
Abstract
Essential steps in the provision of health care for women exposed to intimate partner violence (IPV) are screening and referral for specialized services, as might occur in primary care settings. Prior to participating in a cross-disciplinary IPV training program, medical care (N = 223) and social/behavioral practitioners (N = 197) completed a survey that ascertained current practices, provisions, and perceived barriers related to IPV screening and referral. Roughly half of the study participants did not routinely screen their patients/clients for IPV, with no differences for the professional groupings. Utilization of referral resources was significantly lower for medical care providers, 78.5% of whom did not use any. Perceived barriers to screening and referral were examined as practitioner-based and organization-based, and we identified tangible provisions (protocols and practice materials) as a relevant variable. As we conjectured, organization-based barriers were more strongly associated with lower rates of screening and referral than were practitioner-based barriers, regardless of professional grouping. Moreover, tangible provisions, controlling for perceived barriers, significantly added to routine screening and frequency of referral resources usage, particularly for medical care providers. Results are discussed in the context of a systems-level approach to improving IPV services in health care with organizational practice enhancements.
Keywords
Introduction
The deleterious health consequences of intimate partner violence (IPV) have been established in several major reviews (Akyüz et al., 2012; Cerdá et al., 2012; Ellsberg et al., 2008; Lagdon et al., 2014). IPV is a public health problem with a lifetime prevalence rate for women of 30% worldwide (World Health Organization, 2013). Women exposed to IPV are at increased risk for depression, anxiety, post-traumatic stress disorder, suicidality, anger, and substance abuse, as well as physical health problems, such as fractures, chronic pain, gastrointestinal disorders, hypertension, sinus infections, and reproductive issues (e.g., pelvic inflammation, sexually transmitted diseases, contraceptive interference). These adverse consequences produce higher utilization rates across health care departments—emergency, primary care, medical specialties, and mental health (Plichta, 2004; Tjaden & Thoennes, 2000; Ulrich, et al., 2003).
Medical, mental health, and social service providers are uniquely positioned to identify and intervene in cases of suspected IPV. Yet, as the review by Alvarez et al. (2017) found, despite the serious health concerns associated with IPV, policy recommendations from medical professional organizations, and state laws mandating screening, routine screening rates for IPV in primary care are typically below 10%. Even when providers screen, they often fail to follow-up with appropriate referrals. Rhodes et al. (2011), using police, prosecutor, and medical data to retrospectively examine predictors of emergency room screening behaviors, found only 28% of IPV-exposed women were identified, and of those identified a referral was provided to only 25%. A meta-analysis by O’Doherty et al. (2014) of 11 provider intervention studies found only three studies that included measures of health care providers’ referrals to support agencies; and, in those studies, increases in screening and identification were not associated with increases in referral (Ahmad et al., 2009; Klevens et al., 2012; Trautman et al., 2007).
Considerable research pertinent to health care provider screening and referral has focused on providers’ feelings and perceptions that might constitute barriers to IPV screening, such as providers’ fears of putting patients in greater danger, beliefs that patients will not disclose abuse, concern for legal liability, and lack of language fluency (e.g., Alvarez et al., 2017; Baig et al., 2012; Evans et al., 2019; Sprague et al., 2012). Provider-focused factors have been incorporated into surveys assessing barriers to screening and also as outcome variables for evaluating the effectiveness of training interventions. Other barriers to screening, such as lack of training, inadequate follow-up resources for IPV victims, minimal support staff to counsel victims, absence of office protocols, and time constraints, have received insufficient attention (Sprague et al., 2012). These can be categorized as “organization-based barriers.”
Organization-based barriers may be more relevant than practitioner-based barriers in explaining low IPV screening and referral rates. In their review of 22 studies examining barriers to provider screening for IPV, Sprague et al. (2012) found that concerns for safety and the fear of negative consequences for victims were cited as barriers in less than 20% of studies, while lack of training/knowledge and lack of follow-up resources were cited in 68.2% and 63.6% of studies, respectively. Of all barriers reported across studies, time constraints were most frequently reported, with 81.8% of studies including time constraints as a barrier to screening (Sprague et al., 2012). Thus, shortcomings in IPV screening rates are frequently attributed to organizational impediments.
Pertinently, the few intervention programs that have successfully increased provider screening have been multifaceted, involving intensive skills training and the provision of tangible resources (e.g. referral materials and posters) (Ambuel et al., 2013; Feder et al., 2011; Thompson et al., 1998; Thompson et al., 2000; Zaher et al., 2014). Strictly educational interventions, while generally effective in increasing knowledge concerning IPV and self-efficacy beliefs, have not been found to improve victim identification (Zaher et al., 2014).
The Current Study
No study, to our knowledge, has compared the relative importance of practitioner-based versus organization-based barriers to provider screening and referral. Given the relevance for effective interventions targeting provider screening and referral behaviors, we sought to identify a range of factors associated with practitioner-reported screening and referral practices in a sample of medical care and social/behavioral health providers attending a brief IPV training program. Considering the paucity of studies concerning social/behavioral health providers, we conducted separate analyses for the two provider groups. Drawing from literature on the success of interventions targeting organizational barriers to IPV screening, we hypothesized that organizational barriers, compared to practitioner barriers, would be more strongly associated with providers’ routine screening for IPV, as well as providers’ referral of patients to resources.
Method
Setting
Participants were medical care and social/behavioral providers who chose to attended a Cross-Disciplinary Training (CDT) program (some received continuing education credits) held at various community locations in southern California. Developed by University of California, Irvine faculty, along with a consortium of Orange County domestic/family violence service agencies, the CDT program was aimed at improving IPV screening, counseling, and referrals. The program involved a brief (60–90 minute) PowerPoint presentation on IPV pertinent to health care and service provisions in the community. Resource materials were provided during the training to familiarize participants with services in the local community to which patients could be referred. The program, jointly presented by a medical doctor and a social service professional, was delivered on 30 occasions over a 2-year period. Research ethics approval for the study was obtained from the Institutional Review Board of the University of California, Irvine.
