
Abstract
Existing studies show a mixed relationship between intimate partner violence (IPV) and contraceptive use. This study assesses the association between women’s exposure to IPV and contraceptive use in India. Furthermore, we aim to determine whether husband’s controlling behaviors play a moderating role in the IPV-contraception link. We used nationally representative data from the recent round of the National Family Health Survey (NFHS-4), conducted in 2015-2016. In this study, the use of contraceptives is the outcome variable, categorized into three groups: no/traditional methods, modern methods, and female sterilization. Women’s exposure to IPV in the past year is the key exposure of interest. Socio-economic and demographic variables were used as covariates. Multinomial logistic regression models were performed to examine the association between women’s exposure to IPV and contraceptive use. Of the total participants (N = 58,891), approximately one in every four women (24.1%) experienced any form of IPV in the past year. Slightly over half (50.8%) reported using either traditional methods of contraception or no contraceptive at all. About 14% of the respondents were using modern methods of contraception and 34.9% had undergone sterilization. After controlling for confounding factors, women who experienced IPV were 8% (95% CI [.87, .99]) less likely to report using modern contraceptives than those who did not face any IPV. Conversely, women who faced IPV were 14% (95% CI [1.09, 1.20]) more likely to undergo sterilization. Furthermore, women who experienced any form of IPV and whose husbands endorse controlling attitudes were 12% (95% CI [.81, .95]) less likely to report using modern contraceptives and 11% (95% CI [1.04, 1.17]) more likely to undergo sterilization. Interventions should be made to prevent violence against women that would increase their ability to choose appropriate contraception methods to avoid unintended pregnancies.
Keywords
Introduction
Violence against women is a global public health issue, and a violation of human rights and gender equality (Ellsberg et al., 2001; Heise, 1993; WHO, 2019). Women are subject to different forms of violence even before their birth and until their last breath. Intimate partner violence (IPV) is the most common form of violence against women perpetrated by the partner (Krug et al., 2002). Violence against women is an unfortunate reality and occurs in almost all countries across the world. It is estimated that around one in every third woman worldwide experiences physical and/or sexual violence committed by the partner in their lifetime (Devries et al., 2013; García-Moreno et al., 2006). Despite several efforts to protect the human rights of girls and women, the prevalence of IPV remains unacceptably high in India, with approximately 31% of ever-married women in this country experienced violence by their partners in 2015-2016 (International Institute for Population Sciences [IIPS] & ICF, 2017).
Domestic violence threatens the dignity, autonomy, economic opportunities, and health status (physical and physiological health) of women that adversely impact their lives (Ahmed et al., 2006; Campbell, 2002; Ellsberg et al., 2008; Heise et al., 1994). Evidence suggests that women’s exposure to violence is associated with physical injury, adverse pregnancy outcomes (e.g., low birth weight of babies), maternal morbidity and mortality (Abdollahi et al., 2015; Krug et al., 2002), sexually transmitted infections (Kouyoumdjian et al., 2013; Li et al., 2014), depression, anxiety, suicidal thoughts and attempts, and post-traumatic stress disorders (Devries et al., 2011; Mapayi et al., 2013; Rogathi et al., 2017; Varma et al., 2007). It also impacts intergenerational health outcomes, such as nutrition, morbidity, and mortality in children (Ahmed et al., 2006; Mondal & Paul, 2020; Paul & Mondal, 2020).
