
Abstract
To date, research on social reactions to dating and sexual violence (DSV) disclosure has largely neglected the perspective of disclosure recipients. Moreover, few studies have explored disclosure recipients’ perceptions of the victim and perceptions of their own effectiveness in helping as well as the correlates of these perceptions. The purpose of this study was to address these gaps in the literature. Participants were 783 college students (73.0% female) who reported receiving a DSV disclosure in the past 6 months. Participants who provided more negative social reactions to victim disclosures were less likely to empathize with the victim and more likely to feel victim blame/burdensomeness and confusion/ineffectiveness in their responses. Conversely, those providing more positive social reactions were more likely to empathize with the victim and were less likely to report victim blame/burdensomeness and confusion/ineffectiveness. Further, recipients with a DSV victimization history were more likely to report empathy for the victim. Being a man and having higher post-traumatic stress symptoms were associated with greater victim blame/burdensomeness, while the victim approaching the recipient to disclose and DSV experiences that occurred long ago were associated with lower victim blame/burdensomeness. Finally, depressive symptoms, receiving disclosures from a stranger/casual friend, and less frequent discussion about the incident were significantly associated with increased confusion/ineffectiveness. These findings suggest that perceptions of the victim and helping effectiveness, and factors associated with them, may be promising targets of programs seeking to reduce negative and increase positive social reactions to DSV disclosures.
Dating and sexual violence (DSV) continue to be major problems on college campuses (Edwards, Sylaska, 2015; Fedina et al., 2018; Krebs et al., 2007) and are associated with a host of deleterious mental health and academic problems for students (Banyard et al., 2017; Campbell et al., 2009; Carey et al., 2018; Dworkin et al., 2017). DSV disclosures can be met with positive (e.g., emotional support) and negative (e.g., victim blaming) reactions (Edwards & Dardis, 2020; Sylaska & Edwards, 2014; Ullman, 2010). Negative social reactions can have adverse influences on victims, and predict post-traumatic stress disorder, depression, and problem drinking (Ahrens, 2006; Dworkin et al., 2019; Orchowski & Gidycz, 2015; Peter-Hagene & Ullman, 2013; Ullman et al., 2008). Conversely, positive social reactions from peers can ensure that victims feel supported and are connected to necessary resources (Filipas & Ullman, 2001), although positive social reactions are not necessarily associated with improved mental health outcomes (Dworkin et al., 2019).
While much of the research on social reactions to disclosure has focused on disclosure of sexual violence, qualitative research has confirmed that the types of reactions provided to dating violence survivors are largely similar (e.g., emotional support, tangible aid, and blame; Ahrens et al., 2021). Also, quantitative research shows that negative social reactions are similarly associated with negative psychological outcomes following dating violence (DePrince et al., 2014; Edwards, Dardis, 2015; Schackner et al., 2017; Sullivan et al., 2010). Thus, it is important to understand correlates of social reactions to disclosures of dating and sexual violence.
Although much is known about the impact of social reactions to DSV disclosures on victims, few studies have focused on understanding the experiences and perspectives of disclosure recipients (Edwards et al., 2022a; Edwards & Dardis, 2020). Studies find that 28%–51% of college students report receiving a disclosure of DSV during college, mostly from friends (Banyard et al., 2010; Edwards & Dardis, 2020; Paul et al., 2014). Disclosure recipients can experience distress at receiving a disclosure and find it difficult to support the victim (Ahrens & Campbell, 2000; Christiansen et al., 2012).
Perceptions of Victims and Effectiveness in Helping among DSV Disclosure Recipients
Research is needed to better understand disclosure recipients’ perceptions of how effective they are at helping and why they respond to disclosures of DSV the way that they do. To date, little research has been conducted on perceptions of helping, which includes disclosure recipients’ perceptions of victims and of the effectiveness of their helping efforts. One of several exceptions is Ahrens and Campbell (2000) study of perceptions of victims and helping effectiveness in a sample of 60 college students. They argued that an individual’s ability to react positively to a disclosure of DSV is likely impacted by a number of factors, including their perceptions of the victim and their own capacity to actually help the victim.
Perceptions about the victim include the recipients’ empathy for the victim, as well as the recipients’ perceptions of the victim’s blame/responsibility for their victimization (Ahrens & Campbell, 2000). Assessing perceptions of victim blame is significant given that expressing blame is one of the primary negative social reactions identified in research (Suarez & Gadalla, 2010). In a study of friends, family, and other supporters of rape victims, 25% thought the victim was at least a little responsible and friends blamed the victim more than family members (Christiansen et al., 2012).
