI; Chandan et al., 2019; Valera et al., 2019) to mental health problems, such as post-traumatic stress and depression (Beydoun et al., 2012; Cavanaugh et al., 2012; Estefan et al., 2016). Until recently, little attention has been given to the neural mechanisms behind these consequences, namely those related to mental health problems and physical injury to the central nervous system caused by hits to the head or strangulation. This is surprising due to the fact that nearly 80% of IPV-related injuries are found on the head, neck or face among female victims who reach urgent care (Wong et al., 2014) and 97% of women who have been hit in the head have also suffered strangulation attempts (Shields et al., 2010).
The combined impact of psychological trauma and physical injury to the central nervous system have led to a burgeoning number of neuroscientific studies on the underlying brain mechanisms behind IPV-related sequelae. Of the neuroimaging studies conducted on female survivors, the majority have focused on brain alterations related to post-traumatic stress disorder (PTSD; Aupperle et al., 2012; Aupperle et al., 2013, 2016; Fennema-Notestine et al., 2002; Fonzo et al., 2010, 2013; Moser et al., 2015; Neumeister et al., 2018; Seedat et al., 2005; Simmons et al., 2008; Strigo et al., 2010). Despite the difficulties in making generalizations due to methodological differences, neuroimaging research on IPV-related PTSD indicates functional brain differences in IPV survivors when viewing stimuli with emotional content.
In terms of structural brain differences, there have only been four studies to date that have examined structural alterations related to psychological trauma or general IPV severity (Flegar et al., 2011; Fonzo et al., 2013; Fennema-Nostentine et al., 2002; Roos, et al., 2017). Two of these studies employed an exploratory whole-brain design (Fennema-Notestine et al., 2002; Roos et al., 2017), while the others restricted analyses to specific regions of interest (Flegar et al., 2011; Fonzo et al., 2013) or to one study group of IPV victims to study brain alterations in terms of childhood trauma (Fonzo et al., 2013). While results from these studies coincide in not finding differences between female victims and non-victims in the hippocampus (Flegar et al., 2011; Fennema-Notestine et al., 2002; Roos et al., 2017), additional alterations were found in the exploratory studies (Fennema-Notestine et al., 2002; Roos et al., 2017). In contrast to the first exploratory study in which structural differences were found in the supratentorial cranial vaults, and frontal and occipital gray matter (Fennema-Notestine et al., 2002), no structural differences were found in the study conducted by Roos et al. (2017). Discrepancies across studies may be in part due to the methodological differences for determining brain differences, as well as the inclusion criteria used to determine the comparison groups. For example, in one study the “control” group was made up of women who had not suffered violence in the past year (Roos et al., 2017), which leaves the possibility of having suffered IPV earlier on. In relation to variables that may explain these structural alterations, two studies took into account the potential contributing effect of childhood trauma, and found both structural and functional alterations in relation to childhood trauma in female survivors of IPV (Fennema-Notestine et al., 2002; Fonzo et al., 2013). These studies hypothesized that such associations may be related to a maintained hyperactivation of the affective and limbic regions in response to violence from their partners (Moser et al., 2015) or during childhood (Fonzo et al., 2013). While these studies advance our knowledge on the structural brain alterations found in relation to general IPV and psychological trauma, none specifically assess the alterations related to physical violence.
In terms of physical IPV, of growing interest are the brain alterations related to injuries affecting the central nervous system, namely physical impacts to the head or strangulation attempts. Women who have sustained IPV-related hits to the head and strangulation commonly report post-concussive syndrome and alterations in consciousness and neuropsychological functioning, such as lightheadedness, headaches, and amnesia (Kwako et al., 2011). Further, there appears to be a dose–response effect, such that more hits to the head are related to greater impairment in cognitive functioning (Valera & Berenbaum, 2003) and neurological symptoms such as muscle spasms and dizziness (Smith et al., 2001). To date, only two neuroimaging studies have been conducted on brain alterations related to the cumulative effects of brain injury among female survivors (Valera & Kucyi, 2017; Valera et al., 2019). These studies indicate diminished brain connectivity and cognitive functioning related to TBI (Valera & Kucyi, 2017). In terms of structural connectivity, an association was found between TBI severity and fractional anisotropy in the white matter (Valera et al., 2019). In these studies, the association could not be explained by severity of violence, childhood trauma, mental health problems or substance use, highlighting the impact of cumulative IPV-related TBI on the brain. While these studies did not analyze the specific relationship between brain alterations and strangulation, they controlled the effect of strangulation in regions associated with TBI (Valera & Kucyi, 2017; Valera et al., 2019). These findings demonstrated that structural alterations in white matter lost statistical significance after covarying the effect of strangulation (Valera et al., 2019), indicating an important relationship between IPV-related TBI and the possible effect of anoxia or hypoxia on neural mechanisms in female victims and survivors. Due to the fact that strangulation may result in psychological consequences in addition to anoxia or hypoxia, it is crucial to determine the specific impact of each of these variables (Kwako et al., 2011).
As noted in these studies, the focus has typically been exclusively on PTSD or the cumulative effect of TBI caused by hits to the head. Nonetheless, it is likely that there is a complex interplay of factors affecting the brain that have not yet been explored in the literature. Specifically, we do not know if the brain alterations resulting from TBI due to hits to the head are different from those caused by hypoxia or anoxia from strangulation attempts. Also of note is that severe and/or mild TBI was either considered an exclusion criterion or was not included in the analyses of brain morphometry, making it difficult to ascertain whether brain alterations were at least in part related to these variables. Further, other common mental health consequences related to IPV have not been studied using neuroimaging techniques in female survivors, namely depression and generalized anxiety. Childhood trauma is yet another understudied factor among this population, despite its high rates among IPV victims (Barrios et al., 2015) and impact on neurodevelopment (Fonzo et al., 2013). Thus, we cannot know how each of these factors (i.e., TBI, anoxia/hypoxia, mental health, lifetime trauma) varies in its effect on the brain.
In addition, to date, structural brain alterations in a diverse sample of female survivors (including women with and without IPV-related TBI) have not been examined using an exploratory design. Thus far, much of the structural research conducted on female survivors have based their hypotheses on other populations that have suffered trauma, focusing on specific regions of interest, such as the hippocampus and limbic system (Flegar et al., 2011; Fonzo et al., 2013). The literature suggests that neuroimaging research conducted on other populations (such as athletes and military personnel) has a limited application to female IPV survivors, considering the majority of athletes are relatively healthy men without comorbid mental health disorders (Kwako et al., 2011). Due the unique characteristics of IPV-related injury and the lack of studies on the underlying structural mechanisms (volume, area, and cortical thickness), an exploratory design is merited.