Several studies have documented the impact of the interference of abusive husbands on wives’ access to family planning services (Bergmann & Stockman, 2015; Kaye et al., 2006; Stephenson et al., 2008). In the existing literature, there are indications of a strong but heterogeneous relationship between the IPV and the use of contraception, especially in the developing part of the world, where both the occurrence of IPV and unmet demand for contraception are high (Kidman et al., 2015; Raj & McDougal, 2015; Raj et al., 2015; Silverman et al., 2020; Stephenson et al., 2013). Evidence in Southern Africa (Kacanek et al., 2013), Uganda (Maxwell et al., 2018), Tanzania (Kabir & Kordowicz, 2020), Jordon (O’Hara et al., 2013), Bangladesh (Salam et al., 2006), India (Chen et al., 2020; Stephenson et al., 2008), and elsewhere (Maxwell et al., 2015; Williams et al., 2008) indicates that women who are subjected to various forms of husband-perpetrated violence are less likely to use modern contraception methods, and thereby putting them at greater risks of unintended pregnancies and childbirth. A recent assessment of the incidence of abortions and unintended pregnancies in India reported that around half of the country’s total 48.1 million pregnancies were unintended (Singh et al., 2018). Most unintended pregnancies increase the risks of maternal and child mortality; these occur because of nonuse or failure of contraception (Pallitto et al., 2013).
On the other hand, studies in sub-Saharan Africa (Alio et al., 2009), Bangladesh (Dalal et al., 2012), New Zealand (Fanslow et al., 2008), Honduras (Kuhlmann et al., 2019), and India (Reed et al., 2016) have found a positive relationship between IPV and contraception use, suggesting that women who are exposed to IPV are more likely to protect themselves from unwanted pregnancies. Recent studies show that women experiencing IPV tend to use more “female-controlled” spacing contraception methods (Chen et al., 2020; Raj et al., 2015), or permanent sterilization (Acharya et al., 2019; Patil et al., 2022).
These conflicting findings reinforce the need for further investigation of the complex relationships between IPV and contraception use. One possible explanation for these inconsistent results is that the influence of IPV on contraceptive use is not categorical (Forrest et al., 2018). There are also other factors in a broad range of contexts, such as cultural, societal, and personal relational context playing moderating roles in this relationship. Husband’s controlling behaviors and domineering attitudes are such moderating factors that may play a significant role in the IPV-contraception link. Studies have observed that women experiencing controlling and dominating behaviors by their husbands are more likely to report interference in the use of contraception than those women who do not experience controlling behaviors (Clark et al., 2008). Further research on the role of husband’s controlling behaviors as a moderating factor in the association between IPV and the use of contraception may improve the understanding and promote appropriate contraception use among reproductive women. To the best of our knowledge, none of the studies have investigated the moderating role of husband’s controlling attitudes in the linkage between IPV and contraception. This present study attempts to fill this gap in the literature by examining husband’s controlling attitudes as a moderating factor in the association between women’s exposure to IPV and contraception use among currently married women in India, using a large-scale nationally representative sample survey.
Conceptual Framework
Violence committed by the husband is seen as a manifestation of control, dominance, and aggressive behaviors against women. Violence against women, physical or other forms, is an extreme form of discrimination linked to a continuum of beliefs that men have the right to control women’s behavior (Heise, 1993; Jewkes et al., 2002). Women are kept under “coercive control” by the husband and remained captive in an unreal world created by the abuser, entrapped in a world of confusion, contradiction, and fear (Stark, 2007). They are made dependent through exploitation, isolation from support, and regulating their everyday behaviors (Chakrabarty, 2018). Abusive behaviors of the partner also restrict the decision-making power of wives in the context of unequal gender norms (Kishore & Johnson, 2004). In patriarchal societies like India, unequal gender norms and discriminatory attitudes might put women at greater risk of control and limit their reproductive choices, thereby serving as a moderating role as they are also a common risk factor for both IPV and contraception use (Jewkes et al., 2010; Mondal & Paul, 2021). Husband’s controlling and domineering behaviors are examples of such aspects that stem from the norms of differential gender roles in society (Dobash & Dobash, 1979; Lips, 1991). It is imperative to investigate whether husband’s controlling and domineering behaviors act as a moderating factor in the association between IPV and the use of contraception methods. It is hypothesized that the use of modern methods of contraception may decrease with women’s exposure to IPV, whereas women’s opting for permanent sterilization may increase, particularly for women whose husbands endorse high controlling and domineering behaviors due to their inability to make choices in spacing methods.
