
Abstract
Childhood maltreatment (CM) is thought to be linked to adult narcissistic traits. However, it remains unclear how CM is associated with each type of narcissism, vulnerable and grandiose, and what mechanism mediates these links. One potential candidate is dissociation. This study examines the relations among CM, dissociation, vulnerable narcissism, and grandiose narcissism. A total of 322 women completed self-reported questionnaires assessing CM, dissociation, vulnerable narcissism, and grandiose narcissism. To examine the relations among CM, dissociation, and each type of narcissism, we performed Pearson’s correlations and mediation analyses. In secondary analyses, we conducted latent class analyses to classify different types of CM and to assess their relations with the study variables. We found small to moderate correlations between CM and vulnerable narcissism, (r = .35, p < .001) and CM and grandiose narcissism (r = .2, p < .001), with the former association being greater than the latter (z = –3.25, p < .001). Dissociation was found to mediate the link between CM and each type of narcissism (p < .001). Results suggest that CM may play a role in the etiology of vulnerable and grandiose narcissism, and that dissociation links CM to each type of narcissism. Findings highlight that CM may lead to different responses in terms of narcissism—through the same mediation process.
Introduction
Growing evidence suggests that childhood maltreatment (CM) predicts adult personality and psychopathology (Johnson et al., 2013; Luntz & Widom, 1994; Ruggiero et al., 2000; Stoltenborgh et al., 2015). Of particular interest is the finding that CM predicts adult narcissistic traits (Lobbestael et al., 2010; Talmon & Ginzburg, 2019). However, it is not yet clear whether specific patterns of CM are more likely than others to lead to narcissism, and if so, whether these relationships vary for the two different types of narcissism: the vulnerable and the grandiose variants (Wink, 1991). Furthermore, it is not known what mechanism links CM experiences to each type of narcissism. The aim of this paper is to address these issues among adult females.
Childhood Maltreatment
CM is a collective term for any act of commission or omission by a caregiver that results in harm, potential for harm, or threat of harm to a child under 18 years of age (Gilbert et al., 2009). CM includes experiences of emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect (World Health Organization, 2020). In the general female population, frequencies of 10.9% have been reported for emotional abuse, 11.5% for physical abuse, 18% for sexual abuse, 13.4% for emotional neglect, and 47.3% for physical neglect (Iffland et al., 2013).
Understanding the long-term impact of CM is complicated by at least two factors. First, CM is often associated with minimization, which refers to downplaying or reducing the impact of an event or a related emotion. Although minimization was found to be highly prevalent among women with CM, it has mostly been neglected in previous research on CM. This is unfortunate because one study found that minimization is more prevalent in nonclinical samples than in clinical samples, which may suggest an enhanced self-serving bias among nonclinical samples (Church et al., 2017). In this way, minimization could be part of a defense mechanism used to cope with CM. Since minimization often leads to an under-reporting of the severity of CM experiences, its presence makes it difficult to fully assess CM (Bernstein & Fink, 1998; Church et al., 2017). To address these issues in our study, we assessed minimization, and in secondary analyses, we examined outcomes associated with different levels of minimization.
The second factor making the articulation of links between specific types of CM experiences and outcomes more challenging is that different CM types often co-occur and/or happen repeatedly, highlighting the importance of viewing CM multidimensionally (Scher et al., 2004; Talmon & Ginzburg, 2019). To address the issue of CM types co-occurring, in the current study, we employed a latent class analysis (LCA) which enables us to examine the link between individual patterns of CM experiences and their differential outcomes as suggested by recent work in this area (Charak & Koot, 2015; Shin et al., 2018).
Notwithstanding these two difficulties related to the assessment of CM and the articulation of its different types, several lines of evidence suggest a shared set of detrimental consequences of CM on adult psychopathology (e.g., Bernet & Stein, 1999; Li et al., 2016) and personality (e.g., Johnson et al., 2013). One particular point of interest has been the link between CM and adult narcissistic traits (Lobbestael et al., 2010; Talmon & Ginzburg, 2019).
Childhood Maltreatment and Narcissism
Several studies have suggested that CM is associated with vulnerable narcissism, but effect sizes vary considerably, and it remains unclear whether grandiose narcissism is related to CM at all (e.g., Keene & Epps, 2016; Miller et al., 2010; Schoenleber et al., 2015).