Also, disclosure recipients may be confused about how to help and whether they responded effectively to the disclosure (Ahrens & Campbell, 2000). In one of the few studies of disclosure recipients’ perceptions of their responses (Ahrens & Campbell, 2000), three-quarters of college student disclosure recipients felt positive about helping (e.g., perceived they were needed, the victim was thankful), however, a similar percentage felt uncertain about what the victim needed and how to help. In another study of supporters of rape victims, 76% found it at least a little difficult to support the victim and only 18% were “very much” satisfied with the support they provided (Christiansen et al., 2012). The association between disclosure recipients’ perceptions of helping and actual social reactions to disclosure has not been empirically examined. However, researchers suggest that having empathy for victims is related to positive social reactions, while confusion about how to effectively help the victim and perceiving the victim is to blame are associated with negative social reactions (Edwards & Dardis, 2020; Milliken et al., 2016; Sylaska & Edwards, 2014)
A small body of literature has examined characteristics of disclosure recipients that relate to perceptions of victims and helping effectiveness. For example, Ahrens and Campbell (2000) found that compared to women, men reported being less empathic, engaged in more victim blaming, were more often confused, and felt less effective at responding to friends’ disclosures of sexual assault. Conversely, recipients with a sexual assault history were more empathic and less victim-blaming than those without such histories (Ahrens & Campbell, 2000). In this same study, researchers found that longer friendships between disclosure recipients and victims were related to more positive disclosure impacts on their relationship (Ahrens & Campbell, 2000), pointing to the potential for victim–recipient relationship characteristics to impact perceptions of the disclosure experience. Building on Ahrens and Campbell (2000) findings, Banyard et al. (2010) surveyed 354 college students and found that men reported greater discomfort than women talking to friends disclosing an unwanted sexual experience and more concern that they were causing harm to their friend. Furthermore, men were more likely to perceive they were not supportive enough and felt burdened by their friends’ needs, whereas female students felt less confusion and ineffectiveness about responding to a friend’s disclosure (Banyard et al., 2010).
Other factors have been found to predict actual social reactions provided by disclosure recipients in response to disclosure of DSV and are likely also relevant to understanding disclosure recipients’ perceptions of the victim and their helping effectiveness. Situation-specific factors (e.g., frequency of dating violence incidents disclosed by the victim), individual factors about the recipient (e.g., gender), and relational factors (e.g., recipient–victim closeness) predict social reactions to DSV disclosures (Edwards & Dardis, 2020; Sylaska & Edwards, 2014). Research also finds that victim characteristics (e.g., gender, race), disclosure recipient perceptions of victims (e.g., empathy for victim, blame of victim, and victims’ coping) and both disclosure recipient and victim behavior at the time of disclosure (e.g., drinking, distress) are related to disclosure recipient social reactions (Edwards et al., 2022a).
Current Study
To date, only a few studies have focused on perceptions of victims and perceptions of helping effectiveness. The proposed study builds off this literature in several ways. First, existing research has mainly focused on perceptions of victims and helping effectiveness among friends. The present study moves beyond friends’ disclosures to include disclosure recipients less close to the victim (e.g., acquaintances). Moreover, existing studies had relatively small samples and did not include multiple correlates of perceptions of victims and helping effectiveness, both of which the current study addresses. Finally, previous research has not empirically examined how these perceptions relate to the actual negative and positive social reactions provided. In all, the current study extends previous research in several important ways that may help to understand factors leading to reduced negative and increased positive social reactions to victims.
There were two primary aims to this exploratory study: Aim 1 was to examine how positive and negative social reactions to disclosure relate to disclosure recipients’ perceptions of victims (i.e., victim empathy; victim blame/burdensomeness) and perceptions of helping effectiveness (i.e., confusion/ineffectiveness), while Aim 2 was to document disclosure recipients’ individual (i.e., age, race/ethnicity, gender, sexual orientation, year in college, mental health symptoms, and DSV history), relational (i.e., victim–recipient relationship), and situational factors (i.e., relationship between victim and assailant, when the experience occurred, alcohol involvement in victim’s experience, how victim disclosed to recipient, victim upset during first disclosure to recipient, frequency of recipient and victim talking about the experience, and victim drinking during disclosure) that relate to disclosure recipients’ perceptions of victims and helping effectiveness. Given the exploratory nature of the study, no a priori hypotheses were made.
Method
Procedures
Data for this study comes from a larger study evaluating the impact of an intervention to train potential disclosure recipients to respond effectively to DSV disclosures (Edwards et al., 2022b). The study took place at a residential, medium-size public university in the northeastern United States and received approval from the university’s Institutional Review Board. The university’s Dean of students sent emails to randomly selected, full-time, undergraduate students on the behalf of the researchers. Emails were sent via mass email to 7000 students in four batches across 4 weeks in the fall of 2018. Emails included information about the study and a direct link to an online (Qualtrics) survey. The email informed students that the survey was 20 minutes long and would ask about how they may have helped friends with difficult sexual and/or relationship experiences. Students who had not yet completed their survey after receiving this initial email were sent one to two reminder emails across 2 weeks.
We also sent an email from the research team to all professors at the university with classes greater than 60 students (n = 205), as identified by the course catalog. We provided all university professors study information with recruitment messaging. At least 11 professors confirmed with us that they forwarded information to their students, mostly by email, although it is likely that more did so without responding back to the research team. Upon professors’ request, we visited approximately five classrooms to pass on the information. Lastly, we posted fliers in residence halls and other shared spaces about the study. Given the multiple recruitment strategies used, data were checked for multiple responses by the same participant by checking for duplicate student email addresses and the same name being used multiple times in email addresses (e.g.,
Participants consented to participate online and then completed the eligibility questionnaire; if eligible, they moved on to the survey. Overall, 1831 students started the survey, of which 1268 qualified for, consented to, and completed the survey. Analyses were conducted with data from 783 students who reported receiving a disclosure of DSV in the previous 6 months. All data presented in this paper were collected prior to the intervention.
Participants
Sample Characteristics.
