
Abstract
Prior studies have demonstrated that sexual minority college students are two to four times more likely to experience sexual victimization (e.g., sexual assault and/or unwanted or uncomfortable sexual experiences) compared to their heterosexual counterparts. However, research that has focused on the detrimental effects of sexual victimization on health outcomes has paid more attention to heterosexual college samples and community-based adults. Understanding how sexual victimization influences mental health and substance use outcomes among lesbian, gay, bisexual, queer, and asexual (LGBQA) emerging adults in college is warranted given that this developmental period represents a critical risk period for trauma exposure, risk behavior, and psychological distress. Thus, the current study tested how sexual victimization was associated with depressive symptoms, post-traumatic stress disorder (PTSD) symptoms, and alcohol use disorder (AUD) symptoms among 234 diverse college students who self-identified as LGBQA. Additionally, social support was tested as a moderator. Findings indicated that sexual victimization was related to greater depressive symptoms, PTSD symptoms, and AUD symptoms. In addition, perceived social support moderated the relation between sexual victimization and depressive symptoms, however, in a direction contrary to hypotheses. In particular, higher sexual victimization was associated with greater depressive symptoms among LGBQA students with higher levels of social support (b = .29, p = .00), and was not significant among LGBQA students with lower levels of social support (b = .13, p = .26). The current study highlights the need to consider the detrimental effects of sexual victimization on health outcomes among LGBQA college students, as well as the mechanisms through which social support may be influencing these relations.
Introduction
Sexual minority college students are people who identify as, but not limited to, lesbian, gay, bisexual, queer, and asexual (LGBQA; Rodrigues et al., 2017). Research has indicated that this population is two to four times more likely to experience sexual victimization (e.g., sexual assault and/or unwanted or uncomfortable sexual experiences) compared to their heterosexual counterparts (e.g., Edwards et al., 2015). Further, LGBQA individuals are at particularly high risk for sexual assault given biased systemic oppression and heterosexism within college settings (e.g., McCauley et al., 2018). The prevalence of sexual victimization experiences among LGBQA college students is a concern given the known detrimental effects on a number of health outcomes, such as higher depressive symptoms, post-traumatic stress disorder (PTSD) symptoms, and alcohol use disorder (AUD) symptoms (e.g., Gilmore et al., 2018). Despite the alarming increased risk of sexual assault among LGBQA college students, more attention has been given to heterosexual college samples (e.g., Blayney et al., 2019) and community-based adults who identify as LGBQA (e.g., Hequembourg et al., 2013).
Understanding how sexual victimization influences mental health and substance use outcomes among LGBQA emerging adults in college is warranted given societal and institutional adversities impacting LGBQA college students that present unique challenges and stressors, such as heterosexism and homophobia in college settings (Blosnich & Bossarte, 2012). Further, although prior work has demonstrated that sexual victimization leads to worse depressive symptoms among LGBQA individuals (Boza & Nicholson Perry, 2014), less work has focused on factors that may influence the relation between these two variables, such as social support. Findings from research with general populations (i.e., sexual orientation unspecified) have suggested a buffering effect of social support on health outcomes such as PTSD, depression, and alcohol use (Dworkin et al., 2017). Although scholars have suggested that social support might influence the association between stressors (e.g., sexual victimization) and health outcomes among LGBQA individuals (Meyer, 2003), limited research has tested this notion. Given that understanding these relations may be important to addressing mental health functioning and mental health service needs among LGBQA college students, this is a notable gap.
The Transactional Model of Stress and Coping
The current study is grounded in the transactional model of stress and coping (Lazarus & Folkman, 1984), which provides a useful framework for understanding the relations between sexual victimization and health outcomes. Broadly, the transactional model of stress and coping (Lazarus & Folkman, 1984) suggests that stress is a transaction between situational and personal characteristics that leads a person to perceive an event as stressful and that these external stressors can influence adverse health outcomes. Therefore, drawing from this theoretical framework for this particular study, it is possible that experiencing sexual victimization (i.e., an external stressor) increases depressive symptoms, PTSD symptoms, and AUD symptoms among LGBQA college students.
Furthermore, the model posits that the impact of external stressors on health outcomes can be moderated by a person’s appraisal of the stressor and their resources, such as their various forms of coping strategies. Following this notion, social support can be seen as a coping strategy that can influence these relations. In the context of this present study, it is possible that when LGBQA college students experience sexual victimization, it may interact with social support to influence health outcomes (e.g., depressive symptoms). Given that there is limited empirical research that examines the relation between sexual victimization and health outcomes among LGB+ individuals, the present study explores (a) literature that has examined these associations among primarily heterosexual college students and (b) research that has assessed these relations among LGB+ individuals, including LGBQA college students.