In addition, a comparison group of women who have not suffered IPV has not always been used as a point of reference for alterations (Fonzo et al., 2013). Of the structural neuroimaging studies to include a comparison group, it is not clear whether all participants in this group were non-victims. Due to the impossibility of conducting a longitudinal design to study the cause and effect of IPV-related trauma, it is helpful to include a non-victim comparison group as a point of reference. Finally, the majority of neuroimaging research on IPV has been carried out in the United States and other international populations received less attention despite cultural differences in IPV (White & Satyen, 2015) and neural functioning (Han & Ma, 2014). As such, expanding research beyond these confines to other diverse populations may improve generalizability of results.
Taking these factors into account, the objectives of the present study seeks are twofold. First, the principal aim is to assess the possible structural brain differences between a Spanish sample of female survivors of IPV (including women who had and who had not acquired at least one possible IPV-related TBI) and non-victims using a whole-brain approach. Second, in the case that differences are found between groups, this study aims to assess the relationship between brain structure (i.e., volume, area, and cortical thickness) and the previously studied variables (i.e., PTSD, TBI, strangulation, severity of violence, and childhood trauma). As a part of the second objective, this study will expand on these findings, including additional variables that are related to consequences of IPV but that have not been considered in neuroimaging studies, specifically depression (Hebenstreit et al., 2014) and generalized anxiety (Lacey et al., 2015).
Drawing on the relevant literature in structural alterations in female survivors of IPV, we hypothesize that between group differences will be found in the supratentorial cranial vaults, as well as in the frontal and occipital gray matter (Fennema-Notestine et al., 2002). Further, we hypothesize that these differences will be related to severity of violence, adverse childhood experiences (Fonzo et al., 2013), TBI (Valera et al., 2019), strangulation attempts, generalized anxiety, depression, PTSD, and adverse childhood experiences.
Methods
Participants
The sample size was established based on the study by Sui et al. (2010), which shares in common the exploratory analysis of morphometry. Using their voxel t-value of 3.85, we calculated the power, setting our alpha at .05 and power at 80%. These calculations proposed a sample size of 30 for each group. Of 143 women who demonstrated interest in participating and were screened, 27 women who had not suffered IPV with an age range between 18 and 62 (M = 40.03, SD = 13.26) and 28 female survivors of IPV whose ages ranged between 21 and 62 (M = 41.53, SD = 11.61) were included (please see Figure 1. for details on inclusion/exclusion process). Female survivors were contacted through various information centers for women (that pertain to the Andalusian Women’s Institute), nongovernmental organizations for women throughout Granada Province (Spain), and through word of mouth. Non-victims were recruited via bulletins and announcements posted through Granada (Spain) province in public establishments such as community centers and employment offices. Due to the fact that we planned to include both women who had and had not suffered possible IPV-related TBI, we followed the retrospective study design proposed by Valera and Kucyi (2017) for those who had acquired at least one IPV-related TBI. This design considers the reality that recruiting women through emergency centers or medical records would be misleading due to the fact that the majority of women who have suffered an IPV-related TBI do not seek health services (Banks, 2007; Valera & Kucyi, 2017). Thus, limiting recruitment to medical centers would therefore lead to an unrepresentative sample of female victims and survivors (Campbell et al., 2018). Furthermore, even in the case of seeking medical care, it is likely that pertinent information to IPV-related TBI was not gathered (Haag et al., 2019; Ruff et al., 2009).

Note. IPV-S = IPV survivors; NV = Non-victims; Neurological illness = Ictus, brain tumor, non IPV-related TBI, age-related neuropsychological decline.
In terms of group assignment, all women who wished to collaborate completed the Composite Abuse Scale—Short Form (CAS-SF; Ford-Gilboe, 2015) to measure the possibility of having suffered physical (including strangulation), psychological and/or sexual violence by one’s partner. Due to the high prevalence of IPV in the general population (World Health Organization, 2013) and the tendency to underreport (Goldin et al., 2016; Murray et al., 2016; Zieman et al., 2017), women who identified as non-victims were also asked to complete the CAS-SF. The CAS-SF, which measures violence in the past year, was amplified to include IPV throughout the entire lifespan. Due to the fact that there was no Spanish-version of the CAS-SF available, we followed standardized protocol for measure adaptation and translation as recommended by the International Test Commission guidelines (International Test Commission, 2018). Participants who suffered any type of physical or sexual violence (such as hits or any type of severe violence that could result in sequelae) were removed from the non-victim group. Potential non-victim recruits that reported any instance of psychological violence with a frequency greater than “sometimes” were also excluded. Finally, any potential non-victim that reported having suffered an episode of psychological violence “once” (one point) or “sometimes” (two points) in the past five years, with a total score greater than five was removed from the comparison group. For example, if a participant had experienced five episodes of psychological violence with a frequency of one time for each over five years ago, she was not excluded from the comparison group. However, if she had experienced these episodes in the past five years, she was removed from the comparison group.
Inclusion criteria required that participants were at least 18 years of age, and in the case of not being a native Spanish-speaker, that she be able to understand and speak proficient Spanish in order to follow and understand all instructions. The National Migration Statistics for Spain report that in 2019, 10.49% of the population in Granada was foreign (INE, 2019). Reflecting this number, 10.9% of the 55 women included in our study are foreign born (n = 6). Foreign participants, who were familiar with the Spanish educational system, were asked to indicate their level of education in terms of the Spanish equivalent in order to ensure more accurate comparisons between groups.
Among exclusion criteria, women were assessed prior to participation using a screening questionnaire for (a) neurological illness (such as Epilepsy or Parkinson’s) and age-related cognitive deterioration in participants over the age of 50, as determined by a score below 27 on the Mini Mental State Examination (MMSE; Lobo & Ezquerra, 1979), (b) non IPV-related TBI, defined as a loss of consciousness for over 30 minutes or post-traumatic amnesia for over 24 hours with post-concussive symptoms or cognitive sequelae, (c) recent or habitual consumption of illegal psychoactive substances, (d) non-proficiency in Spanish, (e) claustrophobia, (f) age inferior to 18 or superior to 62, and (g) presence of internal metallic objects (either dental or an intrauterine device) that could be incompatible with magnetic resonance equipment. In terms of alcohol use among IPV survivors, only cases of alcohol abuse (and not general alcohol consumption) were excluded due to the fact that female survivors may self-medicate for symptomology caused by the abuse (WHO, 2017). On the other hand, non-victim participants reporting excessive alcohol consumption were excluded, as determined by an AUDIT-C score of 7 or higher (Bradley et al., 2003; Bush et al., 1998). Finally, it is relevant to mention that female survivors suffering from certain immunological disorders, such as fibromyalgia, were not excluded due to its high prevalence in this population (Chandan et al., 2019), and its relation to TBI and psychological trauma (Afari et al., 2014; Grandhi et al., 2017).