Procedure
Prior to the beginning of each CDT presentation, research assistants administered a brief (5–7 minute) pretraining survey 1
The pretraining survey was constructed by the Olin Group, in conjunction with members of the Orange County Women’s Health Project team, which included the authors.
“Domestic violence” was the term used in the questionnaire, as that was more familiar to the participants than “intimate partner violence”.
Participants’ survey responses were gathered without personal identifiers, and survey anonymity was assured when the surveys were distributed. Participants were instructed to complete the survey as accurately as possible. Once all participants completed the pretraining survey, research assistants collected all survey forms. When survey collection was completed, the training presentation began. To ensure pretraining data accuracy, participants who arrived during survey collection were not given the pretraining survey.
Exclusions and missing data. A total of 692 participants attended the CDT program. To be eligible for inclusion in the present study, participants had to be medical care or social/behavioral providers, had to have fully completed questions concerning our outcome variables (routine screening and use of resources to make referrals), and had to have completed more than 75% of items comprising each of our predictor variables. Excluded from the study sample were 89 administrative/other professionals, 96 medical and nursing students, 78 providers with missing responses on either one or both outcome variables, and nine providers who failed to respond to more than 75% of items on the practitioner and/or organizational barriers scales. Mean imputation was used to account for missing data, and 22 and 13 participants, respectively, had values imputed on the Practitioner Barriers and the Organizational Barriers scales.
Sample
The two-group sample was comprised of 420 participants, whose professional characteristics are given in Table 1. The majority identified as female (N = 339). The medical care provider group (53.1% of the sample) consisted of physicians, physician assistants, medical assistants, dentists, and nurses. The social/behavioral health provider group (46.9% of the sample) consisted of social workers, case managers, counselor/therapists, psychologists, health educators, and peer specialists. Most participants (55.6%) worked in their respective professions for six or more years, and 58% of them spoke to their patients in languages other than English, as they served diverse populations in many facilities throughout a large southern California county.
Characteristics of Medical Care and Social/Behavioral Providers.
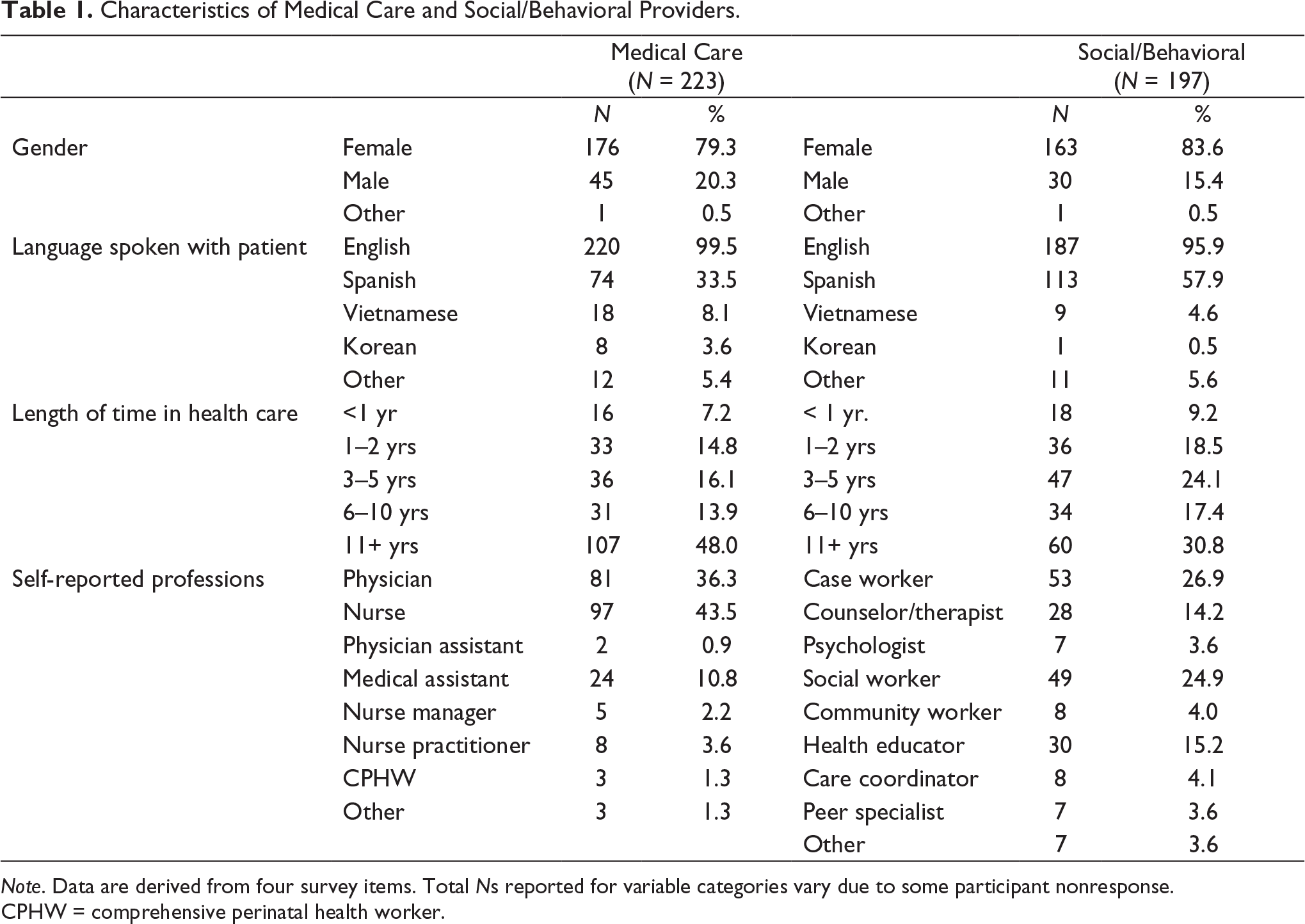
Note. Data are derived from four survey items. Total Ns reported for variable categories vary due to some participant nonresponse.