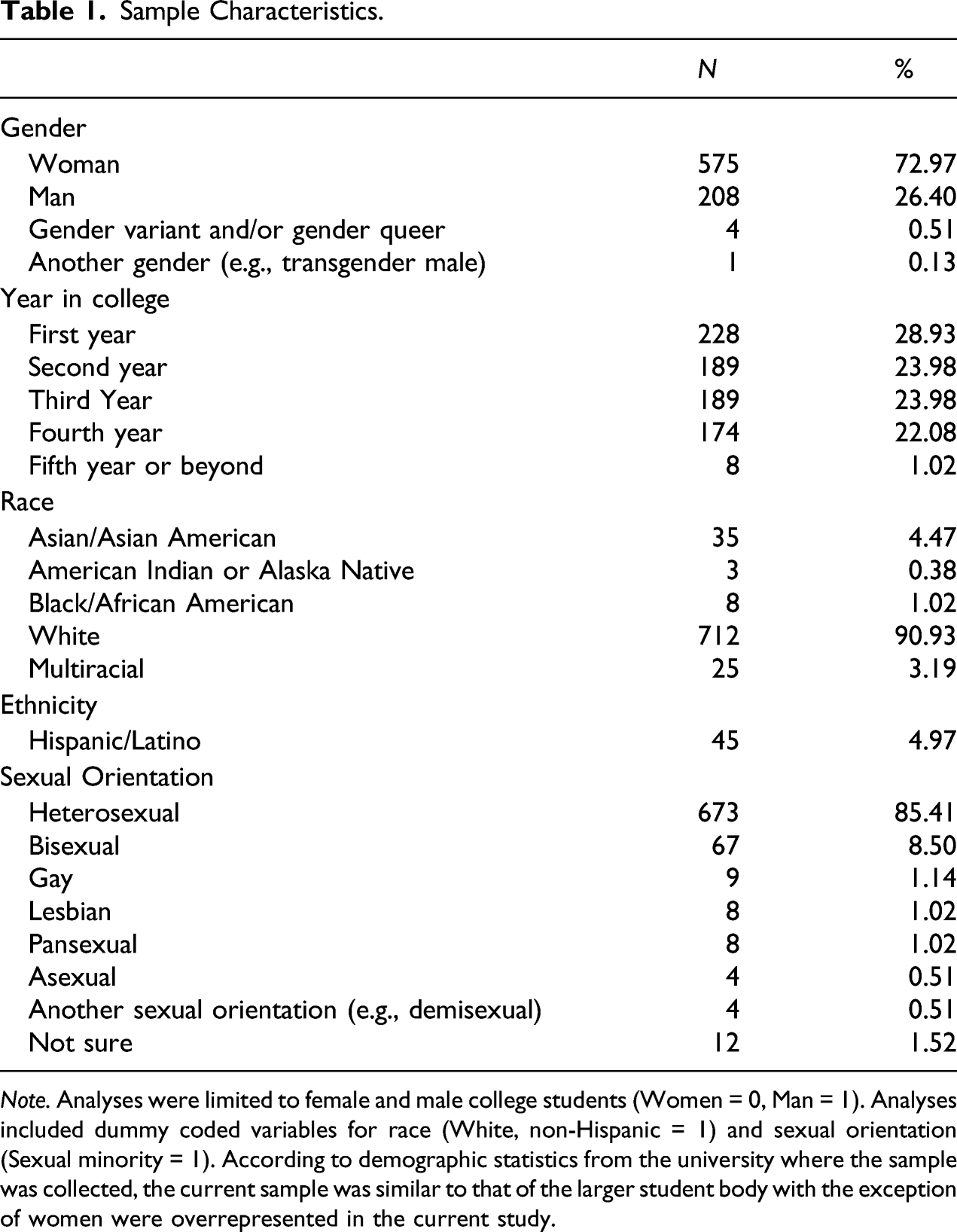
Note. Analyses were limited to female and male college students (Women = 0, Man = 1). Analyses included dummy coded variables for race (White, non-Hispanic = 1) and sexual orientation (Sexual minority = 1). According to demographic statistics from the university where the sample was collected, the current sample was similar to that of the larger student body with the exception of women were overrepresented in the current study.
Measures
Experiences of Disclosure
Participants responded to the item, “In the past 6 months, has someone (e.g., friend, acquaintance, family member, and dating/romantic partner) told you they experienced any of the following?” This item was followed by three sexual assault items (e.g., “someone [including, but not limited to, a romantic partner] used physical force, threats of physical force, alcohol/drugs to incapacitated to have sexual intercourse [oral, anal, and vaginal]”) and 13 items of physical, verbal, and psychological dating violence (e.g., “their partner threw something at them,” “their partner refused to talk to them,” “their partner monitored their phone, email, social media account”).
Perceptions of Helping
Participants responded to two subscales from the Friends’ Perceptions of the Victims and the Assault questionnaire (i.e., Victim Responsibility, Empathy) and two subscales from the Friends’ Perceptions of their Assistance questionnaire (i.e., Confusion, Ineffectiveness; Ahrens & Campbell, 2000). Because the subscales used in the present study have not been psychometrically validated, we examined the factor structure of the items.1 The final measure included three subscales with acceptable reliability that were thematically consistent with the proposed scales from the original measure: (1) empathy (3 items, e.g., “I felt I was able to understand what they were going through”; α = .72), (2) victim blame/burdensomeness (6 items; 4 blame (e.g., “I thought it was unwise to put themselves in that position”), 2 burdensomeness (e.g. “I felt burdened by their needs”); α = .83), and (3) confusion/ineffectiveness (6 items; 4 confusion (e.g., “I didn’t know what to do to help”), 2 ineffectiveness (e.g., “I felt that I wasn’t supportive enough”); α = .80). Response items ranged from 1 = strongly disagree to 5 = strongly agree. Final score on the subscales was a mean of items.