Effects of Sexual Victimization on Health Outcomes Among Primarily Heterosexual College Students
Following the notions proposed by the transactional model of stress and coping (Lazarus & Folkman, 1984), sexual victimization serves as a significant source of physical and psychological trauma with far-reaching health consequences, including subsequent poorer mental health and risky substance use (e.g., McCauley et al., 2018). Following sexual victimization experiences, negative trauma-related beliefs and avoidance behaviors associated with trauma and sexual assault often increase depressive symptoms (Taft et al., 2009) among primarily heterosexual college students (Aosved et al., 2011; Chang et al., 2015; Lindquist et al., 2013; Littleton et al., 2013; Nickerson et al., 2013). For example, in a cross-sectional study involving female college students, survivors of sexual assault reported significantly greater depressive symptoms compared with non-survivors (Littleton et al., 2013). Similarly, male college student survivors of sexual assault, compared with non-survivors, also reported significantly greater depressive symptoms (Aosved et al., 2011). Overall, it is possible that sexual assault is associated with increased depressive symptoms via negative beliefs and avoidance behaviors in both male and female college students; however, more work is needed in this area.
Additionally, findings from prior research have indicated that trauma-related cognitive disruptions and dissociative experiences hinder trauma processing, which increases post-trauma psychopathology, such as PTSD, among sexual assault survivors (Foa & Rothbaum, 1998; Taft et al., 2009). Supporting this notion, sexual victimization has been associated with PTSD among college students (Aosved et al., 2011; Clum et al., 2000; Lindquist et al., 2013; Zinzow et al., 2010).
Furthermore, research suggests that stressful life events, including sexual victimization, affect an individual’s coping resources leading to the use of alcohol in an effort to cope with those stressful life events (Hughes et al., 2014). Therefore, alcohol consumption may be used as a coping mechanism among some survivors of sexual victimization. Following this notion, prior studies have shown that problematic alcohol use often increases after experiencing sexual assault among college students (Bedard-Gilligan et al., 2011; Blayney et al., 2019; Turchik, 2012). For example, women who experienced sexual assault in college reported greater drinking consequences (e.g., passed out or fainted suddenly) than women with no trauma history (Bedard-Gilligan et al., 2011). Further, survivors reported drinking as a way to cope with their sexual assault experience. While prior work has demonstrated that sexual victimization is related to health outcomes (e.g., depressive symptoms, PTSD symptoms, and alcohol use), the majority of studies have tended to focus more on heterosexual college students than LGBQA college students.
Effects of Sexual Victimization on Health Outcomes Among LGB+ Individuals
Prior research examining sexual victimization and health outcomes among LGBQA college students is scarce, but is in line with notions from the transactional model of stress and coping (Lazarus & Folkman, 1984). For example, Kammer-Kerwick et al. (2019) found that gender and sexual minority survivors of sexual victimization experienced significantly higher rates of PTSD, depressive symptoms, and greater disengagement than cisgender heterosexual students.
Related work also provides support for the role of sexual victimization on adverse health outcomes among community-based LGB adults. For example, Heidt et al. (2005) found that sexual victimization was associated with greater psychological distress, depressive symptoms, and PTSD symptoms among a community-based sample of individuals who identified as gay, lesbian, or bisexual. Furthermore, among a community-based sample of gay and bisexual men, individuals with histories of childhood and adult sexual victimizations were more likely to report substance use, including alcohol, than individuals with no history of sexual victimization (Hequembourg et al., 2011). Similarly, sexual victimization was related to higher risky alcohol use among lesbian and bisexual women (Hequembourgh et al., 2013).
All of the above-mentioned studies demonstrate that sexual victimization often leads to worse mental health and substance use, including AUDs, among college and community-based LGB individuals. However, less work has focused on these associations among emerging adults, particularly college students who identify as LGBQA, which is a prevalent gap in the literature.
The Importance of Emerging Adulthood
While there has been research on the influence of sexual victimization on health outcomes, such as depressive symptoms, PTSD symptoms, and alcohol use among community-based adults who identify as sexual minorities (Heidt et al., 2005; Hequembourgh et al., 2011; Hequembourgh et al., 2013), less studies have focused on these associations among emerging adults, particularly college students. Arnett (2000) proposes that emerging adulthood, which is the period between ages 18–25 years of age, is a critical time for identity formation when individuals are continuing to explore who they are and how they fit in the world. Therefore, sexual identity formation is prominent during this stage. Given stress related to negotiating one’s identity during this time, it is possible that sexual minority college students could face greater pressure from institutions (e.g., heterosexist harassment), which could put them at greater risk for victimization, including sexual victimization (McCauley et al., 2018). For example, heterosexism is manifested on college campuses via discrimination and cultural norms that devalue LGBQA individuals and perpetuate heterosexuality as normative and superior (Rankin et al., 2010).
