
Abstract
The objective of this study was to examine differences in change over time in health and safety outcomes among female college students randomized to myPlan, a tailored safety planning app, or usual web-based safety planning resources. Three hundred forty-six women (175 intervention, 171 control) from 41 colleges/universities in Oregon and Maryland completed surveys at baseline, 6- and 12-months from July 2015 to October 2017. Generalized estimating equations were used to test group differences across time. Both groups improved on four measure of intimate partner violence (IPV; Composite Abuse Scale [CAS], TBI-related IPV, digital abuse, reproductive coercion [RC]) and depression. Reduction in RC and improvement in suicide risk were significantly greater in the myPlan group relative to controls (p = .019 and p = .46, respectively). Increases in the percent of safety behaviors tried that were helpful significantly reduced CAS scores, indicating a reduction in IPV over time in the myPlan group compared to controls (p = .006). Findings support the feasibility and importance of technology-based IPV safety planning for college women. myPlan achieved a number of its objectives related to safety planning and decision-making, the use of helpful safety behaviors, mental health, and reductions in some forms of IPV.
Keywords
Introduction
Intimate partner violence (IPV) is a global public health issue and includes psychological, physical, and/or sexual violence (García-Moreno et al., 2013). While close to the same percentage of men (33.6%) and women (36.4%) will experience lifetime IPV, women’s prevalence of severe physical violence (21.4% vs 14.9%), injury (35.2% vs 11.5%), and rates of death are significantly greater (Smith et al., 2017; Smith et al., 2018; Velopulos et al., 2019). Physical health problems are significantly higher among women who have experienced IPV compared with those who have not (Amar & Gennaro, 2005; Fisher et al., 2002; Fisher et al., 2003). Research consistently demonstrates an association between IPV and increased rates of depression, substance misuse, and suicide (Beydoun et al., 2012; Devries et al., 2013; Rees et al., 2011).
Most women experience their first exposure to physical and/or sexual violence prior to age 25 in the context of an intimate relationship (Halpern-Meekin et al., 2013), with college-age women (ages 18–24 years) reporting the highest IPV rates (Desmarais et al., 2012; Smith et al., 2017). Yet, few colleges/universities offer evidence-based programs addressing IPV and the associated health and safety needs with students (Shorey et al., 2012). Young women weigh complex factors (e.g., health, academics, finances) in their safety decisions about abusive relationships. Rather than accessing formal support (e.g., campus security, counselors), most seek help from informal networks, turning to friends who often lack the knowledge or resources to effectively help (Amar & Alexy, 2005).
myPlan is an interactive decision aid and safety planning intervention that is free and accessible via a mobile app and website (myPlanApp.org), appropriate technology for college students (Glass et al., 2015; Glass et al., 2017). myPlan was created drawing upon foundational work in empowerment (Dutton, 1992), a previous trial of an internet safety decision aid for women of all ages (Glass et al., 2017), and the literature on safety planning (Campbell & Glass, 2009; Campbell et al., 2001; Davies & Lyon, 1998; Hardesty & Campbell, 2004; McFarlane et al., 2002, 2004). Evidence supports the use of decision aids to inform complex decision-making for people faced with difficult choices (e.g., end of life decisions, treatment course for chronic illness, safety in abusive relationships; Glass et al., 2012; Stacey et al., 2017). myPlan addresses three key factors: (1) protection, a focus on increasing safety; (2) enhancing decision-making around safety; and (3) reducing IPV to facilitate healing. myPlan was designed to assist diverse survivors to evaluate their relationship health and safety, consider their priorities, and design a safety plan tailored to their needs and priorities, with embedded links to connect directly to resources such as advocacy, mental and reproductive health services.
This article presents the findings from a two-group randomized controlled trial (RCT) to examine differences in change over time in decisional conflict, IPV, depression, substance misuse, suicide risk, and safety planning behaviors among college women randomized to using either the myPlan app or usual web-based safety planning. We hypothesized those in the intervention group would show greater improvement over time on each outcome. We also examined the association between IPV and number and usefulness of attempted safety behaviors, hypothesizing that the number and usefulness of safety behaviors will be associated with greater reduction in IPV among the intervention group.
