
Abstract
Risks of intimate partner violence (IPV) often are higher among immigrant women, due to dependency, language barriers, deportation fears, cultural beliefs, and limited access to services. In the United States, Asian immigrant women experiencing IPV often are reluctant to disclose abuse. Viewing videos that depict IPV survivors who have successfully obtained help might encourage disclosure. After conducting formative research, we created brief videos in four Asian languages (Korean, Mandarin Chinese, Thai, and Vietnamese) for use in primary care clinic consultation rooms. We then conducted in-depth interviews with 60 Asian immigrant women in California to get their perspectives on how helpful the videos might be in achieving disclosure. Most participants believed the videos would promote disclosure in clinics, although those who had been abused seemed more skeptical. Many had stereotyped views of victims, who they felt needed to be emotive to be credible. Videos should be upbeat, highlighting the positive outcomes of escaping violence and showing clearly each step of the process. Various types of IPV should be described, so that women understand the violence is not exclusively physical. Victims would need reassurance that they will not be arrested, deported, or forced to leave their abusers. Discussing the benefits of escaping violence to children could be influential. Victims also must be convinced that providers are trustworthy, confidential, and want to help. To assist immigrant populations to disclose IPV to a health provider, videos need to be culturally relevant, explain various types of violence, allay fears, and show clear processes and benefits.
Keywords
Introduction
Intimate partner violence (IPV) is defined as any violent or coercive behavior, including physical, sexual, and psychological abuse, perpetrated by someone who is or was involved in an intimate relationship with the victim (CDC, 2015). While studies have found that IPV poses a health risk to women of all racial, ethnic, and social backgrounds, the risks may be greater for some groups, such as immigrant women, due to higher incidences of violence compounded by poverty, stigma, language barriers, deportation fears, and limited access to resources and support networks during times of crisis (Lacey et al., 2013; Sharps & Campbell, 2006). In national surveys in the United States, women of Asian descent report the lowest rates of IPV (CDC, 2011). However, these national surveys may underestimate the true prevalence of IPV among Asian immigrant women because of the following: (a) the data is not disaggregated by U.S.-born and immigrant Asian women; (b) the data is not disaggregated by Asian ethnic groups; and (c) Asian women, particularly immigrants, may find it more difficult than others to reveal IPV over the phone (Bauer et al., 2000; Cho, 2012; Kim & Schmuhl, 2018). When data is collected through community-based surveys using peer interviewers, Asian immigrant women report high rates of lifetime IPV, ranging from 18% to 60% (Raj & Silverman, 2003; Stockman et al., 2015; Yoshioka & Dang, 2000; Yoshihama & Tolman, 2015).
Studies have found that Asian immigrant women who experience IPV are less likely than other immigrant women to report abuse to authorities, and to access services such as women’s shelters, legal services, and health care (Bauer et al., 2000; Cho, 2012; Kim et al. 2018; Lee, 2013; Lee & Hadeed, 2009; Runner et al., 2009; Stockman et al., 2015; Tjaden & Thoennes, 2000). Barriers to recognizing and reporting IPV among Asian immigrant women include limited English fluency, low income, immigration status, isolation and lack of social support, unfamiliarity with laws and social services, and cultural norms (Bauer et al., 2000; Bhuyan et al., 2005; Cho, 2012; Kim et al., 2018; Raj & Silverman, 2003; Runner et al., 2009; Yoshioka et al., 2001).
Health care providers are in a unique position to identify and refer IPV victims (Director & Linden, 2004; Fugate, Landis, Riordan, Naureckas, & Engel, 2005; World Health Organization, 2013). However, due to barriers such as lack of time, provider reluctance to initiate discussions on IPV, lack of provider training and education on IPV, or language or other cultural barriers, women experiencing IPV may not be identified within the healthcare setting (Beynon et al. 2012; Renker, 2008; Sprague et al. 2012). Client-related barriers—such as fear, shame, self-blame and lack of knowledge of what help providers can offer—also hinder clients from disclosing IPV to providers.