Childhood Maltreatment and Vulnerable Narcissism
Vulnerable narcissism is characterized by defensive, anxious, and socially reticent behavioral patterns (Wink, 1991). Individuals with high levels of vulnerable narcissism are dependent, introverted, and hypersensitive (Pincus et al., 2009; Wink, 1991). These individuals tend to engage in grandiose fantasies in order to deal with their fragile self-confidence (Talmon & Ginzburg, 2018). With reference to interpersonal relations, vulnerable narcissism is linked to complacency, arrogance, and the use of social avoidance, if the needed admiration is not received (Pincus et al., 2009; Talmon & Ginzburg, 2018; Wink, 1991). Individuals with high levels of vulnerable narcissism are further characterized by a conscious experience of helplessness, emptiness, low self-esteem, and shame (Pincus et al., 2009).
An important factor in the etiology of vulnerable narcissism may be CM. Vulnerability, dependence, and hypersensitivity are considered to be strategies to cope with CM, since they help to maintain attachment to the abusive caretaker(s). The perpetuation of these traits in adulthood may manifest in vulnerable narcissism (Howell, 2003; van Buren & Meehan, 2015). Several lines of evidence suggest an association between CM and vulnerable narcissism (e.g., Keene & Epps, 2016; Nehrig et al., 2019; Talmon & Ginzburg, 2019).
Childhood Maltreatment and Grandiose Narcissism
Grandiose narcissism is characterized by a strong need for admiration, extraversion, strong envy, interpersonal dominance, and the tendency to overestimate one’s capabilities (Miller et al., 2010; Pincus et al., 2009; Wink, 1991). Individuals with high levels of grandiose narcissism perceive themselves as unique and expect special treatment (Morf & Rhodewalt, 2001; Pincus et al., 2009; Wink, 1991). Thus, grandiose narcissism is associated with troubled interpersonal relations as well as a lack of empathy towards the needs of others (Pincus et al., 2009; Wink, 1991).
Similar to vulnerable narcissism, the development of grandiose narcissism may be rooted in CM. Children who experience CM may use superiority, dominance, and aggression to cope with the maltreatment they face. The perpetuation of these behavioral patterns in adulthood may manifest in narcissistic grandiosity (Howell, 2003; Keene & Epps, 2016; Talmon & Ginzburg, 2018). Research investigating the link between CM and narcissistic grandiosity provides an inconsistent picture. Limited evidence suggests that grandiose narcissism is unrelated to CM (Miller et al., 2010). Other lines of evidence suggest that there is an association between CM and grandiose narcissism. However, this association seems to be weaker than the one between CM and vulnerable narcissism (Keene & Epps, 2016; Nehrig et al., 2019; Talmon & Ginzburg, 2018).
A Mediating Role for Dissociation
It is not yet clear what mechanisms might mediate the link between CM and adult narcissism. However, one possible link is dissociation, a state in which usually integrated functions of consciousness, memory, identity, and perception of the environment are disrupted (American Psychiatric Association, 2013). As a clinical disorder, dissociation can manifest in various forms such as psychic numbing, depersonalization, and/or trances, and is considered a common way to cope with reoccurring memories of CM. Dissociation is not a dichotomous phenomenon, but can be understood as a trait exhibiting various levels of severity in individuals with different experiences of CM (Classen et al., 1993; Talmon & Ginzburg, 2019; Terr, 1991). Thus, dissociation can be considered to be either clinical or subclinical depending on the severity of dissociative symptoms (Bernstein & Putnam, 1986; Carlson & Putnam, 1993).
While it is known that dissociation is related to CM, it is becoming increasingly clear that dissociation is associated with both types of narcissism (Kefeli et al., 2018; Talmon & Ginzburg, 2019). As we describe in the following, certain subfacets of dissociation (the vulnerable and the grandiose variant) are hypothesized to be the path linking CM to vulnerable as well as grandiose narcissism (Howell, 2003; Talmon & Ginzburg, 2018, 2019).
In particular, CM and vulnerable narcissism may be linked through vulnerable self-states. Vulnerable self-states are characterized by helplessness, dependence, and self-objectification. These traits drive the dissociation that would occur in response to the abusive experiences with the caretaker. This is achieved with high sensitivity to the caretaker’s feelings and anticipation of their actions. While sensitivity served its protective purposes during childhood, its perpetuation in adulthood may manifest in pathological hypersensitivity, hypervulnerability and dependent behavioral patterns. These are core features of vulnerable narcissism (Howell, 2003). Although there are no studies to date investigating vulnerable dissociative self-states specifically, evidence concerning dissociation in general suggests associations between CM and dissociation as well as between dissociation and vulnerable narcissism (Talmon & Ginzburg, 2018, 2019). Nevertheless, to the best of our knowledge, there is no empirical evidence for the mediating role of dissociation in the relationship between CM and vulnerable narcissism.