Prior to the imaging session, all participants were informed about the study protocol and associated risks, both orally and in writing. All participants were informed about the anonymity and confidentiality standards, and they signed an informed consent document regarding their participation in the study. Participants received 30 euros in compensation for their collaboration. This study was approved by the Ethics Committee at the University of Granada (Spain) (789/CEIH/2019).
Sociodemographic and health-related information on age, education level, origin and place of residency, daily activities, civil status, severity of intimate partner violence, adverse childhood experiences, TBI (due to IPV or other causes), and mental health (generalized anxiety, depression, and PTSD) are displayed in Table 1.
Sociodemographic and Clinical Characteristics of Non-victims and IPV.

Note. ACE = Adverse Childhood Experiences, CAS-SF = Composite Abuse Score, GAD-7 = Generalized Anxiety Disorder, IPV TBI = possible traumatic brain injury caused by intimate partner, PCL-5 = PTSD checklist for DSM-5, PHQ-9 = Patient Health Questionnaire Depression Subscale, Residency = number of inhabitants in place of residency, SD = standard deviation, Strang = strangulation, TBI other = non-IPV related traumatic brain injury.
Material
Possible TBI and strangulation.
Possible TBI was measured using the Brain Injury Severity Assessment (BISA) semi-structured interview developed by Valera and Berenbaum (1997), which considers the definition for mild TBI provided by the American Committee for Mild Traumatic Brain Injury (Committee on Mild Traumatic Brain Injury, 1993). While the criteria for severe TBI is fairly straightforward (i.e., unconsciousness superseding 30 minutes or post-traumatic amnesia for over 24 hours after the event), the definition for mild TBI is less evident. According to the American Committee for Mild Traumatic Brain Injury (Special Interest Group of the American Congress of Rehabilitation Medicine), it is defined as:
Any loss of consciousness; any loss of memory for events immediately before or after the accident; any alteration in mental state at the time of the accident (e.g., feeling dazed, disoriented, or confused); focal neurologic deficit(s) that may or may not be transient. But where the severity of the injury does not exceed the following: loss of consciousness of approximately 30 min or less; after 30 min an initial Glasgow Come Scale of 13–15, and post-traumatic amnesia not greater than 24 hr. (Ruff et al., 2009).
Due to the retrospective design of the BISA interview (Valera & Berenbaum, 1997), usually taking place weeks or months following the traumatic event, the Glasgow score was not assessed. Nonetheless, all other alterations in consciousness outlined by this definition were assessed in the interview in relation to violence caused by the intimate partner (e.g., strangulation attempts, mild and severe TBI following caused by hits to the head or face). Alterations in consciousness were referred to as symptoms that include feeling dizzy, stunned, disoriented, seeing “stars or sports”, losing consciousness or fainting, or having difficulty remembering things that happened right before or after the violent event. For example, the first question asks, “After anything that your partner has ever done to you, have you ever lost consciousness or blacked out?” If the participant reported having, in this case lost consciousness or blacked out, or having experienced any one of the aforementioned symptoms in relation to something her partner did to her, the interviewer would ask follow-up questions related to the cause (e.g., if she was hit with a fist, object, shaken, or strangled). Participants were also asked to estimate the time of the first and most recent incident, and the total number of incidences.
Severity of IPV.
CAS-SF (Hegarty et al., 2012) composed of 15 items related to the severity and frequency of violence was administered. While the original CAS-SF assesses severity of violence in the past 12 months, we assessed lifetime trauma in order to include the entire history of abuse. The CAS-SF includes specific items for psychological, physical, and sexual violence, measuring the frequency of each on a scale of 0 to 5 (0 = never, 1 = once, 2 = a few times, 3 = monthly, 4 = weekly, 5 = daily/almost). The total score ranges from 0 to 75 and is calculated by adding the frequencies of all items and multiplying the sum by 15. The authors recommend using the total score instead of the subscale total scores for each type of abuse. The scale demonstrates an internal consistency of .942 (Ford-Gilboe, 2015).
Adverse childhood events.
All participants filled out the Adverse Childhood Experiences Questionnaire (ACE; Felitti et al., 2019). The ACE Questionnaire consists of 10 questions related to traumatic events in childhood, including items related to childhood about, negligence, and family problems. The scale has a total score ranging between 0 and 10, and demonstrates a reliability alpha of .61 for family problems and .80 for sexual abuse and total score (Ford et al., 2014).
PTSD.
The PTSD Checklist for DSM-5 (PCL-5; Blevins et al., 2015; Bovin et al., 2016; Wortmann et al., 2016), a 20-item questionnaire, was administered to measure PTSD symptomology in accordance with the DSM-5 diagnostic criteria: intrusion, avoidance, cognitive alterations, mood, and hypervigilance. Survivors were prompted to respond to how they experience symptoms in relation to the violence they have suffered from their intimate partner. Non-victims were prompted to respond to symptoms in relation to any event that has been traumatic or stressful in their lives. Symptoms are scored on a Likert scale of 0 to 5 (0 = not at all, 1 = a little bit, 2 = moderately, 3 = quite a bit, 4 = extremely). The total score for the severity of symptoms ranges from 0 to 80 and is calculated by summing the frequency of all 20 items. In veterans, the PCL-5 has demonstrated a high internal consistency (α = .96), test–retest reliability (r = .84), and convergent and discriminative validity (Bovin et al., 2016). Further the PCL-5’s Chronbach’s alpha has demonstrated adequate psychometric properties in female survivors of IPV (α = .93; media interitem r = .44) (Krause et al., 2007)
Generalized anxiety.