Numerous studies have found that the absence of a trusting relationship between the patient and provider—due to the lack of continuity of healthcare providers, language barriers, and uncaring attitudes from healthcare providers—is a formidable barrier to IPV disclosure (Kramer et al., 2004; Prosman et al., 2014; Rhodes et al., 2018; Shiu-Thornton et al., 2005; Stockman et al., 2015). Studies have underscored the importance of the patient-provider encounter in encouraging help-seeking behavior: physicians with open, compassionate communication styles are more likely to spark disclosure of IPV (Chang et al., 2005). In Feder et al.’s (2006) review of studies involving women with a history of IPV, survivors desired responses from health care professionals that were nonjudgmental, nondirective, and individually tailored, with an appreciation of the complexity of IPV. This may be particularly important for Asian immigrant women, who may experience intense shame from disclosure. The literature also emphasizes the importance of cultural competency and use of interpreters among healthcare providers in screening for IPV (McKibbin & Gill-Hopple, 2018).
To date, very little research has been done to identify and reduce client-related barriers to IPV disclosure among Asian immigrant women in the primary healthcare setting, which could be the first step in assisting them to obtain appropriate services. A major difficulty is that Asian immigrants to the United States are highly diverse not only in ethnic background, but also in religious beliefs, cultural practices, socioeconomic status, and immigration experiences (Chang et al., 2009; Lopez et al., 2017). This diversity poses challenges in developing culturally relevant IPV interventions for Asian immigrant communities (Kim & Schmuhl, 2018; Yoshihama & Tolman, 2015).
Our main objective in this study was to obtain Asian immigrant women’s assessments on whether watching videos placed in clinic consultation rooms could prompt patients to discuss IPV with their provider. Through their comments on the videos, we also aimed to learn more about the specific barriers to IPV disclosure that Asian immigrant women face. Our secondary objective was to discern if there were significant differences in perceptions by ethnicity.
Methods
Intervention: Videos Against Violence
For this study, we first developed a strategy to encourage self-disclosure of IPV, and then asked Asian immigrant women to assess it. Our strategy consisted of creating short, culturally appropriate, multi-lingual videos that could be shown in consultation rooms of primary care facilities as women waited to be seen by a provider. We hypothesized that the consultation room could be a “safe space” for a woman to disclose IPV if she felt comfortable revealing her abuse. The expectation was that the videos would provide time for self-reflection, allay a woman’s concerns or fears about self-disclosure, and motivate her to discuss IPV with a health provider. Our focus was on the primary care setting in order to reach women before the physical violence escalated to warrant a visit to an emergency department.
We chose to develop multi-lingual narrative videos, rather than computer-assisted screening, for several reasons. First, videos can overcome low literacy or limited English skills, which could hinder self-assessment. Videos may also be more compelling, can better explain complicated terms, and be more understandable than written information. Furthermore, videos may help facilitate a dialogue between victims and health care providers (Trautman et al., 2007). Research has found that use of empathy and creating “windows of opportunity” for sharing highly charged or emotion-laden information results in patients feeling better able to share and be understood (Levinson et al., 2000). Videos let victims know that providers can help and also give providers an easier way to broach the subject of IPV, opening up space for women to reveal.
For each video, we employed Asian immigrant woman between the ages of 25 and 45, who we hoped would be relatable to Asian female patients. Building on social judgment theory, we aimed to determine what types of communicative messages and under what conditions could lead to IPV disclosure (Sherif & Hovland, 1980). According to this theory, persuasive messages are the most likely to succeed if they fall into an individual’s latitude of acceptance. If the speaker’s point of view is similar to her audience, persuasion is more likely (Sherif & Hovland, 1980). Our goal was for viewers to be able to identify with the woman in the video, consider whether their experience was similar to hers, and be persuaded to disclose their own abuse.
We began by creating a community advisory board composed of IPV experts, therapists, and health providers in Los Angeles to guide the intervention. We also conducted focus group discussions with survivors and immigrant groups. Based on interviews and discussions, we decided to make videos in four languages common in Southern California: Korean, Mandarin Chinese, Thai, and Vietnamese. The board advised us to have the videos end on an upbeat note, explain about the forms of IPV, stress that the woman is valuable and deserves a better life, and address fears such as that immigrant women will be deported if they divulge IPV.