While vulnerable self-states are a survival strategy, and may be used to maintain attachment to the abusive caretaker, grandiose self-states serve as a defense mechanism (Howell, 2003). As mentioned, grandiose self-states are characterized by omnipotence, domination, and terrorizing (Wink, 1991). These characteristics are observable in an abusive caregiver, and are reflected in their interactions with children (Howell, 2003). Howell (2003) suggests that caregivers’ behavioral patterns and the resulting relationship dynamics are reenacted by children. By emulating the caregiver’s behavior, children take on the role of omnipotent protectors for themselves. Employing grandiose self-states enables children to satisfy their needs for safety and shelter independent of the environment (Howell, 2003). Another important effect of employing an omnipotent self-state is that it enables one to dissociate from the abusive reality. While children survive the abuse by attempting to satisfy all their needs autonomously (behaviorally and affectively), they enter an isolated world where there is only one protagonist: the self (Howell, 2003; Terr, 1991). Howell (2003) proposes that long-term manifestations of this defense mechanism are self-centeredness, dominating behaviors, and a sense of grandiosity. In this way, dissociation, originally used to cope with CM, may lead to a grandiose narcissistic personality (Howell, 2003). Although there are no studies to date investigating grandiose dissociative self-states specifically, evidence concerning dissociation in general suggests associations between CM and dissociation as well as between dissociation and grandiose narcissism (Kefeli et al., 2018; Talmon & Ginzburg, 2018, 2019). However, we found no empirical study that investigated the mediating role of dissociation in the link between CM and grandiose narcissism.
The Current Study
The primary aim of the present study was to better understand (a) the relation between CM and each type of narcissism and (b) the mediating role of dissociation. While the link between CM and vulnerable but not grandiose narcissism is empirically well-supported, the mediating role of dissociation has not yet been empirically studied. In the present study, we hypothesized that (a) CM would be positively associated with vulnerable narcissism and that (b) dissociation would mediate the relationship between CM and vulnerable narcissism (Howell, 2003). Because evidence is inconsistent in terms of relations between CM and grandiose narcissism (Keene & Epps, 2016; Miller et al., 2010), we did not have a specific hypothesis for the relations among CM, dissociation, and grandiose narcissism.
Since CM includes various types of abuse and neglect that might differ in their outcomes (e.g., Charak & Koot, 2015), a secondary aim of the present study was to investigate whether and how the outcomes of our mediation model differ among individuals with different patterns of CM. To address this secondary aim, we employed a LCA. While our primary analyses addressed whether the proposed model applies in general, the LCA allowed us to examine whether the mechanisms in the proposed mediation model behaved differently for different patterns of CM. In this way, the LCA complements our primary analyses.
A few studies used LCAs to categorize CM experiences from a person-centered perspective and found four distinct classes differing in severity and variety of CM (e.g., Charak & Koot, 2015; Shin et al., 2018). However, to our knowledge, no study has included the tendency to minimize CM in this kind of analysis (Church et al., 2017). Since we consider minimization to be closely related to CM as well as to CM types, we included minimization in our LCA, and tested how latent classes differ in terms of dissociation, vulnerable narcissism, and grandiose narcissism. Our expectation was that classes with CM would display higher levels of dissociation and higher levels of both types of narcissism than classes with no CM (Howell, 2003; Talmon & Ginzburg, 2018, 2019). In case the LCA would identify a class displaying high levels of minimization, we also expected that individuals in this class would display elevated levels of dissociation as compared to classes with neither CM nor minimization.
Our focus on women was motivated by the fact that although both types of narcissism are prevalent in men and women (Grijalva et al., 2015), previous research has particularly focused on men (e.g., Krusemark et al., 2018; Walters & Horton, 2015). Therefore, little is known about narcissism in women in general, and especially about the role CM might play in the etiology of narcissism in women.
Method
Sample and Procedure
A community sample of 337 Israeli adult women was recruited. The inclusion criteria consisted of being Hebrew-speaking and being 18 years of age or older. 15 participants were excluded from analyses because they completed questionnaires too quickly (<7 minutes), so the final sample size was 322. Participants were recruited via social media platforms and were given the opportunity to take part in a gift card voucher lottery as a compensation for their study participation. Data were collected after receiving approval from Tel Aviv University’s Institutional Review Board (IRB), and obtaining informed consent from the participants (i.e., a full explanation of the study protocol before participating). Participants used Qualtrics Research Software to complete the questionnaires online, which were presented in a randomized order.