Emerging adulthood also represents a critical risk period for trauma exposure, including sexual assault, as demonstrated by a drastic increase in prevalence across trauma types (Acierno et al., 2001; Norris, 1992) and under-reporting (Budd et al., 2017) during this time. For example, research suggests that individuals in the queer community are less likely to report sexual assault experiences due to the stigma and discourses around sexuality (e.g., Braun et al., 2009). Additionally, emerging adulthood represents a developmental period during which time risk behavior and psychological distress increase, including substance use (Kerr et al., 2014) and mental health issues (Oswalt & Wyatt, 2011). Given the increased risk for negative experiences, particularly among LGBQA college students, research is warranted that tests how sexual victimization experiences influence health outcomes, and factors (e.g., social support) that may mitigate these relations among this population.
Consideration of Social Support as a Moderating Mechanism
As noted, based on the transactional model of stress and coping (Lazarus & Folkman, 1984), the relation between sexual victimization (i.e., external stressor) and health outcomes (e.g., depressive symptoms, PTSD symptoms, and AUD symptoms) may be mitigated by social support. Social support has been identified as an important mechanism that provides a sense of acceptance, social connectedness, and a source of additional resources (e.g., network) among LGBQA college students (e.g., Sheets & Mohr, 2009), with social support directly related to less risk for negative health outcomes (e.g., (Boza & Nicholson Perry, 2014); Pflum et al., 2015). Although findings suggest that social support directly influences health outcomes among LGBQA and primarily heterosexual individuals (e.g., Dworkin et al., 2017), less is known about the moderating effect of social support.
Even though no work has tested social support as a moderator between sexual victimization and health outcomes among LGBQA college students specifically, related work has tested whether social support moderated relations between other forms of stressful experiences and health outcomes among college students and LGBQ individuals (Bissonette & Szymanski, 2019; Sattler et al., 2016; Shorey et al., 2011). For example, Shorey et al. (2011) found that the association between dating violence victimization and alcohol problems was weaker for college students who perceived more social support than for college students who perceived less social support. Additionally, Bissonette and Szymanski (2019) found that positive peer-group relations moderated the relation between internalized heterosexism and depression among LGBQ college students. Specifically, they found that internalized heterosexism predicted depression for students with low levels of positive peer-group relations, but not for those with moderate or high levels. Thus, prior studies have demonstrated the moderating effect of social support on relations between stressors and health outcomes broadly. Again, while these studies (Bissonette & Szymanski, 2019; Sattler et al., 2016; Shorey et al., 2011) did not specifically examine sexual victimization as a predictor, it provides evidence that social support may moderate the relation between stressors and health among LGBQA college students.
Current Study
Guided by the transactional model of stress and coping (Lazarus & Folkman, 1984), the current study extends prior research by testing the associations between sexual victimization, social support, and health outcomes among LGBQA college students. While the potential negative cost of experiencing sexual victimization is well understood among primarily heterosexual college populations, we have yet to fully understand the influence of sexual victimization experiences on health outcomes, as well as the moderating role of social support on these relations, among LGBQA college students. Therefore, the purpose of the current study is to answer the following research questions among LGBQA individuals: (a) are sexual victimization experiences associated with health outcomes (i.e., depressive symptoms, PTSD symptoms, and AUD symptoms) and (b) are the associations between experiences of sexual victimization and health outcomes moderated by perceived social support?
We hypothesized that sexual victimization would be related to increased depressive symptoms, PTSD symptoms, and AUD symptoms. Further, we hypothesized that perceived social support would moderate the relations between sexual victimization and health outcomes (i.e., depressive symptoms, PTSD symptoms, and AUD symptoms), such that these associations would be weaker among LGBQA students with greater perceived social support, compared to LGBQA students with less perceived social support.