CPHW = comprehensive perinatal health worker.
Measures
Predictor Variables
Practitioner barriers. A total score summed the ratings for eight statements concerning practitioner barriers to screening, each having a 6-point rating scale of 0 = “strongly disagree” to 5 = “strongly agree.” The statements are as follows: “It is not my role to screen for domestic violence (DV)”; “I am comfortable asking DV screening questions”; “I am worried about offending the patient/client if I screen for DV”; “I don’t think patients/clients will tell me about abuse in their relationship even if I ask”; “Language is a barrier for me to screen for DV”; “I am concerned about potential legal liability for me if I screen for DV”; “I am concerned about negative consequences for me if I get involved with a DV case”; and “I am concerned that if I refer my patient/client for DV services, she or he will be in more danger.” Total possible scores ranged from 0 to 40. The summary score for this 8-item scale has a satisfactory internal reliability (alpha = .76).
Organizational barriers. A total score summed responses to four statements concerning perceptions of organizational barriers to screening, rated on a 6-point scale of 0 = “strongly disagree” to 5 = “strongly agree.” The statements are as follows: “I don’t have enough time to screen, counsel, and refer patients/clients for domestic violence”; “I haven’t had enough training about screening and counseling for domestic violence”; “I don’t know enough about resources to which I can refer patients/clients who screen positively for DV”; and “My institution and/or my superiors are supportive of DV screening, counseling, and referring” (reverse coded). The summary score for this 4-item scale had marginal internal consistency (alpha = .64).
Tangible provisions. A tangible provisions variable was created by summing responses to seven survey items. The first four items concerned the existence of written policies/protocols for domestic violence and asked as separate questions: “Does your office/practice have a written policy/protocol for domestic violence (1) screening, (2) counseling, (3) referring, and (4) mandatory reporting?” The subsequent three items are as follows: (5) “Does your office/practice currently screen patients/clients for domestic violence?” (6) “Does your office/practice have posters about domestic violence displayed where patients/clients can see them?” and (7) “Does your office/practice have materials about domestic violence and how to seek help in the waiting room, restroom, or clinical areas that patients/clients can take with them?” For all seven items, the response options are as follows: “yes,” “no,” and “don’t know/not sure.” A summary variable was created by counting the “yes” responses to the seven items. Scores closer to 7 indicated the presence of more provisions to address IPV.
Criterion Variables
Routine screening. A dichotomous variable was created by collapsing participant responses to the item “How often do you screen a patient/client for domestic violence.” Response options to the item included: “never,” “only when I believe there is a potential indication of domestic violence,” “once a year,” “every 2–3 appointments,” “every appointment,” and an open-ended option “other.” Response options “never” and “only when I believe there is a potential indication of domestic violence” were collapsed to create the category “no routine screening,” while “once a year,” “every 2–3 appointments,” and “every appointment” were collapsed to create the category “routine screening.” Participants who indicated “other” were analyzed on a case-by-case basis and were coded into one of the two dichotomous routine screening categories.
Referral resource use. A continuous variable was created by summing participant responses to six indicators of the use of resources to make a referral for DV services. All six resource indicators were preceded with the question: “In the last 3 months, about how often have you used the following resources to make a referral for DV services?” The indicators included: “I have called 2-1-1 Orange County, 3
“2-1-1 Orange County” is a private, nonprofit organization that connects people to existing programs, providing a county-wide resource database for health and human services; it is continuously accessible online and through a multilingual hotline.
Results
Professional Group Differences
There were 207 (49.3% of 420) participants who routinely screened for domestic violence, and 191 (45.5%) who indicated using at least one resource to make a referral in the past 3 months. No professional group differences were found in routine screening rates, but a significantly greater (p < .001) proportion of social/behavioral providers used designated community resources to make a referral than did medical care providers, as shown in Table 2.
Intimate Partner Violence Routine Screening and Referral Rates.
