
Abstract
Intimate partner violence (IPV) is widespread. Several risk factors are associated with IPV perpetuation, including alcohol use and educational level. The aggression and violence associated with traumatic brain injury (TBI) suggest that brain trauma may also be a risk factor for IPV. To examine the association between TBI and IPV, the authors conducted a meta-analysis of peer-reviewed published studies reporting the prevalence of TBI in IPV perpetrators. The authors compared the frequency of TBI among IPV perpetuators to estimates of TBI in the general population using a single-sample test of proportions. Six studies containing a total of 222 subjects met inclusion criteria. Fifty-three percent (119) of the IPV perpetuators had a history of TBI, a prevalence significantly higher (p < .0001) than estimates of TBI in the general population. The prevalence of TBI among perpetuators of IPV appears significantly higher than the prevalence of TBI in the general population. To the extent that this association is causal, TBI may be a risk factor for interpersonal violence, although comparatively few source studies, lack of standardized information about TBI severity, and the inability to investigate potential confounding variables necessarily limit this conclusion.
Introduction
Intimate partner violence (IPV) is a considerable social problem (Straus & Gelles, 1986; Tjaden & Thoennes, 2000). Data from the National Violence Against Women Survey indicate that nearly 1.9 million women and 3.2 million men are assaulted each year in the United States, with approximately 64% of the female cases and 16% of the male cases occurring in the context of an intimate relationship (Tjaden & Thoennes, 2000). This totals 1,728,000 cases of IPV each year in the United States alone, of which 1,216,000 are female and 512,000 are male. Because of underreporting of IPV, this figure is likely an underestimate (Felson, Messner, Hoskin, & Deane, 2002). Risk factors associated with being the victim of IPV include young age, low socioeconomic status, use of drugs and/or alcohol, relational conflict, cohabitation, cultural or religious support of domestic violence, history of domestic violence and/or abuse, and involvement in other forms of violence (Abramsky et al., 2011; Ellison, Bartkowski, & Anderson, 1999). Additionally, being a victim of IPV is associated with higher rates of psychiatric symptoms, increased health care usage, and negative long-term health outcomes (McCauley et al., 1995; Plichta, 2004).
Considerable research has investigated risk factors for perpetuating IPV. A meta-analysis of the risk factors for male-perpetuated IPV found that emotional/verbal abuse, forced sex, illicit drug use, an attitude condoning violence, traditional sex-role ideology, anger/hostility, career/life stress, history of partner abuse, alcohol use, depression, and jealousy were positively associated with perpetuating domestic violence, while marital satisfaction, age, education level, employment, and income were protective factors (Stith, Smith, Penn, Ward, & Tritt, 2004). These results have been replicated in meta-analyses and original studies in a variety of contexts (Abramsky et al., 2011; Foran & O’Leary, 2008).
Compared to the research of psychosocial factors associated with IPV, relatively few studies have focused on underlying biological variables associated with perpetuating violence in relational contexts. A recent review by Pinto et al. (2010) suggests that biological factors may play a more prominent role in the perpetuation of IPV than previously thought. In their review, Pinto et al. (2010) found that head injury resulting in neuropsychological deficits, elevated psychophysiological reactivity to stimuli, neurochemical, metabolic, and endocrine abnormalities, and, potentially, genetic variables are implicated in the perpetuation of IPV.
The biological factors associated with IPV are in concordance with findings demonstrating an association between traumatic brain injury (TBI) and aggression and violence, behaviors known to be present in perpetuators of interpersonal violence. For example, TBI is associated with an increase in both physical and verbal aggression (Baguley, Cooper, & Felmingham, 2006; Cole et al., 2008) and with violent and criminal behavior (Brooks, Campsie, Symington, Beattie, & McKinlay, 1986; Sarapata, Herrmann, Johnson, & Aycock, 1998). Dyer, Bell, McCann, and Rauch (2006) found that spouses and close family members of TBI patients reported increased verbal aggression and temper outbursts following the TBI. Similarly, interviews of family members and caretakers of TBI survivors have found that 35% of caregivers reported aggression and disinhibition in regard to anger and significantly increased temper outburst in TBI patients (Hall et al., 1994). Case studies also suggest an association between TBI and aggressive and aberrant sexual behavior (Bezeau, Bogod, & Mateer, 2004). Consequently, TBI has been associated with significant psychological distress for the spouses of TBI victims (Blais & Boisvert, 2005; Linn, Allen, & Willer, 1994).