Ultimately, each video ran for about three minutes so as not to impede clinic flow. The videos featured an Asian immigrant woman (mainly actresses) who described her personal experience of IPV and how she had been assisted after disclosing IPV to her provider. The narratives followed the five-step persuasive communication structure of Monroe’s Motivated Sequence: (a) get attention; (b) establish the need (or problem); (c) explain how the need is satisfied; (d) visualize the benefits; and (e) provide action steps (see Supplementary material for more information). We developed a basic script for the videos which began with the survivor’s story of what she had endured (the need), how she decided to disclose IPV to a health professional to get help and the services she received (satisfaction), and how her life has improved (visualization). The videos ended with the woman encouraging the viewer to tell her provider today if she were experiencing IPV (action). Professional videographers filmed and edited the videos. We encouraged each woman in the videos to improvise on the script and make it more relevant to women of her ethnicity. The Korean woman, an actual survivor of IPV, incorporated her own experience into the script (see Supplemental Material for English translations of the scripts).
After developing the videos, we sought the perspective of Asian immigrant women in California about how persuasive this strategy would be in encouraging women of their ethnicity to disclose IPV in health facilities. Having immigrant women view the videos, comment on whether the strategy of showing videos in consultation rooms could be effective, and give suggestions for ways to improve the videos gave us a number of important insights—not only into the viability of the strategy itself, but also into how IPV victims are perceived and what it would take for the videos to achieve their intended goal.
Data Collection and Analysis
For data collection, we relied on in-depth, semi-structured interviews led by female graduate students of the same ethnicity who spoke one of the four languages fluently. Eligible participants were married women, aged 25–55, who had been born outside of the United States and emigrated as adolescents (or later). The students recruited participants through flyers in various sites (health centers, churches, grocery stores), online chat groups, visits to Buddhist temples, newspaper ads, and word of mouth. Participants were told that the study concerned IPV but were not asked if they had personally experienced IPV.
All interviews were conducted in the language of the participant, either in person in a private room or by telephone and lasted 45–60 minutes. The participants all gave informed consent (verbal or written) and were assured of confidentiality. To maintain privacy in phone interviews, participants were told that they could end the call at any time if they could no longer speak openly. Similar to a vignette approach, participants watched the video first and then were interviewed using a guide developed by the study team. Debriefing by the study team occurred after the first two interviews from each group and revisions were made to the question guides. The interviews were audiotaped, transcribed and translated into English. Participants received a $25 gift card as compensation. The UCLA Institutional Review Board approved the study.
Altogether, sixty women were interviewed, fifteen from each ethnicity: Mandarin Chinese (M), Korean (K), Thai (T) and Vietnamese (V). Several of the women had previous experience working with IPV survivors. Half of the Korean participants and three of the Vietnamese participants spontaneously mentioned that they had been or were currently experiencing spousal abuse. None expressed that she was currently in any physical danger, although one had been hospitalized previously for her injuries.
Transcripts were analyzed using content analysis to identify key themes. The transcripts were coded by two senior members of the study team (PT and MW) using open coding to develop a broad coding scheme. The investigators next re-read all transcripts and field notes, and independently coded each transcript (Strauss & Corbin, 1998). Then they met to reach consensus on initial codes to maximize inter-rater reliability. The team identified emergent themes and selected illustrative verbatim quotes to represent these themes. After main themes and sub-themes were identified, another member of the team assisted in quantifying responses to create Table 1, to enable us to investigate differences by ethnicity. Altogether, the sixty participants provided nearly two hundred suggestions for improvement. For this analysis, we used the last four steps of Monroe’s Moderated Sequence as an organizing framework.