Methods
Data Source
We used data from the latest demographic and health survey of India, known as National Family Health Survey-4 (NFHS-4), conducted in 2015−2016. The NFHS-4 is a nationally representative large-scale sample survey of 601,509 households, 699,686 women aged 15-49 years with a response rate of 97%, and 112,122 men aged 15-54 years with a response rate of 92%. The survey was carried out across all the 29 states and 7 union territories of the country. The information covers a wide range of population and health indicators, such as maternal and child health, fertility, mortality, family planning methods, nutritional status, childhood immunization, noncommunicable diseases, domestic violence, and knowledge and attitudes regarding HIV/AIDS. A stratified two-stage sampling design was applied to select the samples. Based on the 2011 Indian Census enumeration, 28,586 clusters of areas – 8,397 in urban, 20,059 in rural areas, and 130 in slums – were selected in the first stage. The method of probability proportional to size was used for the selection of these clusters. A complete household mapping and listing were done in the selected clusters. In the second stage, 22 households were randomly selected with systematic sampling from every selected rural and urban cluster. A detailed description of the sampling design and survey procedure is provided in the national report of NFHS-4 (IIPS & ICF, 2017).
Study Design and Sample Size
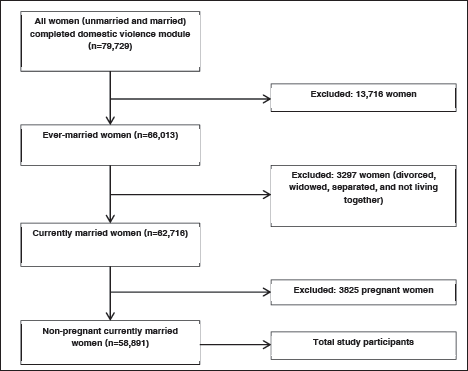
A cross-sectional study design was adopted to assess the association between IPV and contraceptive use among Indian women. Although the NFHS-4 interviewed 699,686 ever-married women aged 15-49 years in the survey, the domestic violence module was only applied to one eligible woman per household randomly selected in agreement with the ethical requirements of the World Health Organization for research on domestic violence (WHO, 2001). At first, 83,397 women were selected in the violence module of this survey. Some women had to be dropped at the time of the survey due to lack of privacy or other reasons, and 79,729 women completed the interview regarding violence, with a response rate of 96%. Complete and valid information about domestic violence committed by the husband was available for 66,013 ever-married women in the NFHS-4 survey. Among them, 58,891 currently married nonpregnant women constitute the final study participants in this research. The pregnant women and women of other than currently married status (e.g., divorced, widowed, separated, and not living together) were excluded. The statistical analysis of this study was performed with 58,891 women that had valid information about outcome variable and exposure variables of interest (Figure 1).
Selection of study participants, NFHS-4 (2015-2016).
Outcome Variable
The outcome variable of this study is the use of contraceptives among currently married nonpregnant women aged 15-49 years at the time of the survey. In the NFHS-4 survey, women were asked whether “they are currently doing something or using any method to delay or avoid getting pregnant.” If any woman responded “yes,” she was further asked about the method that she was using at the time of the survey. For the purpose of the study, the use of contraception was categorized into three groups: (a) no/traditional methods, (b) modern methods, and (c) female sterilization. Women who were not using any method or using traditional methods of contraception, such as withdrawal, rhythm/periodic abstinence were treated into the group of no/traditional methods. The modern methods of contraception include pills, intrauterine devices (IUDs/PPIUDs), injectable male and female condoms, lactational amenorrhea method, diaphragm, Standard Days Method, and foam/jelly. Similarly, female sterilization indicates whether the respondents had undergone permanent sterilization at any point (IIPS & ICF, 2017).