Method
Participants
Students in the current study were part of a larger, university-wide longitudinal study examining the influence of genetic, environmental, and developmental factors on college students’ substance use and emotional health outcomes (Dick et al., 2014). The larger sample includes five cohorts of college students at a southeastern university (2011–2014; 2017). From the larger project, the current study focused on 234 students who identified as gay or lesbian (24%), bisexual (44%), queer (20%), or asexual (12%). Data were derived from the Spring 2017 data collection because this wave of data collection was the first and only wave to include a measure of sexual orientation. The participants in the present study were 18–22 years old (M = 18.46, SD = 0.41) and the majority (74%) self-identified as female. Additionally, about half (56%) of the participants self-identified as White (n = 132), 16% as Black or African American (n = 37), 13% as Asian (n = 30), .9% as American Indian or Native Alaskan (n = 2), 3.9% as Hispanic or Latino (n = 9), .4% as Native Hawaiian or Other Pacific Islander (n = 1), and 9.8% listed “more than one race” (n = 23).
Procedure
The larger study was approved by the university’s Institutional Review Board (HM13352). In the larger study, each cohort of first-year college students, from 2011 through 2014, and again in 2017 who were aged 18 and older were invited to participate in the study by completing an online survey. Then, they were invited to complete a follow-up survey every subsequent spring semester while they were enrolled in college. During each survey, participants were provided with an explanation of the study, and students who chose to participate provided informed consent online. Participants then completed the online survey, which took approximately 15–30 minutes. Once the survey was completed, participants received $10 compensation. In the event that any students experienced any distress during the study, they were referred to the University Counseling Center. Study data were collected and managed using Research Electronic Data Capture (REDCap), which is a web-based application designed to assist with data capture for research studies (Harris et al., 2009). Further, standard practices were used to protect participant confidentiality, including removing identifiers from all data collected, using only numbers to identify participant data, and keeping all data files when not in use in a locked filing cabinet behind a locked office. Data sent to investigators were de-identified and investigators did not have access to students’ personal identifying information. The larger project also had a National Institutes of Health certificate of confidentiality (COC) to further protect the participants.
Measures
Sexual victimization.
Sexual victimization was assessed using an abbreviated version of the Life Events Checklist (LEC) measure (Gray, Litz, Hsu, & Lombardo, 2004). This involved two items: sexual assault (e.g., rape, attempted rape, made to perform any type of sexual act through force or threat of harm) and unwanted or uncomfortable sexual experiences. Participants were asked to indicate if they experienced these events in the past 12 months. Participants were given the response option of “Yes” or “No.” No endorsement of an item was coded as 0, and a positive endorsement of an item was coded as a 1, and items were summed to yield a total score ranging from 0 to 2. Prior studies have used this abbreviated version among college students (Hawn et al., 2018). The alpha for the current study was .66.
Social support.
Social support was measured using 3 items adapted from the 19-item Social Support Survey of the Medical Outcomes Study module (Sherbourne & Stewart, 1991). Items asked about experiences in the past 12 months and included: “How often was someone available to give good advice about a crisis?,” “How often was someone available to get together with you for relaxation?,” and “How often was someone available to confide in or talk about your problems?” Responses were made on a Likert-type scale of 1 = None of the time to 4 = All of the time, with higher scores representing greater perceived social support. A mean score was computed ranging from 1 to 4 of the 3 items, with higher scores indicating higher social support. Previous research has used these items to measure social support among college students (Dick et al., 2014). The alpha for the current study was .84.
Depressive symptoms.
A subset of 4 items from the Symptoms Checklist (SCL-90; Derogatis et al., 1973) was used to assess depressive symptoms (e.g., “feeling hopelessness about the future”) within the last 30 days. Participants responded regarding how much each symptom caused them discomfort on a 5-point rating scale ranging from 1 = Not at all to 5 = Extremely. Previous work has shown support for the validity and reliability of SCL-90 with a diverse college population (Spindle et al., 2017). The alpha for the current study was .86.
Post-traumatic stress disorder symptoms.
Four items from the Primary Care PTSD Screen (PC-PTSD; Prins et al., 2003) were used to screen for probable PTSD symptoms within the past 12 months. Participants responded “Yes,” or “No,” on 4 items, each representing one of the four PTSD symptom clusters (e.g., “Have had nightmares about it or thought about it when you did not want to?”), per the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV-TR). For the present study, a positive endorsement of an item was coded as a “1” and a mean score ranging from 0 to 4 of the 4 items was used to index probable PTSD symptoms; higher scores indicate greater probable PTSD symptoms. Previous research has shown good reliability (α = .94) and validity of the original measure among trauma-exposed college students (Blevins et al., 2015). The alpha for the current study was .84.
Alcohol use disorder symptoms.