The Generalized Anxiety Disorder Questionnaire (GAD-7; Spitzer et al., 2006), a seven-item scale used to detect generalized anxiety, was administered. The GAD-7 measures the frequency with which participants feel bothered by anxiety symptoms during that last two weeks on a Likert scale of 0 to 3 (0 = not at all, 1 = several days, 2 = more than half of the days, 3 = nearly every day). The total score ranges from 0 to 21, and is calculated by adding the frequency of the seven items. In the general population, the GAD-7 has demonstrated adequate psychometric properties in the Spanish population with a high sensitivity (88.8%) and specificity (94.4%) (Garcia-Campayo et al., 2010). In female survivors, it has also demonstrated high internal consistency (94%) (Do, Weiss, & Pollack, 2013)
Depression.
Depressive symptoms were measured using the Patient Health Questionnaire Depression Subscale (PHQ-9; Kroenke & Spitzer, 2002), a nine-item questionnaire that assesses the DSM-IV’s criteria for a provisional diagnosis of major depression. Items are measured on a Likert scale of 0 to 3 (0 = not at all, 1 = several days, 2 = more than half the days, 3 = nearly every day). The total score, ranging from 0 to 27, is calculated by summing the frequency of all nine items. The measure has demonstrated a sensitivity of 84% and a specificity of 72% in a sample of 3,000 primary care patients and 3,000 obstetric and gynecological patients (Kroenke et al., 2001).
Procedure
The present study is part of a larger project (Project Believe: www.projectbelieve.info), which measures neuropsychological and mental health alterations over the course of various sessions. First, interviews and questionnaires about mental health status, TBI, and IPV severity took place in a quiet and comfortable office before the neuroimaging session. Following the questionnaires, image acquisition was carried out in the Center for Research on Mind, Brain, and Behavior (CIMCYC) at the University of Granada.
Image Acquisition
Magnetic resonance images were acquired on a Siemens Prisma 3T Tesla Magnetom scanner (Siemens Medical Solutions, Erlangen, Germany) equipped with a 32-channel receive-only head coil. A sagittal high resolution three-dimensional T1-weighted image was obtained. The acquisition parameters included: Repetition time (TR), 2300ms; Echo time (TE), 3.1ms; flip angle, 9 º; Field of view (FOV), 256 × 256 mm; number of slices, 208; voxel size, 0.8 × 0.8 × 0.8 mm. Data were processed using with the FreeSurfer software version 6.0 (http://surfer.nmr.mgh.harvard.edu) on the “Alhambra” cluster at the University of Granada, Spain. Images were processed following the standard pipeline “recon-all” that has been previously validated to segment and measure brain substructure volumes, cortical thickness, and surface area (Dale et al., 1999; Fischl et al., 1999; Fischl & Dale, 2000). Before preprocessing, all images were visually inspected for acquisition artifacts and quality.
The processing steps were as follows: (a) skull-stripping, (b) automated Talairach registration, (c) gray/white matter segmentation, (d) construction of a model gray–white matter boundary, and (e) cerebral cortex parcellation into regions of interest based on gyral and sulcal structures from the Destrieux atlas (Destrieux et al., 2010).
Design and Data Analysis
Prior to conducting analyses, we verified that there were no differences between groups in the estimated intracranial volume. Outlier analyses were conducted using the R studio software for the volume, area, and thickness all of the brain regions.
Using the statistical program Statistical Analyses for the Social Sciences (SPSS 25), we carried out three student’s t-tests to compare different sociodemographic and clinical variables between groups (i.e., age, education level, residency, alcohol consumption). According to our whole-brain approach, we explored the differences between groups in each of the brain parcellations obtained with the Freesurfer software that divides the whole brain in 160 regions. 160 students’ t-tests were conducted to compare volume, area, and cortical thickness between female survivors and non-victims. A more detailed description of the parcels of the Destrieux atlas can be found elsewhere (Destrieux et al., 2010).
Finally, partial correlations were carried out between each of the variables of interest (severity of violence, adverse childhood experiences, generalized anxiety, depression, PTSD, IPV-related TBI, TBI by other cause) and all brain regions in which between-group differences in volume, area, and cortical thickness were found. This was done in order to study the relationship between each variable and brain region in isolation by controlling for the potential effect of the other variables. For example, to assess the relationship between PTSD and a brain region, all other variables of interest (i.e., severity of violence, adverse childhood experiences, generalized anxiety, depression, IPV-related TBI, TBI by other cause) were included as covariates. Furthermore, the following variables were included as covariates for all partial correlations: age, education, alcohol consumption, and non-IPV related TBI.
Due to the exploratory nature of this study, the number of analyses was not restricted. The alpha level was set at p < .05 for all analyses with the exception of the exploratory t-tests, where the alpha was set at p < .06 in order to examine any potential trends.
Results
Sociodemographic Differences between Survivors and Non-victims
There were no differences in age (t [53] = .446, p = .657), education level X2 (1, N = 55) = 1.467, p = .226), nor alcohol consumption (t [53] = –.892, p = .376) between groups. There were significant differences between groups on the ACE, such that survivors of IPV had been exposed to more childhood adverse experiences (t [53] = 2.337, p = .023). Survivors also reported a greater number of non-IPV related TBI, X2 (1.55) = 4.61, p = .032).
Mental Health Differences between Groups and Acquired Brain Injury
In terms of mental health, there were between-group differences in generalized anxiety (t [53] = 6.667, p = .000), depression (t [53] = 4.77, p = .000), and PTSD (t [53] = 7.31, p = .000). With regard to possible IPV-related TBI, 4 of the 28 IPV survivors reported symptoms compatible with at least one severe TBI (defined as a loss of consciousness greater than 30 minutes or post-traumatic amnesia for over 24 hours). Of the four women who had acquired a possible IPV-related TBI, one had suffered one TBI, while the other three women had suffered two. A total of 16 of the 28 survivors has acquired at least one mild IPV-related TBI (mTBI): six women having acquired one mTBI, three women two mTBI, one woman three mTBI, two women four mTBI, one woman 10 mTBI, and three women over 16. Of the IPV survivors, 18 (64.28%) had suffered a strangulation attempt by their partners.
Brain Structure Differences between Female Survivors and Non-victims
Independent samples t-tests were conducted for the 160 regions into which Freesurfer segmented the whole brain to test for differences in volume, area, and cortical thickness between groups. No differences were found in the global volume of the different lobes, the total volume of gray matter, the supratentorial cranial vault volume, and the total estimated intracranial volume. Statistically significant differences were found in volume for 9 brain regions, 11 regions for area, and 4regions for cortical thickness (see Table 2). For more detailed information, please refer to Table 2 and Figures 2, 3, and 4.
Brain Regions with Between–Group Differences in Volume, Area, and Cortical Thickness.