Social Reactions
Participants responded to the Social Reactions Questionnaire - Shortened (Relyea & Ullman, 2015; Ullman et al., 2014). In a previous paper from the larger study, we performed a factor analysis confiming the two-factor solution that previous versions of the scale also found (Edwards et al., 2022b; Relyea & Ullman, 2015; Ullman et al., 2014). The two factors were negative reactions (10 items; e.g., “Told them that they were irresponsible or not cautious enough”; “Tried to take control of what they did/decisions they made”), and positive reactions (4 items; e.g., “Listened to their feelings”). Response items ranged from 1 = never/extremely unlikely to 5 = always/extremely likely. Final score on the subscales was a mean of items. Reliability was α = .80 for negative reactions and α = .70 for positive reactions.
Correlates of Perceptions of Helping: Individual Factors
Several individual characteristics of the disclosure recipient assessed included: demographics, victimization history, and mental health symptoms.
Demographic Characteristics
Demographics of the disclosure recipient assessed included: age, gender, race/ethnicity, sexual orientation, and year in college.
Sexual Violence (SV) Victimization
Participants responded to two questions asking if they had ever, in their lifetime, experienced unwanted sexual contact or unwanted sexual intercourse (0 = no, 1 = yes), with the questions, “In your lifetime, have you had sexual contact with someone when you didn’t want to?” and “In your lifetime, have you had sexual intercourse with someone when you didn't want to?” (Banyard et al., 2007; Ward et al., 1991). Sexual intercourse was defined as, “any form of sexual penetration including vaginal intercourse, oral sex, and anal intercourse,” and sexual contact was defined as “touching of genitals without a person’s permission (but there is no penetration).” Unwanted sexual intercourse/contact was defined as “those situations in which you were certain at the time that you did not want to engage in the sexual experience and you either communicated this in some way (e.g., you said no; you protested; you said you didn’t want to; you physically struggled; you cried), or you were intimidated or forced by someone or you were incapacitated (e.g., drunk, passed out).” Responses for sexual contact and sexual intercourse questions were combined into one variable indicating lifetime SV victimization, which was reported by 42.78% (n = 335) of participants.
Dating Violence (DV) Victimization
Participants responded to four questions asking if they had ever, in their lifetime, experienced verbal, physical, or psychological dating violence (0 = no, 1 = yes), for example, “My partner insulted or swore or shouted or yelled at me.” These questions are from the Revised Conflict Tactics Scale (Straus & Douglas, 2004). All items were combined into one variable indicating any lifetime DV victimization. In the present study sample, 46.19% (n = 358) of participants reported lifetime DV victimization.
Posttraumatic Stress (PTS) Symptoms
Participants responded to the PTSD Checklist for DSM-5 (Weathers et al., 2013). Participants who reported DSV in their lifetime answered questions about the most traumatic/emotional/intense experience of DSV in their lifetime, whereas participants not reporting DSV answered questions about the most traumatic/stressful experience in their lifetime. Twenty items such as “How much were you bothered by repeated, disturbing, and unwanted memories of the stressful experience?” were asked with respect to the past month. Response items ranged from 0 = not at all to 4 = extremely. Final score was a sum of items. Reliability was α = .95 and participants had a mean of 15.79 PTS symptoms (SD = 16.54).
Depressive Symptoms
Participants responded to the modified, 7-item Center for Epidemiologic Studies Depression Scale (Mirowsky & Ross, 1990), with items such as “I felt that I could not shake off the blues.” Response items ranged from 0 = rarely or none of the time to 3 = most or all of the time. Final score was a sum of items. Reliability was α = .88 and the present sample reported a mean of 7.38 depressive symptoms (SD = 5.16).
Correlates of Perceptions of Helping: Relational and Situational Characteristics
Relational Characteristics of Disclosure
Relationship between the victim and disclosure recipient was assessed with several categories (e.g., friend [close]; stranger, acquaintance, friend [casual]) that were recoded into two categories indicating closeness of the relationship: (1) close friend, serious romantic partner, family member (70.57%, n = 530), and (2) stranger, casual friend, etc. (29.43%, n = 221).
Situational Characteristics of the Assault and Disclosure
Situational Characteristics of the Assault and Disclosure.