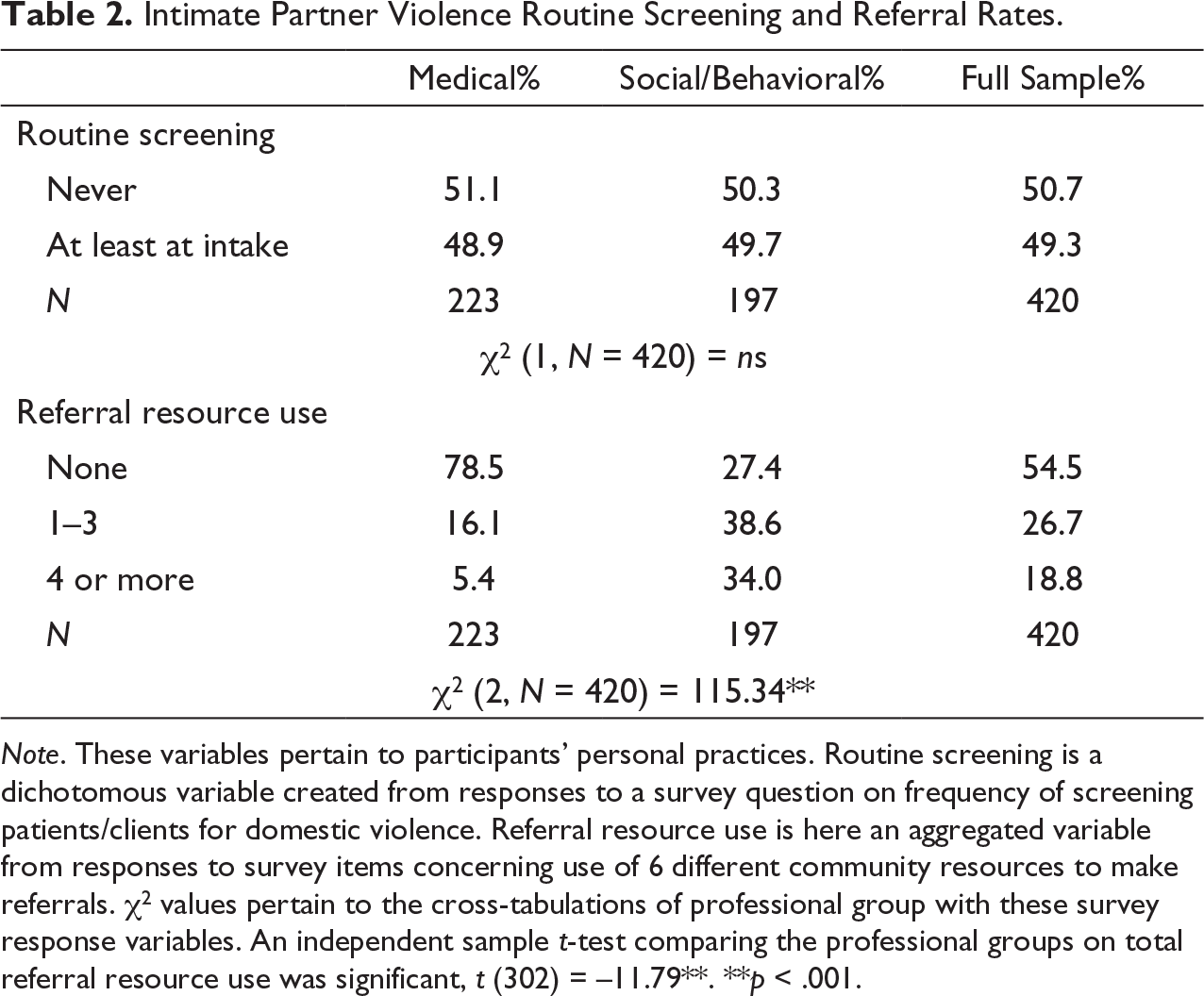
Note. These variables pertain to participants’ personal practices. Routine screening is a dichotomous variable created from responses to a survey question on frequency of screening patients/clients for domestic violence. Referral resource use is here an aggregated variable from responses to survey items concerning use of 6 different community resources to make referrals. χ 2 values pertain to the cross-tabulations of professional group with these survey response variables. An independent sample t-test comparing the professional groups on total referral resource use was significant, t (302) = –11.79**.
**p < .001.
There were significant differences between the professional groups in perceived barriers to IPV screening and referral. Compared to social/behavioral providers, medical care providers reported significantly more practitioner-based barriers (p < .01) and organization-based barriers (p < .001) to screening (Table 3). Despite these differences, the professional groups had some similar concerns, as both provider groups provided the highest endorsement of “not enough training” and “don’t know enough about patient resources” as barriers to screening and referral.
Perceived Barriers to IPV Screening and Referral by Professional Group: Practitioner-Based and Organization-Based.
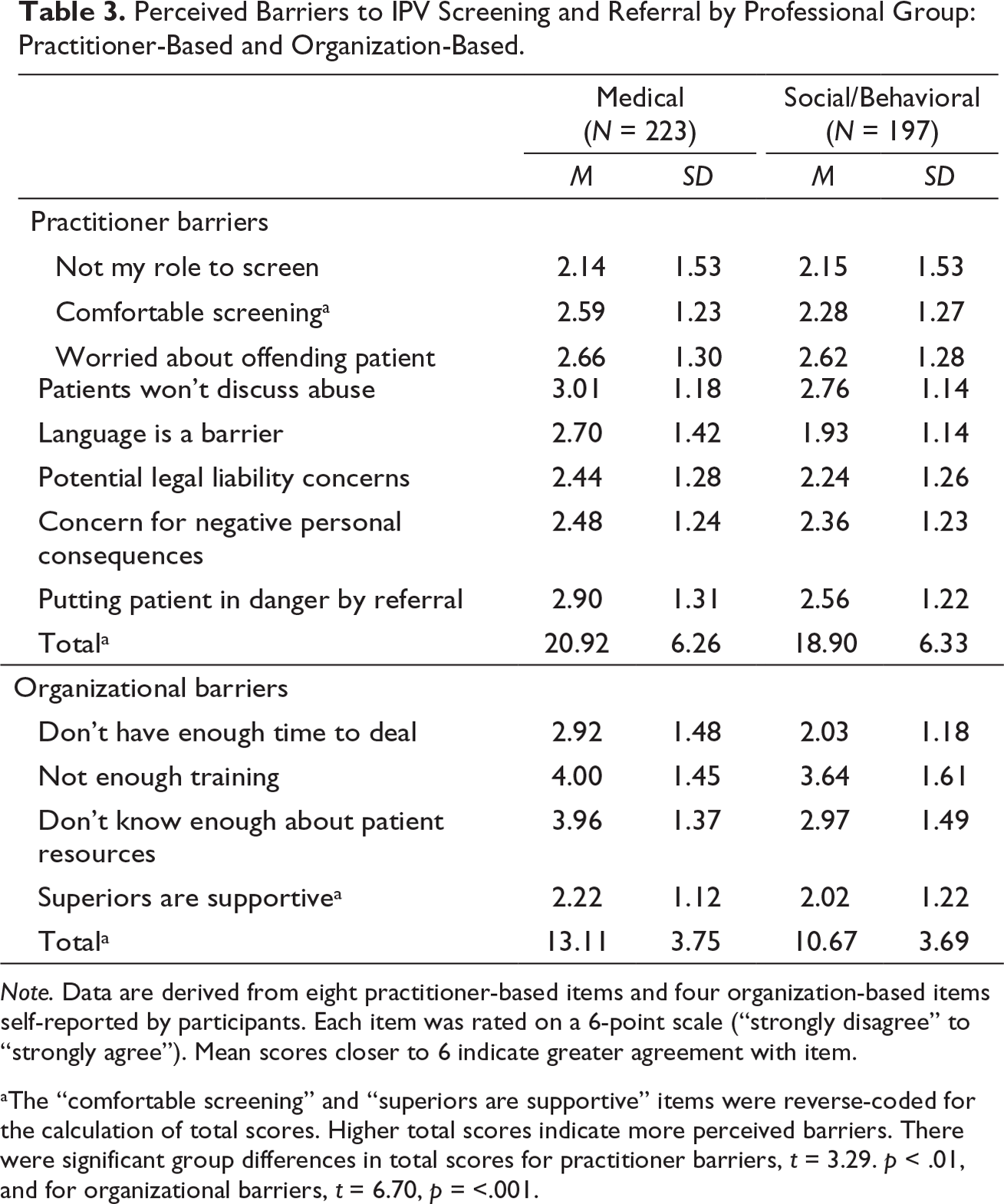
Note. Data are derived from eight practitioner-based items and four organization-based items self-reported by participants. Each item was rated on a 6-point scale (“strongly disagree” to “strongly agree”). Mean scores closer to 6 indicate greater agreement with item.