Predictor Variables
Women’s exposure to IPV in the past year is a key predictor variable in this study. In the domestic violence module of the NHFS-4, a series of questions were asked to the women for extracting information regarding violence perpetrated by their current husbands or most recent husbands. All three forms of spousal violence—physical, emotional, and sexual—have been incorporated into the study. As parts of physical violence, each woman was asked: whether her husband ever (a) “pushed her, shook her, or thrown something at her”; (b) “twisted her arm or pulled her hair”; (c) “slapped her”; (d) “tried to choke or burn her on purpose”; (e) “kicked, dragged, or beaten her up”; (e) “punched her with his fist or with something that could hurt her”; and (f) “threaten or attacked with a knife, gun, or any other weapon.” Women had also been asked questions regarding their experience of sexual violence: whether being (a) “physically forced to have sexual intercourse,” (b) “physically forced to perform any other sexual acts,” or (c) “forced with threats or in any other way to perform sexual acts when she did not want to.” Additionally, emotional violence against women by the husband was measured by three questions: whether her husband (a) “humiliated in front of others”, (iii) “threatened to hurt or harm, or (iii) “insulted or made her feel bad about herself.” The experience of all those violence in the past 12 months was captured by three responses: “often,” “sometimes,” and “not at all.” By aggregating these responses, exposure to these three specific forms of violence was estimated: women who responded “often” or “sometimes” to any physical, sexual, or emotional violence questions respectively were categorized as “yes” (coded as ‘1’) and “no” (coded as ‘0’) in a corresponding dichotomous variable about physical, sexual, or emotional violence. Finally, a composite variable of women’s exposure to IPV was also developed by adding the responses from all the above forms of violence and dichotomized as “yes” (1) and “no” (0), where “1” denotes the experience of any form of violence, which includes physical, emotional, and sexual violence, and “0” indicates no experience of violence.
Furthermore, husband’s controlling behaviors were included as a moderating factor in this study. Husband’s controlling behaviors and domineering attitudes were estimated from a set of six questions: whether the husband/partner (a) “becomes jealous if she talks with other men,” (b) “accuses her of unfaithfulness,” (c) “does not permit her to meet her friends,” (d) “tries to limit her contact with family,” (e) “insists on knowing where she is,” and (f) “doesn’t trust her with money.” The responses were recorded as a dichotomous form of “yes” (1) and “no” (0). From these questions, a composite binary variable was computed. Women who reported affirmative responses to any of these controlling attitude questions were considered as controlled by their husbands, and women with no positive responses were considered as not controlled by their husbands.
Confounders
In addition to the main predictors, several important confounding factors were also incorporated in this study that could potentially influence the use of contraception. These factors are socio-economic and demographic characteristics of women.
Socio-economic factors: These factors include the place of residence (urban and rural), caste (Scheduled Caste [SC], Scheduled Tribe [ST], Other Backward Class [OBC], and none of them [forward caste]), religion (Hindu, Muslim, and others), women’s education (no education, primary, secondary, and higher), husband’s education (no education, primary, secondary, and higher), women’s employment status (not working and working), household wealth quintile (poorest, poorer, middle, richer, and richest). It is worthwhile to mention that the wealth quintile is a composite measure of standard of living which is constructed by the survey using the possession of durable assets (e.g., television, car, and bicycle), dwelling characteristics (e.g., flooring materials), and accessibility to the services (e.g., drinking water and sanitation facilities).
Demographic factors: These include the age of women (15-24, 25-34, and 35-49 years), age at marriage (<18 and ≥18 years), parity (none, 1-2, 3-4, and 5+), spousal age gap (husband younger, husband older: 1-5, 6-10, and 11+ years), marital duration (0-9, 10-19, and 20+ years). Moreover, women’s exposure to mass media was also included in the analysis, calculated from the frequency of listening to the radio, reading newspapers/magazines, and watching television, and dichotomized into two groups: “yes” (1) and “no” (0).