Methods
Study Design and Participants
We collected data from intervention and control groups at baseline, 6- and 12-months from July 2015 to October 2017. Eligible participants were English-speaking women (including cisgender and transgender women), age 18–24, enrolled at least part-time in college/university in Oregon or Maryland, had safe access to email and a personal device with internet, and screened positive for IPV. IPV screening questions asked if a current or ex-partner had done any of the following (past 6 months): threatened to harm her physically; hit, kicked, punched, choked or otherwise physically hurt her; forced or coerced sexual activity; constantly called, texted, emailed or harassed or embarrassed her on social media; or made her feel unsafe in any way. Using the method safest for them, potential participants could provide instructions to be contacted (e.g., only call in the afternoon, do not leave a message) via email or phone by a research assistant (RA) or could contact the RA to complete eligibility, consent, and enrollment.
The study sample was drawn from diverse campus environments (three four-year public, one historically Black college, two four-year private, three community colleges) in Maryland and Oregon. Study recruitment was primarily online via advertisements across a range of platforms, including Facebook, campus bulletins, social media, and student listservs. Study advertisements were shared among students and staff at colleges/universities throughout the two states, resulting in participants from 41 campuses.
Ethics approval was obtained from the Johns Hopkins Medicine Institutional Review Board (IRB 00054334) and the Kaiser Permanente Center for Health Research IRB (Pro00004875) for the oversight of the research in Oregon. RAs were trained in human subjects’ research ethics, safe technology use, IPV-related referrals, and suicidality protocols. Detailed study and safety procedures are explained in the protocol publication (Glass et al., 2015).
Randomization
An automated algorithm randomly assigned enrolled participants to the intervention or control group. The randomization was stratified on state of residence, having children (child/no child in the home), and type of college/university. Random assignment was stratified by state to ensure the proportion of participants in each state assigned to one group or the other remained relatively constant.
Procedures
Following enrollment and randomization, an automated email was sent to the participant’s safe email address containing instructions and links for safely accessing myPlan or usual safety planning. Those randomized to myPlan had two options: download the free, publicly available app from a major U.S. app store or access a web-based version via the study website. Users entered an assigned username and password the first time the app was accessed and created a private 4-digit security PIN code for future access, which could be reset by logging out and back in using the provided username and password. Participants randomized to the control group accessed safety planning via a secure study website. All personal identifiers (only collected at study enrollment) were saved in a physically separate database in a HIPAA compliant network environment. For the duration of the RCT, study data and personal identifiers were never combined.
Data collection was completed via the app/website, allowing participants to complete the instruments whenever convenient, eliminating data input error, and potentially reducing social desirability bias compared to face-to-face interviews (Johnson et al., 2001; Rhodes et al., 2003). Participants were compensated for their time (~3 hours) and expertise with $100 total (baseline $20, 6-month $30, 12-month $50), an amount consistent with other studies.
The myPlan intervention includes: (1) Awareness of myths (jealousy = love) and characteristics of a healthy relationship, (2) My Safety, a self-assessment with immediate feedback on red flags for an unhealthy relationships and the Danger Assessment (DA) or DA-Revised (for women abused by female partners), an assessment of risk for repeat severe IPV, (3) My Priorities, an interactive visual aid that allows users to make pairwise comparisons of the importance between priorities including privacy, feelings for partner, safety, well-being of children (as appropriate), academic success, and social support/status, and (4) My Plan, a personalized safety plan with information and referrals based on responses in the previous sections.