aThe “comfortable screening” and “superiors are supportive” items were reverse-coded for the calculation of total scores. Higher total scores indicate more perceived barriers. There were significant group differences in total scores for practitioner barriers, t = 3.29. p < .01, and for organizational barriers, t = 6.70, p = <.001.
Table 4 shows professional group differences in organizational policies/protocols, office practice on screening, and whether supplemental materials pertinent to domestic violence are provided. Convergent with the findings on perceived barriers, compared to social/behavioral providers, a significantly smaller percentage of medical care providers reported having policies/protocols for screening, counseling, referring, and mandatory reporting (p < .01 for each). They were also less likely to indicate that their offices/practices screened patients for IPV, and they were less likely to report having DV posters and referral materials displayed in the workplace. The bottom of Table 4 shows results for the total count of “yes” endorsements for the seven tangible provisions. Medical care providers reported having significantly less, t (418) = –3.80, p < .001, of the organization-based provisions than did social/behavioral providers.
Tangible Provisions: Organizational Policies/Protocols, Office Screening Practices, and Provisions.
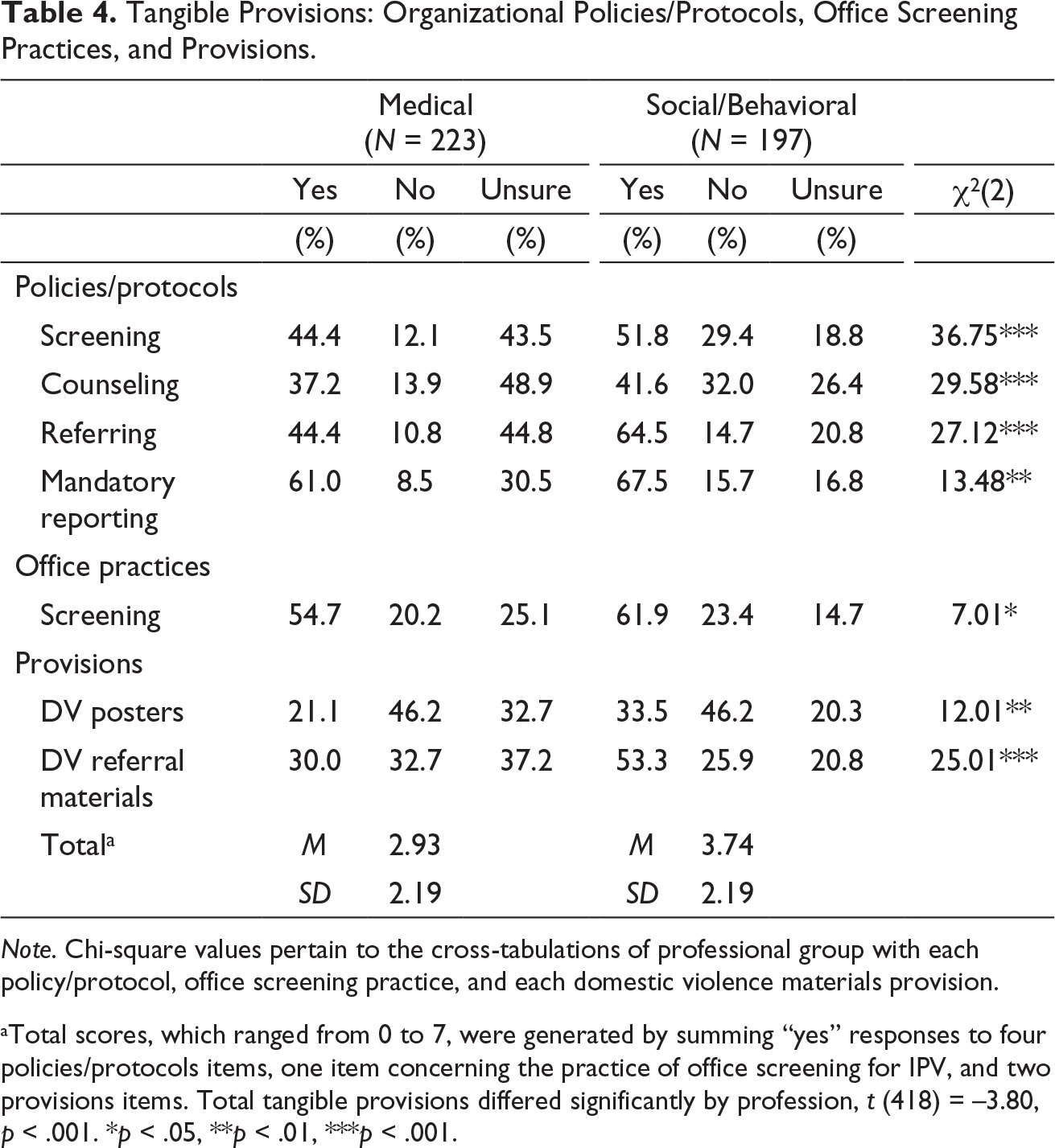
Note. Chi-square values pertain to the cross-tabulations of professional group with each policy/protocol, office screening practice, and each domestic violence materials provision.