The average age of participants was 31.51 (SD = 6.24) years. Two thirds of participants indicated that they were in a relationship. Half of the participants had children (53.9%). 30.7% of participants reported a socioeconomic status below average, 22% indicated a socioeconomic status far below average, 18.3% average, 25.4% above average and 3.7% far above average. On average, participants had 16.04 (SD = 2.93) years of education.
Measures
Childhood maltreatment. CM was assessed using the Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998). The CTQ is a retrospective self-report measurement and consists of 28 items. It assesses five kinds of CM: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. Each of the subscales consists of 5 items. All items are rated on a 5-point Likert-type scale with response options ranging from 1 (never true) to 5 (very often true). Bernstein and Fink (1998) suggest building a sum score of all items of the subscales with higher scores representing higher levels of CM. Accordingly, the sum scores range from 25 to 125. Bernstein and Fink (1998) demonstrated high structural validity (via confirmatory factor analysis) and high convergent validity of the CTQ (via positive correlations with therapists’ ratings (r = .36–.75) and with Childhood Trauma Interview Severity Ratings (CTISR; r = .42–.58). Bernstein et al. (2003) reported an internal consistency of .92. Cronbach’s alpha in the current study was .94. Cronbach’s alpha for the subscale measuring emotional abuse was .86, for physical abuse it was .86, for sexual abuse it was .90, for emotional neglect it was .89, and for physical neglect it was .71. The following cutoff values for the CTQ sum scores have been suggested by Bernstein and Fink (1998): no (to minimal) CM: 25–36, low (to moderate) CM: 37–51, moderate (to severe) CM: 52–68, and severe (to extreme) CM: 69–125. In the present study, we only used these cutoff scores to describe the distribution of CM in our sample. In all other analyses we used continuous scores of the CTQ. In addition to the subscales assessing different types of CM, the CTQ contains a Minimization/Denial scale (MD, 3 items) measuring the tendency to deny or minimize maltreatment experiences (e.g., “I had the perfect childhood.”; Bernstein & Fink, 1998). The scoring of the MD follows a dichotomizing procedure: individuals who rate an item of the MD with 5 (very often true) are credited 1 for this item, all other answers get the value 0. Consequently, the MD ranges from 0 to 3 (Bernstein & Fink, 1998). MacDonald et al. (2016) reported a Cronbach`s alpha of .68 for the MD. Cronbach`s alpha for the MD was .75 in the current study.
Narcissism. Narcissism was assessed using the Brief-Pathological Narcissism Inventory (B-PNI; Schoenleber et al., 2015). The B-PNI consists of 28 items reflecting two subscales: narcissistic vulnerability (e.g., “When people don’t notice me, I start to feel bad about myself,” “When others don’t meet my expectations, I often feel ashamed about what I wanted”) and narcissistic grandiosity (e.g., “I find it easy to manipulate people,” “I often fantasize about performing heroic deeds”). All items are scored on a 6-point Likert-type scale, ranging from 0 (not at all) to 5 (very much like me). We used mean scores for each scale, with higher scores representing greater levels of each type of narcissism (Schoenleber et al., 2015). Schoenleber et al. (2015) demonstrated a high structural validity (via confirmatory factor analyses) and convergent validity (via positive correlations with the full inventory of PNI and other narcissism measures). The reported internal consistency was .93 for vulnerability and .86 for grandiosity (Schoenleber et al., 2015). Cronbach’s alphas for the current sample were .94 for vulnerability .90 for grandiosity.
Dissociation. Dissociation was assessed by the Dissociative Experiences Scale (DES; Bernstein & Putnam, 1986). The DES is a 28-item self-report questionnaire asking participants to indicate the percentage of time they experienced each symptom of dissociation in their daily life (e.g., “Some people find that sometimes they are listening to someone talk and they suddenly realize that they did not hear all or part of what was said,” “Some people are told that they sometimes do not recognize friends or family members”, Bernstein & Putnam, 1986). The DES has three subscales: amnesia, depersonalization, and absorption. Since the subscales were highly correlated (r = .72–.73, p = .003) we used the overall mean score with higher scores representing higher levels of dissociation (Dubester & Braun, 1995, for analyses with the DES subscales see SM). While scores above 30 are suggestive for a dissociative disorder in clinical samples (Bernstein & Putnam, 1986; Carlson & Putnam, 1993; Frischholtz et al., 1990), scores above 20 indicate a substantial number of dissociative experiences in nonclinical samples (Ross et al., 1988, 1990). Support for the scale’s concurrent validity was set by comparing its scores with clinical diagnosis of dissociative disorders (Carlson & Putnam, 1993; Dubester & Braun, 1995). Researchers report high reliability of the DES (retest reliability over 4 weeks of .96, split-half reliability of .83–.93, and internal consistency of .95, Bernstein & Putnam, 1986; Carlson & Putnam, 1993; Frischholtz et al., 1990; Pitblado & Sanders, 1991). Cronbach’s alpha of the DES for the current sample was .93.