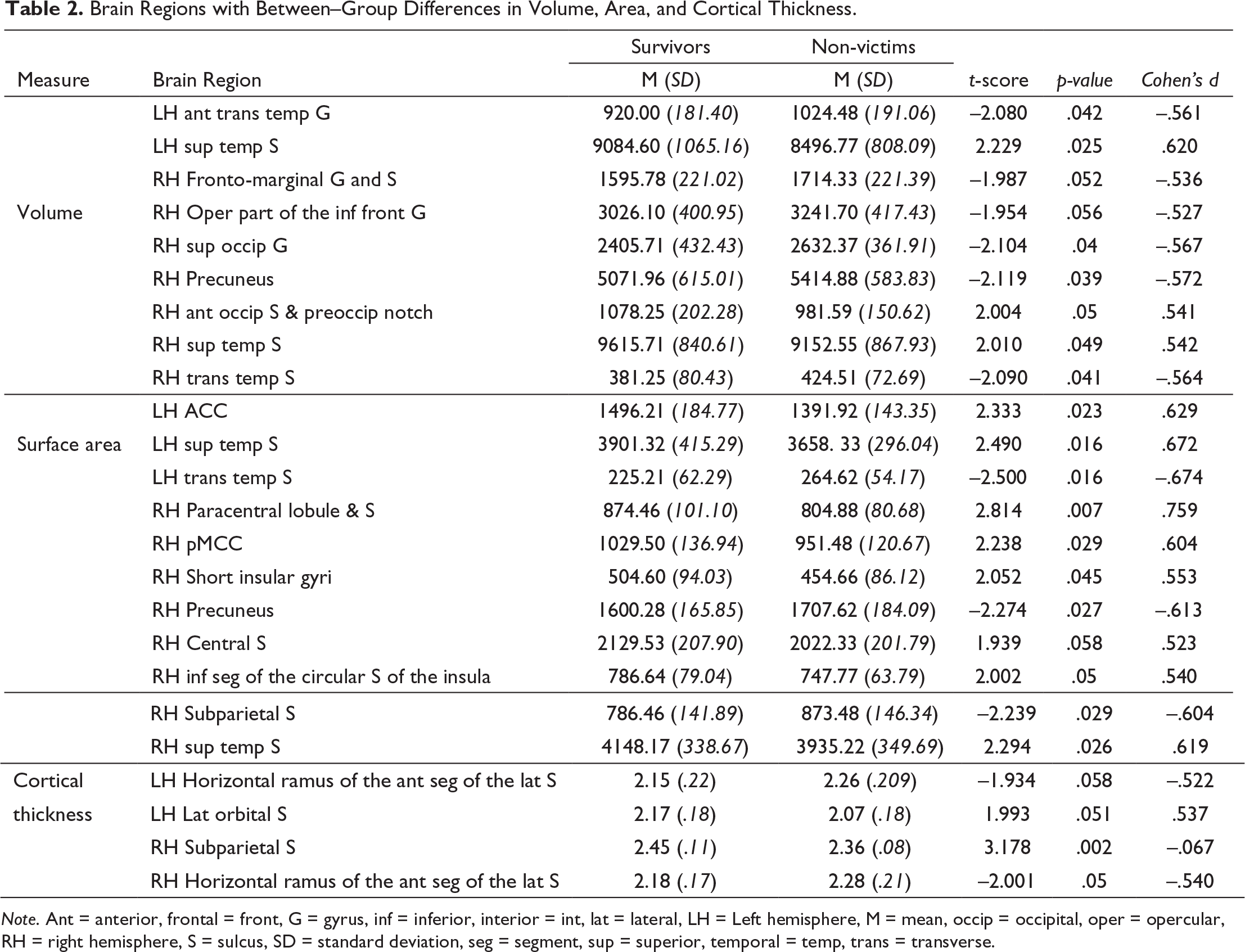
Note. Ant = anterior, frontal = front, G = gyrus, inf = inferior, interior = int, lat = lateral, LH = Left hemisphere, M = mean, occip = occipital, oper = opercular, RH = right hemisphere, S = sulcus, SD = standard deviation, seg = segment, sup = superior, temporal = temp, trans = transverse.
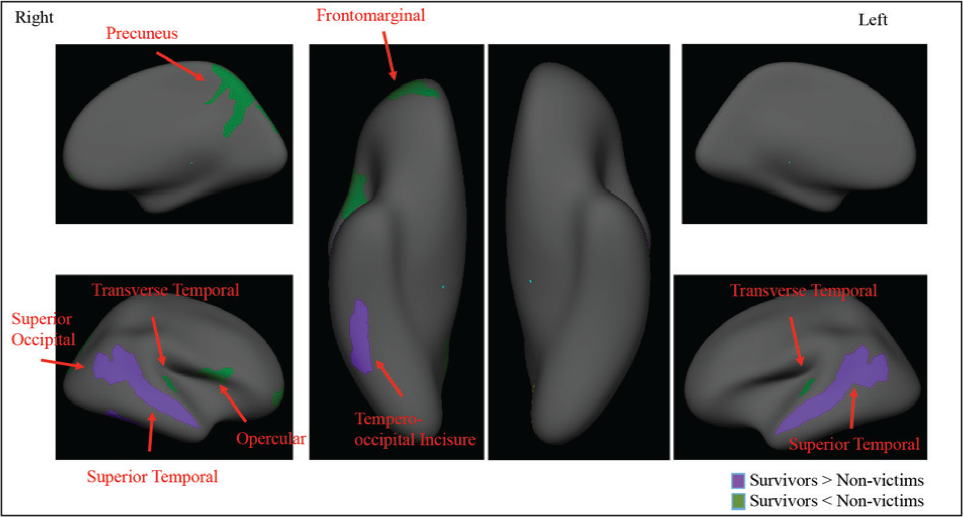
Note. Right= right hemisphere; Left= left hemisphere.