Statistical Analyses
Descriptive statistics were carried out to understand the distribution and characteristics of the study population. Cross-tabulation was done to estimate the bivariate percentage of women’s reported use of contraception methods by the predictor variables, and the differences were later tested by Pearson’s chi-square statistic. The sample weight was applied for the estimation of percentage distribution. Then, multinomial logistic regression models were applied to assess the relationship between women’s exposure to IPV and the use of contraception. Additionally, a two-way interaction model between women’s exposure to IPV and husband’s controlling behaviors was performed to determine whether husband’s controlling and domineering attitudes moderated the link between IPV and contraception use. We performed both the crude and adjusted regression models to assess the association between women’s exposure to IPV and the use of contraception. The adjusted regression models were controlled for a range of demographic and socio-economic characteristics of women. The regression results were presented by the relative risk ratio with 95% confidence intervals (CIs), and significance levels were shown by p-values. All the statistical analyses were performed using STATA version 14.0 (StataCorp LP, College Station, TX, USA).
Results
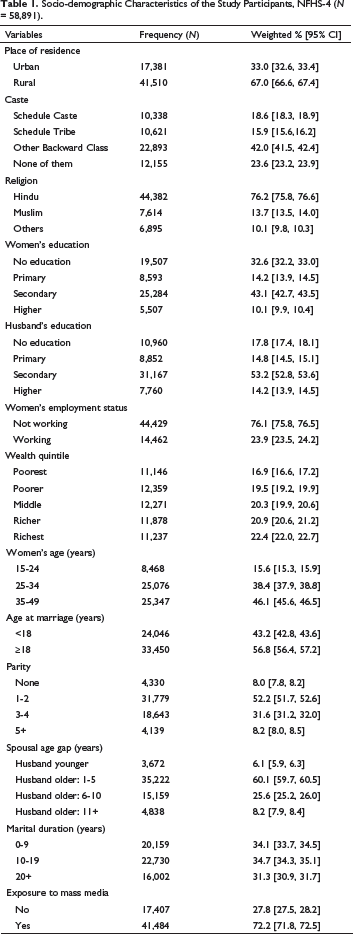
Socio-demographic Characteristics of the Study Participants, NFHS-4 (N = 58,891).
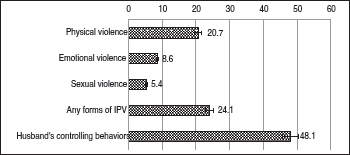
Of the total study participants, 20.7% of women reported the experience of physical violence, 8.6% experienced emotional violence, and 5.4% experienced sexual violence by their partners in the past year. As a matter of fact, nearly one in every four sample women (24.1%) experienced any form of IPV in the past year. Approximately half of women (48.1%) reported experience of controlling and domineering attitudes by the husband (Figure 2).
Prevalence of various forms of IPV and husband’s controlling behaviors.
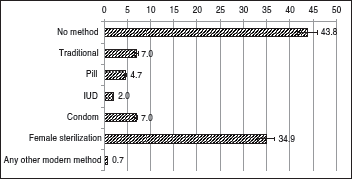
Slightly over half of the respondents (50.8%) were either not using any method or using traditional methods of contraception. About 35% of women had undergone sterilization. With regards to the modern methods of contraception, 4.7% were using pills, 2% were using IUDs, and 7% reported using condoms at the time of the survey (Figure 3).
Percentage of contraceptive use among the study participants.
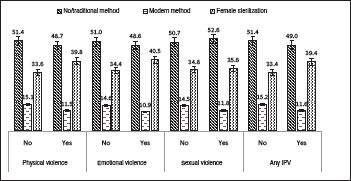
The current use of modern contraceptives was significantly lower among those women who experienced physical, emotional, or sexual IPV in the past year. On the other hand, women who experienced IPV were more likely to be sterilized than those who did not encounter any form of IPV (Figure 4).