Data Analysis
We started with descriptive analyses by checking the distribution of CM in the sample. We then calculated bivariate correlations between the study variables.
In order to examine the primary hypothesis, we ran a mediation analysis with the SPSS macro PROCESS (Hayes, 2012) to test whether the link between CM and both vulnerable and grandiose narcissism travel through dissociation. For this purpose, we only included the CM general score as a predictor and the DES general mean as a mediator. Nevertheless, we also conducted both mediation analyses with the DES subscales as mediators (see SM).
Our secondary analysis was to conduct LCA with reference to the CM types and the MD using Mplus. The common criteria used to identify the model that fits best with the data are highest log-likelihood, lowest Bayesian Information Criterion (BIC), highest entropy, BLRT, and LMR-A p-values smaller than .05 (Field, 2013; Hagenaars & McCutcheon, 2002). Among these indices, BIC, which allows to evaluate different models relatively to each other, is considered to be the best indicator for goodness of fit and therefore, is the most important criterion when choosing between different models that result from LCA (Nylund et al., 2007). Entropy ranges from 0 to 1 with values close to 1 suggesting a clear delineation of classes (Celeux & Soromenho, 1996). Our next step was to compare levels of dissociation and each type of narcissism between the classes that resulted from the LCA. We did that by conducting Kruskal–Wallis tests with Dunn’s pairwise comparisons. Our final step was to conduct two multinomial mediation analyses with the class-variable as the predictor, dissociation as the mediator, and each type of narcissism as the outcome.
Results
Preliminary Analyses
Adhering to the cutoff values for the CTQ sum scores suggested by Bernstein and Fink (1998), most of the participants reported no CM (61.3%). In total, 24.8% of subjects indicated low CM levels, 7.4% indicated moderate CM levels, and 6.5% indicated severe CM levels. Age was positively correlated with CM levels (r = .12, p = .03), whereas socioeconomic status was negatively correlated with CM (r = –.12, p = .03). Therefore, all of the following analyses were conducted controlling for age and socioeconomic status. There was no association between CM and years of education (r = –.06, p = .30), relational status (t(321) = .53, p = .60), or number of children (t(321) = .28, p = .78).
The correlations among the study variables are presented in Table 1. As can be seen, the correlation between vulnerable and grandiose narcissism was .60 (p < .001). We found high positive correlations among the CM types (r = .38–.71). Minimization was found to be negatively correlated with CM (r = –.23, p < .001). Moreover, minimization exhibited negative associations with vulnerable (r = –.17, p < .001) and grandiose narcissism (r = –.15, p < .001). No significant correlations between minimization and dissociation were found (r = –.01, p = .99).
Descriptive Statistics and Pearson’s Correlations Among Study Variables.
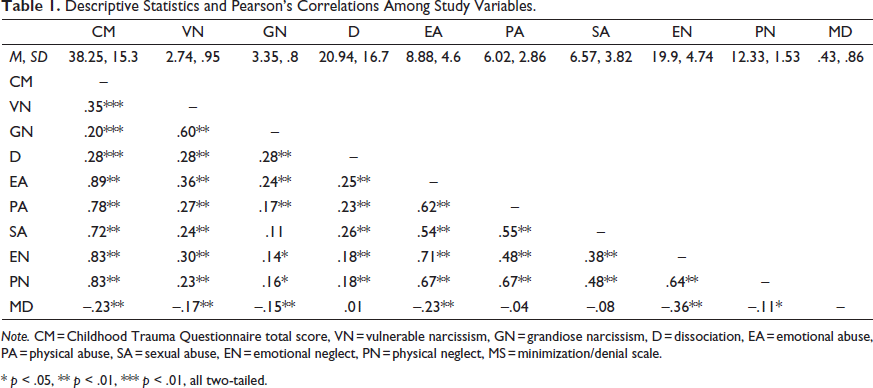
Note. CM = Childhood Trauma Questionnaire total score, VN = vulnerable narcissism, GN = grandiose narcissism, D = dissociation, EA = emotional abuse, PA = physical abuse, SA = sexual abuse, EN = emotional neglect, PN = physical neglect, MS = minimization/denial scale.
* p < .05, ** p < .01, *** p < .01, all two-tailed.