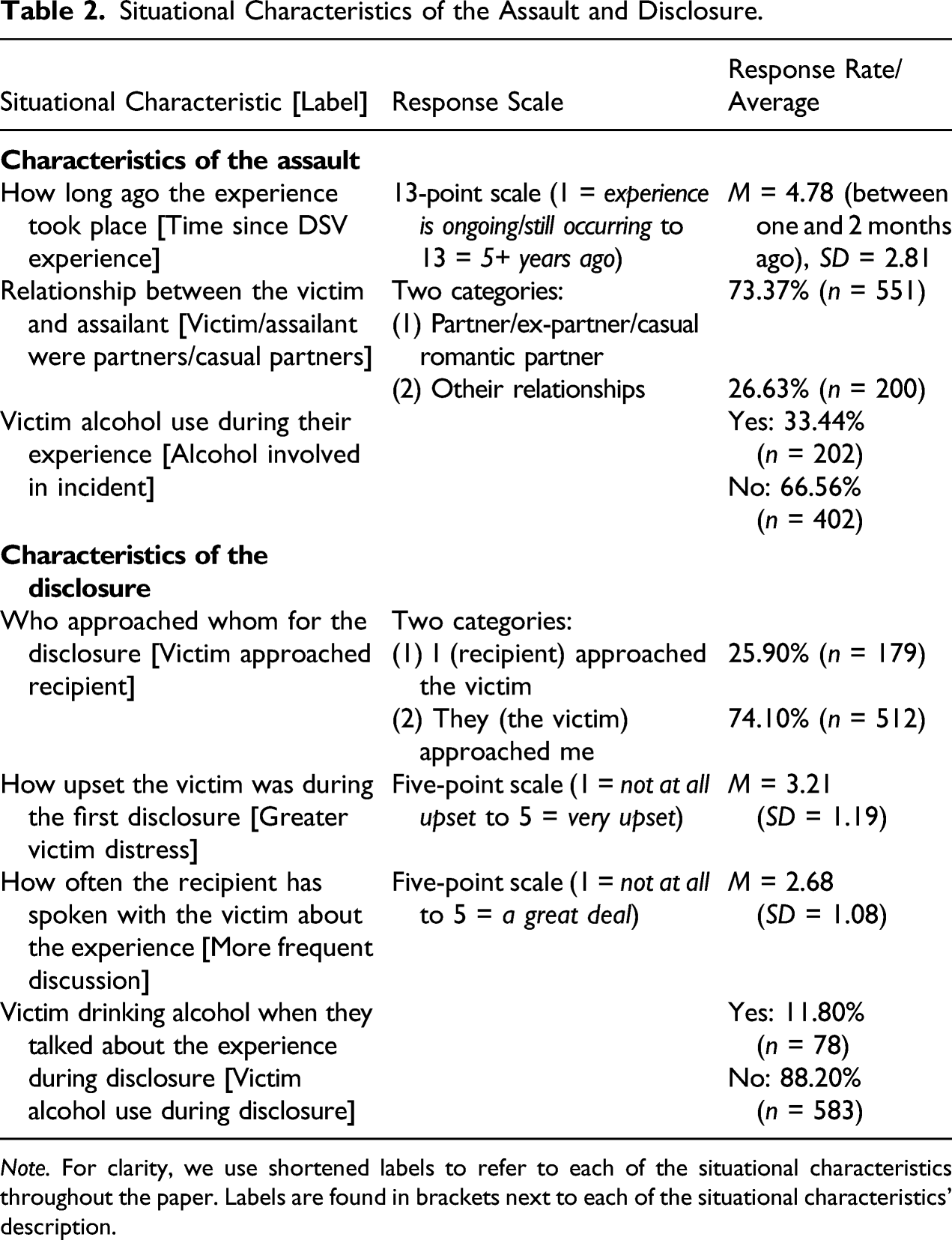
Note. For clarity, we use shortened labels to refer to each of the situational characteristics throughout the paper. Labels are found in brackets next to each of the situational characteristics’ description.
Data Analysis Plan
We checked for skewness of all variables; skewness (absolute value) ranged from 0.34 to 1.40, which was within acceptable limits (Kim, 2013). For Aim 1 (examining associations between social reactions to disclosure and perceptions of helping), we calculated Pearson’s bivariate correlations to assess the associations between positive and negative social reactions and the perceptions of helping subscales (i.e., empathy, victim blame/burdensomeness, and confusion/ineffectiveness). For Aim 2 (examining correlates of perceptions of helping), we first conducted Pearson’s bivariate correlations of individual, relational, and situational factors with the perceptions of helping subscales (i.e., empathy, victim blame/burdensomeness, and confusion/ineffectiveness). Second, we conducted three multiple regressions predicting empathy, victim blame/burdensomeness, and confusion/ineffectiveness. Only significant variables in the bivariate correlations were included in multiple regressions. Due to the exploratory nature of the study and the many variables included in the models, the p < .01 level of significance was used.
Results
Aim 1: Associations between Social Reactions to Disclosure and Perceptions of Victim & Helping Effectiveness
Providing negative social reactions was associated with lower empathy (r = −.16, p < .001), greater victim blame/burdensomeness (r = .54, p < .001), and greater confusion/ineffectiveness (r = .15, p < .001). Providing positive social reactions was associated with greater empathy (r = .23, p < .001), lower victim blame/burdensomeness (r = −.22, p < .001), and lower confusion/ineffectiveness (r = −.14, p < .001).
Aim 2: The Relationship between Individual, Relational, and Situational Factors and Perceptions of Victim & Helping Effectiveness
Bivariate Associations
Bivariate Correlations for Perceptions of Helping Subscales.