aTotal scores, which ranged from 0 to 7, were generated by summing “yes” responses to four policies/protocols items, one item concerning the practice of office screening for IPV, and two provisions items. Total tangible provisions differed significantly by profession, t (418) = –3.80, p < .001. *p < .05, **p < .01, ***p < .001.
Potential Covariates
Gender and years of practitioner experience were explored as potential confounds of the relation between our barriers and provisions variables and the criterion variables of routine screening and referrals. A series of correlations and a chi-square test found no statistically significant associations for these potential covariates; hence, we excluded them.
Barriers and Provisions Bearing on Screening and Referral
We conducted a series of hierarchical regressions to ascertain whether organizational barriers and tangible provisions explained variation in provider routine screening and referral resource use above and beyond practitioner barriers. Separate regression models were run for each of our criterion variables, within each professional group. Models concerning routine screening were analyzed using binary logistic regression, while ordinary least squares (OLS) regression was used for the referral resource use criterion. Across all models, practitioner barriers were entered on the first Step, followed by organizational barriers and tangible provisions in the second and third Steps, respectively. Results for medical care providers are presented in Table 5, while those for social/behavioral providers are presented in Table 6.
Medical Care Providers’ IPV Routine Screening and Referral Resource Use as Associated with Barriers and Provisions.
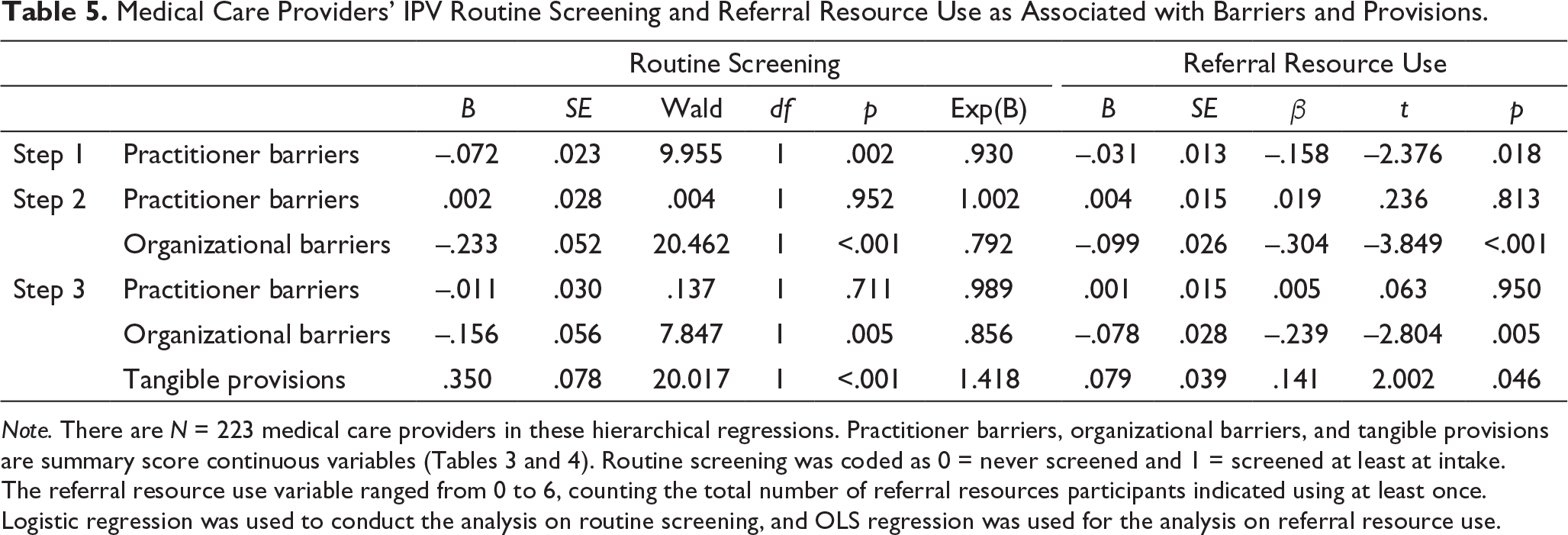
Note. There are N = 223 medical care providers in these hierarchical regressions. Practitioner barriers, organizational barriers, and tangible provisions are summary score continuous variables (Tables 3 and 4). Routine screening was coded as 0 = never screened and 1 = screened at least at intake. The referral resource use variable ranged from 0 to 6, counting the total number of referral resources participants indicated using at least once. Logistic regression was used to conduct the analysis on routine screening, and OLS regression was used for the analysis on referral resource use.
Social/Behavioral Providers’ IPV Routine Screening and Referral Resource Use as Associated With Barriers and Provisions.