Primary Analyses
Primary analyses revealed positive correlations between CM and vulnerable narcissism (r = .35, p < .001), grandiose narcissism (r = .20, p < .001), and dissociation (r = .28, p < .001) (Table 1). Among CM types, emotional abuse correlated most strongly with both phenotypes of narcissism and dissociation. The correlation between CM and vulnerable narcissism was significantly higher than the correlation between CM and grandiose narcissism (z = –3.25, p < .001).
According to the mediation analysis, dissociation mediates the link between CM and both phenotypes of narcissism. With vulnerable narcissism as a dependent variable, the model explained 18% of the variance, while the indirect effect through dissociation was significant (p < .001) and explained 1.1% of variance in vulnerable narcissism (Figure 1). Applied to grandiose narcissism, the same model explained 11% of the variance, while the indirect effect through dissociation was significant (p < .001) and explained 1.4% of variance (Figure 2). Both mediation analyses were also conducted without covariates as well as with the subscales of the DES. The results of these analyses can be found in the supplemental materials.
Secondary Analyses
Since BIC—which is typically viewed as the best indicator of goodness of fit in LCA (Nylund et al., 2007)—was lowest in the 5-class model (BIC = 8167.42, see Table 2), we preferred the 5-class model to the others, even though it was not significant (p = .17) and some classes had very small proportions (see Frost et al., 2020; Warmingham et al., 2019). A high entropy value probability of 0.97 in the 5-class model lends support to this decision by suggesting adequate latent class separation in the 5-class model. Another reason for choosing the model with 5 classes was that the different classes considerably differed in their CM patterns, highlighting the importance of distinguishing at least five classes. However, models with 6 and more classes did not reveal interpretable classes with different CM patterns. Therefore, we decided to focus on the 5-class model. Detailed results of the LCA are summarized in Table 2.
Latent Class Analyses and Fit Indices.
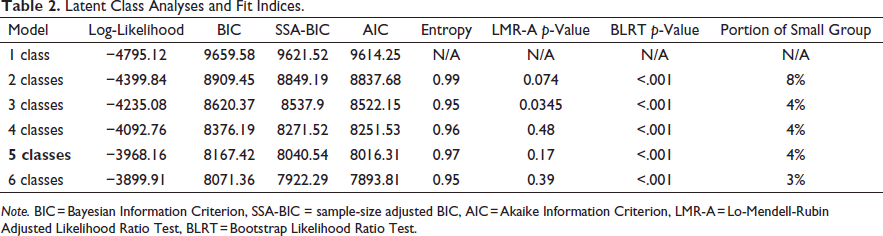
Note. BIC = Bayesian Information Criterion, SSA-BIC = sample-size adjusted BIC, AIC = Akaike Information Criterion, LMR-A = Lo-Mendell-Rubin Adjusted Likelihood Ratio Test, BLRT = Bootstrap Likelihood Ratio Test.
Overall, 65.5% (n = 211) of participants were classified as the first class (no or minimal maltreatment and no minimization, in the following referred to as “healthy class”); 11.5% (n = 37) were classified as the second class (no or minimal maltreatment and high minimization, in the following referred to as “minimization class”); 3.4% (n = 11) were classified as the third class (high maltreatment and no minimization, in the following referred to as “high CM class”), 6.2% (n = 20) were classified as the fourth class (high sexual abuse and moderate emotional abuse, in the following referred to as “sexual abuse class”) and 13.7% (n = 44) were classified as the fifth class (high emotional abuse, high emotional neglect and moderate physical neglect, in the following referred to as “emotional maltreatment class”). The distributions of CM types for the five classes can be found in the supplemental material.
We used Dunn’s tests to calculate pairwise comparisons and found the following differences among the classes (for detailed results see supplemental material). In doing so, we adjusted p-values by the Bonferroni correction for multiple testing, meaning p was multiplied by the number of tested hypotheses m, in this case m = 10.
The healthy class scored significantly lower regarding vulnerable narcissism than the high CM class (z = –3.67, p = .003, one-tailed) and the emotional maltreatment class (z = –2.82, p = .02, one-tailed). Furthermore, the healthy class displayed significantly less dissociation than the high CM class (z = –3.53, p = .001, one-tailed) and the sexual abuse class (z = –2.66, p = .04, one-tailed). The minimization class reported significantly lower scores on vulnerable narcissism compared to the high CM class (z = –3.67, p = .003, one-tailed), the sexual abuse class (z = –3.14, p = .01, one-tailed), and the emotional maltreatment class (z = –3.90, p = .001, one-tailed). The minimization class displayed lower grandiose narcissism scores than the emotional maltreatment class (z = –3.33, p = .005, one-tailed). Moreover, the minimization class scored significantly lower in dissociation than the high maltreatment class (z = –3.23, p = .005, one-tailed). The distributions of vulnerable and grandiose narcissism within the classes are illustrated in Figure 3. Figure 4 illustrates the class-wise distributions of dissociation.