Symptoms related to AUD were measured using the AUD criterion from the Diagnostic and Statistical Manual of Mental Health Disorders, 5th Edition (DSM-V; American Psychiatric Association, 2013). The 16-item measure assessed items related to the DSM-V AUD criterion (e.g., “Have you continued to drink even though it was causing you medical, emotional, or psychological problems?”). Each item was answered using a 3-point scale with the following answer options 1 = Never, 2 = 1–2 times, 3 = 3 or more times. Participants endorsing a “3” were coded as positive for the symptom, and a sum of the 16 symptoms was calculated. Individuals who did not report drinking alcohol or ever having been drunk were coded as 0 for all AUD symptoms. AUD symptom sum scores ranged from 0 to 13. Prior research has demonstrated good validity and reliability (α = .94) among diverse emerging adults (Lind et al., 2017). The alpha for this current study was .87.
Controls.
Given that prior work has demonstrated that sex, age, and race/ethnicity are associated with mental health outcomes and AUD symptoms (Chang et al., 2015; Jackson et al., 2010; Kessler et al., 2010; Walker et al., 2020), these variables were included as covariates in the models. Sex was coded as 1 = Male and 2 = Female.
Results
Preliminary Analyses
Correlations and Descriptive Statistics.
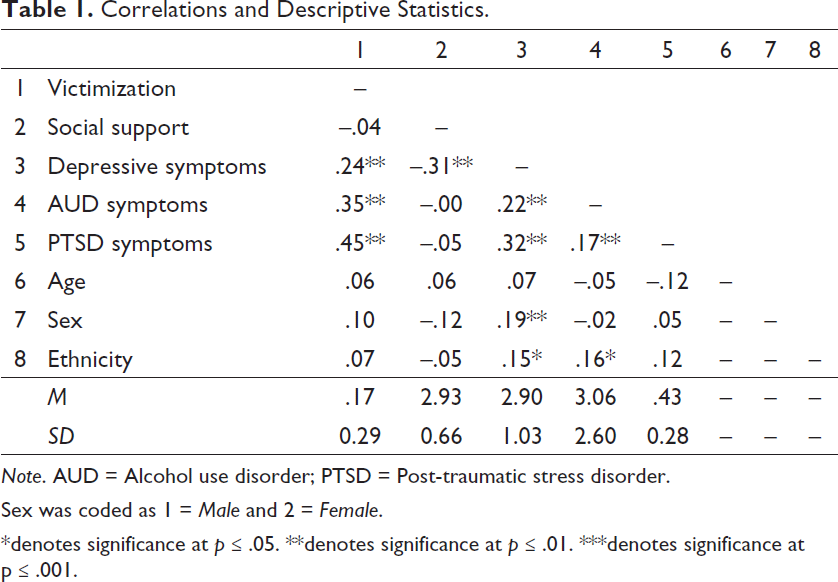
Note. AUD = Alcohol use disorder; PTSD = Post-traumatic stress disorder.
Sex was coded as 1 = Male and 2 = Female.
*denotes significance at p ≤ .05. **denotes significance at p ≤ .01. ***denotes significance at p ≤ .001.
Analytic Approach
In order to test the study hypotheses, our analytic strategy included running a series of regression models in Mplus version 7.2 (Muthén & Mutheén, 2012). Missing data were handled using the multiple imputation method in SPSS (Enders, 2010) and there were no concerning outliers. Three separate multiple regression analyses were conducted for each outcome of interest. Each analysis included a main effect model that tested the association between sexual victimization predicting each health outcome (e.g., PTSD symptoms). Additionally, each analysis included an interaction variable (i.e., sexual victimization X social support) to test whether social support functioned as a moderator for the relation between sexual victimization and each health outcome (e.g., AUD symptoms). Given that all models included interactions, all predictor variables were mean-centered, as recommended by Aiken and West (1991), and the centered variables were used to compute the product of two variables (i.e., sexual victimization and social support) to create the interaction term to test the moderation hypotheses. Any significant interactions were probed and graphed at one standard deviation above and below the mean (Preacher et al., 2006).
Tests of Hypotheses
In testing the hypothesized research questions, several findings emerged. First, sexual victimization explained 23.3% and 15.6% of variance in PTSD and AUD, respectively, with sexual victimization being related to greater PTSD symptoms (β = .45, p < .001) and AUD symptoms (β = .34, p < .001). However, we found no significant moderation effects of perceived social support on the relation between sexual victimization and PTSD or AUD symptoms.