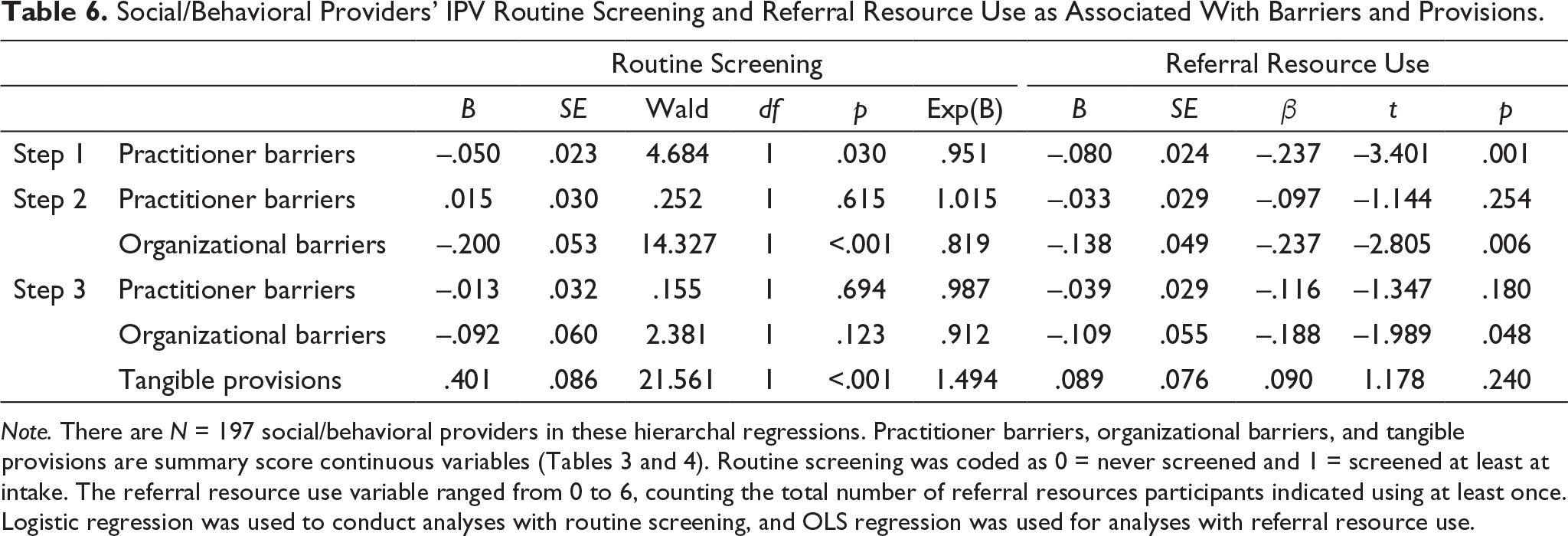
Note. There are N = 197 social/behavioral providers in these hierarchal regressions. Practitioner barriers, organizational barriers, and tangible provisions are summary score continuous variables (Tables 3 and 4). Routine screening was coded as 0 = never screened and 1 = screened at least at intake. The referral resource use variable ranged from 0 to 6, counting the total number of referral resources participants indicated using at least once. Logistic regression was used to conduct analyses with routine screening, and OLS regression was used for analyses with referral resource use.
For medical care providers, baseline models revealed a significant inverse relationship between practitioner barriers and both routine screening and referral resource use. However, once organizational barriers were entered on Step 2, these associations became nonsignificant, and organizational barriers emerged as being significantly associated with routine screening and referral resource use. Regarding proportion of variance explained, statistical prediction of routine screening and referral resource use were significantly improved by the addition of organizational barriers: respectively, χ 2 change (1, N = 223) = 23.55, p <.001, and R change = .06, F (1, 220) = 14.81, p < .001. On Step 3, the inclusion of tangible provisions in the final models further accounted for variance in routine screening, χ 2 change (1, N = 223) = 21.97, p < .001), and referral resource use, R change = .02, F (1, 219) = 4.01, p < .05. In the final models for both criteria, organizational barriers and tangible provisions, but not practitioner barriers, were significant predictors. The more organizational barriers and the less tangible provisions medical care providers reported, the lower their referral resource use, and the lower their likelihood of having routinely screened for IPV.
Similarly, baseline models for social/behavioral providers revealed that practitioner barriers were significantly and inversely related to both routine screening and referral resource use. Consistent with the findings for medical care providers, these associations became nonsignificant once organizational barriers were entered, and organizational barriers were significant as statistical predictors of both criterion variables. Change statistics showed that the addition of organizational barriers significantly improved prediction of social/behavioral providers’ routine screening practices, χ 2 change (1, N = 197) = 15.69, p <.001, and referral resource use, R change = .04, F (1, 194) = 7.87, p < .01. The addition of tangible provisions in Step 3 explained additional variance in routine screening, χ 2 change (1, N = 197) = 24.50, p < .001, but not referral resource use, R change = .01, F (1, 193) = 1.39, p = .24. In the final models for the social/behavioral providers, tangible provisions were significantly associated with routine screening; for referral resource use, only the organizational barriers variable was significant (semipartial r 2 = .018).
Discussion
Our study investigated whether barriers to IPV screening, disaggregated by their source (i.e., whether provider-based or organization-based), were differentially associated with IPV screening and referral practices. We further differentiated our inquiry by professional grouping, conducting separate analyses for medical care and social/behavioral care providers. The major findings of our study are that organization-based barriers to IPV screening are strongly associated with deficits in screening practices, beyond what can be attributed to provider-based barriers, and that an organization’s tangible provisions for IPV screening and referrals are incrementally associated with whether screening is done routinely and whether community referral resources are used.
While we found no professional group differences in whether the participants themselves routinely screened for IPV, the medical care providers less frequently used community resources for IPV referrals, and they perceived significantly more practitioner and organizational barriers to screening and referral. Also, compared to their social/behavioral counterparts, medical care providers reported having significantly less organization-based policies/protocols for IPV-related practices and informative material provisions. Neither participant gender nor years of experience were statistically relevant factors.