Usual safety planning received by the control group is guided by basic emergency safety planning information provided to students on-campus and found through IPV websites targeting young women in unsafe relationships. The usual safety planning site is different from the intervention in three important ways. First, usual safety planning does not include opportunities to assess the health and safety of a relationship, such as the validated DA or DA-R to assess risk for repeat and severe violence by the partner or ex-partner, the red flags assessment, and healthy relationships information provided in the intervention site. Second, the usual safety planning site does not include an interactive safety priority activity or visual aid to provide feedback on priorities. Third, the control site includes a static emergency safety plan only with two resources (a national IPV hotline and national LGBTQ hotline), rather than more comprehensive safety information and resources beyond just emergency planning, and the usual safety plan is not tailored based on user characteristics (e.g., wants to stay in the relationship vs leave, is LGBTQ) or to the user’s risk assessment and/or safety priorities as detailed above for the myPlan intervention. A detailed description of the intervention and control sites is provided in the published study protocol (Glass et al., 2015).
Primary and Secondary Outcomes
Study measures included participant demographics such as age, race, ethnicity, year in college/university, living situation, employment, demographics of the abusive partner, and characteristics of the relationship status (current or ex-partner) and length.
Primary outcomes included use and helpfulness of 34 safety strategies (Parker et al., 1999) at 12-months, with a response scale of have not tried, tried but not helpful, or tried and helpful. Safety behaviors are scored by taking the number of items found helpful, dividing by the number tried, and multiplying by 100 to get the percent of safety strategies tried that were helpful. Decisional conflict was measured immediately post-intervention, with questions adapted from validated subscales of the Decisional Conflict Scale (DCS; O’Connor, 1995; O’Connor, 1993/2010). The scale has 12-items on advantages and disadvantages of safety options and values related to them and uses a 5-point Likert response scale from “strongly agree” to “strongly disagree.” The DCS provides a total score (sample α = .91), with higher scores indicating a greater degree of decisional conflict (i.e., poorer decision process; Rhodes et al., 2003; Sullivan & Bybee, 1999), as well as four subscale scores (feeling informed, certainty about decision, values clarity, and support).
Secondary outcomes included past 6-months IPV and reproductive coercion (RC), past-week depression and suicide risk, substance misuse, and preparation for decision-making. IPV was measured using the Composite Abuse Scale (CAS; Beeble et al., 2008; Foshee et al., 1996), a 30-item validated measure of four independent types of abuse: (1) severe combined abuse (defined as one or more episodes of severe combined abuse, for example, use of a weapon, rape or attempted rape), (2) physical abuse with emotional abuse and/or harassment, (3) physical abuse only, and (4) emotional abuse and/or harassment only. To calculate a total score (sample α = .93), we used an adapted response scale: never = 0, only once = 1, several times = 2, or many times = 3. Additional IPV variables included seven “yes” or “no” items examining digital abuse, measured with items adapted from existing studies; “[Partner] shared (or threatened to share) content that was supposed to be private (e.g., a nude picture)” (Glauber et al., 2007; Muise et al., 2009; Tokunaga, 2011). This yielded a score of 0–7 with higher values indicating more forms of digital abuse (sample α = .72). Four items examined traumatic brain injury (TBI)-related IPV (beating to the head, choking/strangling), and a dichotomous score (yes/no) for any experience of TBI-related IPV was created.
RC was defined as a positive response to either or both items assessing if (1) partner tried to get her pregnant when she did not want to be and (2) participant prevented or ended a pregnancy and did not tell their partner out of fear. Depression was measured with the Center for Epidemiologic Studies Depression Scale, Revised (CESD-R; Eaton et al., 2004; Radloff, 1977), a 20-item self-report measure that assesses for depressive symptoms (sample α = .95). Items are rated based on frequency in the “past week or so” from 0 (Rarely or none of the time—less than one day) to 4 (Nearly every day for two weeks). Suicide risk was defined as a response of one or more days in the past week to the CESD questions “I wished I were dead” or “I wanted to hurt myself.”