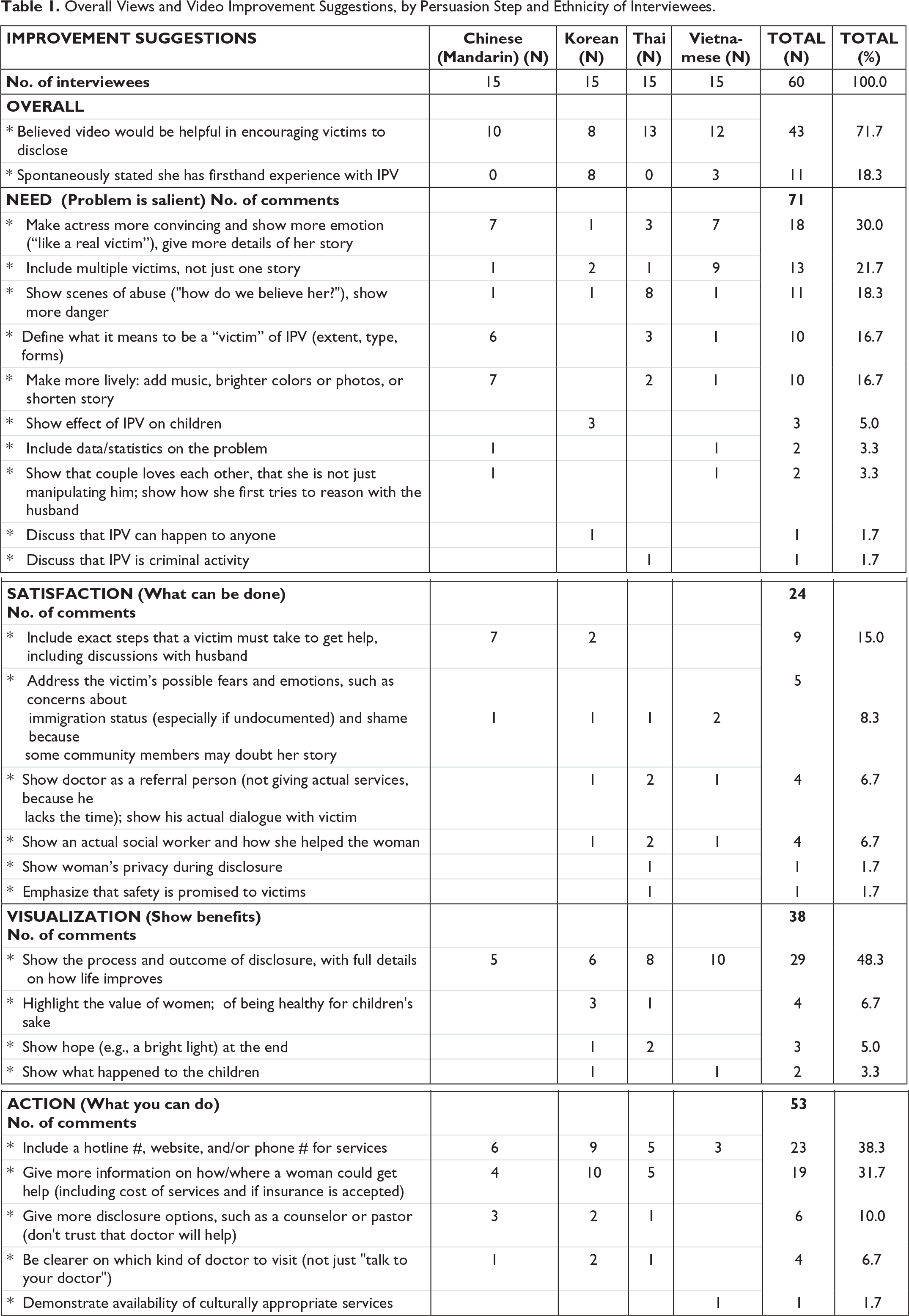
Overall Views and Video Improvement Suggestions, by Persuasion Step and Ethnicity of Interviewees.
Results
Positive Aspects
Nearly three-fourths of participants indicated that they felt the videos would be useful in encouraging IPV victims to disclose, although it is notable that only about half of the Korean speakers agreed (Table 1). No differences by ethnicity were discerned in participants’ comments on the positive aspects of the videos. Most participants felt that it was valuable to have the videos depict a woman survivor’s personal story and to hear her discuss what happened after she disclosed. They felt that the videos would help victims to feel less alone. Viewers would be able to identify with the woman and reflect on whether they were in a similar situation. Moreover, many believed that the videos conveyed well that it is acceptable to tell someone about the IPV, rather than keep it a secret.