According to our multinomial mediation analysis, the class-variable exhibits an indirect effect on vulnerable narcissism through dissociation when comparing class 1 and 3 (p = .007), as well as when comparing class 1 and 4 (p = .02, see SM). While the whole model explained 17% of the variance, the indirect effect of the class-variable accounted for 7% of the variance in vulnerable narcissism. Applied to grandiose narcissism, the same model explained 12% of the variance, while the indirect effects through dissociation were significant when comparing class 1 and 3 (p = .01) as well as when comparing class 1 and 4 (p = .03). The indirect effect of the class-variable through dissociation explained 3% of the variance in grandiose narcissism (see SM).
Discussion
To the best of our knowledge, this study represents the first report on the mediating role of dissociation in the link between CM and both vulnerable and grandiose narcissism. In addition, a latent class approach allowed us to distinguish five classes of CM experiences that were differentially associated with dissociation, vulnerable narcissism, and grandiose narcissism.
Childhood Maltreatment and Narcissism
Our findings suggest an association between CM and both types of narcissistic traits. However, we found that CM is more strongly correlated with vulnerable narcissism than with the grandiose variant. This finding is supported by previous studies (e.g., Keene & Epps, 2016; Nehrig et al., 2019; Talmon & Ginzburg, 2019), suggesting that CM and vulnerable narcissism are more closely coupled than CM and grandiose narcissism.
One interpretation of these findings is that especially vulnerable but also grandiose narcissism represent strategies for coping with CM. Both involve internal ways to inflate the self as well as to seek external means for the same purpose. The perpetuation of these behavioral patterns in adulthood can manifest in pathological vulnerability, dependence, and hypersensitivity to criticism. These are core features of vulnerable narcissism as well as in grandiose fantasies about the self while expecting admiration by the external world, namely narcissistic grandiosity (Howell, 2003; Keene & Epps, 2016; Talmon & Ginzburg, 2018).
The Mediating Role of Dissociation
The current findings support the idea that dissociation partly mediates the link between CM and both types of narcissism. To understand why dissociation plays a role in the relation between CM and both vulnerable and grandiose narcissism, one might consider the sense of betrayal towards the child, which is common in cases of CM (Freyd, 2008).
More specifically, Freyd (2008) argues that children in abusive environments need to minimize this sense of trust violation by their caregivers. Thus, children have to suppress their emotions and behavioral impulses, and to do so, they might dissociate from the abusive reality (Blizard, 1997; Bromberg, 1994; Ferenczi, 2018; Freyd, 2008; Howell, 2003). As a result, the intense attachment to their internal world might contribute to a sense of self-focus, self-centeredness and a lack of empathy towards others, which are core features of both vulnerable and grandiose narcissism (Howell, 2003). In this way, dissociation could mediate the link between CM and both types of narcissism, as suggested by Howell (2003). In fact, Howell (2003) suggests that two distinct dissociative states (i.e., vulnerable vs. grandiose dissociative self-states) might underlie the link between CM and each phenotype of narcissism.
However, since the DES did not allow us to measure vulnerable and aggressive dissociative self-states as proposed by Howell (2003), we can only lend support for the hypothesis that the link between CM and both types of narcissism is mediated by dissociative experiences measurable by the DES, and that the mediating role of the subfacet absorption is the greatest (see SM). To lend support for Howell’s (2003) specific model, future studies should develop and consider measures assessing vulnerable and grandiose facets of dissociation specifically.
Differentiating Experiences of Childhood Maltreatment
While the results of our mediation analyses suggest that the links between CM and both types of narcissism travel partly through dissociation, the results of the LCA suggest caution in interpreting these findings. Besides the healthy class, the inclusion of the MD in the LCA uncovered another group of individuals with apparently no CM experiences: those who scored low on the CTQ and high on the MD. Interestingly, these individuals did not differ from the healthy class in terms of dissociation and narcissism. If individuals in this class minimize actually experienced CM, the finding that these individuals did not display enhanced levels of dissociation and narcissism as compared to the healthy class would be inconsistent with Howell’s (2003) hypothesis. It is possible that individuals in this class use other strategies for coping with their CM experiences besides dissociation and narcissism.