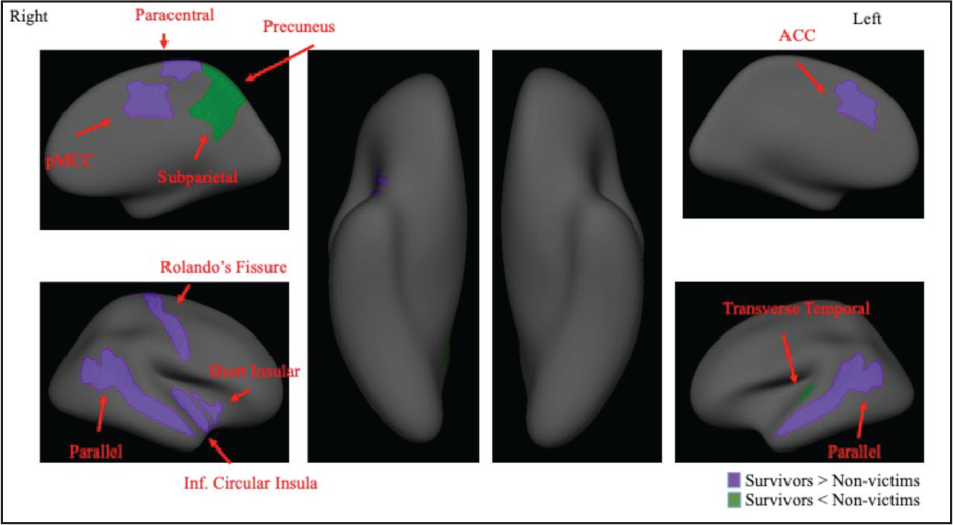
Note. Right= right hemisphere; Left= left hemisphere; pMCC= posterior middle cingulate cortex; Inf.= Inferior; ACC= anterior cingulate cortex.
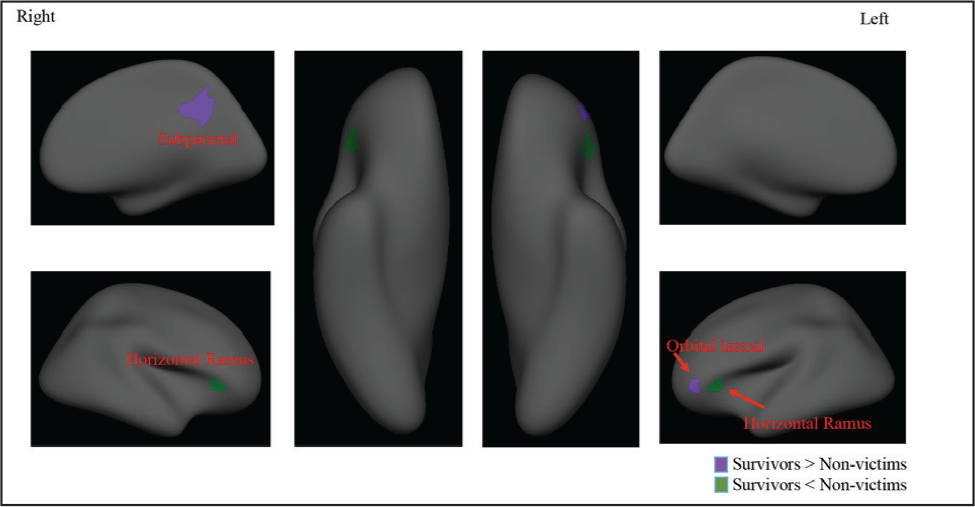
Note. Right= right hemisphere; Left= left hemisphere.
Relationship between Clinical Variables and Brain Regions
First, Spearman (for the dichotomous variables of IPV-related TBI, other TBI, strangulation, and education) and Pearson’s correlations (for continuous variables of age, alcohol consumption, depression, PTSD, generalized anxiety, severity of IPV, adverse childhood experiences) were conducted to study the relationship between the sociodemographic, clinical, and violence variables. Results demonstrate high correlations principally between violence and clinical variables (please see Table 3).
Association between Severity of Trauma, Mental Health Variables, TBI and Strangulation Attempts.
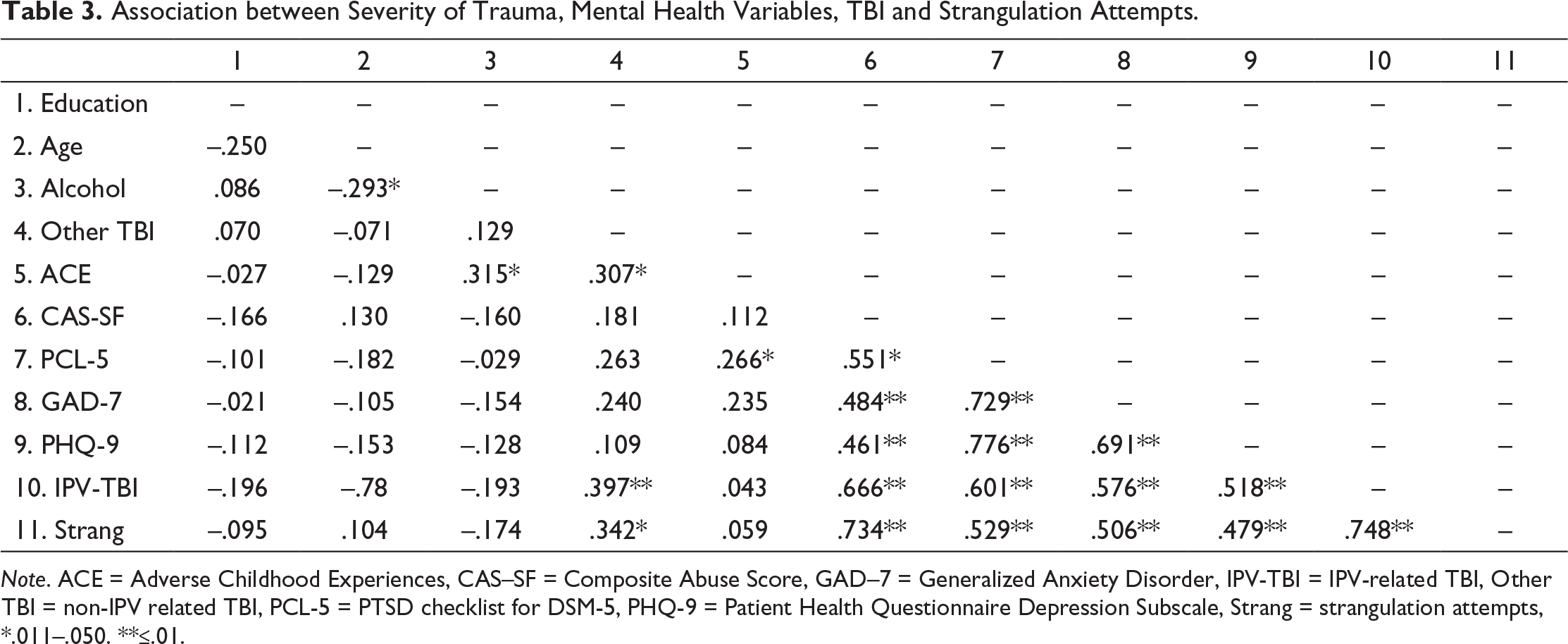
Note. ACE = Adverse Childhood Experiences, CAS–SF = Composite Abuse Score, GAD–7 = Generalized Anxiety Disorder, IPV-TBI = IPV-related TBI, Other TBI = non-IPV related TBI, PCL-5 = PTSD checklist for DSM-5, PHQ-9 = Patient Health Questionnaire Depression Subscale, Strang = strangulation attempts, *.011–.050. **≤.01.