Several participants stressed the importance of ensuring that every patient viewed the videos alone, as abusers often wanted to be present during the exam to discourage women from revealing the IPV. They had serious safety concerns about showing videos in a waiting room where the abuser might be present. They also felt that if the patient watched it with a friend or family member, she might be embarrassed or ashamed, and would just pretend that it was not relevant for her:
You don’t know how serious the domestic violence has been for her. If her husband is very abusive, he may think, “You are watching this, are you going to report me?” He may hurt her even more. (M2)
Most participants felt that the story in the video was inspiring and would encourage disclosure, because it showed women who were able to get help and were living free of violence. They particularly liked that the videos ended on a positive note, with hope for the future, rather than showing ongoing sadness and problems, which could be construed as pitiful. Messages like “you’re worth it” or “you deserve happiness” were considered the most powerful:
I think this video is very helpful for those women who keep all their sufferings to themselves. This is a way out of no way. It was mentioned that she went to the counselor. In addition, she said you should give yourself happiness. You should give your children a happy mother. I think this is very convincing. (M8)
The majority of participants reported that they admired the victim and thought she was brave. They recognized how difficult it is in their respective cultures to “air the family’s dirty laundry.” Some specifically mentioned that they would want to help her and that “the community could learn a lot from her.” They related well to her and her story:
In the video, she seemed very peaceful. So if I were the victim, I would think “I want to become like her.” The video could make the victim realize what she is going through. Victims want to escape from it. I mean, who wants to live like that? So I think woman will be encouraged. (K3)
Participants also felt that it was worthwhile to reassure victims that a health care provider would be a good person to confide in, because they are helpful, trustworthy, and will maintain confidentiality. Many believed that victims might not know that the healthcare setting is a safe place to discuss IPV and to get referrals. There is a common perception that a health clinic is not an appropriate place to discuss domestic problems. Participants felt that it would be a relief to know that help was close at hand:
The video helped me realize that getting help is easier than I thought. My doctor or nurse could help me too. Contacting the police might be too intimidating. I think police officers tend to ask insensitive questions. Some victims might not feel comfortable to answer those questions. Doctors seem more gentle. When we don’t feel well, we think of doctors. I don’t know if police officers would really help me if I was a victim. But if I think of my doctor, I think of someone who is kind and is willing to help. (T10)
Many participants remarked that a video alone might not be able to convince a woman to ask for help right away, since it cannot overcome all of the hurdles that a woman experiencing IPV faces. However, they felt that the videos were a valuable first step in the process. They noted that the IPV message had to be repeated frequently until someone was ready to hear it:
To convince someone, to wake them up, so that they can realize, speak out, “reach out” and to believe in another person, to trust another person, I think is very hard but I never lose hope. Even if we think that the ring of a bell takes a thousand years to reach someone’s ears, they will awaken and hear it one day. That is the hope. (V7)
Domestic violence is a very sensitive subject and many women are not open to it. You must say it once, twice, and three four five times. That’s the only way to bring it to the Vietnamese community. (V2)
Suggestions for Improvement
During the interviews, participants were probed to provide suggestions for improvements to the videos. A few were reluctant to be critical, but virtually all gave numerous suggestions for how to make the videos more convincing to immigrant women (Table 1). The suggestions are categorized using the last four steps Monroe Moderated Sequence.
a. Need (problem is salient).
The Monroe step that received the most comments concerned whether the IPV storyline was sufficiently compelling. About one-third of participants felt the videos needed to be more emotional and dramatic to convince viewers that IPV was serious enough to warrant disclosure. Some ethnic differences emerged. The majority of Chinese and Vietnamese participants maintained that a “real” victim would not be able to tell her “horror” story without becoming sad or emotional. For Thai participants, most felt that the video needed to give more details and show scenes of abuse to make the story credible. Indeed, some thought that a real victim would be too ashamed or fearful of being identified to consent to have her face shown:
I think the woman in the video should show evidence of abuse to make her story more convincing. She was only saying that she was abused, but there was no proof. I was wondering the whole time if she was telling the truth. She began telling us that her husband was good to her in the beginning, then everything went downhill. She said he hurt her, but there was nothing to prove her story. (T8)
I think the woman in the video could be more convincing. Do you know TV shows that interview victims of abuse, like children who have been abused or tortured? When they film the interviews, they blur or cover the victims’ faces. The victims would wear a cap and a pair of black sunglasses to protect their identities. If the producer could do that, the video would be more convincing, more realistic. (T9)
Many participants were concerned that people only consider IPV to be dangerous and worthy of disclosure if the woman is physically attacked or threatened. Hence, they felt the videos should stress that there are many forms of IPV, not just physical abuse but could also be emotional, sexual, or financial abuse. To bring this point home, some participants, particularly Vietnamese, believed that the videos should showcase a variety of IPV stories, so that viewers could see different examples and more easily identify their personal experience as IPV:
No one deserves to be treated violently. No one has the right to control your life. You should be the one who controls your own life. To spread this idea, we should eradicate the misunderstanding around domestic violence which considers only physical abuse as domestic violence. The definition of domestic violence should be broadened. We should tell people that mental abuse, economic abuse and being controlled are all domestic violence. This is very important. (M2)
I think the experience of one person cannot cover all situations. More people’s experiences should be covered. If there is only one kind of experience, others may wonder whether they can seek help. (M6)
Some participants felt that the message that IPV has negative effects on children needed to be emphasized. They noted that women often keep quiet about IPV to keep the family intact for the sake of the children. They suggested that the videos would be improved if they challenged this prevailing viewpoint by telling viewers that women experiencing IPV should seek help because of their children. A few participants felt that women would respond to the message that their children deserve to have a happy and healthy mother. But the more common opinion, particularly among Koreans, was that women could be more easily persuaded to disclose if they were convinced it was better for their children—both now and when they formed their own families:
You can tolerate violence if you are alone. But it is very likely that son will resemble the father, including violence. Women are important, but children are important too. So it would be effective to persuade if there is any mention that children improved after getting help. (K12)
The concern about the effect of violence on children could make the video more effective... since women tend to tolerate it if it only affects them, but not children. They will not be able to bear it [if children are at risk]. (K2)
b. Satisfaction (what can be done).
A number of participants felt that the video was too general in terms of the steps that would be taken once the victim revealed the IPV to her physician. They felt that victims would be more likely to divulge IPV if they could know exactly how the process would play out. This would help them to feel prepared for what was to come and to weigh their options. Some even suggested that the video depict an actual conversation between a victim and health provider, so that the viewer could witness what would transpire and get advice vicariously:
If I were the woman who wanted to seek help, I would wonder what help I can receive after I told my doctor. What would I need to do next? What would happen next? Every time you do anything, I will need to have some expectation about the consequence. If you know about the consequence, you will have more confidence and guts to do it. The information is too general. I can tell my doctor. But what my doctor will do with this? This is what I really care about. How will my doctor help me? …I want to know the step-by-step road map to solve the problem. Then I know I can solve the problem. I can feel more relieved. I will feel more comfortable to talk about my story. (M13)
Many also felt that the video needed to be more specific in terms of the help available for different types of IPV. Similar to the issue discussed earlier about what constitutes abuse, participants weren’t clear about what services would be available for various types of abuse or even whether it would be appropriate to report it:
This video has not talked about the range of domestic violence which can be helped by professionals. For most people, physical abuse is definitely warranted to seek help. But are emotional or verbal abuse also warranted to seek help? I don’t know whether it’s OK to seek help. (M6)
In addition, participants believed that women should be reassured that they will not be required to take certain actions just because they disclosed IPV to a provider. Some were worried that women might be disempowered by the process. They felt that the videos should explain that women who divulge IPV would not be forced to leave their abusers unless they chose to do so, and that speaking up would not necessarily lead to divorce, since divorce was seen as socially unacceptable to some participants. Victims should know that their safety and privacy would not be compromised. Instead, victims should feel convinced that reporting IPV would be good for them and their children, and would not lead to deportation or other harms, even if they were undocumented:
I think we should let them know that seeking help is doing good to your family. Seeking help is saving your family. It’s not damaging your family. It will not lead to divorce or loss of immigrant status. (M5)
We want them [doctors] to understand and for them to say, “This is not your fault,” and to refer us, give us the correct information so that we go [seek help]. To encourage us, not to patronize us, not to force us or to parent us because we have already been through enough and we don’t need to be anyone else’s victim. We don’t need anyone to force upon us anything else. (V7)
c. Visualization (show benefits).
Nearly half of the participants felt that it was essential for the video to give full details about how a woman’s life improves after disclosure of IPV. Some were skeptical that women would be willing to divulge IPV and seek help because of community opprobrium, financial hardships, parental dismay and concerns about losing face. However, if the IPV was traumatic and the benefits of disclosure were manifest, they believed that women might consider divulging IPV. Participants suggested that the last scene of the video needed to be particularly uplifting to convey to women that disclosing was worthwhile:
Toward the end, there should a bright light to symbolize hope or a new beginning for victims of abuse who contact this organization. The message is “the organization is here to help you!” (T1)
Once she’s okay you should show a scene of how she’s happy, relaxed and what she has achieved—like a flower blossoming—something analogous. (V10)
d. Action (what you can do).