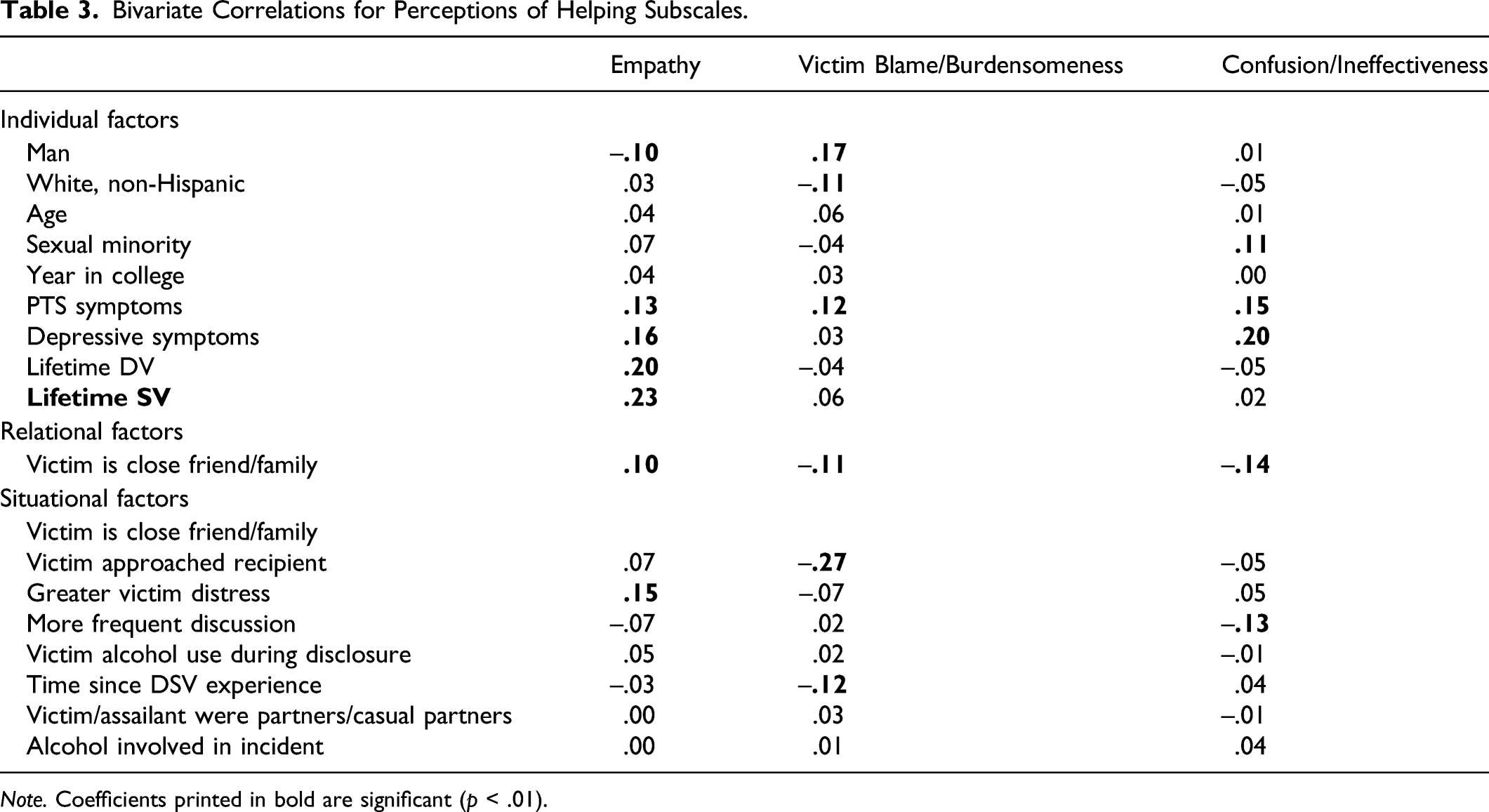
Note. Coefficients printed in bold are significant (p < .01).
Regarding victim blame/burdensomeness, being a man and greater PTS symptoms were associated with greater blame/burdensomeness. Being non-Hispanic White, a close friend/family member of the victim, the victim approaching the recipient to disclose, and a longer time since the DSV experience were associated with lower victim blame/burdensomeness.
Finally, regarding confusion/ineffectiveness, identifying as sexual minority, greater PTS symptoms, and greater depressive symptoms were associated with greater confusion/ineffectiveness. Being a close friend/family member of the victim and discussing the victim’s experience more frequently were associated with lower confusion/ineffectiveness.
Multiple Regression Model for Empathy
Multiple Regression for Perceptions of Helping Subscales.

Note. Rows printed in bold are significant (p < .01). LL is defined as the lower level of the 95% confidence interval. UL is defined as the upper level of the 95% confidence interval.
Multiple Regression Model for Victim Blame/Burdensomeness
The model for victim blame/burdensomeness was significant, F(6, 614) = 16.01, p < .001, and accounted for 13.53% of the variance (Table 4). Men and disclosure recipients with greater post-traumatic stress symptoms had greater victim blame/burdensomeness than women and disclosure recipients with fewer post-traumatic stress symptoms. Disclosure recipients approached by the victim had less victim blame/burdensomeness than those who approached the victim themselves. Disclosure recipients receiving a DSV disclosure that occurred less recently had less victim blame/burdensomeness, compared to those receiving a DSV disclosure that happened more recently. Being non-Hispanic White and the victim being a close friend or family, while not significant at the p < .01 level, were marginally related to less victim blame/burdensomeness (p < .05).