Percentage of contraceptive use by various forms of IPV.
Contraceptive Use by Socio-demographic Characteristics of the Respondents, NFHS-4.

Multinomial Logistic Regression Models Assessing the Association of IPV and Other Socio-demographic Covariates with Contraception Use of Women (Base Outcome: No/Traditional Methods of Contraception).

Note. RRR = relative risk ratio; ref = reference category.
Our study also revealed that several socio-demographic factors were significantly associated with the use of modern contraceptives and female sterilization. The use of modern contraceptive was higher among women belonged to the “forward castes” and Muslims. Among many socio-demographic factors, spousal education and household wealth status were found to be important predictors of modern contraceptive use. Compared to women with no education, higher educated women were 25% more likely to use modern methods of contraception. Nevertheless, husband’s education seems to be less important than women’s education for using modern contraceptives. Household wealth status was positively correlated with the use of modern contraceptives in which the richest women were more than twice as likely to use modern methods of contraception than the poorest quintile women. Besides, the respondents having five or more children were associated with a five-fold increased likelihood of modern contraceptive use and 29 times more likely to undergo sterilization. Furthermore, a larger spousal age gap, longer marital duration, and exposure to mass media were found to be positively correlated with female sterilization (Table 3).
Interaction Analysis Showing the Influence of Women’s Exposure to IPV and Husband’s Controlling Behaviors on Contraceptive Use of Women (Base Outcome: No/Traditional Methods of Contraception).
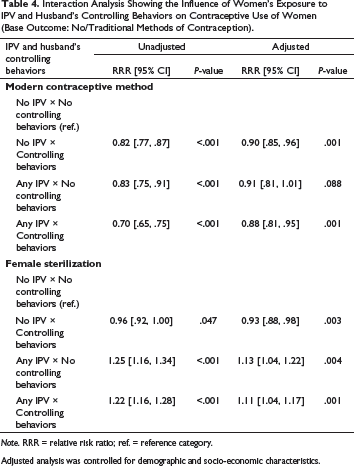
Note. RRR = relative risk ratio; ref. = reference category.
Adjusted analysis was controlled for demographic and socio-economic characteristics.
Discussion
This study investigates the association between women’s experience of IPV and contraceptive use, controlling for a wide range of socio-demographic confounding variables. Also, we attempt to determine whether husband’s controlling and domineering attitudes play a moderating role in the association between IPV and contraceptive use. The findings of this study indicate that women who experienced any form of IPV were less likely to use modern contraceptives. The lower use of modern contraceptives is even more pronounced when women confront both IPV and the controlling attitudes of the husband. Previous studies conducted in India reported similar results where physical violence perpetrated by the husband was associated with a lower likelihood of modern contraceptive adaptation (Stephenson, 2006; Stephenson et al., 2008, 2013). Although studies on the relationship between husband’s controlling attitudes and contraceptive use are sparse, few studies have found a strong negative association between husband’s gender-role attitudes and contraceptive use (Clark et al., 2008; Stephenson et al., 2006).
Violence perpetrated by partners is regarded as an expression of power, supremacy, and abusive acts against wives. IPV threatens the health and well-being of women by undermining their role in personal and household decision-making. It is evident that women who experienced IPV are more likely to be disempowered (Kishor & Johnson, 2004). Given that abused women have low levels of decision-making autonomy and lack of self-efficacy, their ability to make choices in adopting contraception is often restricted. Therefore, women who faced violence are less motivated to use modern methods of contraception that further put them at a greater risk of unintended pregnancies (Raj & McDougal, 2015; Stephenson et al., 2008). The current study reveals that controlling attitudes of the husband play a moderating role in the association between women’s exposure to IPV and contraception use, indicating that women who experience violence and whose husbands endorse domineering attitudes may have greater difficulties in contraceptive use to accomplish their fertility aspirations. Our recent study in India found that husband’s controlling behaviors are strongly associated with an increased risk of domestic violence against women (Mondal & Paul, 2021). Therefore, IPV and controlling attitudes of the husband are intermeshed into one another to achieve patriarchal goals. According to the feminist theory, under patriarchal social structures, men occupy superior positions, and women are expected to have subordinate and inferior positions—this power imbalance results in controlling and dominating behaviors of men against women (Dobash & Dobash, 1971; Lips, 1991). Accordingly, men commit spousal abuse and endorse domineering attitudes to control women and adhere to marital regulations within patriarchal systems.