The association between TBI and aggressive and violent behavior suggest that TBI may be associated with IPV. In this regard, Rosenbaum and Hoge (1989) found that 61% of men evaluated for IPV had a history of severe TBI with a mean age of injury onset at age 16. Likewise, Turkstra, Jones, and Toler (2003) found that 15 of the 20 (75%) convicted IPV perpetuators had a history of TBI.
In that TBI is associated with aggression and that there appears to be high rates of TBI among IPV batterers, we evaluated the hypothesis that the prevalence of TBI pooled across multiple studies would be significantly higher for IPV perpetuators than the estimated prevalence of TBI in the general population.
Method
Source Study Identification and Selection
We used the following search terms to identify articles reporting prevalence rates of TBI in IPV offenders: domestic violence or domestic abuse and TBI, partner violence or partner abuse and TBI, domestic violence or abuse and head injury, domestic violence or abuse and brain, IPV and brain injury, and partner abuse or violence and brain. These terms were used in the electronic search engines PubMed from the National Library of Medicine, PsychINFO, and Google Scholar. We also searched reference sections from identified articles for additional relevant articles. We included any article that reported the prevalence of TBI in a sample of IPV offenders. Because of varying definitions of TBI, we included all articles reporting a significant blow to the head and any article reporting loss of consciousness following a blow to the head. We did not attempt to differentiate between different TBI severities because of disagreement about what constitutes mild, moderate, and severe TBI. We excluded other types of acquired brain damage, such as anoxic brain injury or damage related to stroke, tumor, or other forms of nontraumatic damage.
Prevalence of TBI in the General Population
The prevalence of TBI in the general population is poorly defined (Farrer & Hedges, 2011). To compare the meta-analytically derived prevalence of TBI in IPV offenders to the prevalence of TBI in the general population, we replicated methods we have previously published, wherein we identified epidemiological studies reporting TBI prevalence in the general population to obtain a plausible range of TBI prevalence in the general population (Farrer & Hedges, 2011). Briefly, the reported prevalence of TBI in the general population varies widely. Silver et al. (2001) found a prevalence of TBI in the general population of 8.5%. In contrast, averaging data reported by Templer et al. (1992) of TBI prevalence from two colleges and a school of professional psychology showed a prevalence of TBI in the general population of 25.9%. In a cohort of 1,003 subjects, McKinlay et al. (2008) found that by the age of 25 years, 38.5% of the men and 24.2% of the women had had a TBI. Based on these reported prevalences of TBI in the general population, we estimated that TBI prevalence in the general population could reasonably range from a low of approximately 10% to a high of approximately 38.5%. Based on this estimated range, we selected possible values for TBI prevalence in the general population of 10%, 20%, 25%, and 38.5% to which to compare the pooled value of TBI prevalence we found for perpetuators of IPV.
Statistical Analysis
Because none of the studies meeting inclusion and exclusion criteria reported TBI prevalence in a control group, we were unable to calculate effect sizes for individual source studies from which to obtain a summary effect size. As such, a pooled weighted mean frequency was calculated by summing the total number of subjects from each study who had a history of TBI and then dividing by the number of total subjects summed across all studies. After calculating the pooled frequency, a single-sample test of proportions was used to measure whether the overall prevalence of TBI in IPV offenders was statistically different from the estimated prevalences of TBI in the general population.
Results
Six peer-reviewed articles that met inclusion criteria and recorded subject age, location of the study, total number of subjects in each study, total number of subjects with TBI in each study, percentage of subjects with TBI in each study, whether the subjects were incarcerated, and the method of assessing TBI in each study were identified (Table 1 ). The weighted mean age across all samples was 32.6 years, and all of the subjects were male.