Multiple Regression Model for Confusion/Ineffectiveness
The model for confusion/ineffectiveness was significant, F(5, 696) = 11.91, p < .001, and accounted for 7.88% of the variance (Table 4). Disclosure recipients with greater depressive symptoms reported greater confusion/ineffectiveness. Disclosure recipients who were close friends/family members with the victim reported less confusion/ineffectiveness than those who were not close friends/family members with the victim. Disclosure recipients who had more frequent discussion about the victimization reported less confusion/ineffectiveness than did those who discussed the victimization less frequently. Disclosure recipient’s sexual orientation and PTS symptoms were not significantly associated with confusion/ineffectiveness.
Discussion
The present study highlights the importance of understanding disclosure recipients’ perceptions of both the victim and their own helping effectiveness. Regarding Aim 1, we found that disclosure recipients’ perceptions of the victim and helping effectiveness were significantly related to their positive and negative social reactions to disclosure. The finding that confusion/ineffectiveness was associated with more negative social reactions provided suggests that, at least to some extent, students are aware that the reactions they provided were not helpful. However, the temporal ordering of the relationship between perceptions of helping and social reactions is unclear. One possibility is that people who feel more confused/ineffective provide negative reactions as a result. The second possibility is that people who provide more negative reactions are more likely to feel more confused/ineffective as a result. These findings suggest that students need to be equipped with skills and training to respond positively and not negatively to victim disclosures and feel more confident in their ability to do so.
The finding that positive social reactions were associated with greater empathy and negative social reactions were associated with greater victim blame/burdensomeness suggests that disclosure recipients are conveying their perceptions of the victim to them (Bonnan-White et al., 2018). Therefore, one point of intervention might be to help disclosure recipients notice and identify these attitudes, try to challenge them, refrain from saying/doing harmful things and try to engage in supportive actions.
Turning to Aim 2, several individual characteristics of the disclosure recipient were significantly related to perceptions of helping. Consistent with previous findings (Ahrens & Campbell, 2000; Banyard et al., 2010), men reported higher victim blame/burdensomeness. However, gender was not significantly related to empathy, which differs from previous research (Ahrens & Campbell, 2000; Edwards et al., 2022a). Therefore, it is possible that men’s ability to empathize with victims is not the mechanism by which they feel victim blame/burdensomeness. Further research with male disclosure recipients is needed to unpack these mechanisms.
Moreover, we found that symptoms of depression were associated with confusion/ineffectiveness. As depressive symptoms often include feelings of low self-worth and self-efficacy, it is unsurprising that those with higher depressive symptoms might also struggle with low perceived competence to cope with DSV disclosures. Similarly, PTS symptoms were significantly associated with victim blame/burdensomeness. It is important to note that PTS symptoms were not necessarily assessed in relation to the recipient’s own experience of DSV. While some participants answered the PTS checklist about a DSV experience, others without such experiences answered about a recent traumatic/stressful event. This suggests that it is not necessarily the case that disclosure recipients were experiencing distress as a result of being reminded of a personal experience, although victimization history was related to empathy. It is possible that disclosure recipients with higher PTS symptoms may feel more emotionally depleted and therefore feel more burdened by the victim’s disclosure. Disclosure recipients with higher PTS symptoms may also experience interpersonal difficulties or irritability that may lead them to feel burdened by the victim. It is also possible that negative cognitions about the self and the world (characterized in PTSD symptom cluster D; APA, 2013) contribute to victim blame. According to one cognitive theory of the development of PTSD, adherence to “just world beliefs” (i.e., beliefs that the world is fair and that people get what they deserve; (Lerner, 1980)) are violated by innocent victimhood; efforts to maintain belief in a just and fair world therefore lead to self-blame, contributing to risk for PTSD (Resick & Schnicke, 1993). These beliefs about one’s own blameworthiness may also extend to others: indeed, prior research shows that adherence to just world beliefs is positively associated with perceptions of victim blame (Furnham, 2003; Strömwall et al., 2013). Further research is needed to explore the pathways from just word beliefs to self and other blame. Programs should include mental health resources for participants both to support their own well-being and mechanisms for self-care in the context of receiving disclosures as well as their ability to effectively assist victims who disclose DSV.
The finding that previous DSV victimization experiences were related to victim empathy aligns with previous studies showing that disclosure recipients’ victimization history was associated with the recipient anticipating greater impacts on the victim’s life as a result of their experience and greater emotional distress in response to hearing disclosures of SV (Ahrens & Campbell, 2000; Banyard et al., 2010). These results are perhaps not surprising given findings that DSV victims are more likely to report being a disclosure recipient and that history of DSV victimization is associated with more positive social reactions in response to disclosure (Edwards et al., 2022a; Paul et al., 2014). While the results show that one’s own victimization history is particularly useful in empathizing with DSV victims, programming must consider how to foster such empathy in those without victimization histories and provide resources to program participants reporting victimization histories.
The results of this study move beyond previous research examining perceptions of helping when the victim is a friend (Ahrens & Campbell, 2000; Banyard et al., 2010), to consider instances where the victim is merely an acquaintance or stranger. Disclosure recipients in closer relationships with the victim were less likely than those in less close relationships to report confusion/ineffectiveness regarding their responses to victims. If a disclosure recipient is closer to the victim, they may better understand what types of reactions would help them and they may also have a longer relationship and be able to see whether their reactions help or not and have a greater investment in the victim’s welfare (Christiansen et al., 2012). In contrast, in a less close relationship, the encounter may be brief, so the disclosure recipient may not see the impact of their social reactions, leading to confusion over whether their behavior was helpful. The significance of the type of relationship has direct implications for developing interventions to promote positive responses to disclosure. It is necessary to consider how empathy can be fostered and recipients’ can feel greater confidence in their ability to respond to disclosures from individuals with whom they are less close. Given universities’ move towards bystander intervention programming as a means to prevent DSV by encouraging students to intervene regardless of whether they know the potential victim, it is imperative that programming foster empathy for those outside of recipients’ friendship networks.