We identified tangible provisions as a potentially important variable bearing on IPV screening and referral practices and found it to be significantly associated with routine screening for both professional groups, controlling for practitioner and organizational barriers. With the addition of each tangible provision, there was approximately a 40% increase in the likelihood that medical care practitioners would routinely screen. Regarding referral resource use, which was a count variable, the tangible provisions variable was incrementally significant for medical care providers, explaining an additional 2% of variation beyond the barrier variables, but was not significant for social/behavioral providers. For the latter group, organizational barriers became the only significant variable in accounting for referral resource use.
Our study participants were practitioners working with diverse populations in many facilities in a southern California county, and the majority of them spoke to their patients in languages other than English. Our results are consistent with the Davis et al. (1992) review findings regarding 50 clinical trials of medical education programs, for which interventions that integrated educational and organizational elements (e.g., protocols, materials, prompts) were more effective than were purely educational interventions in affecting sustained changes in provider screening and counseling behaviors. Our results support emerging literature stressing the need for systemic approaches in affecting sustained change in IPV screening (Evans et al., 2019; Hamberger et al., 2015). Studies conducted on the effect of organizational-level changes on provider screening and referral behavior show outcomes that are in line with our study’s findings (e.g., Ambuel et al., 2013; Campbell et al., 2001; Keily et al., 2010; McCaw, 2011).
Study Limitations
Our study data were obtained from voluntary participants in a county-wide women’s health project’s continuing education program on domestic violence, recruited with the support of their work organizations. Thus, they are a nonrandom, convenience sample, self-selected with an interest in domestic violence as a health problem. This sample selection bias may be reflected in participants’ reported screening rate (49.3% indicated routinely screening), which is much higher than what is typically reported in the literature. Alvarez et al. (2017) stated that “studies consistently show that routine screening rates in primary care are 10% or lower” (p. 480), and their review of 35 studies found a range of 2%–50%. Further, the cross-sectional nature of our study limits inferences about whether the perceived barriers and identified provisions causally influence screening and referral practices.
Our referral resource use variable did not differentiate whether providers, who indicated using any of six resources, actually made a direct referral for services or simply provided information to patients about community services. Also, the referral resources use section of our survey had four response options, and three of them (“1–2 times,” “3–5 times,” and “more than 5 times”) were collapsed into one category, condensing variation in frequency of use. O’Doherty et al. (2014) in their review called attention to there being substantial variation in how “referral” is operationalized as an outcome criterion, which then obscures understanding of the screening-referral relationship. How organizational barriers and provisions in our study bear on providers’ actual referral behavior needs clarification through future research.
While factors affecting provider screening behavior have been widely investigated, less is known about factors predicting providers’ referral of patients to IPV services. Our study demonstrated that the presence of organizational barriers decreased the likelihood that providers would utilize resources to make referrals for IPV services, but our assessment was from the standpoint of practitioners’ perceptions of barriers that we classified as organizational. It would have been better to have had some independent index of our identified organizational barriers (i.e., insufficiencies regarding IPV training, knowledge of community resources, supportiveness of supervisors, and patient care time available for IPV screening).
Study Implications and Conclusions
Sawyer et al. (2016), in their review of IPV training interventions for allied health care practitioners, identified four studies that assessed postintervention changes in provider behaviors. Educational interventions had significant effects on behavior across all four studies, although in one study (Hsieh et al., 2006), the outcome measure was a provider’s self-reported intention to screen. The other three studies, which assessed providers’ behavior, involved multicomponent interventions, combining didactic and interactive elements. Boursnell and Prosser (2010) incorporated frameworks, flow charts, and focus groups, and Jayatilleke et al. (2015) integrated role-playing and case reports, in addition to the provision of a 60-page manual on IPV. The intervention by Janssen et al. (2002) featured “hands-on” demonstrations, as well as the provision of resource cards and posters. The Sawyer et al. (2016) review unfortunately missed the study by Ambuel et al. (2013) of a multifaceted intervention in primary care clinics and an emergency department, involving a 20-hour training of health care advocates concerning IPV, 3-hour training of all clinical and administrative staff, and provision of a “clinical toolbox” of resources. They found significant improvements in clinicians’ behavior and in system-level provisions, evidenced by practitioner surveys at three time points, chart audits, and environmental audits, which were sustained two years after the intervention.
That tangible provisions pertinent to IPV were in our study predictive of providers’ reported screening behaviors, controlling for their perceived barriers, points to the value of augmenting organizational practices (such as implementing IPV protocols and providing patients with informational materials) that can boost traditionally low screening rates. An example of a potentially valuable organization-based provision would be computer-assisted self-administered screening, which was found in the review by Hussain et al. (2015) to increase the odds of IPV disclosure by 37% and 23%, respectively, in comparison to face-to-face screening and to self-administered written screening. To improve IPV referral practices, attention should be given to boosting training opportunities and providing easy links to referral resources.
The implementation of such organizational changes hinges on the support of leaders, managers, and policymakers. Hamberger et al. (2015) noted that the first steps in implementing organization-based changes in IPV screening are securing buy-in of key system decision-makers and the planning of system-wide implementation. Partnership with community agencies and experts on IPV, intensive training of in-house advocates to build on-site IPV expertise, and saturation training of clinical and administrative staff, as was done in the Ambuel et al. (2013) intervention study, then can provide for sustainable systems change (Hamberger et al., 2015).
Given the increased health care costs associated with IPV, research demonstrating the cost-effectiveness of organizational interventions will be crucial in eliciting the support of health care leaders and insurance providers. Relevant outcome variables could include patient follow-up rates of IPV exposure, mental and physical health outcomes, health care service usage, and health care costs. While time windows for patient care will likely remain constricted, added practitioner training on the ramifications of IPV for physical and psychological health, on IPV screening tools, and on available community resources, along with support from service managers, would all be feasible organizational practice enhancements.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the training program, with which this study was associated, was provided by the Blue Shield of California Foundation through Charitable Ventures of Orange County and the Orange County Women’s Health Project, under the directorship of Allyson W. Sonenshine, JD.