The Monitoring the Future Drug and Alcohol Questionnaire (O’Malley et al., 1984) was used to measure alcohol and drug misuse. Participants reported how many occasions (0 = never to 6 = 40 or more times) they used alcohol in the last 30 days, got drunk in the last 6 months (1 = none to 5 = nearly all), and binge drank in the last 2 weeks (1 = none to 5 = nearly all), yielding three frequency scores. Participants were also asked how many occasions they used drugs (marijuana, club drugs/hallucinogens, stimulants/narcotics, prescription drugs, other) in the last 30 days (O’Connor, 1995; O’Connor, 1993/2010). Two variables were created: any use of marijuana and any drug use excluding marijuana in the last 30 days.
The Preparation for Decision-Making Scale (Bennett et al., 2010; Graham & O’Connor, 1995) is a 10-item scale that assesses perception on usefulness of a decision support intervention in preparing to make a decision and has a response scale of 1 (not at all) to 5 (a great deal). Participants in both groups completed these items after first use of myPlan or usual safety planning and at 12-months follow-up. We examined individual scale items as we were interested in the specific ways the intervention informed decision-making.
Statistical Power Analysis
The power analysis was based on an effect size calculated from the results of an online IPV intervention (Eden et al., 2015) to enhance safety seeking, compared to usual safety planning. The effect size, f, was computed to be .58, a medium effect size equivalent to a mean change from baseline to follow-up of 14.4% for the intervention group compared to a change of 10.4% in the control group from baseline to 12-months. Assuming an autocorrelation of .3, 150 participants in the intervention and 150 participants in the control group, at attrition rate of 20%, the study has .99 power to detect a significant group-by-time interaction.
Statistical Analyses
Chi-square and t-tests examined if randomization achieved balance between groups at baseline. Mixed effect regressions were used to test group differences across time with Binomial, Gaussian, or Poisson distributions depending on the outcome. The main analyses included time, group, and time-by-group interaction accounting for the nesting of participants within colleges and time within participants. Mixed-effects regressions were used to examine differences between groups in decisional conflict immediately post-use of the intervention or control app and at 12-months. Mixed-effects regression with change from baseline to 12-months in IPV as the dependent variable and group, safety behaviors, and their interaction as independent variables tested the relationship in the number and usefulness of safety behaviors with decreased IPV. Analyses were conducted in STATA 16.0, using an intention-to-treat approach. All women were included in the main analyses as these models do not require complete data at each time point.
Results
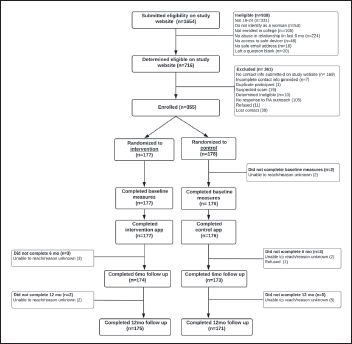
A total of 353 women enrolled and completed the baseline survey (N = 177 intervention; N = 176 control) (Figure 1). Six-month retention was 98.3% for both the intervention (N = 174) and control (N = 173) groups. Twelve-month retention was 98.9% for the intervention group (N = 175) and 96.6% (N = 171) for the control group. Randomization achieved balance on all variables with the exception of age and RC (Table 1). The sample was racially diverse, primarily undergraduates equally divided across year in school, and mostly attending a state or private 4-year college/university and living off-campus. The majority reported their abusive partner was male, an ex-partner, and not living with them.
Demographic and Relationship Characteristics by Study Arm Measured at Baseline.
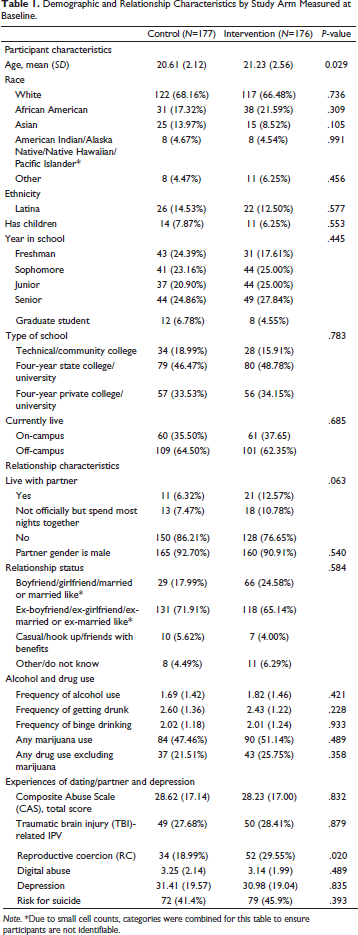
Note. *Due to small cell counts, categories were combined for this table to ensure participants are not identifiable.