Nevertheless, previous studies conducted in India and other countries have found mixed associations between husband-perpetrated violence and contraceptive use. For instance, a study conducted in rural Maharashtra of India found that women who experienced physical IPV were less likely to use condoms and more likely to use the IUD method (Chen et al., 2020). Similarly, a previous study conducted in India showed a weak relationship between IPV and contraceptive use, which indicates that women’s exposure to IPV had no significant association with modern methods of contraceptive use (Forrest et al., 2018). A study conducted in Bangladesh, India, and Nepal reported that women who were exposed to sexual violence were more than twice as likely to use modern contraceptive methods than those who did not face sexual IPV (Raj & McDougal, 2015). Another study by Raj et al. (2015) in South Asian countries also found similar results. A study conducted by Dalal et al. (2012) in Bangladesh suggests that women’s experience of IPV was associated with a greater use of contraception. Some of the earlier studies conducted in African countries (Alio et al., 2009; Okenwa et al., 2011) and New Zealand (Fanslow et al., 2008) also exhibit a positive association between women’s exposure to IPV and contraceptive use. There could be several reasons for the inconclusive relationship in those previous studies. This may partly be explained by the cultural or regional differences of these countries. Another could be the methodological complexities adopted in these studies, in which some studies considered both traditional and modern methods of contraception aggregately as contraceptive use in the analysis. Abused women may act differently in using various methods of contraceptives due to reproductive coercion by the husband. Besides, women who experienced IPV might have used contraceptives in the past, and they are more likely to be discontinued and are not using at the time of the survey (Kishor & Johnson, 2004). There is an emerging body of literature that examined the relationship of women’s IPV experience and contraceptive use by type, such as “male-controlled” (e.g., condom, periodic abstinence/rhythm, and withdrawal) and “female-controlled” (e.g., pill, IUD, and injectable) contraceptives. Studies have found a strong positive link between IPV and “female-controlled” contraceptives use (Chen et al., 2020; McDougal et al., 2020; Reed et al., 2016). Further, more comprehensive research is necessary to explore the relationship between spousal violence and various types of contraceptive use.
There is also a growing body of research that established the linkage between IPV and contraceptive discontinuation. In Nigeria, women who experienced IPV had an elevated risk of contraceptive discontinuation (Kupoluyi, 2020). A multicountry study using Demographic Health Survey (DHS) data found inconsistent results in the association between various forms of IPV and contraceptive discontinuation behaviors, indicating country-specific associations (MacQuarrie et al., 2016).
Our study also found that women who experienced IPV were more likely to undergo sterilization, even after adjusting for confounding variables. However, the strength of this association is slightly reduced when husbands endorse controlling and domineering attitudes toward their wives. An earlier study conducted in India using NFHS-3 (2005-06) data also found that domestic violence victimized women were less likely to be sterilized than their nonvictimized counterparts (Patil et al., 2022). Notwithstanding, several previous studies have found inconsistent results regarding the association between women’s exposure to IPV and female sterilization. A study conducted in South Asian countries showed that physical marital violence was positively associated with sterilization, whereas women who experienced sexual violence were less likely to be sterilized (Raj et al., 2015). Forrest et al. (2018) found that women’s experience of IPV was associated with a lower likelihood of undergoing sterilization if women intend to use contraceptives.