While most participants believed that the video would be helpful in encouraging IPV disclosure, about one-half felt that it was important to give women options for how and to whom to disclose. Many spontaneously recommended that the video display a hotline number available in their language 24 hours per day. Others doubted whether a woman suffering from IPV would, or should, actually trust a health care provider with this information. They felt that the provider’s ability to help was limited, largely due to time constraints but also lack of empathy and patience. For this reason, some suggested that women be encouraged to consult with a counselor or pastor:
It’s not realistic to tell women to just talk to their doctors or nurses. My doctor’s office is open Monday–Friday only. What if I need help on the weekend? Who do I talk to? (T1)
Doctors only see a patient for a few minutes. So I don’t know if doctors take time with that kind of situation. It [the video] can be misleading for women to expect that. I don’t think doctors will have the time or the feelings like she portrayed her doctor… Instead I’d have the doctor just give her resources about where to find help. (V3)
Discussion
This study provides Asian immigrant women’s perspectives on a video-based intervention to encourage IPV disclosure in primary healthcare settings. First, most believed that showing a short video about an Asian immigrant survivor’s experiences would be helpful to victims, even if they did not divulge right away. Second, the results align with other studies that have found Asian immigrants lack awareness about the scope of IPV, which includes not only physical violence but also emotional, sexual, and financial abuse (Kim & Schmuhl, 2018; Shiu-Thornton et al., 2005). Our study revealed that many immigrant women may be quietly enduring IPV because they believe it must be severe physical abuse to warrant seeking help.
Our study also confirmed that disclosure of IPV is very difficult among the four Asian ethnic groups. Other studies have similarly found that Asian immigrant women often endure IPV due to patriarchal traditions and strong stigma about divorce, particularly among Koreans (Chang et al., 2009; Kim & Schmuhl, 2018). Asian women also do not seek help out of an obligation to portray their families as lacking conflict, and because they view family violence as a private matter (Bui, 2003; Kwok, 2013; Raj & Silverman, 2003; Shiu-Thornton et al., 2005).
Participants felt it was necessary for the videos to give detailed information about women’s (and children’s) lives following a disclosure, so that a victim could directly weigh the benefits versus the costs. Generally, participants felt that women would only disclose severe abuse, because the costs that could arise in the form of family disruption, financial instability, and humiliation were considerable, which has been echoed in other studies (Kasturirangan et al., 2004; Kim & Schmuhl, 2018). Being convinced that children would benefit from disclosure might tip the balance, because other studies have found that some women stay in an abusive marriage for the sake of their children (Bhuyan et al., 2005; Shiu-Thornton et al., 2005).
Our study also found that many participants perceived healthcare providers to be too busy, unprepared, or insufficiently empathetic to assist IPV victims. Similar to other studies, some participants did not view healthcare providers as reliable or sympathetic resources (Chang et al., 2005; Kim & Schmuhl, 2018). Participants also believed that many women would not know that it was appropriate to divulge IPV in clinics. To overcome these barriers, health clinics need to inform women that the consultation room is a safe and confidential space to disclose IPV, and to implement and enforce policies that clients are seen alone. Without assurances of confidentiality, our study aligns with others that have found that Asian immigrant women may feel too fearful to disclose; clinicians need to establish trust and rapport with immigrant clients if they wish to help them with IPV (Feder et al., 2006; Kim et al., 2018). Consistent with other studies, we found that women affirmed that they would be unlikely to reveal IPV to a provider who does not speak their language or understand their culture (Bent-Goodley, 2005; Kim & Schmuhl, 2018; Kwok, 2013; Lee & Hadeed, 2009; Shiu-Thornton et al., 2005; Stockman et al., 2015). This likely explains why many participants recommended that the videos show a hotline number that victims could call anytime to speak to someone in their own language. To improve the likelihood of disclosure, clinic staff need to be multi-lingual or to have access to translation services, as well as training on how to identify and refer clients who report IPV. Many other studies have recommended providing patients with multi-lingual resources and information, such as posters, brochures, and informational cards to encourage future disclosure (Chang et al., 2005; Han et al., 2010; Lee & Hadeed, 2009).