Over three quarters (75.9%) of women experienced severe combined IPV, 11.0% emotional abuse and/or harassment without other forms of IPV, 5.7% physical and emotional abuse/harassment, and .6% physical IPV alone; 6.8% screened eligible for the study but did not report IPV in the 6-months prior to the baseline assessment. A total of 28% reported TBI-related IPV and 24.2% reported RC. On average, women reported 3.19 (SD = 2.07) of 7 forms of digital abuse.
At baseline, the majority (77.9%) reported drinking alcohol in the last 30 days. The mean score for getting drunk over last 6 months was 2.52 (SD = 1.30), indicating participants were drunk between a few to half of the occasions they drank. The mean score of binge drinking was 2.02 (SD = 1.21), indicating binge drinking on a few occasions in the past two weeks. Nearly half (49.3%) reported marijuana use and 23.6% used other types of drugs in past 30 days (Table 1).
Safety Behaviors, IPV, Depression, Risk for Suicide
Both groups improved over time in the percent of helpful safety behaviors used (Table 2), but the change over time did not differ between the two groups (p = .294). IPV decreased significantly over time for both groups as measured by CAS (b = −7.574; 95% CI − 8.56, −6.59; p < .001), TBI (b = −.966; 95% CI − 1.24, −.69; p < .001), digital abuse (b = −.457; 95% CI − .54, −.37; p < .001) and RC (b = −.296; 95% CI −.52, −.70; p = .010). The intervention group had a significantly greater reduction in RC than the control group (χ2 = 8.16, p = .017). Depression improved significantly over time for both (b = −2.175; 95% CI −3.22, −1.23; p < .001), but the change over time did not differ between groups (p = .653). The intervention group had a significantly greater improvement over 12-months than the control group on suicide risk (b = −.799; 95% CI − 1.159, −.01; p = .048).
Means (SE) for the Outcomes Over Time by Study Arm.
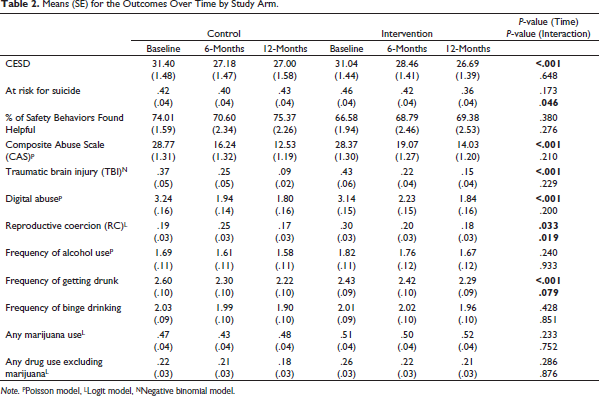
Note. PPoisson model, LLogit model, NNegative binomial model.
Alcohol and Drug Use
Both groups significantly declined over time in the frequency of getting drunk (b = −.134; 95% CI −.23, −.04; p = .005), but did not differ on the rate of decline over time. The change over time in frequency of alcohol use and binge drinking, as well as marijuana or other drug use, was not significant.