Sexual victimization explained 20.5% of variance in depressive symptoms, with sexual victimization being associated with greater depressive symptoms (β = .21, p < .001). Additionally, findings indicated that perceived social support moderated the relation between sexual victimization and depressive symptoms (β = .13, p = .03), however, in a direction contrary to hypotheses (Figure 1). Simple analysis revealed that higher sexual victimization was associated with greater depressive symptoms among sexual minorities with high levels (+1 SD) of social support (β = .18, p < .001), but the relation between sexual victimization and depressive symptoms was not significant among sexual minorities with low levels (–1 SD) of social support (β = .03, p = .26). Additionally, findings indicated that perceived social support was related to lower depressive symptoms (β = –.29, p < .001), while sex (β = .36, p = .01) and race (β = .05, p = .04) were associated with higher depressive symptoms.
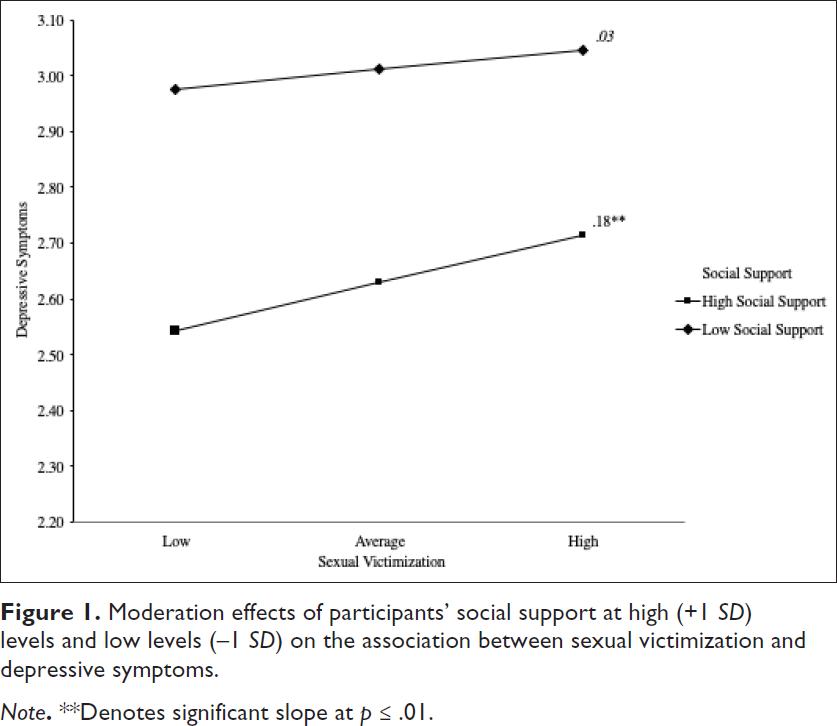
Moderation effects of participants’ social support at high (+1 SD) levels and low levels (–1 SD) on the association between sexual victimization and depressive symptoms.
Discussion
Guided by the transactional model of stress and coping (Lazarus & Folkman, 1984), the purpose of the current study was to test the effects of sexual victimization on health outcomes among LGBQA college students, as well as the moderating role of social support. Below, we discuss (a) findings of the relations between sexual victimization and health outcomes (i.e., depressive symptoms, PTSD symptoms, and AUD symptoms), (b) the role of social support, and (c) limitations and future directions.
Associations Between Sexual Victimization and Health Outcomes
The first hypothesis regarding the direct relations between sexual victimization and health outcomes (i.e., depressive symptoms, PTSD symptoms, and AUD symptoms) was supported. Specifically, we found that sexual victimization was associated with greater depressive symptoms, PTSD symptoms, and AUD symptoms. These findings are consistent with prior research, which has demonstrated that greater experiences of sexual victimization are associated with increased depressive symptoms, PTSD symptoms, and risky alcohol use among heterosexual populations (Aosved et al., 2011; McCauley et al., 2018; Zinzow et al., 2010) and among community-based sexual minorities (Hequembourgh et al., 2011; Hequembourgh et al., 2013).
The current study adds to the growing body of literature documenting the detrimental effects of sexual victimization on health outcomes and extends this literature by specifically demonstrating that sexual victimization experiences relate to poorer health outcomes among LGBQA college students. These associations, combined with higher reports of heterosexism, discrimination, and under-reporting of sexual victimization (Budd et al., 2017) on college campuses suggest the importance of considering connections among sexual victimization, institutional and systemic oppression, sexual identities, and health outcomes. Given that sexual victimization negatively affected health outcomes among a population that is already at risk for health concerns and sexual victimization, more attention to risk and protective factors that may be targeted with sexual assault prevention and intervention, as well as mental health and health care among sexual minority college students is warranted. For example, researchers and practitioners could benefit from identifying protective factors that reduce mental health outcomes among sexual minority survivors of sexual victimization. Additionally, future work may want to examine the relation between non-inclusive health care providers or law enforcement and health outcomes among LGBQA survivors in order to ensure appropriate sexual assault interventions within these fields.