Future research is necessary to understand this potential coping strategy in the context of CM and to examine factors that determine which strategy is used to cope with each type of CM. Since we could not find any report on the construct validity of the MD, future studies may use other, validated instruments to assess minimization. These studies may also consider objective ways to assess CM (e.g., official records) to ensure that CM experiences are assessed fully and are unbiased (i.e., without minimization).
By exploratively conducting both primary mediation analyses also with the latent class-variable as the predictor, we found that the indirect effect of the class-variable on both types of narcissism through dissociation only occurs when comparing the healthy class with the high CM class and when comparing the healthy class with the sexual abuse class. These findings suggest caution in using a general score of CM or strictly divide CM into subtypes when examining longer term sequelae in research but also in clinical contexts. As for research purposes, novel approaches such as LCA are needed allowing to differentiate CM experiences and to classify them based on shared patterns. As for clinical purposes, we provide detailed implications of our findings below.
Clinical Implications
In patients reporting CM experiences, Howell’s model seems to apply. The tendency to dissociate from CM and to form a narcissistic self could point to a unique way of coping with CM and may have relevant effects on the therapeutic process and relationship. Therapists treating patients that suffer from Narcissistic Personality Disorder could conceptualize their case by focusing on the violated self behind a narcissistic personality, namely, one that results from the attempt to deal with CM. Furthermore, therapists should be aware that CM experiences can be “deleted,” meaning that although they may be inaccessible to the conscious memory of the patient, they may still lead to clinical symptoms (Hagenaars et al., 2011). Additionally, the classification of CM into emotional, physical, and sexual abuse as well as emotional and physical neglect may draw attention away from shared clinical outcomes of different CM types. Thus, we suggest clinicians take even low general scores of CM in routine diagnostics as a reason to examine CM experiences individually and in-depth to get an impression of their impact in the patients’ symptoms. Furthermore, we encourage clinicians to include measures of minimization when assessing CM. Minimization may not only make the assessment of CM more challenging, but it may also have implications for the therapeutic treatment, relationship, and outcomes.
Limitations and Future Directions
The present study has a number of strengths, including the large sample size appropriate to examine the intended effects, as an a priori power analysis demonstrated. Nevertheless, the findings of this study should be considered in the light of its limitations.
First, since the present study is cross-sectional and reports on adulthood outcomes, we could only use retrospective self-reports of CM. Although recent research highlights the importance of subjective evaluation in the field of childhood maltreatment (Danese & Widom, 2020), report or response biases are possible. Future studies in this context should assess and take into account the levels of minimization and dissociation in their sample when interpreting CM reports. To address this specific limitation, future studies may assess CM via objective data such as official records. In light of the limitations of the present study, causal inferences are not possible. However, these findings may lay the groundwork for future longitudinal studies in this field. These studies may also screen participants for PTSD symptoms to control for them as these could influence study outcomes. While significant characteristic differences among the classes that resulted from the LCA support the uniqueness and distinctiveness of each class, some classes were very small in size. Future studies may aim to replicate the present findings with larger sample sizes. Although the mode we used to recruit participants for this study (social media platforms, particularly Facebook) enabled us to include participants who differed in socioeconomic status, race, ethnicity, religion, and culture, a further limitation is the fact that only women were included. Although this approach is supported by previous work in this area (Alexander, 2011; Martinez-Torteya et al., 2014), it decreases the ability to generalize our findings. Indeed, previous findings suggest that childhood abuse is related to both types of narcissism in females, while childhood abuse is not related to either of the types in males (Ensink et al., 2018). In addition to gender, the current sample might have some special characteristics such as the military service mandatory for all Israeli including women, religion-related aspects of education, or the high percentage of individuals living in urban areas that might further limit the generalizability of the present findings to other populations. To address these potential limitations, future studies may aim to assess the patterns of relation between CM, dissociation, and narcissism beyond genders, as well examining other cultural and religious contexts.
In sum, our findings suggest the important role of CM in the etiology of both phenotypes of narcissism and point to dissociation as one interesting candidate to link these two phenomena. Furthermore, they highlight two major factors in this pattern of relation: the impacts of different experiences of CM and the tendency to minimize CM. Both should be assessed and taken into account when diagnosing and treating childhood trauma and pathological narcissism.
Supplemental Material
Supplemental Material - Childhood Maltreatment and Narcissism: The Mediating Role of Dissociation
Supplemental Material for Childhood Maltreatment and Narcissism: The Mediating Role of Dissociation by Nina Bertele, Anat Talmon, James J. Gross, in Journal of Interpersonal Violence
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.