Decisional Conflict and Decision Preparedness
Both groups had immediate improvement on all subscales of decisional conflict, change in total DCS for intervention group was greater than control group, and the intervention group women were significantly more positive on “helped you think about which risks and benefits of each safety option are most important to you” (3.82 vs 3.68, p = .038) than control group women. Difference by group was not significant by DCS subscales, informed (p = .513), clarity (p = .246), support (p = .897), and certainty (p = .116) after first use of the intervention. In examining decision preparedness at 12-months, intervention group women were significantly more positive on “prepared to make better safety decisions” (4.11 vs 3.89, p = .022) than control group women.
Relationship Between Safety Behaviors and Decrease in IPV
We hypothesized a stronger relationship between the number of safety behaviors tried and reduction in IPV for the intervention group as compared to the control group. The interaction of group by number of safety behaviors tried was significant (b = −.99; 95% CI − 1.63, −.35; p = .002), meaning the safety behaviors tried effected IPV differentially for the intervention and control groups. The number of behaviors tried was not related to reduction in IPV for the control group (b = .221; 95% CI −.26, .70; p = .364), but it was for the intervention group (b = −.764; 95% CI − 1.19, −.34; p < .001). As the number of safety behaviors tried increased, there was a greater decrease in IPV from baseline to 12-months for the intervention group.
Increases in the percent of safety behaviors found helpful (out of those tried) at 6-months significantly reduced IPV from baseline to 12-months in the intervention group compared to control (b = −.174; 95% CI −.30, −.05; p = .006). The percent of safety behaviors found helpful was not related to IPV reduction for the control group (b = .086; 95% CI −.01, .18; p = .065), but was for the intervention group (b = −.089; 95% CI −.17, .01; p = .039). As the percent of safety behaviors found helpful increases, there is a greater reduction in IPV from baseline to 12-months for the intervention group. The two groups were not different on the number of safety behaviors tried at 6-months (7.78 vs 7.56, p = .685) or the percent found helpful (70.50 vs 68.77, p = .580). Women perceive safety behaviors to be equally helpful in both groups, but only in the intervention group are safety behaviors associated with a reduction in IPV.
Discussion
Use of myPlan significantly reduced young women’s experience of RC, an often-undisclosed form of IPV with potentially life-changing consequences, and risk of suicide, a growing public health crisis for young women, compared to usual safety planning. Women in both groups reported increases in percent of safety behaviors used and helpful, as well as decreases in decisional conflict, misuse of alcohol, symptoms of depression, and IPV, however the changes over time were not significantly different by group. While these results do not support the effectiveness of myPlan over usual safety planning on all outcomes, they support the usefulness of technology-based safety planning for young women that have recently (past 6 months) experienced IPV by a partner or ex-partner.
Awareness of RC remains low and it may not be understood as an abuse/control tactic or one that negatively impacts health (Follingstad et al., 1999). When intervention group participants indicated RC, myPlan tailored their safety plan to include relevant information and safety behaviors; for example, accessing campus or community-based reproductive health services. The tailored plan may have underscored the importance of seeking health and other supportive services to reduce risk of repeat RC. This finding reinforces the role of college-based health providers to provide education about the association between IPV and health outcomes, allowing women a safe place to disclose RC and other forms of IPV and access trauma-informed care.
Engagement in safety behaviors at 6-months significantly reduced IPV from baseline to 12-months in the intervention group, but not in the control group. While IPV decreased overall in the control group, this reduction was not associated with trying more safety strategies or strategies tried to be helpful. Safety plans clearly have benefits, yet a tailored plan with strategies based on input may assist the woman to better understand her situation and take targeted safety actions (Messing et al., 2017).
The intervention group had a significantly greater reduction in suicide risk, but not in symptoms of depression compared to the control group. Participants scored substantively over the threshold of 15, indicating risk for depression with higher scores indicating depression or major depression (depending on how many days symptoms are reported). Depression and suicidality are strongly associated with IPV, and given the seriousness of the IPV in this sample and the evidence of increases in depression and suicidality among U.S. college students (American College Health Association, 2019), the level of depression and suicidality is not surprising, even if highly concerning. Women that used myPlan and who had been in the relationship for a longer period of time had a significantly greater reduction in depression symptoms and risk for suicide from baseline to 12-months compared to the control group. Without intervention, IPV is rarely a one-time event and generally increases in severity and frequency over time, and often leads to isolation from informal and formal support, likely impacting mental health (Johnson, 2006). Intervention group women had access to the DA, with immediate feedback that likely helped in understanding risk of repeat severe IPV (Campbell et al., 2003), identify priorities for safety, and access services that could have reduced exposure to severe IPV, isolation, depression, and suicidality.