There were several situational aspects of the disclosure that were associated with perceptions of helping. The victim approaching the recipient to disclose was associated with less victim blame/burdensomeness, and more frequent discussion about the incident was associated with less confusion/ineffectiveness. Approaching the victim about their experience is likely a distressing situation for the recipient because they might be uncertain about how the victim will feel about being approached and may potentially impact their ability to empathize with the victim. Moreover, it is possible that less frequent discussion limits the recipient’s ability to process what happened to the victim leading to less confidence in their ability to help the victim. The finding that disclosure recipients perceived less victim blame when the DSV occurred longer ago compared to more recently could be due to the fact that victims are likely more distressed regarding recent DSV (Dworkin et al., 2021). This could lead a disclosure recipient to feel a greater need to help the victim leading to increased burden. Assisting victims with decisions like whether to get a medical exam or report the incident to authorities might create more burden for recipients as opposed to disclosures with fewer expectations for direct, instrumental support.
There are several limitations to this study. First, the sample was not highly diverse in terms of gender, race, ethnicity, and sexual orientation. Further research is needed to understand disclosure recipients’ perceptions of helping in more diverse populations, particularly given the importance of sociocultural contexts broadly, and systems of oppression in relation to help-seeking and recovery experiences (Dworkin & Weaver, 2021). For example, the gender and race of both the victim and disclosure recipient are related to social reactions to disclosure in that men tend to respond less supportively to sexual assault disclosures and women of color tend to receive more negative social reactions (Banyard et al., 2010; Ullman, 2021). Also, preliminary research suggests that sexual and gender minorities face additional barriers (e.g., fear of being outed) to disclosing DSV and that some groups of sexual minorities (e.g., bisexual women) may receive more negative social reactions to disclosure than other sexual minorities (Edwards et al., 2021). The sample size was too small to examine whether the observed relationships vary as a function of intersectional social identities. Future research is needed to further develop the perceptions of helping scale with more diverse populations. Second, given the study’s cross-sectional design, the relationship between social reactions and perceptions of helping cannot be interpreted temporally, which limits our ability to understand if social reactions cause perceptions of the victim and helping effectiveness or vice versa. We also cannot be certain that the individual, relational, and situational factors are not conflated with recipients’ social reactions. Also, there may be additional contextual details about the disclosure and DSV experience not captured in the present study. Qualitative research could provide a better understanding of the relationships found here as well as underlying mechanisms. Finally, we did not include all of the possible subscales from the Ahrens and Campbell (2000) measure assessing the experiences of disclosure recipients because this study’s data comes from a larger intervention study to promote positive social reactions to disclosure of DSV (see Edwards et al., 2022b), so subscales were selected based on intervention targets.
In conclusion, the findings of this study highlight how disclosure recipients’ perceptions of the victim and their own helping effectiveness are intertwined with the ways they respond to disclosures of DSV. Taken together, these results point to an array of factors that can be targeted in programming to reduce perceptions of victim blame/burdensomeness, increase victim empathy, and increase students’ confidence in their ability to respond in positive/helpful ways and avoid negative social reactions. Given the wide array of individual, relational, and situational factors that are associated with such perceptions, research is needed to explore the underlying mechanisms by which these factors influence perceptions to inform interventions seeking to improve individuals’ reactions to DSV disclosures and reduce deleterious outcomes associated with victims receiving negative social reactions (Dworkin et al., 2019).
Endnotes
We began with 19 items and performed exploratory factor analysis (EFA) with one half of the sample using Promax rotation (Tabachnick & Fidell, 2013) to allow for the expectation that factors would be correlated. The rotations indicated a three-factor solution: empathy; victim blame/burdensomeness; and confusion and ineffectiveness. We eliminated four items that had cross loadings above .20 on more than one factor and used a minimum loading threshold of .45 (Hair et al., 1998). Next, to examine model fit we conducted a confirmatory factor analysis with the second half of the sample not used for the EFA. Although the model’s chi-square was significant (significant chi-square tests are common among models with large sample size, even in cases of good model fit; Gatignon, 2010; Kyriazos, 2018), χ2(87) = 166.79, p < .001, the remaining fit statistics indicated acceptable model fit (RMSEA = .051, CFI = .943).
Footnotes
Acknowledgments
We would like to thank Jania Marshall, Caroline Leyva, Jane Stapleton, Robert Eckstein, Prentiss Phillips, Victoria Stanek, Allison Depuy, Drew Doyle, Lianna Nawn, Meredith Baker, Nicole Westfall, Lauren Flynn, Hannah Nordstorm, Kristina Kalla, Michael Green-Kelsey, Abi Beaulieu, Eleonora Giovine, Ross Jones, and Sarah Russo for their assistance with this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the National Institute of Health (NIH), Grant # 5R34AA024849-03. Manuscript preparation was supported by Grant # R00AA026317 (Dworkin). The findings and implications presented in this paper do not represent the official views of the NIH.