The Role of Social Support
Results of the current study partially supported the second hypothesis regarding the moderation effect of social support on the relations between sexual victimization and health outcomes. Findings indicated that social support did not moderate the relation between sexual victimization and PTSD symptoms and AUD symptoms, which is inconsistent with the literature regarding social support (Bissonette & Szymanski, 2019; Hyman et al., 2003). However, social support was directly associated with lower depressive symptoms, which is consistent with prior studies regarding social support as a protective factor against poorer mental health outcomes (Pflum et al., 2015). Further, social support moderated the relation between sexual victimization and depressive symptoms, although the direction of effects was contrary to our expectations. Specifically, higher sexual victimization was associated with greater depressive symptoms among LGBQA college students with high levels of perceived social support, but was not significant among LGBQA college students with low levels of perceived social support.
It is unclear why social support strengthened the relation between sexual victimization and depressive symptoms. Prior studies have indicated that social support networks for sexual minority youth, in both peer and family contexts, are limited compared to heterosexual peers (Williams et al., 2005). For example, Button et al. (2012) found that sexual minority youth, including college-aged individuals, reported less social support than their heterosexual peers. Further, LGBQA youth reported more worries about losing their friendships (i.e., drifting apart or terminating because of conflict) than their heterosexual peers (Diamond & Lucas, 2004). Additionally, extensive research has indicated that a majority of sexual victimization is committed by someone known to the survivor and connected to their friend group (Gross et al., 2006; U.S. Department of Justice, 2003). Therefore, it is possible that the perpetrator of sexual victimization may be within LGBQA student survivors’ social network, and out of fear of losing their friendships, they may avoid disclosing their sexual trauma and withdraw themselves to avoid interacting with their perpetrator or those connected to the perpetrator, which ultimately may increase their depressive symptoms. Additional research is needed in order to better understand the social networks of LGBQA student survivors of sexual assault, as well as coping mechanisms with regard to their social network, and the perpetrator’s role in their social network.
As noted, there were no significant moderation effects for social support in the relations between sexual victimization and PTSD symptoms or AUD symptoms. To our knowledge, the current study is the first to test the influence of social support on these associations among LGBQA college students. These null findings could be attributed to the measure that combines different types of social support, which may miss some of the specific forms that have been associated with PTSD and AUD symptoms.
For example, prior research has shown that specific forms of social support, such as appraisal and self-esteem, mitigate PTSD symptoms following a sexual violence experience (Hyman et al., 2003), which may be lost when using composite measures of social support. Future studies should evaluate the effects of appraisal social support and self-esteem social support on the relation between sexual victimization and health outcomes among LGBQA college students to test this notion more specifically. Further, different types of social support, such as peer support and functional social support, have been linked with alcohol use among college students (Bachrach & Read, 2017; Kahle, Veliz, McCabe, & Boyd, 2019). Thus, future research might need to independently assess different types of social support that might moderate the relation between sexual victimization and AUD symptoms.
Limitations and Future Directions
While the present study contributes to our understanding of the ways in which sexual victimization and social support inform depressive symptoms, PTSD symptoms, and AUD symptoms among LGBQA college students, there are various limitations to acknowledge. The first limitation is the cross-sectional design of the study. It is difficult to disentangle the potentially interdependent effects of sexual victimization and health outcomes, particularly given the potentially confounding effects of repeated sexual victimization. Additionally, prior work has demonstrated that sexual victimization continues to influence health outcomes over time as survivors recover (Sigurvinsdottir & Ullman, 2015). Therefore, future work should examine how sexual victimization experiences may prospectively influence health outcomes over time, and how social support may moderate those relations.
Second, given the limited sample size, differences based on sexual orientation, sex, and ethnicity/race could not be tested. Prior work has demonstrated that bisexual individuals often report greater sexual victimization, depressive symptoms, alcohol use, and PTSD symptoms when compared to lesbian, gay, and heterosexual individuals (Bostwick et al., 2010; Sigurvinsdottir & Ullman, 2015; Walters et al., 2013). Further, LGBQA young adults may have access to different social support resources both in general and in the campus context. For example, asexual-identified people reported that their social support networks are usually small and consist of online friends and occasionally romantic partners (Hinderliter, 2013; Rothblum et al., 2018). Given that asexual young adults are an understudied population in this literature and LGBQA young adults may have access to different social support resources, future research is warranted. Additionally, White women are sometimes more likely than Black (e.g., Gross et al., 2006), Latina (Koss & Dinero, 1989). and Asian women to experience sexual assault—but not always (e.g., Cantor et al., 2015). Further, prior studies have demonstrated that sexual victimization among sexual minorities varies by sex (e.g., Conron et al., 2010). Therefore, future work should assess these types of differences with larger samples of LGBQA students.