Due to a high correlation between the different clinical variables and the abnormal distribution of the sample, non-parametric partial correlations were conducted to measure the relationship between the variables of interest and brain regions. Despite not finding differences between groups in age, education, non-IPV related mild TBI, and alcohol consumption, these variables were included as covariates in the analyses.
In sum, non-parametric partial correlations were carried out for each of the brain regions that were significantly different in structure between groups (either in volume, area or in cortical thickness) with each of the variables of interest in isolation in order to control for the high correlation between clinical and violence variables (as seen in Table 3): adverse childhood experiences, severity of IPV, depression, PTSD, generalized anxiety, IPV-related TBI, TBI by other cause, and strangulation attempts. For all analyses, the variables of education level, age, alcohol consumption, non-IPV-related TBI were included as covariates. Furthermore, to understand the specific relationship of each variable of interest in relation to the volume, area or thickness of each brain region, all other variables of interest were included as covariates. Different brain regions were positively correlated with IPV severity, TBI, PTSD, and childhood adverse events in terms of volume and surface area, with the last two variables showing significance in the same cortical region (the superior temporal sulcus of the right hemisphere; see Table 4). TBI consistently demonstrated a negative correlation with different brain regions in both surface area and volumetric measures, while strangulation attempts showed a specific negative correlation with cortical thickness in one specific brain region (the horizontal ramus of the anterior segment of the lateral sulcus). No relationship was found between brain regions and generalized anxiety and depression. All r values presented in Table 4 reflect the specific relationship of each variable to the different brain regions.
Partial Correlations between Clinical/Violence Measures with Brain Regions between Female Survivors and Non–victims.

Note. ACE = Adverse Childhood Experiences, ant = anterior, CAS-SF = Composite Abuse Score, G = gyrus, GAD-7 = Generalized Anxiety Disorder, inf = inferior, interior = int, IPV-TBI = IPV-related TBI, lat = lateral, LH = left hemisphere, M = mean, occip = occipital, PCL-5 = PTSD checklist for DSM-5, PHQ-9 = Patient Health Questionnaire Depression Subscale, RH = right hemisphere, S = sulcus, SD = standard deviation, seg = segment, strang = strangulation attempts, sup = superior, temporal = temp, trans = transverse, *.011-.050. **≤.01.
Discussion
Using a whole-brain exploratory analysis, this study found structural differences between female IPV survivors and non-victims in terms of area, volume, and cortical thickness. Furthermore, a morphological analysis demonstrated a relationship between these regions and the different potential causal mechanisms of brain alterations, namely, severity of IPV, childhood adversities, generalized anxiety, depression, PTSD, IPV-related TBI, non-IPV-related TBI, and strangulation attempts. All variables, with the exception of depression and generalized anxiety, were associated with at least one of the structural measures (area, volume, or thickness) in distinct brain regions.
In line with our first hypothesis, structural brain differences were found between female survivors and non-victims of IPV, principally in volume. Generally, regions were greater among female non-victims than IPV survivors, although the direction of this difference depended largely on the type of measure (i.e., volumetric, surface area, or thickness) and brain region. Critically, these differences remained even after controlling for alcohol and substance use, age, education, and non-IPV related mild TBI. Similar to previous structural studies comparing IPV survivors and non-victims, we did not find between-group differences in the hippocampus (Flegar et al., 2011; Fonzo et al., 2013, Fennema-Notestine et al., 2002; Roos et al., 2017). On the other hand, our findings do not coincide with the only two structural studies to have used an exploratory design. In Roos et al. (2017), no structural differences were found, either in volume or in thickness (Roos et al., 2017). In the study conducted by Fennema-Notestine et al. (2002), differences were only found in the supratentorial region, frontal lobes, and occipital lobes, regions that were not significantly different among our sample. It is possible that the significant findings of the present study differ due to the fact that Roos et al. (2017) excluded for TBI, and did not assess for lifetime trauma in the comparison group. On the other hand, our findings may differ from those of Fennema-Notestine et al. (2002) due to the fact that the number of women to have suffered mild TBI in their sample was not reported. Further, Fennema-Notestine et al. (2002) applied different methods for establishing structural differences, which may also in part explain these discrepancies.
To test our second hypothesis, we studied the association between different potential causal mechanisms for the structural brain differences between groups. We first examined the association between structural differences and PTSD, considering the majority of previous neuroimaging studies with IPV survivors have centered on alterations related to PTSD (Aupperle et al., 2016; Fonzo et al., 2010; Moser et al., 2015; Neumeister et al., 2017) and the high prevalence of PTSD among this population (Lagdon et al., 2014). To study this relationship, without limiting analyses to the specific regions commonly assessed in these studies, an exploratory analysis was employed to examine whether the brain regions found to be structurally different were related to PTSD severity. In line with previous research, we found alterations related to PTSD in the occipital (Fennema-Notestine et al., 2002; Neumeister et al., 2018; Strigo et al., 2010) and temporal regions (Aupperle et al., 2012; Aupperle et al., 2013; Fennema-Notestine et al., 2002; Fonzo et al., 2013; Strigo et al., 2010). Some authors propose that the occipital (Neumeister et al., 2018) and temporal (Aupperle et al., 2012; Aupperle et al., 2013; Fonzo et al., 2010, 2013) regions could be related to abnormal processing of negative or fear-producing stimuli. This theory may also back a similar model proposed by other authors, which hypothesized that the temporo-occipital network is involved in the PTSD symptoms of hypervigilance and intrusion of trauma-related memories (Weston, 2014), and controlled processing, such as flashbacks (Whalley et al., 2013).