Alcohol and drug use was common among women in this study and the results were consistent with 2018 national survey data of young adults (aged 18–25; Substance Abuse and Mental Health Services Administration, 2019). Both the intervention and control groups significantly declined over time in the frequency of getting drunk (p < .001), the groups did not differ on the rate of decline over time. Evidence indicates that alcohol and drug use are related to IPV for college men and women, with women reporting being under the influence of alcohol and drugs when they are psychologically, sexually, and physically victimized (Baker & Stith, 2008; Fossos et al., 2007; Giancola, 2002; Gidycz et al., 2007; Shorey et al., 2011). An adaptation of myPlan is planned to strengthen content on the harmful effects of substance misuse and association with IPV, with tailoring to campus and community-based substance abuse and counseling programs.
The majority of women (65% in intervention and 71% in control groups) reported that IPV in the past 6 months was perpetrated by an ex-partner. Safety planning is critical for women while in an abusive relationship and when they decide to end the relationship, as the use of violence does not necessarily stop when the relationship ends. In fact, ending a relationship can be very dangerous and could trigger the abuser to increase the severity of IPV, including threats and use of harassment, stalking, and physical/sexual violence, due to their feeling of loss of control of the relationship, and can result in woman returning to the relationship to try and reduce their exposure to IPV. As relationships are dynamic and change over time, myPlan provides women 24/7 access to reassess danger and safety priorities to tailor their plan to the situation.
Limitations
Limited geographic diversity (Maryland and Oregon colleges/universities) and stringent criteria for participation (IPV in past 6 months) limit generalizability. Although approximately 2/3 of the sample identified as white, there was a higher proportion of underrepresented minorities in the sample than in U.S. colleges/universities (African Americans, 19.5% vs 13% nationwide, Indigenous students 4.5% vs 1% nationwide). The proportion of Latina students (13.5%) in our study was lower than the 21% U.S. proportion (Postsecondary National Policy Institute (PNPI), 2018). The majority (92%) identified their abusive partner as male and an ex-partner. More effort is needed in collaboration with campus LGBTQ programs to increase participation and improve relevance of myPlan to sexual minority students. Baseline survey measures completed by both groups (e.g., CAS, safety strategies) may have biased findings, as the questions themselves may have functioned as an intervention increasing women’s self-awareness of IPV/RC, safety behaviors, and mental health. Despite randomization, there were differences between groups in participant age and RC experiences, which may have affected outcomes. There is no true control group, as it is unethical to provide “nothing” to women in abusive relationships. Reductions in IPV over time may have been the effect of providing safety planning to both groups, or regression to the mean.
Conclusion
myPlan is a free, secure, anonymous resource accessible 24/7 that facilitates women’s engagement with safety decisions and planning. myPlan is, to our knowledge, the first safety decision and planning intervention delivered via a mobile and web-based app developed specifically for college-aged women, including racial/ethnic and sexual minority young women. The study demonstrates the promise of technology-based interventions to reduce reproductive coercion and risk of suicide among women that had recently experienced IPV by a partner or ex-partner. Importantly, myPlan and other technology-based tools are part of the comprehensive campus and community response to IPV and should not be considered or used as a replacement for skilled advocacy and counseling provided survivor-centered services on campuses and surrounding communities.
CONSORT flow diagram.
Footnotes
Acknowledgments
The study was only possible because young women provided their expertise and time, and college/university staff and student groups advocated for health and safety on campus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Grant Number 1R01HD076881-01A1.
Trial Registration
This study is registered at