Interestingly, some of the criticisms of the videos revealed that the participants have a stereotyped view of how IPV victims appear and act. Because IPV is a common subject in popular media, such as soap operas, participants may have an unrealistic view of how victims behave. Many participants believed that all women who have experienced IPV would be very emotional and passionate. As a result, some did not find the survivor’s story to be credible, which would lessen the impact of the video. Hence, it might be advisable for the videos to feature more emotional stories to garner greater empathy and engagement from the viewer.
In addition, the videos might be more impactful if they showed a role-play scenario with actual providers counselling victims. Similarly, Kim et al. (2018) found that IPV screening for Korean immigrant women in health care settings can be improved by informing patients about the role of health care providers in addressing IPV and establishing rapport before IPV screening. To overcome the perception that the healthcare setting is not an appropriate place to discuss such matters or that providers are too busy to deal with IPV, providers depicted in the videos should appear empathetic and ready to help. Ending the videos on a happy, hopeful note also seemed important to convey optimism for the future. Previous studies indicate that when physicians show empathy and create “windows of opportunity” for sharing highly charged or emotion-laden information, patients feel better understood (Levinson et al., 2000; McCauley et al., 1998). Multiple exposures to the videos may be needed to give a woman enough time to reflect on her circumstances and make the decision to disclose.
Overall, participants’ views about the videos did not seem to differ significantly by ethnicity. In general, viewers wished for more details about the abuse, the process of getting help, and the aftermath. Desiring a broader definition or more examples of IPV was expressed more frequently by Chinese and Vietnamese participants, while Thai participants seemed to consider disclosure more shameful (victim needing to hide one’s face). The Korean participants’ views did diverge somewhat from the others: they were more likely to consider the IPV problem salient, to discuss the issue of children’s well-being, and to emphasize the importance of discussing the value of women’s lives and happiness. However, these differences may relate to the fact that Korean video was the only one to portray an actual victim, and one-half of the Korean participants had personal experience with IPV.
This study had several limitations. First, because the actresses were encouraged to modify their stories to make them more culturally appropriate, the videos were not uniform. While this might make them more impactful, it also may have had some effect on how the videos were perceived by the participants. Other stories might elicit different feedback. Second, while no participant was asked to divulge their IPV experiences, nearly one in five did spontaneously reveal her past or ongoing IPV. Initially, we had planned to conduct focus groups with various ethnicities, but we soon learned that Asian immigrant women were reluctant to discuss IPV in front of others, even if they were not being asked about personal experiences. Actual survivors of IPV might have a different perspective of the videos than those who were not survivors, but our study was not designed to discern this. Lastly, it is not possible to know if the videos would have the intended impact with (or without) the changes suggested. Determining if the videos would indeed increase disclosure among Asian immigrant women was outside the scope of this study. More research is needed to measure the extent to which culturally appropriate videos encourage disclosure in this population.
Conclusions
For Asian immigrant women, the challenges of disclosing IPV and getting appropriate help are daunting. They may lack awareness of IPV, or feel trapped, isolated, ashamed, and fearful of negative consequences of disclosure. The risks of disclosure and the lack of awareness of services to help may seem to outweigh the benefits, so they continue to suffer silently. Moreover, many are not aware that health providers might be able to assist them. This study’s results suggest that culturally relevant interventions based on persuasion theory—such as multi-lingual videos placed in primary health clinic consultation rooms—may help to overcome some of the barriers to immigrants’ disclosure and start them on the path to a better future.
Supplemental Material
Supplemental material for Encouraging Asian Immigrant Women to Disclose Intimate Partner Violence in Primary Care Settings.
Supplemental material for Encouraging Asian Immigrant Women to Disclose Intimate Partner Violence in Primary Care Settings. by Paula Tavrow, Danny Azucar, Dan Huynh, Caroline Yoo, Di Liang, Wanda Pathomrit, Mellissa Withers in Journal of Interpersonal Violence
Footnotes
Acknowledgments
We wish to acknowledge the advice of our community partners, particularly the Center for the Pacific Asian Family, the Coalition to Abolish Slavery and Trafficking, 1736 Family Crisis Center, and the Thai Community Development Center. We thank Weiyu Yang for providing assistance in data analysis. Finally, we are grateful to the participants of this study for sharing their perspectives.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a community partnership grant from the UCLA Fielding School of Public Health.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.