In India, the rate of female sterilization is high, which accounts for about two-thirds of all contraceptive use (IIPS & ICF, 2017). In patriarchal contexts like India, it is very difficult for women to take personal and household decisions owing to male supremacy and power imbalance that undermines the reproductive choices of women (Bhasin, 1993). Moreover, difficulties in contraceptive choices heighten when women face domestic violence, which triggers victimized women to opt for permanent sterilization. In conservative cultural parts of India, son preference and early marriage practices remain pervasive (Pande & Astone, 2007; Paul, 2020). Abused women in such conservative settings may choose to go through the process of early childbearing and opt for permanent sterilization.
The observed associations between socio-demographic factors and contraception use and female sterilization are expected, which are consistent with the results of several previous studies. Rural women were more likely to opt for sterilization than urban women. Compared to Hindu women, Muslim women were more likely to use modern contraceptives and less likely to opt for sterilization. Women’s education was positively associated with modern spacing methods and negatively associated with female sterilization. Husband’s education was also associated with a lower probability for female sterilization. However, husband’s education appeared to be less important for spacing methods. Women from the wealthier economic groups were more likely to use modern contraceptives and opt for sterilization than those from the poorest economic status. Similar findings have been reported in other studies of India (Patil et al., 2022; Stephenson et al., 2013).
Women who got married at 18 years or above were more likely to use spacing methods and less likely to opt for sterilization than those married before 18 years. Parity had a strong positive influence on both modern spacing methods and irreversible sterilization. A larger spousal age gap and longer marital duration increased the probability of opting for sterilization among women. Furthermore, women who had exposure to mass media were more likely to adopt spacing methods and permanent sterilization.
The strength of this research is that we used a range of socio-economic and demographic factors as controlling variables to determine the observed association between women’s experience of IPV and contraceptive use using nationally representative samples. Besides, we assessed the moderating role of husband’s controlling attitudes in the association between women’s exposure to IPV and contraceptive use that would expand the understanding in the IPV-contraception link and inform the policymakers to make target-based interventions for abused women.
Although our research has made valuable contributions to the emerging literature on the relationship between IPV and contraceptive use, the study is not free from limitations. First, the information on husband-perpetrated violence is retrospective (experience in the past year). Therefore, the potential recall bias in reporting IPV could not be denied. Moreover, there is a possibility of underreporting of violence by women that may be attributed to social stigma, fear, and the sensitive nature of the information. Evidence suggests that the acceptance of wife beating is considerably higher in Indian society (Jejeebhoy, 1998), which could also lead to underreporting of husband’s controlling behaviors. Second, the causal link between IPV and contraceptive use cannot be assumed due to the cross-sectional design of the study. Future studies can explore the causal association between women’s exposure to IPV and the use of contraception using longitudinal data. Third, although the present study used nationally representative samples, the study results cannot be generalized for all ever-married women due to the inclusion of only currently married women in the analysis. Future research is needed to examine whether the results are consistent for other groups of women – could it be sexually active unmarried or formerly married women. Fourth, we did not observe various forms of IPV—physical, emotional, and sexual—separately to determine the IPV-contraceptive link. Various types of IPV could have differential impacts on contraceptive use and that would provide more nuanced findings.
Conclusion
This study provides significant evidence in the growing literature on the relationship between women’s experience of IPV and contraceptive use in India. Our study finds that women who experienced IPV were less likely to use modern contraceptives and more likely to undergo sterilization. Furthermore, our study made unique contributions to the existing research by assessing the moderating role of husband’s controlling attitudes in the IPV-contraception link. The findings indicate that the combined impact of IPV and husband’s controlling attitudes result in greater difficulties in using modern contraceptives among married women. Interventions should be made to prevent violence against women that would enhance their ability to choose appropriate contraception methods. Further, efforts on promoting gender equality, raising awareness against gender-based violence, and encouraging programs to change harmful gender norms might result in health-promoting behaviors among women.
Footnotes
Declaration of Conflicting Interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.