Characteristics of Source Studies
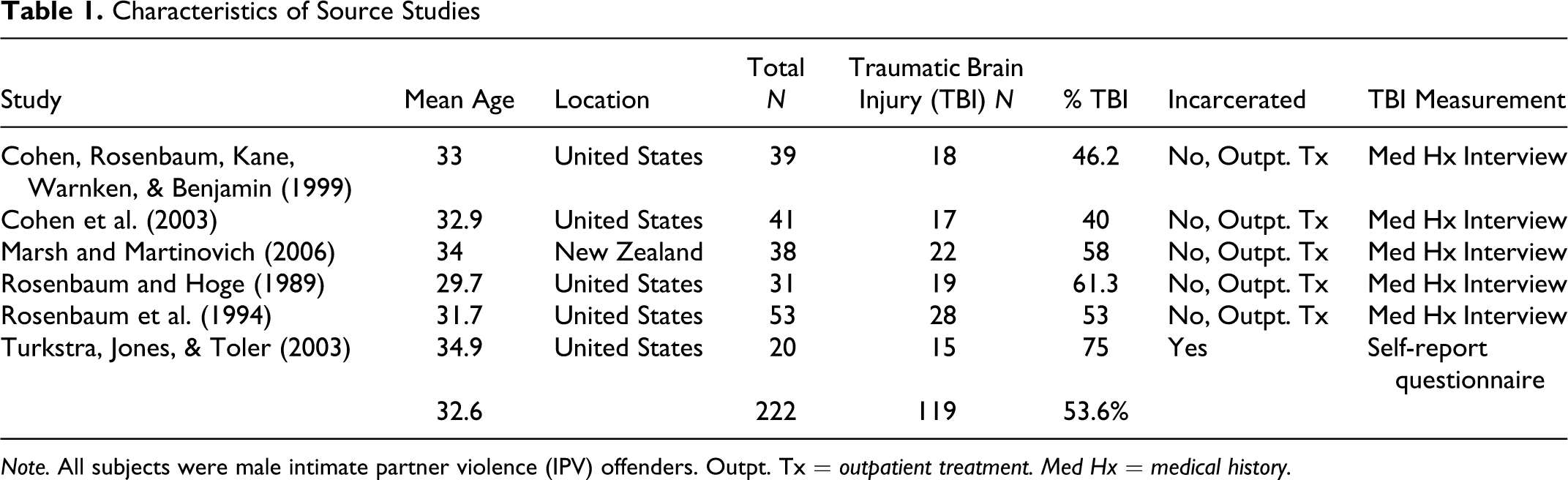
Note. All subjects were male intimate partner violence (IPV) offenders. Outpt. Tx = outpatient treatment. Med Hx = medical history.
Five of the six studies comprised samples from the United States and one from New Zealand. All were from fully developed nations. Of the total combined sample of 222 IPV offenders, 119 had a history of TBI (53.6%). We compared this frequency against estimated frequencies of TBI in the general population of 10%, 20%, 25%, and 38.5% (Table 2 ). The weighted prevalence of 53.6% across the identified studies was significantly higher than all comparison estimates of TBI in the general population (p < .0001).
Z Scores for the Weighted Mean Frequency of Traumatic Brain Injury Among Perpetuators of Intimate Partner Violence Pooled From the Source Studies Compared to Selected Estimated Frequencies of Traumatic Brain Injury in the General Population
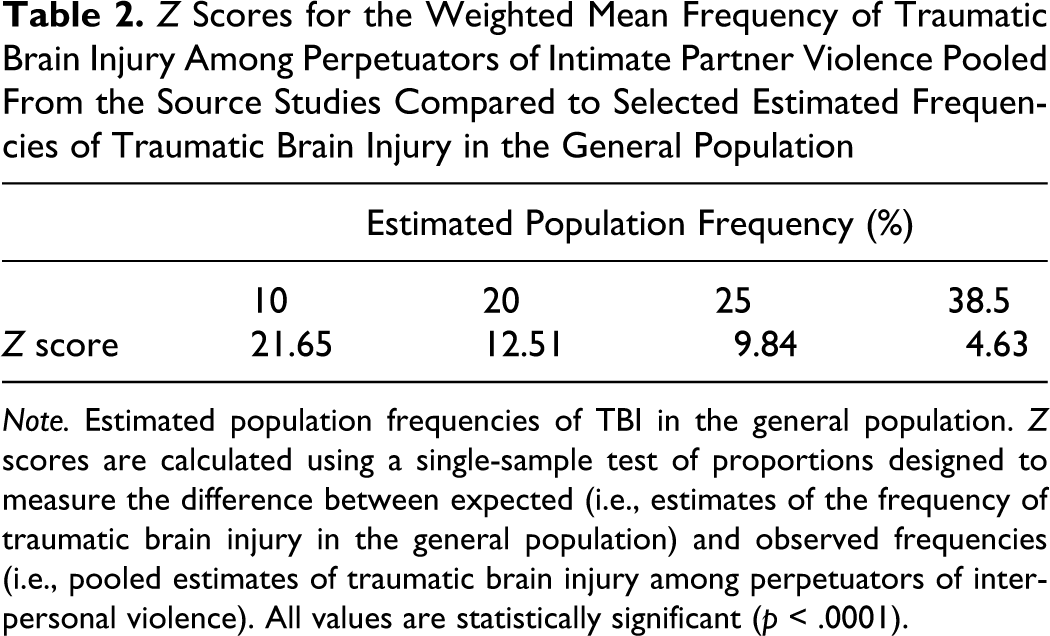
Note. Estimated population frequencies of TBI in the general population. Z scores are calculated using a single-sample test of proportions designed to measure the difference between expected (i.e., estimates of the frequency of traumatic brain injury in the general population) and observed frequencies (i.e., pooled estimates of traumatic brain injury among perpetuators of interpersonal violence). All values are statistically significant (p < .0001).