On the other hand, alterations in the temporal region have also been related to childhood abuse in female survivors of IPV (Fonzo et al., 2013). Our findings coincide with previous studies as a relationship between adverse childhood experiences was associated with the temporal regions in which structural differences were found between female survivors and non-victims. These findings are particularly relevant due to the fact that childhood abuse and traumatic experiences are highly prevalent among female victims of IPV (Cimino et al., 2019) and due to the fact that experiencing violence in these formative years can produce neurodevelopmental alterations (Puetz et al., 2017). In contrast to previous studies, we have studied the relationship between brain alterations and mental health problems beyond the stress caused by childhood and adult traumatic experiences, namely depression and generalized anxiety. In our sample, these variables did not explain the structural differences found between female survivors and non-victims. These non-significant findings may be due to the fact that we did not employ strict diagnostic criteria. A more precise and comprehensive analyses may potentially reveal an association between brain alterations and other mental health disorders. With this in mind, we consider it necessary to continue researching these variables due to their high prevalence among female victims and survivors of IPV (Chandan et al., 2019).
Similar to other studies in this field, our results showed an association between TBI and brain alterations in limbic (Valera & Kucyi, 2017; Valera et al., 2019) and parietal regions (Valera & Kucyi, 2017), even after controlling for the effect of confounding variables such as the severity of violence, adverse childhood events, mental health problems, substance and alcohol use, and non-IPV related TBIs. Despite having been hypothesized that brain alterations may be related to both TBI and strangulation attempts, they have never been studied separately to clarify whether brain alterations may differ by mechanism. Here, we found a trend for a relationship between strangulation attempts and one of the brain regions, namely the horizontal ramus of the anterior segment of the lateral sulcus. This difference may indicate that the sequelae resulting from anoxia or hypoxia are specific and unique to those found in TBI due to hits to the head. While the specific brain alterations related to strangulation have not yet been studied among IPV survivors, this hypothesis is reflected in the work of Valera et al. (2019), where the association between TBI and structural alterations disappear when controlling for the effect of strangulation. Although these findings do not demonstrate a direct influence, they indicate that strangulation may potentially explain at least part of the variance in brain alterations related to IPV. Clearly more research is needed to understand the lasting effects and alterations provoked by these different mechanisms of violence.
To the best of our knowledge, this study represents the first attempt at studying structural differences comparing non-victims to female survivors (both have and have not sustained IPV-related TBI) using a whole-brain methodology, instead of limiting analyses to the regions that are typically assessed in trauma patients, such as the hippocampus (Flegar et al., 2011). Furthermore, this study contributes to the literature due to its strict protocol of controlling for a comprehensive list of factors related to brain alterations in the general population and in female survivors of IPV, such as age, education level, substance and alcohol use, non-IPV related TBI, IPV-related TBI, strangulation attempts, adverse childhood events, IPV severity, depression, PTSD, and generalized anxiety. Despite these contributions, this study has important limitations that limit the generalizability of findings. Of notable importance, due to this study’s exploratory design, we did not correct for the number of analyses conducted. As such, it is possible that some of the significant findings may not appear in studies using larger samples. We greatly encourage future research to re-examine the brain areas found to be different between groups and to analyze the same variables of interest with a larger sample size. An additional limitation is that we did not assess diagnostic criteria for mental health illnesses due to the fact that we were primarily interested in studying the severity of symptoms on a continuum. Nonetheless, using diagnostic criteria may help determine whether there are brain alterations related to mental health sequelae such as generalized anxiety, depression, PTSD, complex PTSD. Further, the present study did not include specific measures for TBI and strangulation, such as recency or a differentiation between severe and mild TBI. Specifically, to measure strangulation attempts, we employed the CAS-SF questionnaire, which only gathers information on the presence and frequency. This measure does not include details on alterations in consciousness caused by strangulation attempts, a critical factor to determining whether the violent act may have led to possible hypoxic or ischemic injury. It would be important for future studies to include information about the different possible causal mechanisms to better understand the specific types impairment resulting from TBI or hypoxia/anoxia caused by strangulation attempts, as well as the effect of having suffered repetitive trauma over an extended period of time. This may also help us to determine the trajectory impairment, such as what factors influence the development of sequelae or difficulties in rehabilitation. Finally, it would be interesting to analyze the relationship between cognitive functioning and brain alterations, as has been done in previous studies (Fennema-Notestine et al., 2002; Valera & Kucyi, 2017). This would allow for a richer understanding of the functional consequences of alterations found in female survivors.
In sum, following a whole-brain methodology, this study has found structural brain differences in area, volume, and cortical thickness between female survivors of IPV and non-victims in the lateral sulcus, temporal, frontal, occipital, parietal, and limbic regions. Further, these brain regions were related to adverse childhood experiences, severity of IPV, PTSD, IPV-related TBI, and strangulation attempts. This study contributes a deeper understanding of the factors related to brain alterations in female survivors of IPV and suggests that there is a complex interplay of variables related to IPV that may be relevant for front-line workers and professionals working with this population. Due to our findings of specific and differentiated brain alterations related to possible TBI and strangulation, and clear evidence in the literature of functional sequelae related to both, it is imperative that first-response professionals run at least a screening to know whether the victim has acquired a possible TBI or hypoxic and/or ischemic damage from strangulation attempts. While more information is needed to understand the evolution of impairment caused by these mechanisms, earlier detection may lead to improved care and recovery. Further, our findings point to the importance of assessing overall trauma. Unfortunately, many IPV survivors have also been victims of childhood abuse or adverse experiences in early development. These accumulated traumatic experiences may result in long-term brain alterations that are pertinent to rehabilitation and therapy. Our findings highlight the importance of a holistic approach in supporting victims and survivors, considering not only physical violence but also lifetime adverse events during development as well as psychological trauma.
Footnotes
Acknowledgments
We would like to show our deepest gratitude to all of the women who participated in the study and to the professionals at the Women's Associations (Centro de Información de la Mujer) in the town halls of Motril, Armilla, Albolote, and Maracena, namely Pilar García Fajardo, Carmen Losada Reinoso, María José Gálvez Jiménez, Nuria Pérez, and Maite Sanz Hiraldo. A special thank you to researchers Carmen Fernández Fillol and Álvaro Lozano Ruiz for their help and support in carrying out this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Authors declare no affiliations with or involvement in any organization or entity with financial interest or non-financial interest in the information discussed in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by the I+D+I Operative Program FEDER project of the Andalusian Government in 2018 (B-CTS-493-UGR18). J.C.D. was funded by a predoctoral fellowship of the Ministry of Education and Professional Training in Spain as well as the postdoctoral Puente contract at the University of Granada (Spain). J.V.R was funded by a Grant from the Spanish Ministry of Science, Innovation and Universities (FJCI-2017-33396).