Additionally, as part of a larger study in which we aimed to reduce participant burden, sexual victimization was assessed as a two-item measure of the endorsement of experiencing sexual victimization. The two-item version of the measure has been used among college students and demonstrated good validity (Hawn et al., 2018). However, future studies should consider using multi-item measures of sexual victimization with multiple dimensions to test differences in relations based on types of sexual victimization.
Conclusion
Despite limitations, the current study advances knowledge on the effects of sexual victimization experiences in several ways. First, we add to the body of literature on sexual victimization and health outcomes by examining these relations among LGBQA college students. Understanding the detrimental effects that sexual victimization has on health outcomes during emerging adulthood is important in informing intervention and prevention development that may affect LGBQA college students’ mental and psychosocial health. Second, we tested whether social support works as a moderating variable in the relations between sexual victimization and health outcomes. Findings indicated that when examining the effects of sexual victimization on depressive symptoms, it is important to consider social support in intervention efforts and mental health services. For example, clinicians may want to assess how social support and social reactions affect mental health outcomes among LGBQA survivors of sexual victimization.
Overall, findings from the current study, with continued evidence-based support, may have treatment, clinical, health care, and college campus implications. For example, treatment programming can incorporate education and intervention designed to reduce engagement in problematic alcohol use and manage psychological distress (e.g., PTSD) among LGBQA college student survivors of sexual victimization on college campuses and among health care providers. For example, documenting the sexual violence experienced by LGBQA communities is an important step towards acknowledging the harm caused by this violence, ensuring that adequate and appropriate support services are provided (Duke & Davidson, 2009). In addition, clinicians should assess for health risk behaviors and psychological distress associated with sexual victimization at intake assessments, as well as develop interventions that highlight protective factors and resources that will help LGBQA college students recognize and cope with their sexual victimization experiences. In conclusion, the present study provides insight into the ways in which sexual victimization experiences along with social support inform health outcomes among LGBQA college students, and highlight that continued research in this area will be fruitful.
Footnotes
Authors’ Note
Data from this study are available to qualified researchers via dbGaP (phs001754).
Acknowledgments
We would like to thank the Spit for Science participants for making this study a success, as well as the many university faculty, students, and staff who contributed to the design and implementation of the project.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The content is solely the responsibility of the authors and does not necessarily represent the views of the NIH or the FDA.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Spit for Science has been supported by Virginia Commonwealth University, P20AA017828, R37AA011408, K02AA018755, P50 AA022537, and K01AA024152 from the National Institute on Alcohol Abuse and Alcoholism, and UL1RR031990 from the National Center for Research Resources and National Institutes of Health Roadmap for Medical Research. This research was also supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number U54DA036105 and the Center for Tobacco Products of the U.S. Food and Drug Administration.
Author Biographies
Eryn N. DeLaney’s, MS, work is primarily focused on exploring the influence of intersectionality, resilience/protective factors (e.g., social support) and stressors/risk factors (e.g., sexual victimization), and adjustment across a broad array of domains, including academic, psychological, and behavioral functioning among ethnic-racial and sexual minority students and student-athletes.
Chelsea Derlan Williams’, PhD, work focuses on understanding how risk and resilience factors contribute to psychological, educational, and health outcomes/disparities among Latinx, African American, and Multiracial youth, emerging adults, and families. She centers on ethnic-racial identity, ethnic-racial socialization, discrimination/colorism, and cultural experiences across the lifespan, and aims to extend our understanding of these processes in adolescence/emerging adulthood to earlier developmental periods (e.g., early and middle childhood) by advancing theory and measurement in innovative ways.
Della V. Mosley’s, PhD, work is centered on the psycho-political wellness of people and communities that are marginalized. Additionally, she focuses on social justice, prevention, holistic wellness, and strengths in her research. Della pursues contextually rich, qualitative, and intersectional approaches to exploring the experiences and promoting the wellness of Black, queer, trans, and/or gender-expansive people.
Sage E. Hawn’s, PhD, work assesses the intersection of biological and environmental factors that influence the development of PTSD and problematic alcohol use. More specifically, her clinical research career is focused on the investigation of etiologic and maintenance factors that contribute to trauma-related psychopathology.
Danielle M. Dick’s, PhD, work primarily focuses on how genetic and environmental influences contribute to the development of patterns of substance use (drinking and smoking) and related behaviors, such as antisocial behavior and depression.