Discussion
The results of this meta-analysis of the prevalence of TBI in IPV perpetuators from six source studies containing a total of 222 subjects suggest that TBI is significantly more prevalent in the IPV population than estimates of TBI in the general population, even when the prevalence of TBI in IPV is compared to the most extreme general population estimates of TBI. As such, TBI may be associated with IPV. We were particularly interested in comparing the weighted average of TBI prevalence across the six identified studies to the TBI prevalence of 38.5 reported by McKinlay et al. (2008) for several reasons. First, the McKinlay et al. (2008) reported TBI prevalence at the age of 25 years, which was similar to the weighted mean age from our identified studies of 32.6 years. Second, they had a sample of 25-year-old males enabling us to approximately match on sex. Finally, McKinlay et al. (2010) reported the highest prevalence of TBI of the studies we reviewed, which made the comparison with our pooled data more conservative in that the high prevalence of TBI reported by McKinlay et al. (2008) would make it more difficult to find a significant difference between the prevalence of TBI in their sample compared to our pooled data. The average difference in age between our pooled sample and the McKinlay et al. (2008) sample is a limitation to our findings that requires consideration. The average age in our pooled sample was 32.6 years, higher than the age of 25 years in the McKinlay et al. (2008) sample by an average of 7.6 years. It is possible that by the time the men in the McKinlay et al. (2008) sample reach the age of 32.6 years, the percentage of subjects with TBI would have become comparable to the percentage of TBI in our pooled sample, particularly because men have a higher risk of sustaining TBI than women (Bruns & Hauser, 2003). Nonetheless, TBI incidence appears to decline from a high at approximately the age of 20 years to a low in middle age before increasing again in late life (Bruns & Hauser, 2003). The declining incidence of TBI seen after approximately the age of 20 years may result in the men in the McKinlay et al. (2008) not reaching the 53.6% TBI prevalence found from pooling the IPV studies by age 32.6 years. Of course, directly comparable data are required to determine whether the actual prevalence of TBI in the McKinlay et al. (2008) subjects would equal the pooled prevalence of 53.6% in the IPV sample.
An association between TBI and IPV is consistent with previous reports from spouses and partners that a brain-injured partner frequently shows increased aggression and violence after the TBI. For example, McKinlay, Brooks, Bond, Martinage, and Marshall (1981) found that approximately 70% of brain-injured partners had an increase in irritability and aggressive tendencies after the TBI. Likewise, spouses and family members of TBI survivors report an increase in overt verbal and physical aggression following TBI (Grafman et al., 1996). Mauss-Clum and Ryan (1981) surveyed family members of those with neurological damage, wherein family members reported a large increase in irritability and temper outbursts and a decrease in self-control. Approximately one quarter of the spouses of these TBI survivors reported an increase of verbal abuse and threats of physical violence. In addition, the behavioral changes associated with TBI appear both chronic and progressive with TBI survivors remaining at high levels of aggression even 5 years after the injury (Baguley et al., 2006; Brooks et al., 1986). For example, Brooks, Campsie, Symington, Beattie, and McKinlay (1986) found that the number of family members reporting threats of violence from TBI subjects increased from 15% at 1 year postinjury to 54% at 5 years postinjury. Thus, violence and aggression resulting from a TBI may worsen over time instead of improving.
Although aggression is consistently higher in TBI survivors than in controls who have non-TBI injuries (Tateno, Jorge, & Robinson, 2003), other factors may confound the association between TBI and IPV. For example, alcohol use is associated with violence and aggression, and IPV is more common if both or either partner has an alcohol-abuse disorder compared to couples with no alcohol abuse (Abramsky et al., 2011). Further, alcohol use is consistently found to be associated with brain injuries (Kreutzer, Marwitz, & Witol, 1995). In assessing aggressive behavior following TBI, Tateno, Jorge, and Robinson (2003) found that TBI survivors with the highest levels of aggression had significantly higher levels of alcohol abuse compared to the nonaggressive TBI subjects. Within IPV cases, alcohol abuse is a common problem among offenders with a history of TBI (Rosenbaum & Hoge, 1989). Although the association between TBI and alcohol use and between IPV and alcohol use suggests that alcohol use may confound the association between TBI and IPV, it is also plausible that alcohol may be part of a causal pathway between TBI and IPV and not an actual confounder. Even if alcohol does confound the association between TBI and IPV, the association could still be present after adjustment for the confounding relationship. Unfortunately, the source articles in this meta-analysis as a group did not contain enough information to determine how alcohol use might have affected the association between TBI and IPV. However, a study investigating the association between TBI and psychiatric outcome reported that TBI was not associated with alcohol use after correction for demographic and personality factors (Anstey et al., 2004), a finding further suggesting that the association between TBI and IPV may be independent of alcohol abuse. Further research is needed to elucidate the relationship between alcohol use, TBI, and IPV.
Although this is the first meta-analysis of the prevalence of TBI among IPV perpetuators, several limitations in addition to the potential for confounding and age differences between the pooled sample and the subjects in the McKinlay et al. (2008) sample temper the findings reported from this meta-analysis. Because of limited information reported across source studies, we were unable to categorize TBI according to severity and thus unable to determine whether a linear relationship exists between TBI severity and IPV frequency or severity. We identified only six source studies that met inclusion criteria containing a total of only 222 subjects, averaging 37 subjects per source study. Our results are, therefore, susceptible to additional studies and should be viewed as tentative. The comparatively few available source studies preclude meta-regression analyses to explore whether alcohol, socioeconomic standing, or other factors may affect the association between TBI and IPV. Further, the designs of the source studies tended to be cross sectional, limiting the ability of our study to determine causal relationships, even though previous findings indicate that aggression increases after TBI (Grafman et al., 1996; McKinlay et al., 1981). Similarly, it is possible that personality factors associated with IPV are also risk factors for TBI.
Another methodological concern with this meta-analysis is that it is difficult to determine the prevalence of TBI in the general population to which to compare the prevalence of TBI among IPV perpetuators. We used estimates from several studies reporting estimates of TBI in the general population, but these estimates showed considerable interstudy variation and were from small numbers of subjects (Farrer & Hedges, 2011). Although most of the estimates of TBI prevalence in the general population we used were not matched for age, sex, and socioeconomic position to the IPV perpetuators, the longitudinal findings of McKinlay et al. (2008) of a TBI prevalence of 38.5% in males by age 25 make a reasonable comparison for our pooled estimate of TBI prevalence in that all subjects in our meta-analysis were males with an average age of 32.6 years. That is, the sample of McKinlay et al. (2008) was matched for sex and approximately matched for age to our pooled sample and as a high estimate of TBI in the general population makes the comparison between TBI in the general population and the IPV sample more conservative. Although it may not have been matched for socioeconomic and education levels, the prevalence of TBI found among IPV perpetuators (53.6%) was significantly higher than the 38.5% reported by McKinlay et al. (2008).
An additional limitation is that the source studies included in this meta-analysis gathered information about TBI history through either a self-report measure or interview with the participants. People charged with interpersonal violence may overreport events such as TBI that might mitigate their responsibility for the alleged crime, leading to biased estimates of TBI among those charged with IPV. However, obtaining information about TBI history by both self-report and from medical records in an incarcerated sample, Schofield, Butler, Hollis, and D’Este (2011) found a 70% agreement between self-report and medical records and concluded that self-reported TBI among prison populations is reasonably accurate.
In conclusion, the results of this meta-analysis suggest that the prevalence of TBI among perpetuators of IPV is significantly higher than the prevalence of TBI in the general population. To the extent that this association is causal, TBI may be a risk factor for IPV, although comparatively few source studies, lack of standardized information about TBI severity, and inability to investigate potential confounding necessarily limit this conclusion.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research were supported by funds from the Psychology Department at Brigham Young University.